
Human Respiratory Syncytial Virus Epidemiological Burden in Pediatric Outpatients in Italy: A Systematic Review

 , ,
, ,  , , ,
, , ,  ,
,  , , and
, , and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Record Study Search
2.3. Inclusion and Exclusion Criteria
2.4. Screening and Study Selection
2.5. Data Retrieval and Analysis
2.6. Quality Assessment of the Included Studies
3. Results
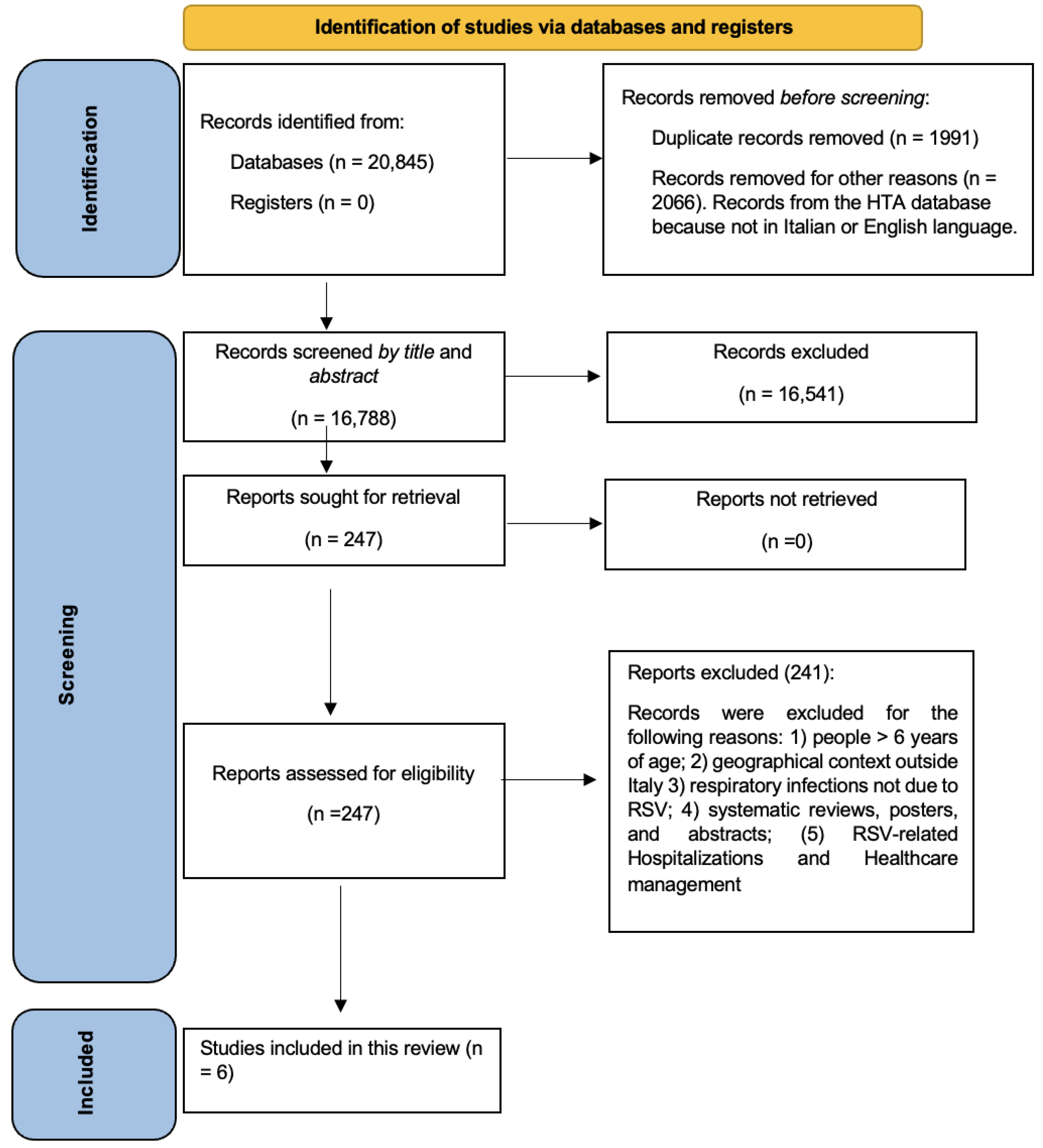
3.1. Selection Process
3.2. HRSV-Associated Epidemiological Burden in Italy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; A Madhi, S.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Del Riccio, M.; Spreeuwenberg, P.; Osei-Yeboah, R.; Johannesen, C.K.; Vazquez Fernandez, L.; Teirlinck, A.C.; Wang, X.; Heikkinen, T.; Bangert, M.; Caini, S.; et al. Burden of Respiratory Syncytial Virus in the European Union: Estimation of RSV-associated hospitalizations in children under 5 years. J. Infect. Dis. 2023, jiad188. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics. Report of the committee of infectious diseases. In Red Book 2018–2021, 31st ed.; American Academy of Pediatrics: Elk Grove Village, IL, USA, 2018; pp. 682–692. [Google Scholar]
- Lively, J.Y.; Curns, A.T.; A Weinberg, G.; Edwards, K.M.; A Staat, M.; Prill, M.M.; I Gerber, S.; E Langley, G. Respiratory Syncytial Virus-Associated Outpatient Visits Among Children Younger Than 24 Months. J. Pediatr. Infect. Dis. Soc. 2019, 8, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Heppe Montero, M.; Gil-Prieto, R.; Walter, S.; Aleixandre Blanquer, F.; Gil De Miguel, Á. Burden of severe bronchiolitis in children up to 2 years of age in Spain from 2012 to 2017. Hum. Vaccin. Immunother. 2022, 18, 1883379. [Google Scholar] [CrossRef]
- Kuhdari, P.; Brosio, F.; Malaventura, C.; Stefanati, A.; Orsi, A.; Icardi, G.; Gabutti, G. Human respiratory syncytial virus and hospitalization in young children in Italy. Ital. J. Pediatr. 2018, 44, 50. [Google Scholar] [CrossRef] [PubMed]
- Simões, E.A.F. The Burden of Respiratory Syncytial Virus Lower Respiratory Tract Disease in Infants in the United States: A Synthesis. J. Infect. Dis. 2022, 226, S143–S147. [Google Scholar] [CrossRef]
- Reeves, R.M.; van Wijhe, M.; Tong, S.; Lehtonen, T.; Stona, L.; Teirlinck, A.C.; Fernandez, L.V.; Li, Y.; Giaquinto, C.; Fischer, T.K.; et al. Respiratory Syncytial Virus-Associated Hospital Admissions in Children Younger Than 5 Years in 7 European Countries Using Routinely Collected Datasets. J. Infect. Dis. 2020, 222, S599–S605. [Google Scholar] [CrossRef]
