
Surveying a Sample of the Spanish Ophthalmologic Community about Vaccination against Herpes Zoster


 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
- Select your professional category.
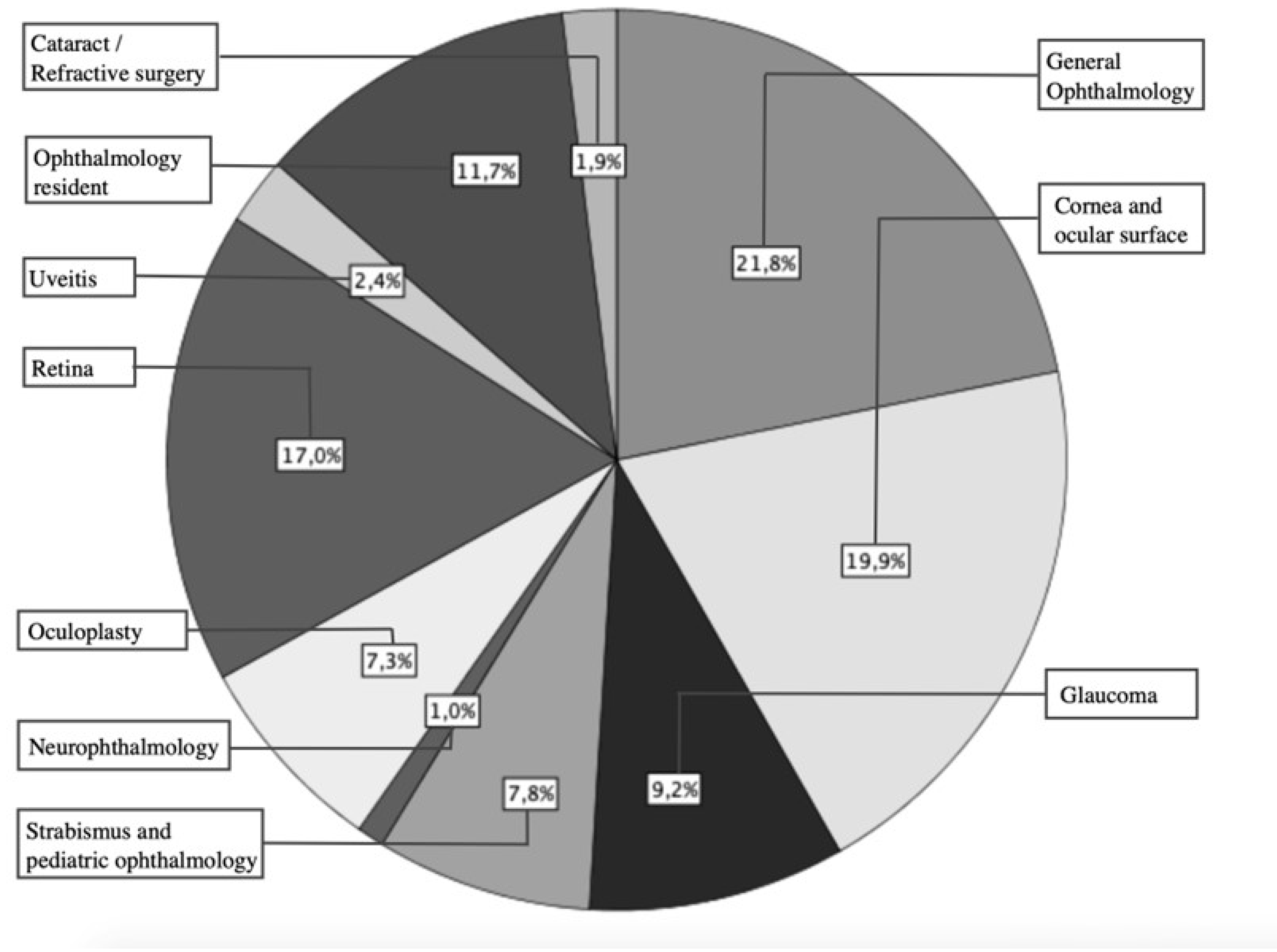
- Select the subspecialty to which you dedicate most of your time.
