
Occurrence and Risk Factors of Relapse Activity after Vaccination against COVID-19 in People with Multiple Sclerosis: 1-Year Follow-Up Results from a Nationwide Longitudinal Observational Study

 , , , ,
, , , , 

Abstract
:1. Introduction
2. Materials and Methods
Statistics
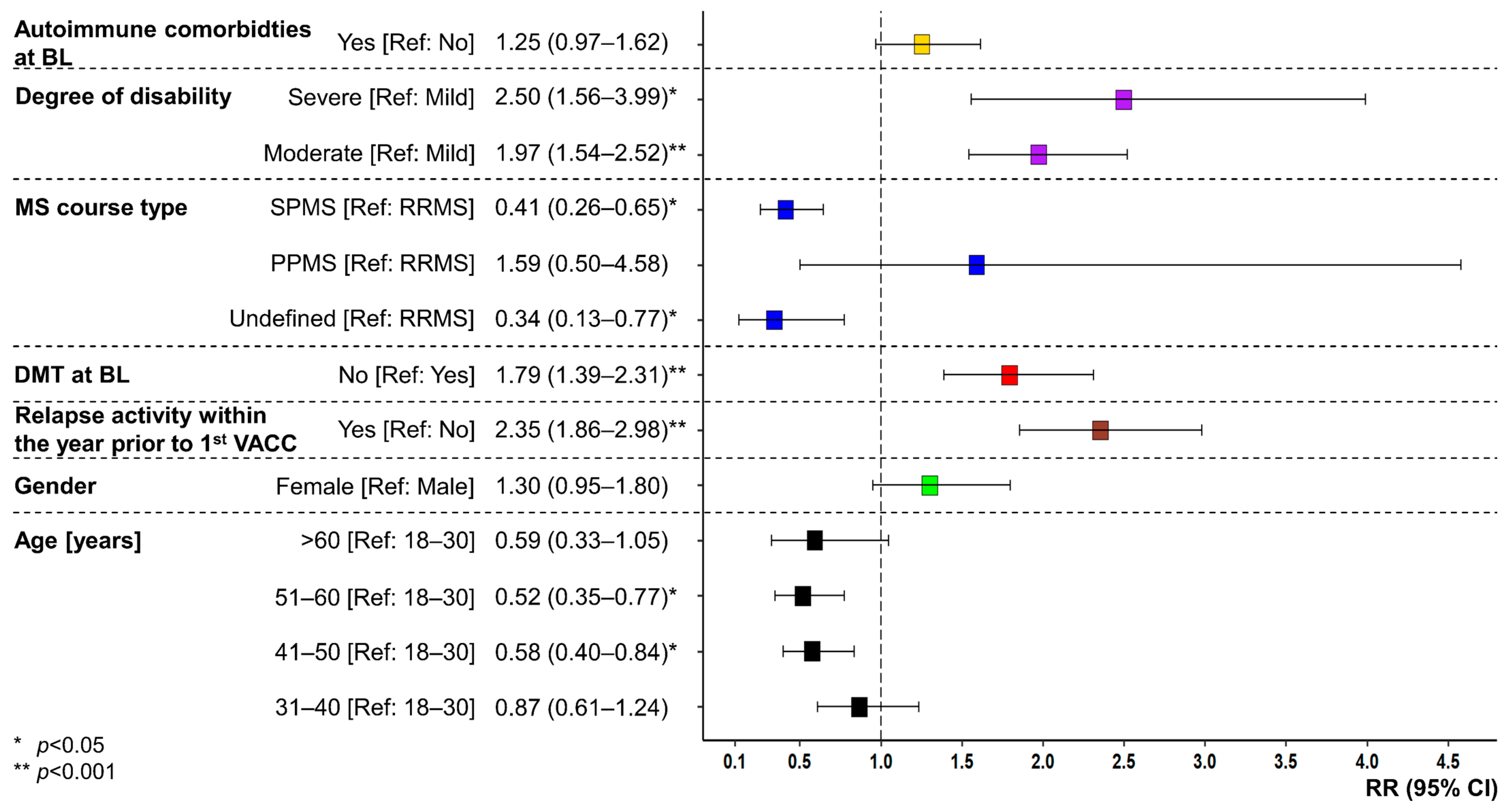
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Monschein, T.; Hartung, H.-P.; Zrzavy, T.; Barnett, M.; Boxberger, N.; Berger, T.; Chataway, J.; Bar-Or, A.; Rommer, P.S.; Zettl, U.K. Vaccination and Multiple Sclerosis in the Era of the COVID-19 Pandemic. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1033–1043. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 8 December 2023).
