
Graves’ Disease after mRNA COVID-19 Vaccination, with the Presence of Autoimmune Antibodies Even One Year Later
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
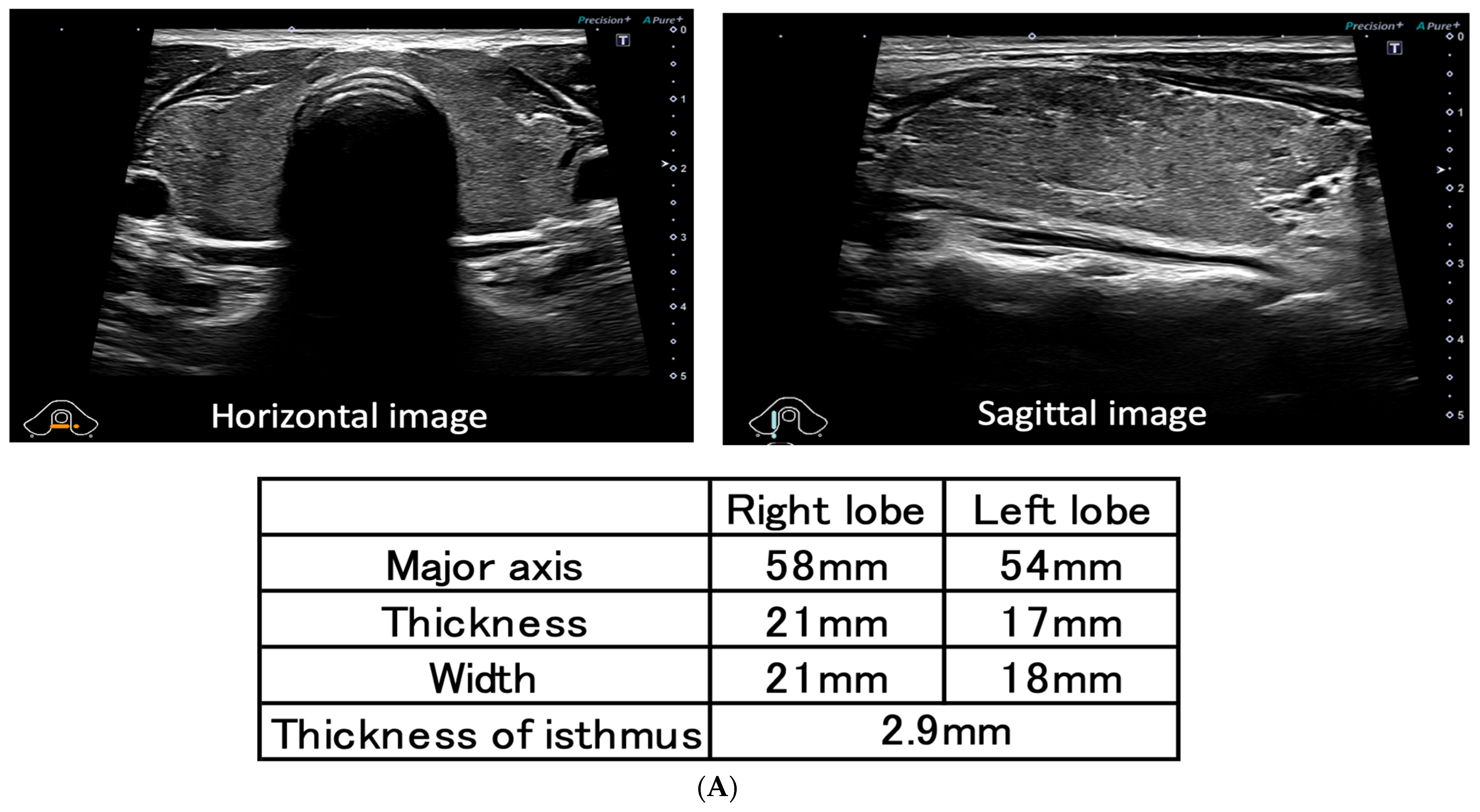
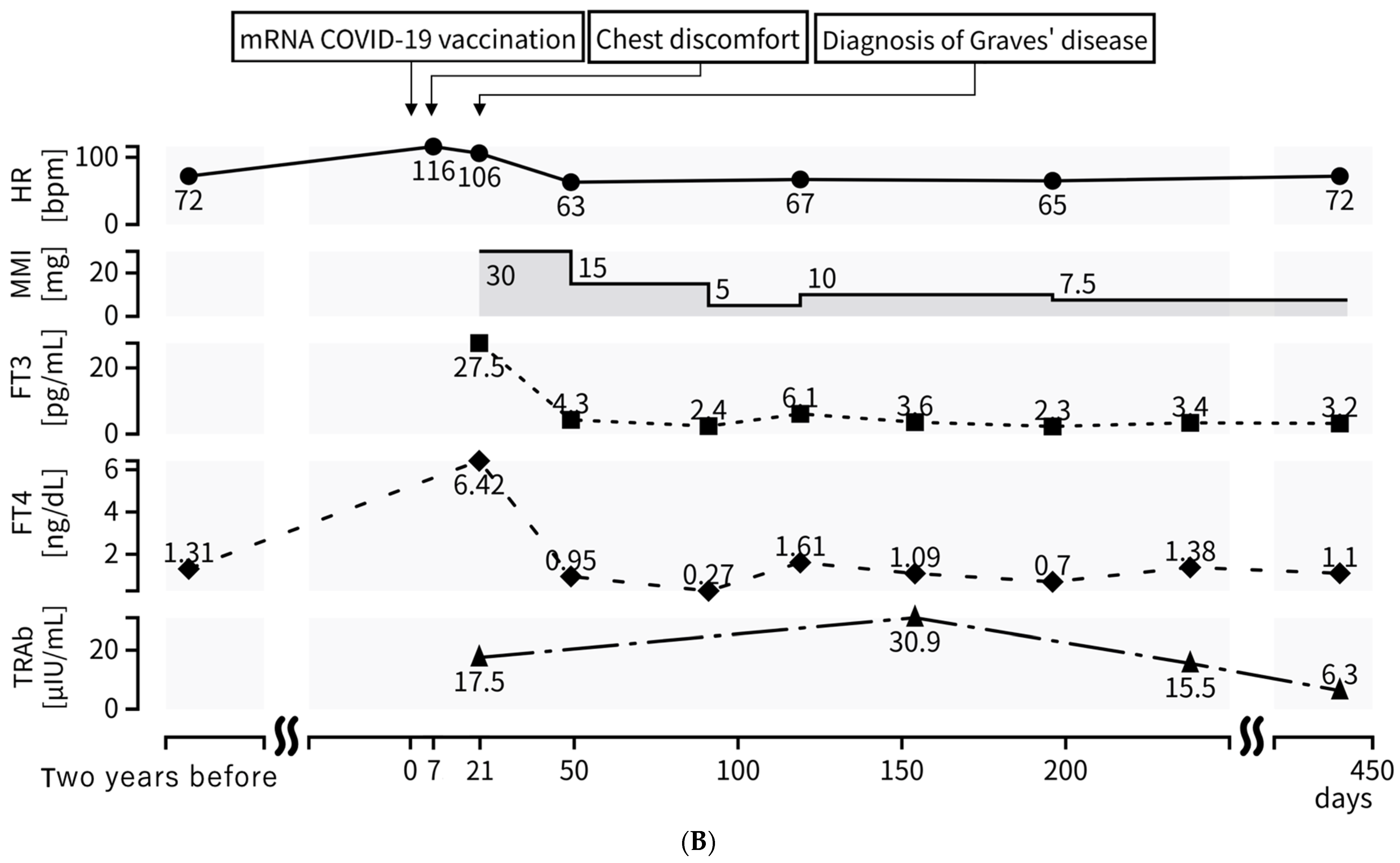
2. Case Presentation
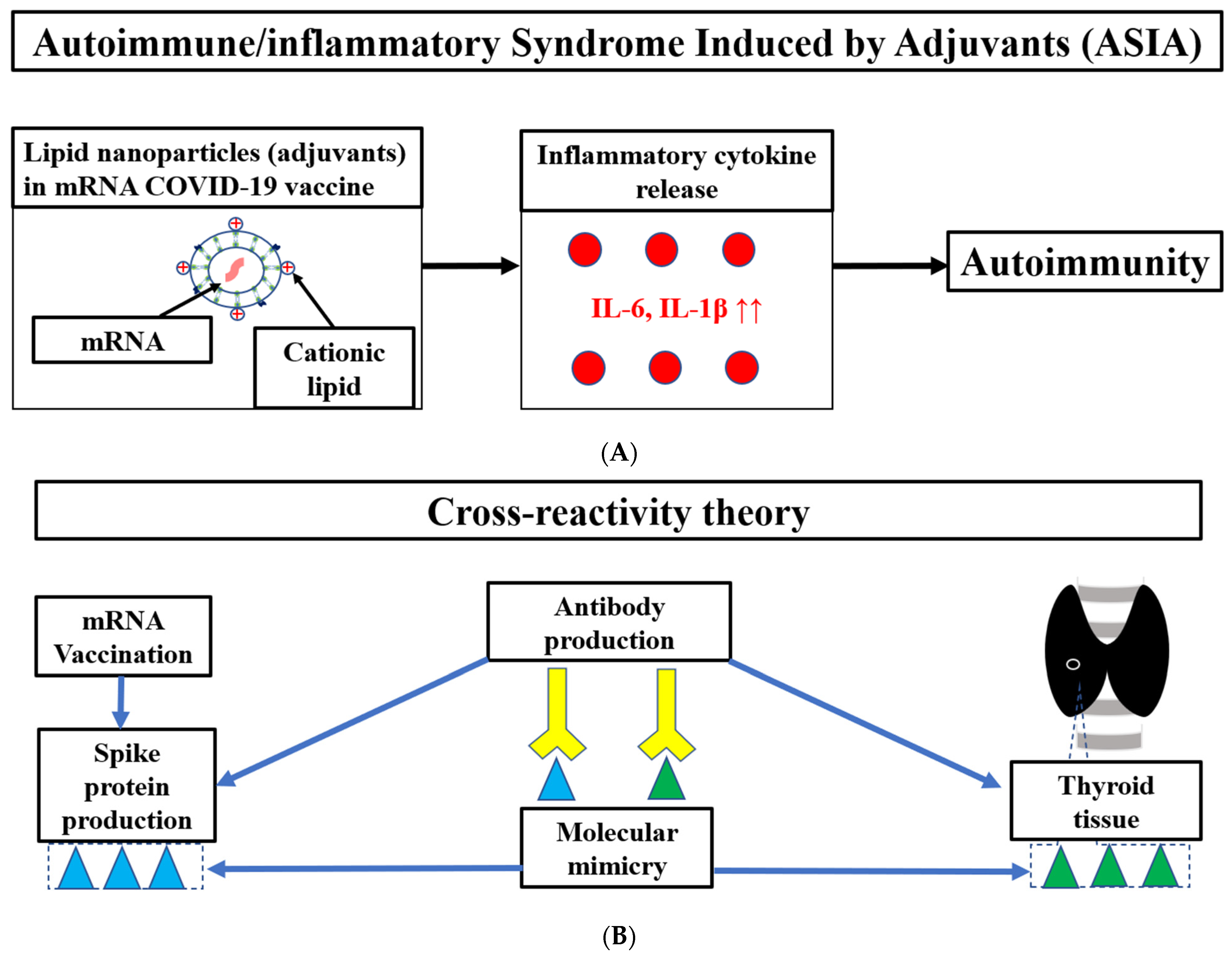
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| mRNA | messenger RNA |
| COVID-19 | coronavirus disease 2019 |
| ACS | acute coronary syndrome |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| ASIA | autoimmune/inflammatory syndrome induced by adjuvants |
| TSH | thyroid-stimulating hormone |
| TRAb | TSH receptor antibody |
| LNPs | lipid nanoparticles |
| FT3 | free triiodothyronine |
| FT4 | free thyroxine |
| ECG | Electrocardiogram |
| HR | heart rate |
| IL | Interleukin |
| MMI | Thiamazole |
| ACE2 | angiotensin-converting enzyme |
| TSBAb | TSH-stimulation blocking antibody |
| TSAb | thyroid stimulating antibody |
| TPO | thyroid peroxidase |
| ABCs | age-associated B cells |
| TLR | toll-like receptor |
| HLA | human leukocyte antigen |
References
- WHO. COVID-19 Dashboard. Geneva: World Health Organization, 2020. Available online: https://covid19.who.int/ (accessed on 24 April 2023).