- Professional experience.
- Work center where you carry out most of your activity.
- Autonomous Community in which you carry out most of your work activity.
- How often do you see patients who have suffered or are suffering from ophthalmological involvement of HZ?
- Do you think that HZ is a common cause of vision loss?
- What percentage of HZ disease do you consider has ophthalmological involvement?
- Do you know about the existence of vaccines for HZ?
- Do you know if there is an HZ vaccine marketed in Spain?
- If so, do you know in which cases vaccination is recommended?
- Have you ever indicated vaccination against HZ to any of your patients?
- If you want to recommend vaccination against HZ, do you know how to request it?
- How effective is vaccination with Shingrix (recombinant vaccine) in the prevention of ophthalmicus HZ?
- How effective is vaccination with Zostavax (attenuated virus vaccine) in the prevention of ophthalmicus HZ?
- If vaccination against HZ were effective and safe, do you think it would be important to recommend it from an ophthalmological point of view?
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jeng, B.H. Herpes Zoster Eye Disease: New Ways to Combat an Old Foe? Ophthalmology 2018, 125, 1671–1674. [Google Scholar] [CrossRef] [PubMed]
- Li, J.Y. Herpes Zoster Ophthalmicus: Acute Keratitis. Curr. Opin. Ophthalmol. 2018, 29, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Yawn, B.P.; Wollan, P.; Harpaz, R. Increasing Incidence of Herpes Zoster over a 60-Year Period from a Population-Based Study. Clin. Infect. Dis. 2021, 63, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Gebremeskel, B.G.; Acosta, C.J. Systematic Review of Incidence and Complications of Herpes Zoster: Towards a Global Perspective. BMJ Open 2014, 4, e004833. [Google Scholar] [CrossRef] [PubMed]
- Pinchinat, S.; Cebrián-Cuenca, A.M.; Bricout, H.; Johnson, R.W. Similar Herpes Zoster Incidence across Europe: Results from a Systematic Literature Review. BMC Infect. Dis. 2013, 13, 170. [Google Scholar] [CrossRef] [PubMed]
- Masa-Calles, J.; López-Perea, N.; Vila Cordero, B.; Carmona, R. Vigilancia y Epidemiología Del Herpes Zóster En España. Rev. Española Salud Pública 2021, 95, 25–26. [Google Scholar]
- Marra, F.; Chong, M.; Najafzadeh, M. Increasing Incidence Associated with Herpes Zoster Infection in British Columbia, Canada. BMC Infect. Dis. 2016, 16, 589. [Google Scholar] [CrossRef]
- Kong, C.L.; Thompson, R.R.; Porco, T.C.; Kim, E.; Acharya, N.R. Incidence Rate of Herpes Zoster Ophthalmicus: A Retrospective Cohort Study from 1994 through 2018. Ophthalmology 2020, 127, 324–330. [Google Scholar] [CrossRef]
- Harpaz, R.; Leung, J.W. The Epidemiology of Herpes Zoster in the United States during the Era of Varicella and Herpes Zoster Vaccines: Changing Patterns among Older Adults. Clin. Infect. Dis. 2019, 69, 341–344. [Google Scholar] [CrossRef]