- Meissner, H.C. Viral Bronchiolitis in Children. N. Engl. J. Med. 2016, 374, 62–72. [Google Scholar] [CrossRef]
- Pneumonia Etiology Research for Child Health (PERCH) Study Group. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: The PERCH multi-country case-control study. Lancet 2019, 394, 757–779. [Google Scholar] [CrossRef]
- Boyoglu-Barnum, S.; Chirkova, T.; Anderson, L.J. Biology of Infection and Disease Pathogenesis to Guide RSV Vaccine Development. Front. Immunol. 2019, 10, 1675. [Google Scholar] [CrossRef]
- Griffiths, C.; Drews, S.J.; Marchant, D.J. Respiratory Syncytial Virus: Infection, Detection, and New Options for Prevention and Treatment. Clin. Microbiol. Rev. 2017, 30, 277–319. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; Baraldi, E.; Bonanni, P.; Bozzola, E.; Coscia, A.; Lanari, M.; Manzoni, P.; Mazzone, T.; Sandri, F.; Piacentini, G.; et al. Epidemiology and prevention of respiratory syncytial virus infections in children in Italy. Ital. J. Pediatr. 2021, 47, 198. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.B.; Weinberg, G.A.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Schultz, A.F.; Poehling, K.A.; Szilagyi, P.G.; Griffin, M.R.; Williams, J.V.; et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics 2013, 132, e341–e348. [Google Scholar] [CrossRef]
- Rha, B.; Curns, A.T.; Lively, J.Y.; Campbell, A.P.; Englund, J.A.; Boom, J.A.; Azimi, P.H.; Weinberg, G.A.; Staat, M.A.; Selvarangan, R.; et al. Respiratory Syncytial Virus-Associated Hospitalizations Among Young Children: 2015-2016. Pediatrics 2020, 146, e20193611. [Google Scholar] [CrossRef] [PubMed]
- Wilkesmann, A.; Ammann, R.A.; Schildgen, O.; Eis-Hübinger, A.M.; Müller, A.; Seidenberg, J.; Stephan, V.; Rieger, C.; Herting, E.; Wygold, T.; et al. Hospitalized children with respiratory syncytial virus infection and neuromuscular impairment face an increased risk of a complicated course. Pediatr. Infect. Dis. J. 2007, 26, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Stagliano, D.R.; Nylund, C.M.; Eide, M.B.; Eberly, M.D. Children with Down syndrome are high-risk for severe respiratory syncytial virus disease. J. Pediatr. 2015, 166, 703–709.e2. [Google Scholar] [CrossRef] [PubMed]
- Arriola, C.S.; Kim, L.; Langley, G.; Anderson, E.J.; Openo, K.; Martin, A.M.; Lynfield, R.; Bye, E.; Como-Sabetti, K.; Reingold, A.; et al. Estimated Burden of Community-Onset Respiratory Syncytial Virus-Associated Hospitalizations Among Children Aged <2 Years in the United States, 2014–2015. J. Pediatric. Infect. Dis. Soc. 2020, 9, 587–595. [Google Scholar] [CrossRef]