- Chaudhary, J.K.; Yadav, R.; Chaudhary, P.K.; Maurya, A.; Kant, N.; Rugaie, O.A.; Haokip, H.R.; Yadav, D.; Roshan, R.; Prasad, R.; et al. Insights into COVID-19 Vaccine Development Based on Immunogenic Structural Proteins of SARS-CoV-2, Host Immune Responses, and Herd Immunity. Cells 2021, 10, 2949. [Google Scholar] [CrossRef]
- Parums, D.V. Editorial: First Approval of the Protein-Based Adjuvanted Nuvaxovid (NVX-CoV2373) Novavax Vaccine for SARS-CoV-2 Could Increase Vaccine Uptake and Provide Immune Protection from Viral Variants. Med. Sci. Monit. 2022, 28, e936523. [Google Scholar] [CrossRef]
- Kelly, H.; Sokola, B.; Abboud, H. Safety and Efficacy of COVID-19 Vaccines in Multiple Sclerosis Patients. J. Neuroimmunol. 2021, 356, 577599. [Google Scholar] [CrossRef]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public. Health 2021, 9, 698111. [Google Scholar] [CrossRef]
- Novak, N.; Tordesillas, L.; Cabanillas, B. Adverse Rare Events to Vaccines for COVID-19: From Hypersensitivity Reactions to Thrombosis and Thrombocytopenia. Int. Rev. Immunol. 2022, 41, 438–447. [Google Scholar] [CrossRef]
- Lotan, I.; Wilf-Yarkoni, A.; Friedman, Y.; Stiebel-Kalish, H.; Steiner, I.; Hellmann, M.A. Safety of the BNT162b2 COVID-19 Vaccine in Multiple Sclerosis (MS): Early Experience from a Tertiary MS Center in Israel. Eur. J. Neurol. 2021, 28, 3742–3748. [Google Scholar] [CrossRef]
- Filippi, M.; Bar-Or, A.; Piehl, F.; Preziosa, P.; Solari, A.; Vukusic, S.; Rocca, M.A. Multiple Sclerosis. Nat. Rev. Dis. Primers 2018, 4, 43. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G. Multiple Sclerosis—A Review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef]
- MS International Federation (MSIF) Number of People with MS. Atlas of MS. Available online: https://www.atlasofms.org/map/global/epidemiology/number-of-people-with-ms (accessed on 8 December 2023).
- Harbo, H.F.; Gold, R.; Tintoré, M. Sex and Gender Issues in Multiple Sclerosis. Ther. Adv. Neurol. Disord. 2013, 6, 237–248. [Google Scholar] [CrossRef]
- Coyle, P.K. What Can We Learn from Sex Differences in MS? J. Pers. Med. 2021, 11, 1006. [Google Scholar] [CrossRef]
- Winkelmann, A.; Loebermann, M.; Reisinger, E.C.; Hartung, H.-P.; Zettl, U.K. Disease-Modifying Therapies and Infectious Risks in Multiple Sclerosis. Nat. Rev. Neurol. 2016, 12, 217–233. [Google Scholar] [CrossRef]
- Pawlitzki, M.; Zettl, U.K.; Ruck, T.; Rolfes, L.; Hartung, H.-P.; Meuth, S.G. Merits and Culprits of Immunotherapies for Neurological Diseases in Times of COVID-19. EBioMedicine 2020, 56, 102822. [Google Scholar] [CrossRef]