- Yawn, B.P.; Wollan, P.C.; St. Sauver, J.L.; Butterfield, L.C. Herpes Zoster Eye Complications: Rates and Trends. Mayo Clin. Proc. 2013, 88, 562–570. [Google Scholar] [CrossRef]
- Weinmann, S.; Naleway, A.L.; Koppolu, P.; Baxter, R.; Belongia, E.A.; Hambidge, S.J.; Irving, S.A.; Jackson, M.L.; Klein, N.P.; Lewin, B.; et al. Incidence of Herpes Zoster among Children: 2003–2014. Pediatrics 2019, 144, 331–332. [Google Scholar] [CrossRef] [PubMed]
- Schmader, K.E.; Levin, M.J.; Gnann, J.W.; McNeil, S.A.; Vesikari, T.; Betts, R.F.; Keay, S.; Stek, J.E.; Bundick, N.D.; Su, S.C.; et al. Efficacy, Safety, and Tolerability of Herpes Zoster Vaccine in Persons Aged 50–59 Years. Clin. Infect. Dis. 2012, 54, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, A.; Galor, A. Current Vaccines for the Prevention of Herpes Zoster. Curr. Opin. Ophthalmol. 2018, 29, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Oxman, M.N.; Levin, M.J.; Johnson, G.R.; Schmader, K.E.; Straus, S.E.; Gelb, L.D.; Arbeit, R.D.; Simberkoff, M.S.; Gershon, A.A.; Davis, L.E.; et al. A Vaccine to Prevent Herpes Zoster and Postherpetic Neuralgia in Older Adults. N. Engl. J. Med. 2005, 352, 2271–2284. [Google Scholar] [CrossRef]
- Sun, Y.; Kim, E.; Kong, C.L.; Arnold, B.F.; Porco, T.C.; Acharya, N.R. Effectiveness of the Recombinant Zoster Vaccine in Adults Aged 50 and Older in the United States: A Claims-Based Cohort Study. Clin. Infect. Dis. 2021, 73, 949–956. [Google Scholar] [CrossRef]
- Ojeda Ruiz, E.; Cordero, B.V.; Sastre, M.; Amillategui, R.; Santos, D.; Masa-Calles, J.; López-Perea, N.; Carmona Alférez, R. Red Nacional de Vigilancia Epidemiológica Herpes Zóster. Informe epidemiológico sobre la situación de Herpes Zóster en España, 1998-2018 Resultados de la Red Nacional de Vigilancia Epidemiológica Madrid. Madrid, Spain, August 2020. [Google Scholar]
- Williams, W.W.; Lu, P.J.; O’Halloran, A.; Kim, D.K.; Grohskopf, L.A.; Pilishvili, T.; Skoff, T.H.; Nelson, N.P.; Harpaz, R.; Markowitz, L.E.; et al. Surveillance of Vaccination Coverage among Adult Populations-United States, 2015. MMWR Surveill. Summ. 2017, 66, 1–28. [Google Scholar] [CrossRef]
- Walensky, R.P.; Anne Schuchat, D.; Daniel Jernigan, P.B.; Bunnell, R.; Layden, J.; Kent, C.K.; Gottardy, A.J.; Leahy, M.A.; Martinroe, J.C.; Spriggs, S.R.; et al. Morbidity and Mortality Weekly Report Surveillance of Vaccination Coverage Among Adult Populations-United States, 2018 Surveillance Summaries Centers for Disease Control and Prevention MMWR Editorial and Production Staff (Serials) MMWR Editorial Board. 2021. Available online: https://www.cdc.gov/mmwr/volumes/70/ss/ss7003a1.htm (accessed on 9 April 2023).
- American Academy of Ophthalmology Recommendations for Herpes Zoster Vaccine for Patients 50 Years of Age and Older. Available online: https://www.aao.org/education/clinical-statement/recommendations-herpes-zoster-vaccine-patients-50- (accessed on 9 April 2023).