- Wright, M.; Piedimonte, G. Respiratory syncytial virus prevention and therapy: Past, present, and future. Pediatr. Pulmonol. 2011, 46, 324–347. [Google Scholar] [CrossRef]
- Rezaee, F.; Linfield, D.T.; Harford, T.J.; Piedimonte, G. Ongoing developments in RSV prophylaxis: A clinician’s analysis. Curr. Opin. Virol. 2017, 24, 70–78. [Google Scholar] [CrossRef]
- European Medicines Agency. Synagis—Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/synagis-epar-product-information_en.pdf (accessed on 12 July 2023).
- European Medicines Agency. Beyfortus, Nirsevimab. Summary of Opinion (Initial Authorisation). 15 September 2022. EMA/CHMP/647784/2022. Committee for Medicinal Products for Human Use (CHMP). Available online: https://www.ema.europa.eu/en/documents/smop-initial/chmp-summary-positive-opinion-beyfortus_en.pdf (accessed on 12 July 2023).
- Agenzia Italiana del Farmaco (AIFA). DETERMINA 2 Novembre 2017. Revoca della Determina n. 1407/2016 del 20 Ottobre 2016, Recante: «Sostituzione del Piano Terapeutico di cui All’allegato 1) della Determina 15 Maggio 2015, n. 604» e Conferma delle Determine Numeri 604/2015 del 15 Maggio 2015, Recante: «Riclassificazione del Medicinale per uso Umano "Synagis", ai sensi Dell’articolo 8, comma 10, della legge 24 Dicembre 1993, n. 537» e 1234/2016 del 15 Settembre 2016, Recante: «Inserimento del Medicinale "Palivizumab" (Synagis) Nell’elenco dei Medicinali Erogabili a Totale Carico del Servizio Sanitario Nazionale». (Determina DG/1836/2017). (17A07585) (GU Serie Generale n.262 del 09-11-2017). Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario;jsessionid=dJR5FAdYFLSNYnPO-kP3PA__.ntc-as3-guri2a?atto.dataPubblicazioneGazzetta=2017-11-09&atto.codiceRedazionale=17A07585&elenco30giorni=false (accessed on 12 July 2023).
- European Medicines Agency. Beyfortus, Nirsevimab. Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/beyfortus-epar-product-information_en.pdf (accessed on 12 July 2023).
- Società Italiana di Pediatria Posizione del Board Calendario per la Vita e SIN su Anticorpo Monoclonale per Prevenzione Malattie da VRS. Available online: https://sip.it/2023/02/17/vrs-calendario-per-la-vita-e-sin/ (accessed on 12 July 2023).
- Manti, S.; Staiano, A.; Orfeo, L.; Midulla, F.; Marseglia, G.L.; Ghizzi, C.; Zampogna, S.; Carnielli, V.P.; Favilli, S.; Ruggieri, M.; et al. UPDATE—2022 Italian Guidelines on the Management of Bronchiolitis in Infants. Ital. J. Pediatr. 2023, 49, 19. [Google Scholar] [CrossRef]
- PATH. RSV Vaccine and mAb Snapshot. Available online: https://www.path.org/resources/RSV-vaccine-and-mab-snapshot/ (accessed on 12 July 2023).