- Rosenblum, H.G.; Gee, J.; Liu, R.; Marquez, P.L.; Zhang, B.; Strid, P.; Abara, W.E.; McNeil, M.M.; Myers, T.R.; Hause, A.M.; et al. Safety of mRNA vaccines administered during the initial 6 months of the US COVID-19 vaccination programme: An observational study of reports to the Vaccine Adverse Event Reporting System and v-safe. Lancet Infect. Dis. 2022, 22, 802–812. [Google Scholar] [CrossRef] [PubMed]
- Aye, Y.N.; Mai, A.S.; Zhang, A.; Lim, O.Z.H.; Lin, N.; Ng, C.H.; Chan, M.Y.; Yip, J.; Loh, P.H.; Chew, N.W.S. Acute myocardial infarction and myocarditis following COVID-19 vaccination. QJM 2023, 116, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Awaya, T.; Moroi, M.; Enomoto, Y.; Kunimasa, T.; Nakamura, M. What Should We Do after the COVID-19 Vaccination? Vaccine-Associated Diseases and Precautionary Measures against Adverse Reactions. Vaccines 2022, 10, 866. [Google Scholar] [CrossRef] [PubMed]
- Pujol, A.; Gómez, L.-A.; Gallegos, C.; Nicolau, J.; Sanchís, P.; González-Freire, M.; López-González, A.; Dotres, K.; Masmiquel, L. Thyroid as a target of adjuvant autoimmunity/inflammatory syndrome due to mRNA-based SARS-CoV2 vaccination: From Graves’ disease to silent thyroiditis. J. Endocrinol. Investig. 2021, 45, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Cohen Tervaert, J.W.; Martinez-Lavin, M.; Jara, L.J.; Halpert, G.; Watad, A.; Amital, H.; Shoenfeld, Y. Autoimmune/inflammatory syndrome induced by adjuvants (ASIA) in 2023. Autoimmun. Rev. 2023, 22, 103287. [Google Scholar] [CrossRef]
- Lui, D.T.W.; Lee, K.K.; Lee, C.H.; Lee, A.C.H.; Hung, I.F.N.; Tan, K.C.B. Development of Graves’ Disease After SARS-CoV-2 mRNA Vaccination: A Case Report and Literature Review. Front. Public Health 2021, 9, 778964. [Google Scholar] [CrossRef]
- Yamamoto, K.; Mashiba, T.; Takano, K.; Suzuki, T.; Kami, M.; Takita, M.; Hamaki, T. A Case of Exacerbation of Subclinical Hyperthyroidism after First Administration of BNT162b2 mRNA COVID-19 Vaccine. Vaccines 2021, 9, 1108. [Google Scholar] [CrossRef]
- Vojdani, A.; Vojdani, E.; Kharrazian, D. Reaction of Human Monoclonal Antibodies to SARS-CoV-2 Proteins with Tissue Antigens: Implications for Autoimmune Diseases. Front Immunol. 2021, 11, 617089. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, Z.; Wang, P.; Li, X.M.; Shuai, Z.W.; Ye, D.Q.; Pan, H.F. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 2022, 165, 386–401. [Google Scholar] [CrossRef]
- Galindo, D.E.B.; Bachiller, B.R.; Roza, L.G.; de Morales, J.M.G.R.; Lasheras, F.S.; Arnáiz, E.G.; Cobo, D.A.; Pomar, M.D.B.; Rodríguez, I.C. Increased incidence of Graves’ disease during the SARS-CoV2 pandemic. Clin. Endocrinol. 2022, 98, 730–737. [Google Scholar] [CrossRef]
- di Filippo, L.; Castellino, L.; Allora, A.; Frara, S.; Lanzi, R.; Perticone, F.; Valsecchi, F.; Vassallo, A.; Giubbini, R.; Rosen, C.J.; et al. Distinct Clinical Features of Post-COVID-19 Vaccination Early-onset Graves’ Disease. J. Clin. Endocrinol. Metab. 2022, 108, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Şendur, S.N.; Oğuz, S.H.; Ünlütürk, U. COVID-19 vaccination and thyroiditis. Best Pract. Res. Clin. Endocrinol. Metab. 2023. [Google Scholar] [CrossRef] [PubMed]