- Löbermann, M.; Boršo, D.; Hilgendorf, I.; Fritzsche, C.; Zettl, U.K.; Reisinger, E.C. Immunization in the Adult Immunocompromised Host. Autoimmun. Rev. 2012, 11, 212–218. [Google Scholar] [CrossRef]
- Mailand, M.T.; Frederiksen, J.L. Vaccines and Multiple Sclerosis: A Systematic Review. J. Neurol. 2017, 264, 1035–1050. [Google Scholar] [CrossRef]
- Zrzavy, T.; Kollaritsch, H.; Rommer, P.S.; Boxberger, N.; Loebermann, M.; Wimmer, I.; Winkelmann, A.; Zettl, U.K. Vaccination in Multiple Sclerosis: Friend or Foe? Front. Immunol. 2019, 10, 1883. [Google Scholar] [CrossRef]
- Witman Tsur, S.; Adrian Zaher, E.; Tsur, M.; Kania, K.; Kalinowska-Łyszczarz, A. Current Immunological and Clinical Perspective on Vaccinations in Multiple Sclerosis Patients: Are They Safe after All? Int. J. Mol. Sci. 2021, 22, 3859. [Google Scholar] [CrossRef]
- Langer-Gould, A.; Qian, L.; Tartof, S.Y.; Brara, S.M.; Jacobsen, S.J.; Beaber, B.E.; Sy, L.S.; Chao, C.; Hechter, R.; Tseng, H.F. Vaccines and the Risk of Multiple Sclerosis and Other Central Nervous System Demyelinating Diseases. JAMA Neurol. 2014, 71, 1506–1513. [Google Scholar] [CrossRef]
- Amaral, M.P.; Branco, L.M.; Strasser, A.; Dixit, V.M.; Bortoluci, K.R. Paradise Revealed III: Why so Many Ways to Die? Apoptosis, Necroptosis, Pyroptosis, and Beyond. Cell Death Differ. 2020, 27, 1740–1742. [Google Scholar] [CrossRef]
- Taniguchi, K.; Karin, M. NF-κB, Inflammation, Immunity and Cancer: Coming of Age. Nat. Rev. Immunol. 2018, 18, 309–324. [Google Scholar] [CrossRef]
- Frahm, N.; Fneish, F.; Ellenberger, D.; Haas, J.; Loebermann, M.; Parciak, T.; Peters, M.; Pöhlau, D.; Rodgers, J.; Röper, A.-L.; et al. SARS-CoV-2 Vaccination in Patients with Multiple Sclerosis in Germany and the United Kingdom: Gender-Specific Results from a Longitudinal Observational Study. Lancet Reg. Health Eur. 2022, 22, 100502. [Google Scholar] [CrossRef]
- Frahm, N.; Fneish, F.; Ellenberger, D.; Haas, J.; Löbermann, M.; Peters, M.; Pöhlau, D.; Röper, A.-L.; Schilling, S.; Stahmann, A.; et al. Frequency and Predictors of Relapses Following SARS-CoV-2 Vaccination in Patients with Multiple Sclerosis: Interim Results from a Longitudinal Observational Study. J. Clin. Med. 2023, 12, 3640. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of Multiple Sclerosis: 2017 Revisions of the McDonald Criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Koch, R. Institute—Ständige Impfkommission. Available online: https://www.rki.de/DE/Content/Kommissionen/STIKO/stiko_node.html (accessed on 8 December 2023).