- Arexvy. European Medicines Agency (EMA). Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/arexvy (accessed on 8 September 2023).
- Abrysvo. European Medicines Agency (EMA). Available online: https://www.ema.europa.eu/en/medicines/human/summaries-opinion/abrysvo (accessed on 8 September 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Don, M.; Fasoli, L.; Paldanius, M.; Vainionpää, R.; Kleemola, M.; Räty, R.; Leinonen, M.; Korppi, M.; Tenore, A.; Canciani, M. Aetiology of community-acquired pneumonia: Serological results of a paediatric survey. Scand. J. Infect. Dis. 2005, 37, 806–812. [Google Scholar] [CrossRef]
- Pellegrinelli, L.; Galli, C.; Bubba, L.; Cereda, D.; Anselmi, G.; Binda, S.; Gramegna, M.; Pariani, E. Respiratory syncytial virus in influenza-like illness cases: Epidemiology and molecular analyses of four consecutive winter seasons (2014–2015/2017–2018) in Lombardy (Northern Italy). J. Med. Virol. 2020, 92, 2999–3006. [Google Scholar] [CrossRef]
- Tramuto, F.; Maida, C.M.; Di Naro, D.; Randazzo, G.; Vitale, F.; Restivo, V.; Costantino, C.; Amodio, E.; Casuccio, A.; Graziano, G.; et al. Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI. Vaccines 2021, 9, 1334. [Google Scholar] [CrossRef]
- Van Summeren, J.J.G.T.; Rizzo, C.; Hooiveld, M.; Korevaar, J.C.; Hendriksen, J.M.T.; Dückers, M.L.A.; Loconsole, D.; Chironna, M.; Bangert, M.; Demont, C.; et al. Evaluation of a standardised protocol to measure the disease burden of respiratory syncytial virus infection in young children in primary care. BMC Infect. Dis. 2021, 21, 705. [Google Scholar] [CrossRef]
- Rizzo, C.; Loconsole, D.; Pandolfi, E.; Ciofi Degli Atti, M.L.; van Summeren, J.; Paget, J.; Russo, L.; Campagna, I.; Croci, I.; Gesualdo, F.; et al. SARS-COV2 Not Detected in a Pediatric Population With Acute Respiratory Infection in Primary Care in Central and Southern Italy From November 2019 to Early March 2020. Front. Pediatr. 2021, 9, 620598. [Google Scholar] [CrossRef]
- Pellegrinelli, L.; Galli, C.; Bubba, L.; Seiti, A.; Anselmi, G.; Primache, V.; Signorini, L.; Delbue, S.; Binda, S.; Pariani, E. Respiratory syncytial virus in pediatric influenza-like illness cases in Lombardy, Northern Italy, during seven consecutive winter seasons (from 2014–2015 to 2020–2021). Influenza Other Respir. Viruses 2022, 16, 481–491. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Broberg, E.K.; Campbell, H.; Nair, H.; European RSV Surveillance Network. Seasonality of respiratory syncytial virus and its association with meteorological factors in 13 European countries, week 40 2010 to week 39 2019. Euro Surveill. 2022, 27, 2100619. [Google Scholar] [CrossRef]
- Tang, J.W.; Loh, T.P. Correlations between climate factors and incidence—A contributor to RSV seasonality. Rev. Med. Virol. 2014, 24, 15–34. [Google Scholar] [CrossRef]
- Baker, R.; Park, S.; Yang, W.; Vecchi, G.; Metcalf, C.; Grenfell, B. The impact of COVID-19 nonpharmaceutical interventions on the future dynamics of endemic infections. Proc. Natl. Acad. Sci. USA 2020, 117, 30547–30553. [Google Scholar] [CrossRef]
- Eden, J.S.; Sikazwe, C.; Xie, R.; Deng, Y.M.; Sullivan, S.G.; Michie, A.; Levy, A.; Cutmore, E.; Blyth, C.C.; Britton, P.N.; et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat. Commun. 2022, 13, 2884. [Google Scholar] [CrossRef]
- Bozzola, E. 2021 respiratory syncytial virus resurgence in Italy: The need to protect all neonates and young infants. Int. J. Environ. Res. Public Health 2022, 19, 380. [Google Scholar] [CrossRef] [PubMed]
- Hamid, S.; Winn, A.; Parikh, R.; Jones, J.M.; McMorrow, M.; Prill, M.M.; Silk, B.J.; Scobie, H.M.; Hall, A.J. Seasonality of Respiratory Syncytial Virus—United States, 2017–2023. MMWR Morb Mortal Wkly Rep. 2023, 72, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Istituto Superiore di Sanità. Rapporto InfluNet, Settimana 2023-17 (Aggiornamento 5 Maggio 2023). Available online: https://w3.iss.it/site/rmi/influnet/pagine/rapportoinflunet.aspx (accessed on 31 May 2023).