- Morita, S.; Takagi, T.; Inaba, H.; Furukawa, Y.; Kishimoto, S.; Uraki, S.; Shimo, N.; Takeshima, K.; Uraki, S.; Doi, K.; et al. Effect of SARS-CoV-2 BNT162b2 mRNA vaccine on thyroid autoimmunity: A twelve-month follow-up study. Front. Endocrinol. 2023, 14, 1058007. [Google Scholar] [CrossRef] [PubMed]
- Soriano, A.; Nesher, G.; Shoenfeld, Y. Predicting post-vaccination autoimmunity: Who might be at risk? Pharmacol. Res. 2015, 92, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Alameh, M.G.; Tombácz, I.; Bettini, E.; Lederer, K.; Sittplangkoon, C.; Wilmore, J.R.; Gaudette, B.T.; Soliman, O.Y.; Pine, M.; Hicks, P.; et al. Lipid nanoparticles enhance the efficacy of mRNA and protein subunit vaccines by inducing robust T follicular helper cell and humoral responses. Immunity 2021, 54, 2877–2892.e7. [Google Scholar] [CrossRef]
- Ndeupen, S.; Qin, Z.; Jacobsen, S.; Bouteau, A.; Estanbouli, H.; Igyártó, B.Z. The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. iScience 2021, 24, 103479. [Google Scholar] [CrossRef]
- Guidelines | Japan Thyroid Association. Available online: https://www.japanthyroid.jp/en/guidelines (accessed on 24 April 2023).
- Kamijo, K. Study on cutoff value setting for differential diagnosis between Graves’ disease and painless thyroiditis using the TRAb (Elecsys TRAb) measurement via the fully automated electrochemiluminescence immunoassay system. Endocr. J. 2010, 57, 895–902. [Google Scholar] [CrossRef]
- Takasu, N.; Matsushita, M. Changes of TSH-Stimulation Blocking Antibody (TSBAb) and Thyroid Stimulating Antibody (TSAb) Over 10 Years in 34 TSBAb-Positive Patients with Hypothyroidism and in 98 TSAb-Positive Graves’ Patients with Hyperthyroidism: Reevaluation of TSBAb and TSAb in TSH-Receptor-Antibody (TRAb)-Positive Patients. J. Thyroid. Res. 2012, 2012, 182176. [Google Scholar] [CrossRef]
- Takasu, N.; Noh, J.Y. Hashimoto’s thyroiditis: TGAb, TPOAb, TRAb and recovery from hypothyroidism. Expert Rev. Clin. Immunol. 2008, 4, 221–237. [Google Scholar] [CrossRef]
- Tun, N.N.Z.; Beckett, G.; Zammitt, N.N.; Strachan, M.W.J.; Seckl, J.R.; Gibb, F.W. Thyrotropin Receptor Antibody Levels at Diagnosis and After Thionamide Course Predict Graves’ Disease Relapse. Thyroid 2016, 26, 1004–1009. [Google Scholar] [CrossRef]
- Huang, Y.; Jin, B.; Huang, Y.; Dong, A. Consistency Between Thyrotropin Receptor Antibody (TRAb) and Thyroid-Stimulating Antibody (TSAb) Levels in Patients with Graves Disease. Lab. Med. 2022, 53, 412–416. [Google Scholar] [CrossRef]
- Ramos, S.G.; Rattis, B.; Ottaviani, G.; Celes, M.R.N.; Dias, E.P. ACE2 Down-Regulation May Act as a Transient Molecular Disease Causing RAAS Dysregulation and Tissue Damage in the Microcirculatory Environment Among COVID-19 Patients. Am. J. Pathol. 2021, 191, 1154–1164. [Google Scholar] [CrossRef]
- Robles, J.P.; Zamora, M.; Adan-Castro, E.; Siqueiros-Marquez, L.; de la Escalera, G.M.; Clapp, C. The spike protein of SARS-CoV-2 induces endothelial inflammation through integrin α5β1 and NF-κB signaling. J. Biol. Chem. 2022, 298, 101695. [Google Scholar] [CrossRef]
