


Continuing Medical Education Improves Physician Communication Skills and Increases Likelihood of Pediatric Vaccination: Findings from the Pediatric Influenza Vaccination Optimization Trial (PIVOT)—II

 ,
,
Abstract
1. Introduction
2. Materials and Methods
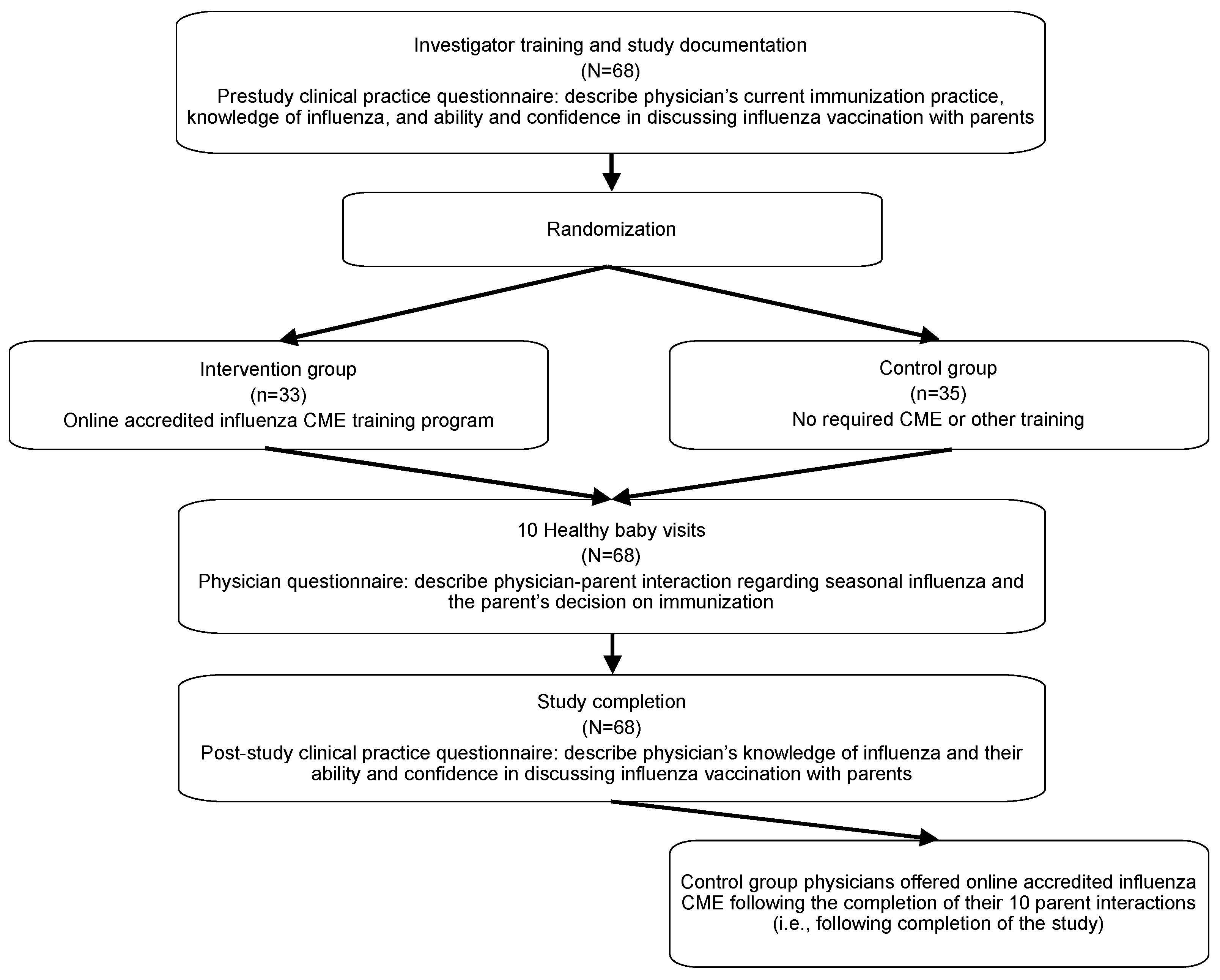
2.1. Study Design and Population
2.2. Study Intervention: IMB Model-Based CME
2.3. Study Procedures
2.4. Statistical Methods
3. Results
3.1. Baseline Demographics and Immunization Practices
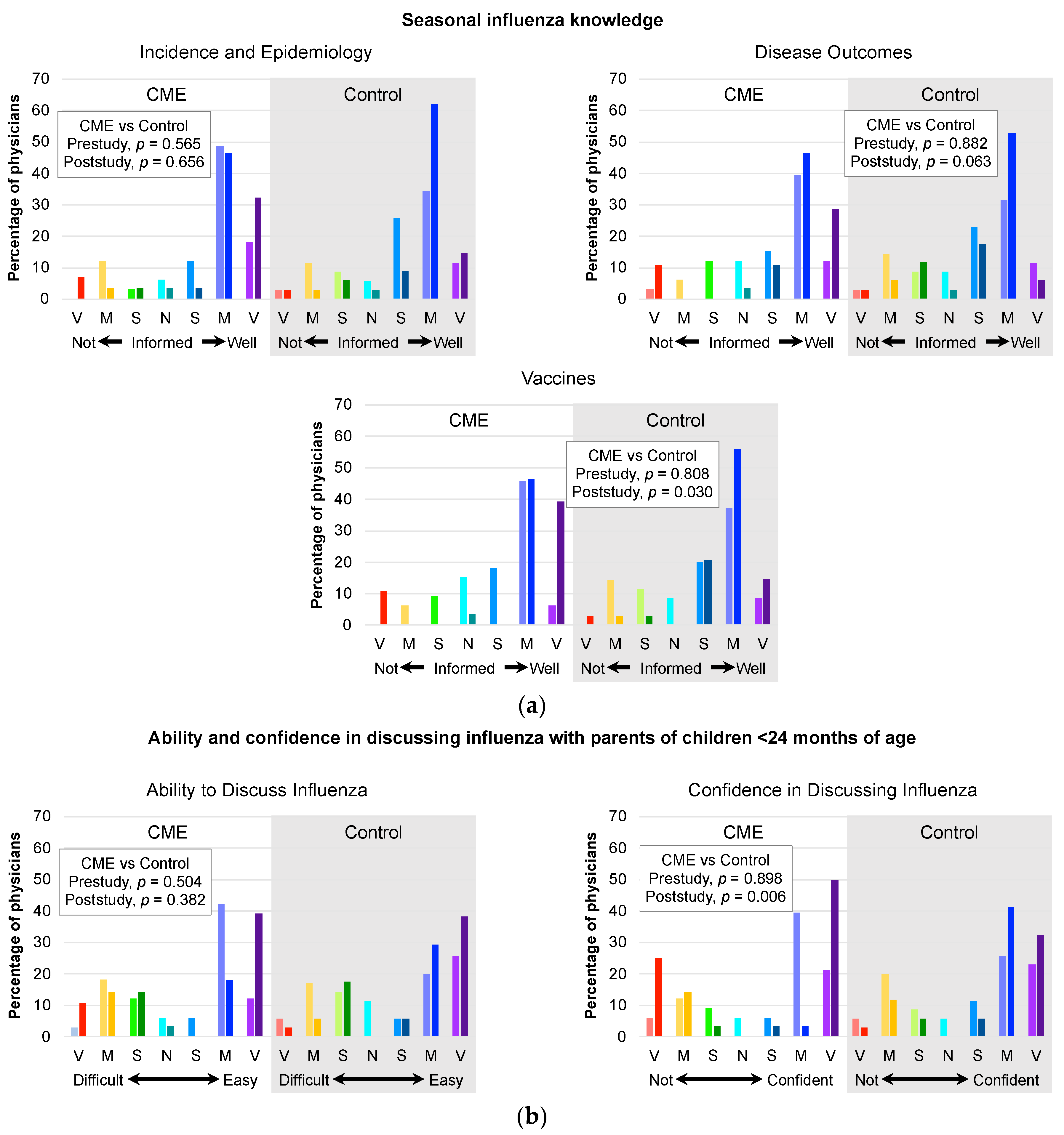
3.2. Influenza Knowledge and Ability and Confidence in Influenza Discussions
3.3. Healthy Baby Visit Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nair, H.; Brooks, W.A.; Katz, M.; Roca, A.; Berkley, J.A.; Madhi, S.A.; Simmerman, J.M.; Gordon, A.; Sato, M.; Howie, S.; et al. Global burden of respiratory infections due to seasonal influenza in young children: A systematic review and meta-analysis. Lancet 2011, 378, 1917–1930. [Google Scholar] [CrossRef] [PubMed]
- United Nations Department of Economic and Social Affairs. World Population Prospects. 2017. Available online: https://esa.un.org/unpd/wpp/ (accessed on 28 August 2017).