- Bont, L.; Checchia, P.A.; Fauroux, B.; Figueras-Aloy, J.; Manzoni, P.; Paes, B.; Simões, E.A.; Carbonell-Estrany, X. Defining the Epidemiology and Burden of Severe Respiratory Syncytial Virus Infection Among Infants and Children in Western Countries. Infect. Dis. Ther. 2016, 5, 271–298. [Google Scholar] [CrossRef] [PubMed]
- Posizione del Board del Calendario Vaccinale per la Vita e della Società Italiana di Neonatologia sul Possibile Utilizzo di Anticorpi Monoclonali a Lunga Emivita per la Prevenzione Universale delle Malattie da Virus Respiratorio Sinciziale (VRS o RSV) nel Neonato. Available online: https://www.sin-neonatologia.it/wp-content/uploads/2023/02/Position-Paper_Anticorpo-monoclonale-per-VRS.pdf (accessed on 31 May 2023).

{kind=link}
{kind=link}
| Author | Region/City | Time of Observation | Case Definition | Age (as Reported by Each Study) | hRSV-Cases/Total (n/N) | hRSV-Positivity Proportion (%) |
|---|---|---|---|---|---|---|
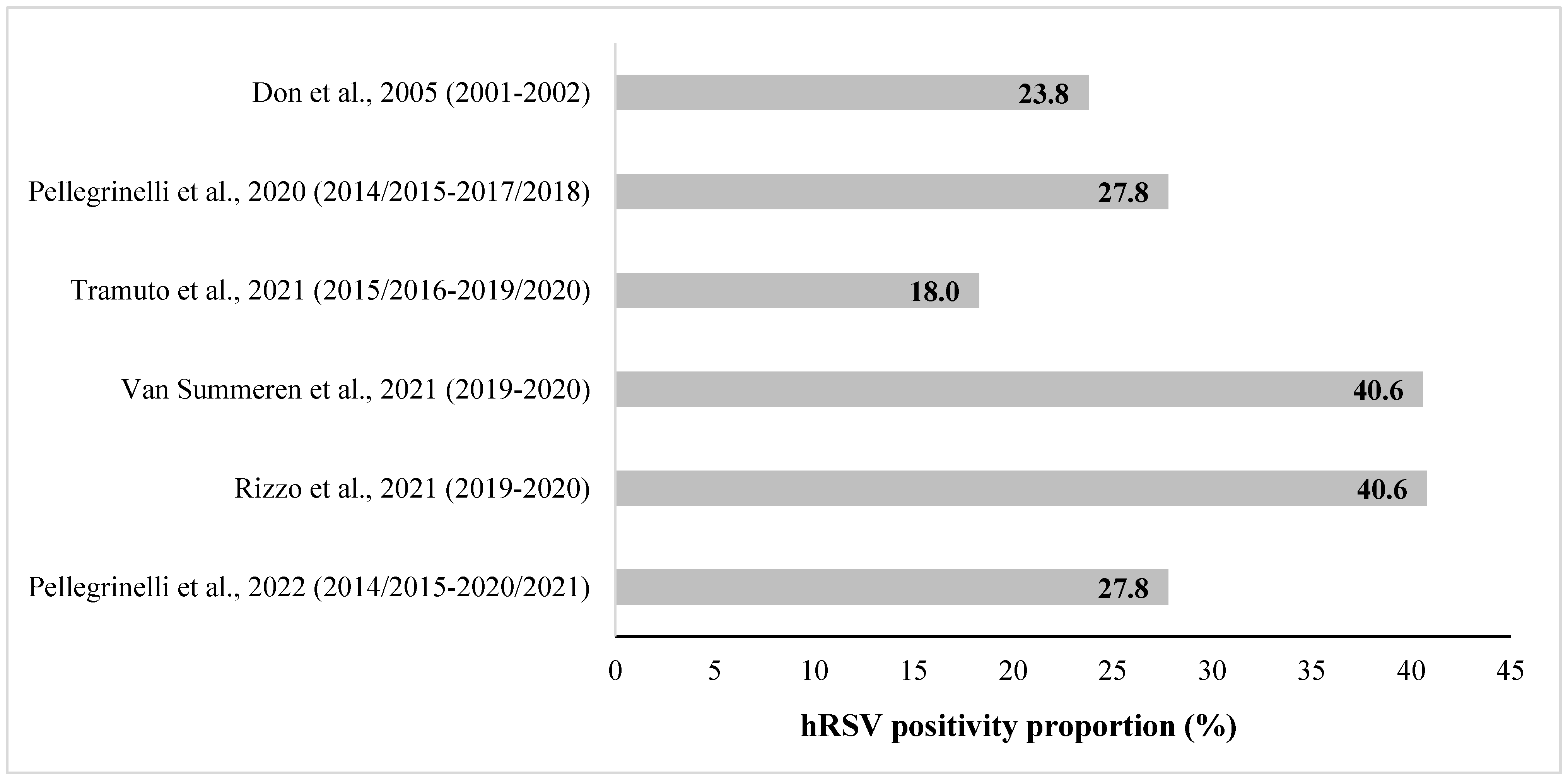
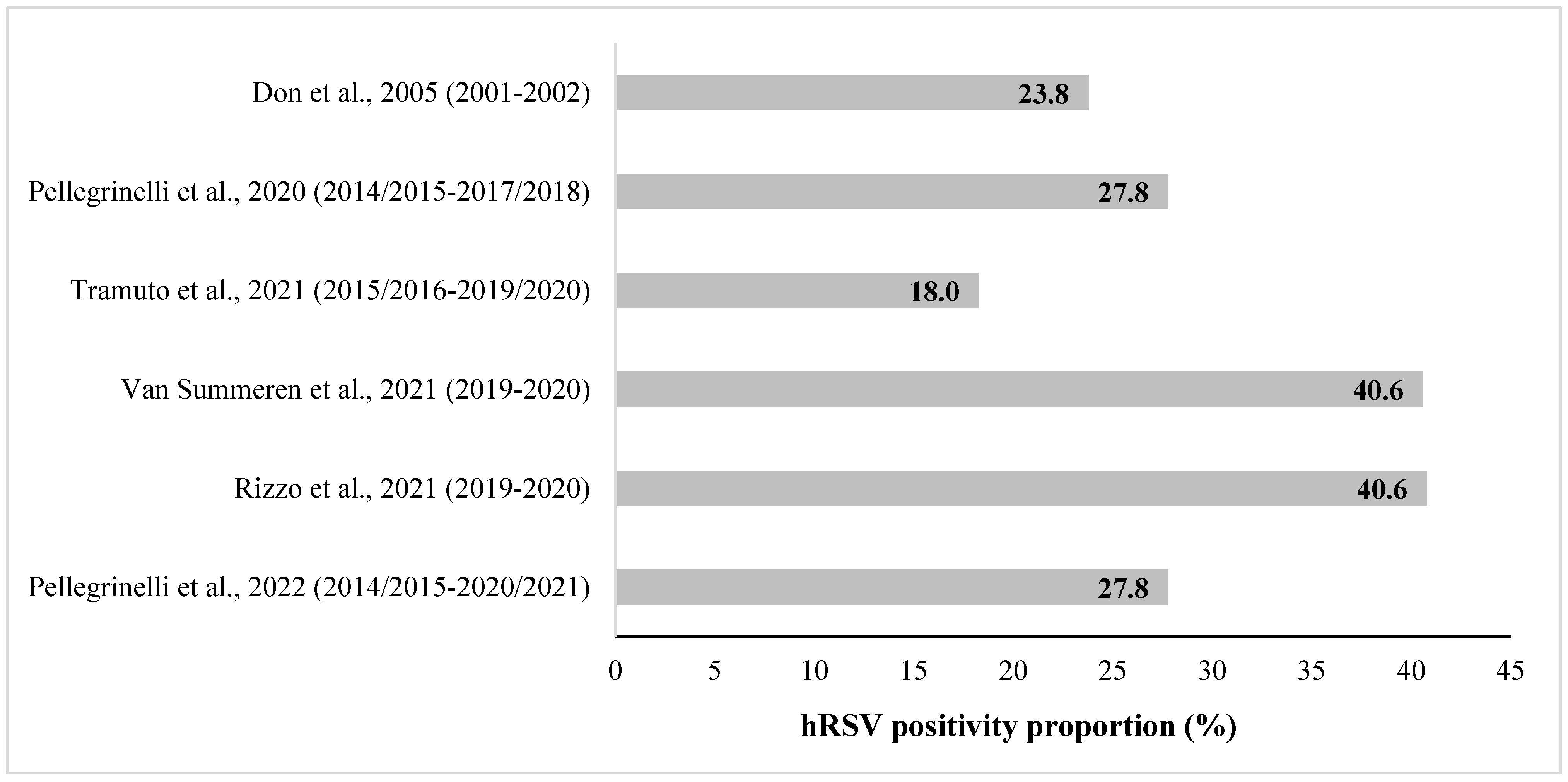
| Don M, 2005 [31] | Udine (city, Northern Italy) | Season 2001/2002 | CAP | <5 years | 10/42 | 23.8 |