- Learmonth, Y.C.; Motl, R.W.; Sandroff, B.M.; Pula, J.H.; Cadavid, D. Validation of Patient Determined Disease Steps (PDDS) Scale Scores in Persons with Multiple Sclerosis. BMC Neurol. 2013, 13, 37. [Google Scholar] [CrossRef]
- Fneish, F.; Ellenberger, D.; Frahm, N.; Stahmann, A.; Fortwengel, G.; Schaarschmidt, F. Application of Statistical Methods for Central Statistical Monitoring and Implementations on the German Multiple Sclerosis Registry. Ther. Innov. Regul. Sci. 2023, 57, 1217–1228. [Google Scholar] [CrossRef]
- Nahm, F.S. Nonparametric Statistical Tests for the Continuous Data: The Basic Concept and the Practical Use. Korean J. Anesthesiol. 2016, 69, 8–14. [Google Scholar] [CrossRef]
- Mishra, P.; Pandey, C.M.; Singh, U.; Keshri, A.; Sabaretnam, M. Selection of Appropriate Statistical Methods for Data Analysis. Ann. Card. Anaesth. 2019, 22, 297–301. [Google Scholar] [CrossRef]
- Paek, I. Conservativeness in Rejection of the Null Hypothesis When Using the Continuity Correction in the MH Chi-Square Test in DIF Applications. Appl. Psychol. Meas. 2010, 34, 539–548. [Google Scholar] [CrossRef]
- Crans, G.G.; Shuster, J.J. How Conservative Is Fisher’s Exact Test? A Quantitative Evaluation of the Two-Sample Comparative Binomial Trial. Stat. Med. 2008, 27, 3598–3611. [Google Scholar] [CrossRef]
- Ludbrook, J.; Dudley, H. Issues in Biomedical Statistics: Analysing 2 x 2 Tables of Frequencies. Aust. N. Z. J. Surg. 1994, 64, 780–787. [Google Scholar] [CrossRef]
- Prescott, R.J. Two-Tailed Significance Tests for 2 × 2 Contingency Tables: What Is the Alternative? Stat. Med. 2019, 38, 4264–4269. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical Notes for Clinical Researchers: Chi-Squared Test and Fisher’s Exact Test. Restor. Dent. Endod. 2017, 42, 152–155. [Google Scholar] [CrossRef]
- Au, W.Y.; Cheung, P.P.-H. Effectiveness of Heterologous and Homologous Covid-19 Vaccine Regimens: Living Systematic Review with Network Meta-Analysis. BMJ 2022, 377, e069989. [Google Scholar] [CrossRef]
- van Kessel, R.; Forman, R.; Milstein, R.; Mastylak, A.; Czabanowska, K.; Czypionka, T.; Durand-Zaleski, I.; Hirche, A.; Krysinska-Pisarek, M.; Maynou, L.; et al. Divergent COVID-19 Vaccine Policies: Policy Mapping of Ten European Countries. Vaccine 2023, 41, 2804–2810. [Google Scholar] [CrossRef]
- Koch, R. Institute—Impfungen A—Z—STIKO-Empfehlung Zur COVID-19-Impfung. Available online: https://www.rki.de/DE/Content/Infekt/Impfen/ImpfungenAZ/COVID-19/Impfempfehlung-Zusfassung.html (accessed on 8 December 2023).
- Wu, Q.; Dudley, M.Z.; Chen, X.; Bai, X.; Dong, K.; Zhuang, T.; Salmon, D.; Yu, H. Evaluation of the Safety Profile of COVID-19 Vaccines: A Rapid Review. BMC Med. 2021, 19, 173. [Google Scholar] [CrossRef]
- Achiron, A.; Dolev, M.; Menascu, S.; Zohar, D.-N.; Dreyer-Alster, S.; Miron, S.; Shirbint, E.; Magalashvili, D.; Flechter, S.; Givon, U.; et al. COVID-19 Vaccination in Patients with Multiple Sclerosis: What We Have Learnt by February 2021. Mult Scler 2021, 27, 864–870. [Google Scholar] [CrossRef]
- Lotan, I.; Romanow, G.; Levy, M. Patient-Reported Safety and Tolerability of the COVID-19 Vaccines in Persons with Rare Neuroimmunological Diseases. Mult. Scler. Relat. Disord. 2021, 55, 103189. [Google Scholar] [CrossRef]