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef] [PubMed]
- Lafond, K.E.; Nair, H.; Rasooly, M.H.; Valente, F.; Booy, R.; Rahman, M.; Kitsutani, P.; Yu, H.; Guzman, G.; Coulibaly, D.; et al. Global Role and Burden of Influenza in Pediatric Respiratory Hospitalizations, 1982–2012: A Systematic Analysis. PLoS Med. 2016, 13, e1001977. [Google Scholar] [CrossRef] [PubMed]
- Poehling, K.A.; Edwards, K.M.; Griffin, M.R.; Szilagyi, P.G.; Staat, M.A.; Iwane, M.K.; Snively, B.M.; Suerken, C.K.; Hall, C.B.; Weinberg, G.A.; et al. The Burden of Influenza in Young Children, 2004–2009. Pediatrics 2013, 131, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. 2016/17 Seasonal Influenza Vaccine Coverage in Canada; Public Health Agency of Canada: Ottawa, ON, Canada, 2018.
- Public Health Agency of Canada. Canadian Immunization Guide Chapter on Influenza and Statement on Seasonal Influenza Vaccine for 2017–2018. Available online: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-statement-seasonal-influenza-vaccine-2017-2018.html (accessed on 19 April 2022).
- WHO. Influenza (Seasonal); WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/en/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 19 April 2022).
- Australian Government Department of Health. 2019 Influenza Vaccines. Available online: https://beta.health.gov.au/news-and-events/media-releases/2019-influenza-vaccines (accessed on 19 April 2022).
- Grohskopf, L.A.; Sokolow, L.Z.; Broder, K.R.; Walter, E.B.; Fry, A.M.; Jernigan, D.B. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2018–2019 Influenza Season. MMWR. Recomm. Rep. 2018, 67, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Joint Committee on Vaccination and Immunisation. Advice on Influenza Vaccines for 2019/20. Available online: https://www.gov.uk/government/groups/joint-committee-on-vaccination-and-immunisation#influenza-vaccines-jcvi-advice (accessed on 19 April 2022).