- Galvis, V.; Tello, A.; Carreño, N.I.; Berrospi, R.D.; Niño, C.A.; Rey, J.J. Herpes Zoster Vaccination: An Urgent Priority. Cornea 2018, 37, e57–e58. [Google Scholar] [CrossRef]
- Tsui, E.; Gillespie, C.; Perskin, M.; Zabar, S.; Wu, M.; Cohen, E.J. Evaluating Physician Attitudes and Practices Regarding Herpes Zoster Vaccination. Cornea 2018, 37, 947–951. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO Framework to Improve Searching PubMed for Clinical Questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Shankar, P.R.; Davenport, M.S.; Woolen, S.A.; Carlos, R.C.; Maturen, K.E. Survey Research: A Primer for the Academic Radiologist. Acad. Radiol. 2018, 25, 751–756. [Google Scholar] [CrossRef]
- Bennett, C.; Khangura, S.; Brehaut, J.C.; Graham, I.D.; Moher, D.; Potter, B.K.; Grimshaw, J. Reporting Guidelines for Survey Research: An Analysis of Published Guidance and Reporting Practices. PLoS Med. 2011, 8, e1001069. [Google Scholar] [CrossRef] [PubMed]
- Kelley, K.; Clark, B.; Brown, V.; Sitzia, J. Good Practice in the Conduct and Reporting of Survey Research. Int. J. Qual. Health Care 2003, 15, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Draugalis, J.L.R.; Coons, S.J.; Plaza, C.M. Best Practices for Survey Research Reports: A Synopsis for Authors and Reviewers. Am. J. Pharm. Educ. 2008, 72, 11. [Google Scholar] [CrossRef] [PubMed]
- Peterson, R. Constructing Effective Questionnaires; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2014; ISBN 9780761916413. [Google Scholar]
- Álvarez-Pasquín, M.J.; Morató, M.L.; Sampedro, A.; San-Martín, M. Perception of Herpes Zoster in the General Population. Vacunas 2011, 12, 86–94. [Google Scholar] [CrossRef]
- Jacob, V.; Chattopadhyay, S.K.; Hopkins, D.P.; Murphy Morgan, J.; Pitan, A.A.; Clymer, J.M. Increasing Coverage of Appropriate Vaccinations: A Community Guide Systematic Economic Review. Am. J. Prev. Med. 2016, 50, 797–808. [Google Scholar] [CrossRef]
- Amirthalingam, G.; Andrews, N.; Keel, P.; Mullett, D.; Correa, A.; de Lusignan, S.; Ramsay, M. Evaluation of the Effect of the Herpes Zoster Vaccination Programme 3 Years after Its Introduction in England: A Population-Based Study. Lancet Public Health 2018, 3, e82–e90. [Google Scholar] [CrossRef]
- Sanidad, Grupo de Trabajo. Comisión de Salud Pública Del Consejo Interterritorial Del Sistema Nacional de Salud. Ministerio de Sanidad, Marzo 2021. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/programasDeVacunacion/docs/HerpesZoster_RecomendacionesVacunacion.pdf (accessed on 9 April 2023).
- Price, N.B.; Grose, C. Corticosteroids Contribute to Serious Adverse Events Following Live Attenuated Varicella Vaccination and Live Attenuated Zoster Vaccination. Vaccines 2021, 9, 23. [Google Scholar] [CrossRef]
- Lu, A.; Sun, Y.; Porco, T.C.; Arnold, B.F.; Acharya, N.R. Effectiveness of the Recombinant Zoster Vaccine for Herpes Zoster Ophthalmicus in the United States. Ophthalmology 2021, 128, 1699–1707. [Google Scholar] [CrossRef]
- Pan, C.X.; Lee, M.S.; Nambudiri, V.E. Global Herpes Zoster Incidence, Burden of Disease, and Vaccine Availability: A Narrative Review. Ther. Adv. Vaccines Immunother. 2022, 10, 251513552210845. [Google Scholar] [CrossRef]
- Vallejo Torres, L.; Linertová, R.; Sanromá Ramos, E.; Ramos García, V.; Toledo Chávarri, A.; Herrera Ramos, E.; Pérez Martín, J.J.; Limia Sánchez, A.; Soler Soneira, M.; Castilla Catalán, J.; et al. Coste-Efectividad de la Vacunación Frente a Herpes Zóster. Ministerio de Sanidad, Consumo y Bienestar Social. Servicio de Evaluación del Servicio Canario de la Salud; 2018. Informes de Evaluación de Tecnologías Sanitarias. Available online: https://www3.gobiernodecanarias.org/sanidad/scs/content/05752564-e041-11e9-abf6-eb731501abed/SESCS_2018_VacunasZoster.pdf (accessed on 9 April 2023).