- Dreyer-Alster, S.; Menascu, S.; Mandel, M.; Shirbint, E.; Magalashvili, D.; Dolev, M.; Flechter, S.; Givon, U.; Guber, D.; Stern, Y.; et al. COVID-19 Vaccination in Patients with Multiple Sclerosis: Safety and Humoral Efficacy of the Third Booster Dose. J. Neurol. Sci. 2022, 434, 120155. [Google Scholar] [CrossRef]
- Bae, S.; Lee, Y.W.; Lim, S.Y.; Lee, J.H.; Lim, J.S.; Lee, S.; Park, S.; Kim, S.K.; Lim, Y.J.; Kim, E.O.; et al. Adverse Reactions Following the First Dose of ChAdOx1 nCoV-19 Vaccine and BNT162b2 Vaccine for Healthcare Workers in South Korea. J. Korean Med. Sci. 2021, 36, e115. [Google Scholar] [CrossRef]
- Czarnowska, A.; Tarasiuk, J.; Zajkowska, O.; Wnuk, M.; Marona, M.; Nowak, K.; Słowik, A.; Jamroz-Wiśniewska, A.; Rejdak, K.; Lech, B.; et al. Safety of Vaccines against SARS-CoV-2 among Polish Patients with Multiple Sclerosis Treated with Disease-Modifying Therapies. Vaccines 2022, 10, 763. [Google Scholar] [CrossRef]
- Kong, L.; Wang, X.; Chen, H.; Shi, Z.; Lang, Y.; Zhang, Y.; Zhou, H. Relapses after SARS-CoV-2 Vaccination in Patients with Neuromyelitis Optica Spectrum Disorder and Multiple Sclerosis. Mult. Scler. Relat. Disord. 2022, 68, 104167. [Google Scholar] [CrossRef] [PubMed]
- Doubrovinskaia, S.; Mooshage, C.M.; Seliger, C.; Lorenz, H.; Nagel, S.; Lehnert, P.; Purrucker, J.; Wildemann, B.; Bendszus, M.; Wick, W.; et al. Neurological Autoimmune Diseases Following Vaccinations against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): A Follow-up Study. Eur. J. Neurol. 2023, 30, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Ciampi, E.; Uribe-San-Martin, R.; Soler, B.; García, L.; Guzman, J.; Pelayo, C.; Jürgensen, L.; Guzman, I.; Vera, F.; Galleguillos, L.; et al. Safety and Humoral Response Rate of Inactivated and mRNA Vaccines against SARS-CoV-2 in Patients with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2022, 59, 103690. [Google Scholar] [CrossRef] [PubMed]
- Ismail, I.I.; Salama, S. A Systematic Review of Cases of CNS Demyelination Following COVID-19 Vaccination. J. Neuroimmunol. 2022, 362, 577765. [Google Scholar] [CrossRef] [PubMed]
- Kataria, S.; Rogers, S.; Bilal, U.; Baktashi, H.; Singh, R. Multiple Sclerosis Relapse Following COVID-19 Vaccination: A Case Report and Literature Review. Cureus 2022, 14, e21374. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, M.; El-Hajj Sleiman, J.; Beauchemin, P.; Rangachari, M. SARS-CoV-2 and Multiple Sclerosis: Potential for Disease Exacerbation. Front. Immunol. 2022, 13, 871276. [Google Scholar] [CrossRef]
- Finsterer, J. SARS-CoV-2 Triggered Relapse of Multiple Sclerosis. Clin. Neurol. Neurosurg. 2022, 215, 107210. [Google Scholar] [CrossRef]
- Satheesh, N.J.; Salloum-Asfar, S.; Abdulla, S.A. The Potential Role of COVID-19 in the Pathogenesis of Multiple Sclerosis-A Preliminary Report. Viruses 2021, 13, 2091. [Google Scholar] [CrossRef]
- Zeydan, B.; Kantarci, O.H. Impact of Age on Multiple Sclerosis Disease Activity and Progression. Curr. Neurol. Neurosci. Rep. 2020, 20, 24. [Google Scholar] [CrossRef]