| Pellegrinelli L, 2020 [32] | Lombardy (region, Northern Italy) | From 2014/2015 to 2017/2018 | ILI | ≤5 years | 51/183 | 27.8 |
| Tramuto F, 2021 [33] | Sicily (region, Southern Italy) | From 2015/2016 to 2019/2020 | ILI, SARI | 0–11 months 12–23 months 2–4 years | 44/232 107/561 319/1816 | 19.0 19.1 17.6 |
| Van Summeren JJGT, 2021 [34] | Lazio (region, Central Italy) and Puglia (region, Southern Italy) | Season 2019/2020 | ARI | <5 years | 119/293 | 40.6 |
| Rizzo C, 2021 [35] | Lazio (region, Central Italy) and Puglia (region, Southern Italy) | Season 2019/2020 | ARI | 0–12 months 13–24 months 25–60 months | 53/130 26/70 40/93 | 40.8 37.1 43.0 |
| Pellegrinelli L, 2022 [36] | Lombardy (region, Northern Italy) | From 2014/2015 to 2020/2021 | ILI | ≤5 years | 103/370 | 27.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boccalini, S.; Bonito, B.; Salvati, C.; Del Riccio, M.; Stancanelli, E.; Bruschi, M.; Ionita, G.; Iamarino, J.; Bentivegna, D.; Buscemi, P.; et al. Human Respiratory Syncytial Virus Epidemiological Burden in Pediatric Outpatients in Italy: A Systematic Review. Vaccines 2023, 11, 1484. https://doi.org/10.3390/vaccines11091484