- Kimura, A.; Kishimoto, T. IL-6: Regulator of Treg/Th17 balance. Eur. J. Immunol. 2010, 40, 1830–1835. [Google Scholar] [CrossRef]
- Sachinidis, A.; Garyfallos, A. COVID-19 vaccination can occasionally trigger autoimmune phenomena, probably via inducing age-associated B cells. Int. J. Rheum. Dis. 2021, 25, 83–85. [Google Scholar] [CrossRef]
- Hao, Y.; O’Neill, P.; Naradikian, M.S.; Scholz, J.L.; Cancro, M.P. A B-cell subset uniquely responsive to innate stimuli accumulates in aged mice. Blood 2011, 118, 1294–1304. [Google Scholar] [CrossRef]
- Irrgang, P.; Gerling, J.; Kocher, K.; Lapuente, D.; Steininger, P.; Habenicht, K.; Wytopil, M.; Beileke, S.; Schäfer, S.; Zhong, J.; et al. Class switch toward noninflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Sci. Immunol. 2023, 8, eade2798. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Yajima, T.; Shimaoka, T.; Ogawa, S.; Saito, T.; Yamaoka, K.; Takeuchi, T.; Kubo, M. Synergistic effect of IgG4 antibody and CTLs causes tissue inflammation in IgG4-related disease. Int. Immunol. 2019, 32, 163–174. [Google Scholar] [CrossRef]
- Patel, A.H.; Amin, R.; Lalos, A.T. Acute Liver Injury and IgG4-related Autoimmune Pancreatitis following mRNA based COVID-19 vaccination. Hepatol. Forum 2022, 3, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Tasnim, S.; Al-Jobory, O.; Hallak, A.; Bharadwaj, T.; Patel, M. IgG4 related pleural disease: Recurrent pleural effusion after COVID-19 vaccination. Respirol. Case Rep. 2022, 10, e01026. [Google Scholar] [CrossRef] [PubMed]
- Masset, C.; Kervella, D.; Kandel-Aznar, C.; Fantou, A.; Blancho, G.; Hamidou, M. Relapse of IgG4-related nephritis following mRNA COVID-19 vaccine. Kidney Int. 2021, 100, 465–466. [Google Scholar] [CrossRef]
- Antonelli, A.; Ferrari, S.M.; Ragusa, F.; Elia, G.; Paparo, S.R.; Ruffilli, I.; Patrizio, A.; Giusti, C.; Gonnella, D.; Cristaudo, A.; et al. Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101387. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, F.; Awaya, T.; Ohira, M.; Enomoto, Y.; Moroi, M.; Nakamura, M. Graves’ Disease after mRNA COVID-19 Vaccination, with the Presence of Autoimmune Antibodies Even One Year Later. Vaccines 2023, 11, 934. https://doi.org/10.3390/vaccines11050934
Nakamura F, Awaya T, Ohira M, Enomoto Y, Moroi M, Nakamura M. Graves’ Disease after mRNA COVID-19 Vaccination, with the Presence of Autoimmune Antibodies Even One Year Later. Vaccines. 2023; 11(5):934. https://doi.org/10.3390/vaccines11050934
Chicago/Turabian StyleNakamura, Fuminori, Toru Awaya, Masahiro Ohira, Yoshinari Enomoto, Masao Moroi, and Masato Nakamura. 2023. "Graves’ Disease after mRNA COVID-19 Vaccination, with the Presence of Autoimmune Antibodies Even One Year Later" Vaccines 11, no. 5: 934. https://doi.org/10.3390/vaccines11050934
APA StyleNakamura, F., Awaya, T., Ohira, M., Enomoto, Y., Moroi, M., & Nakamura, M. (2023). Graves’ Disease after mRNA COVID-19 Vaccination, with the Presence of Autoimmune Antibodies Even One Year Later. Vaccines, 11(5), 934. https://doi.org/10.3390/vaccines11050934