- Alonso, R.; Chertcoff, A.; Leguizamón, F.D.V.; Galleguillos Goiry, L.; Eizaguirre, M.B.; Rodríguez, R.; Sosa, M.; Carballido, S.; Cruchet, V.; de Jong-Martis, A.; et al. Evaluation of Short-Term Safety of COVID-19 Vaccines in Patients with Multiple Sclerosis from Latin America. Mult. Scler. J. Exp. Transl. Clin. 2021, 7, 20552173211061543. [Google Scholar] [CrossRef]
- Maniscalco, G.T.; Scavone, C.; Mascolo, A.; Manzo, V.; Prestipino, E.; Guglielmi, G.; Aiezza, M.L.; Cozzolino, S.; Bracco, A.; Moreggia, O.; et al. The Safety Profile of COVID-19 Vaccines in Patients Diagnosed with Multiple Sclerosis: A Retrospective Observational Study. J. Clin. Med. 2022, 11, 6855. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Rosso, M.; Santoro, J.D. Wilhelm Uhthoff and Uhthoff’s Phenomenon. Mult. Scler. 2020, 26, 1790–1796. [Google Scholar] [CrossRef] [PubMed]
- Elser, H.C.; Koch-Henriksen, N.; Magyari, M. Seasonal Patterns of Relapse and Disability in Danish MS Patients: A Population-Based Cohort Study. Mult. Scler. Relat. Disord. 2021, 49, 102739. [Google Scholar] [CrossRef] [PubMed]
- Harding, K.; Tilling, K.; MacIver, C.; Willis, M.; Joseph, F.; Ingram, G.; Hirst, C.; Wardle, M.; Pickersgill, T.; Ben-Shlomo, Y.; et al. Seasonal Variation in Multiple Sclerosis Relapse. J. Neurol. 2017, 264, 1059–1067. [Google Scholar] [CrossRef]
- Cabreira, V.; Abreu, P.; Soares-dos-Reis, R.; Guimarães, J.; Sá, M.J. Multiple Sclerosis, Disease-Modifying Therapies and COVID-19: A Systematic Review on Immune Response and Vaccination Recommendations. Vaccines 2021, 9, 773. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Total (N = 2466) | PV Relapse (N = 341) | No PV Relapse (N = 2125) | p | |
|---|---|---|---|---|
| Gender, N (%) | 0.001 Fi | |||
| Female | 1939 (78.6) | 294 (86.2) | 1645 (77.4) | |
| Male | 521 (21.1) | 47 (13.8) | 474 (22.3) | |
| Divers | 6 (0.2) | 0 (0.0) | 6 (0.3) | |
| Age [years] at BL, median (Q25, Q75) * | 46.9 (37.8, 54.8) | 41.4 (34.1, 51.4) | 47.8 (38.6, 55.2) | <0.001 U |
| Age groups [years], N (%) | <0.001 Chi | |||
| 18–30 | 226 (9.2) | 44 (13.0) | 182 (8.6) | |
| 31–40 | 615 (25.0) | 120 (35.5) | 495 (23.4) | |
| 41–50 | 691 (28.1) | 88 (26.0) | 603 (28.5) | |
| 51–60 | 693 (28.2) | 63 (18.6) | 630 (29.7) | |
| >60 | 232 (9.4) | 23 (6.8) | 209 (9.9) | |
| MS disease course at BL, N (%) | <0.001 Chi | |||
| RRMS | 1827 (74.1) | 285 (83.6) | 1542 (72.6) | |
| SPMS | 434 (17.6) | 33 (9.7) | 401 (18.9) | |
| PPMS | 102 (4.1) | 12 (3.5) | 90 (4.2) | |
| Undefined | 103 (4.2) | 11 (3.2) | 92 (4.3) | |
| Disability level (PDDS) at FU3, N (%) * | 0.025 Chi | |||
| Mild (0–1) | 1248 (52.3) | 153 (47.7) | 1095 (53.1) | |
| Moderate (2–4) | 829 (34.8) | 133 (41.4) | 696 (33.7) | |
| Severe (≥5) | 307 (12.9) | 35 (10.9) | 272 (13.2) | |
| Coincident autoimmune diseases at BL, N (%) | 530 (21.5) | 95 (27.9) | 435 (20.5) | 0.003 Chi |
| DMT at BL, N (%) | 1806 (73.2) | 225 (66.0) | 1581 (74.4) | 0.001 Chi |
| IFNβ/GLAT | 535 (21.7) | 59 (17.3) | 476 (22.4) | 0.090 Fi |
| CLAD/DMF/TER | 507 (20.6) | 77 (22.6) | 430 (20.2) | |
| S1P RM | 306 (12.4) | 28 (8.2) | 278 (13.1) | |
| anti-CD20 MAB | 283 (11.5) | 42 (12.3) | 241 (11.3) | |
| Natalizumab | 102 (4.1) | 10 (2.9) | 92 (4.3) | |
| Other | 65 (2.6) | 9 (2.6) | 56 (2.6) | |
| Unknown DMT | 8 (0.3) | 0 (0.0) | 8 (0.4) | |