Boccalini S, Bonito B, Salvati C, Del Riccio M, Stancanelli E, Bruschi M, Ionita G, Iamarino J, Bentivegna D, Buscemi P, et al. Human Respiratory Syncytial Virus Epidemiological Burden in Pediatric Outpatients in Italy: A Systematic Review. Vaccines. 2023; 11(9):1484. https://doi.org/10.3390/vaccines11091484
Chicago/Turabian StyleBoccalini, Sara, Benedetta Bonito, Cristina Salvati, Marco Del Riccio, Enrica Stancanelli, Mario Bruschi, Giulia Ionita, Johanna Iamarino, Davide Bentivegna, Primo Buscemi, and et al. 2023. "Human Respiratory Syncytial Virus Epidemiological Burden in Pediatric Outpatients in Italy: A Systematic Review" Vaccines 11, no. 9: 1484. https://doi.org/10.3390/vaccines11091484
APA StyleBoccalini, S., Bonito, B., Salvati, C., Del Riccio, M., Stancanelli, E., Bruschi, M., Ionita, G., Iamarino, J., Bentivegna, D., Buscemi, P., Ciardi, G., Cosma, C., Stacchini, L., Conticello, C., Bega, M., Schirripa, A., Paoli, S., Bertizzolo, L., Parisi, S., ... Bechini, A. (2023). Human Respiratory Syncytial Virus Epidemiological Burden in Pediatric Outpatients in Italy: A Systematic Review. Vaccines, 11(9), 1484. https://doi.org/10.3390/vaccines11091484