- Ferrara, M.; Romano, V.; Iovino, C.; Kadhim, M.R.; van Dijk, E.H.C.; Boon, C.J.F.; Grassi, P.; Demirel, S.; Cartes, C.; Romano, M.R. Tips to Optimize Digital Education in Ophthalmology: Results from ESASO Survey. Eur. J. Ophthalmol. 2023, 33, 745–753. [Google Scholar] [CrossRef]
- Ferrara, M.; Romano, V.; Steel, D.H.; Gupta, R.; Iovino, C.; van Dijk, E.H.C.; Ferrara, M.; Steel, D.H.; Gupta, R.; Iovino, C.; et al. Reshaping Ophthalmology Training after COVID-19 Pandemic. Eye 2020, 34, 2089–2097. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Years of Experience | |||||
|---|---|---|---|---|---|
| <5 | 5–10 | 10–20 | >20 | p Value | |
| Percentage of ophthalmologists who considered that HZ is a common cause of visual loss n (%) | 29 (74%) | 18 (58%) | 21(51%) | 28(43%) | p = 0.003 |
| Question | “Yes” Respondents n (%) | ||
|---|---|---|---|
| All Respondents | Respondents Excluding Trainees | Cornea and Ocular Surface Subgroup | |
| Do you know about the existence of vaccines for HZ? | 151 (73.3) | 127 (72.6) | 35 (89.7) |
| Do you know if there is a HZ vaccine marketed in Spain? | 104 (50.5) | 89 (50.9) | 24 (61.5) |
| Do you know in which case vaccination is indicated? | 60 (29.1) | 54 (30.9) | 16 (41) |
| If you want to recommend vaccination against HZ, do you know how to request it? | 20 (9.7) | 19 (10.9) | 5 (12.8) |
| Efficacy Rate Estimation of the Shingrix© and Zostavax© Vaccines | All Respondents n(%) | Cornea and Ocular Surface Subgroup n(%) | ||
|---|---|---|---|---|
| Shingrix© | Zostavax© | Shingrix© | Zostavax© | |
| <20% | 9 (4.4) | 14 (6.8) | 2 (4.9) | 3 (7.3) |
| 20–50% | 69 (33.5) | 70 (34) | 10 (24.4) | 10 (24.4) |
| 50–80% | 95 (41.6) | 98 (47.6) | 21 (51.2) | 21 (51.2) |
| >80% | 33 (16) | 24 (11.7) | 8 (19.5) | 7 (17.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Mellado, A.; Alcaraz-Clemente, L.; Rodríguez-Calvo-de-Mora, M.; Sánchez-González, J.-M.; Ortiz-Perez, S.; Rocha-de-Lossada, C. Surveying a Sample of the Spanish Ophthalmologic Community about Vaccination against Herpes Zoster. Vaccines 2023, 11, 952. https://doi.org/10.3390/vaccines11050952
Sánchez-Mellado A, Alcaraz-Clemente L, Rodríguez-Calvo-de-Mora M, Sánchez-González J-M, Ortiz-Perez S, Rocha-de-Lossada C. Surveying a Sample of the Spanish Ophthalmologic Community about Vaccination against Herpes Zoster. Vaccines. 2023; 11(5):952. https://doi.org/10.3390/vaccines11050952
Chicago/Turabian StyleSánchez-Mellado, Alberto, Luis Alcaraz-Clemente, Marina Rodríguez-Calvo-de-Mora, José-María Sánchez-González, Santiago Ortiz-Perez, and Carlos Rocha-de-Lossada. 2023. "Surveying a Sample of the Spanish Ophthalmologic Community about Vaccination against Herpes Zoster" Vaccines 11, no. 5: 952. https://doi.org/10.3390/vaccines11050952
APA StyleSánchez-Mellado, A., Alcaraz-Clemente, L., Rodríguez-Calvo-de-Mora, M., Sánchez-González, J.-M., Ortiz-Perez, S., & Rocha-de-Lossada, C. (2023). Surveying a Sample of the Spanish Ophthalmologic Community about Vaccination against Herpes Zoster. Vaccines, 11(5), 952. https://doi.org/10.3390/vaccines11050952