| Relapse within the year prior to 1st VACC, N (%) * | 362 (20.0) | 91 (34.7) | 271 (17.5) | <0.001 Chi |
| Relapse within 6 months prior to 1st VACC, N (%) * | 197 (10.9) | 57 (21.8) | 140 (9.0) | <0.001 Chi |
| Relapse within 3 months prior to 1st VACC, N (%) * | 87 (4.8) | 29 (11.1) | 58 (3.7) | <0.001 Chi |
| Time from last relapse (before 1st VACC) to 1st VACC [years], median (Q25, Q75) | 3.2 (1.3, 6.9) | 1.85 (0.6, 4.5) | 3.5 (1.5, 7.2) | <0.001 U |
| Total (N = 2466) | PV relapse (N = 341) | No PV relapse (N = 2125) | p | |
|---|---|---|---|---|
| 1st VACC, N (%) * | 0.675 Fi | |||
| Ad26.COV2.S | 26 (1.1) | 6 (1.8) | 20 (0.9) | |
| AZD1222 | 265 (10.8) | 38 (11.1) | 227 (10.7) | |
| Elasomeran | 241 (9.8) | 33 (9.7) | 208 (9.8) | |
| NVX-CoV2373 | 3 (0.1) | 0 (0.0) | 3 (0.1) | |
| Tozinameran | 1926 (78.3) | 264 (77.4) | 1662 (78.4) | |
| 2nd VACC, N (%) * | 0.359 Fi | |||
| Ad26.COV2.S | 1 (<0.1) | 0 (0.0) | 1 (<0.1) | |
| AZD1222 | 77 (3.2) | 5 (1.5) | 72 (3.5) | |
| Elasomeran | 284 (11.9) | 41 (12.5) | 243 (11.8) | |
| NVX-CoV2373 | 1 (<0.1) | 0 (0.0) | 1 (<0.1) | |
| Tozinameran | 2024 (84.8) | 283 (86.0) | 1741 (84.6) | |
| 1st Booster VACC, N (%) * | 0.610 Fi | |||
| Ad26.COV2.S | 5 (0.2) | 1 (0.3) | 4 (0.2) | |
| AZD1222 | 7 (0.3) | 1 (0.3) | 6 (0.3) | |
| Elasomeran | 728 (33.2) | 92 (32.2) | 636 (33.3) | |
| NVX-CoV2373 | 1 (<0.1) | 1 (0.3) | 3 (0.2) | |
| Tozinameran | 1453 (66.2) | 191 (66.8) | 1262 (66.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fneish, F.; Frahm, N.; Peters, M.; Ellenberger, D.; Haas, J.; Löbermann, M.; Pöhlau, D.; Röper, A.-L.; Schilling, S.; Stahmann, A.; et al. Occurrence and Risk Factors of Relapse Activity after Vaccination against COVID-19 in People with Multiple Sclerosis: 1-Year Follow-Up Results from a Nationwide Longitudinal Observational Study. Vaccines 2023, 11, 1859. https://doi.org/10.3390/vaccines11121859
Fneish F, Frahm N, Peters M, Ellenberger D, Haas J, Löbermann M, Pöhlau D, Röper A-L, Schilling S, Stahmann A, et al. Occurrence and Risk Factors of Relapse Activity after Vaccination against COVID-19 in People with Multiple Sclerosis: 1-Year Follow-Up Results from a Nationwide Longitudinal Observational Study. Vaccines. 2023; 11(12):1859. https://doi.org/10.3390/vaccines11121859
Chicago/Turabian StyleFneish, Firas, Niklas Frahm, Melanie Peters, David Ellenberger, Judith Haas, Micha Löbermann, Dieter Pöhlau, Anna-Lena Röper, Sarah Schilling, Alexander Stahmann, and et al. 2023. "Occurrence and Risk Factors of Relapse Activity after Vaccination against COVID-19 in People with Multiple Sclerosis: 1-Year Follow-Up Results from a Nationwide Longitudinal Observational Study" Vaccines 11, no. 12: 1859. https://doi.org/10.3390/vaccines11121859
APA StyleFneish, F., Frahm, N., Peters, M., Ellenberger, D., Haas, J., Löbermann, M., Pöhlau, D., Röper, A.-L., Schilling, S., Stahmann, A., Temmes, H., Paul, F., & Zettl, U. K. (2023). Occurrence and Risk Factors of Relapse Activity after Vaccination against COVID-19 in People with Multiple Sclerosis: 1-Year Follow-Up Results from a Nationwide Longitudinal Observational Study. Vaccines, 11(12), 1859. https://doi.org/10.3390/vaccines11121859