- Campitelli, M.A.; Inoue, M.; Calzavara, A.J.; Kwong, J.C.; Guttmann, A. Low Rates of Influenza Immunization in Young Children Under Ontario’s Universal Influenza Immunization Program. Pediatrics 2012, 129, e1421–e1430. [Google Scholar] [CrossRef] [PubMed]
- Flood, E.M.; Rousculp, M.D.; Ryan, K.J.; Beusterien, K.M.; Divino, V.M.; Toback, S.L.; Sasané, M.; Block, S.L.; Hall, M.C.; Mahadevia, P.J. ‘Parents’ decision-making regarding vaccinating their children against influenza: A web-based survey. Clin. Ther. 2010, 32, 1448–1467. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, S.R.; Daum, R.S. Physician Knowledge and Perspectives Regarding Influenza and Influenza Vaccination. Hum. Vaccines 2005, 1, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.E.; Webster, R.K.; Weinman, J.; Amlôt, R.; Yiend, J.; Rubin, G.J. Psychological factors associated with uptake of the childhood influenza vaccine and perception of post-vaccination side-effects: A cross-sectional survey in England. Vaccine 2017, 35, 1936–1945. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Bloom, B.S. Effects of continuing medical education on improving physician clinical care and patient health: A review of systematic reviews. Int. J. Technol. Assess. Health Care 2005, 21, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.; Davis, M.E.; Jadad, A.; Perrier, L.; Rath, D.; Ryan, D.; Sibbald, G.; Straus, S.; Rappolt, S.; Wowk, M.; et al. The case for knowledge translation: Shortening the journey from evidence to effect. BMJ 2003, 327, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Grimshaw, J.M.; Eccles, M.P.; Lavis, J.N.; Hill, S.J.; Squires, J.E. Knowledge translation of research findings. Implement. Sci. 2012, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Sohn, W.; Ismail, A.I.; Tellez, M. Efficacy of Educational Interventions Targeting Primary Care Providers’ Practice Behaviors: An Overview of Published Systematic Reviews. J. Public Health Dent. 2004, 64, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Fisher, W.A.; Fisher, J.D.; Shuper, P.A. Social psychology and the fight against AIDS: An Information-Motivation-Behavioral Skills model for the prediction and promotion of health behavior change. In Advances in Experimental Social Psychology; Olson, J.M., Zanna, M.P., Eds.; Elsevier: Waltham, MA, USA, 2014; Volume 50, pp. 105–194. [Google Scholar]
- Rourke, L.; Godwin, M.; Rourke, J.; Pearce, S.; Bean, J. The Rourke Baby Record Infant/Child Maintenance Guide: Do doctors use it, do they find it useful, and does using it improve their well-baby visit records? BMC Fam. Pract. 2009, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Riverin, B.; Li, P.; Rourke, L.; Leduc, D.; Rourke, J. Rourke Baby Record 2014: Evidence-based tool for the health of infants and children from birth to age 5. Can. Fam. Physician 2015, 61, 949–955. [Google Scholar] [PubMed]
- Elflein, J. Influenza Vaccination Rate among Canadian Children in 2015–2016, by Age. Available online: https://www.statista.com/statistics/978358/children-with-influenza-vaccinations-canada/ (accessed on 17 January 2022).
- Vesikari, T.; Knuf, M.; Wutzler, P.; Karvonen, A.; Kieninger-Baum, D.; Schmitt, H.-J.; Baehner, F.; Borkowski, A.; Tsai, T.F.; Clemens, R. Oil-in-Water Emulsion Adjuvant with Influenza Vaccine in Young Children. N. Engl. J. Med. 2011, 365, 1406–1416. [Google Scholar] [CrossRef] [PubMed]
- Vesikari, T.; Kirstein, J.; Go, G.D.; Leav, B.; Ruzycky, M.E.; Isakov, L.; de Bruijn, M.; Oberye, J.; Heijnen, E. Efficacy, immunogenicity, and safety evaluation of an MF59-adjuvanted quadrivalent influenza virus vaccine compared with non-adjuvanted influenza vaccine in children: A multicentre, randomised controlled, observer-blinded, phase 3 trial. Lancet Respir. Med. 2018, 6, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Albarracín, D.; Gillette, J.C.; Earl, A.N.; Glasman, L.R.; Durantini, M.R.; Ho, M.-H. A Test of Major Assumptions About Behavior Change: A Comprehensive Look at the Effects of Passive and Active HIV-Prevention Interventions Since the Beginning of the Epidemic. Psychol. Bull. 2005, 131, 856–897. [Google Scholar] [CrossRef] [PubMed]
- Fisher, W.A.; Fisher, J.D. The Information-Motivation-Behavioral Skills Model: A general social psychological approach to understanding and promoting health behaviour. In Social Psychological Foundations of Health and Illness; Suls, J., Wallston, K., Eds.; Blackwell: London, UK, 2003; pp. 82–106. [Google Scholar]



{kind=link}
{kind=link}
| Characteristic | CME Intervention | Control (No CME) | Total | p Value 1 |
|---|---|---|---|---|
| (n = 33) | (n = 35) | (n = 68) | ||
| Female sex, n (%) | 16 (48.5) | 21 (60.0) | 37 (54.4) | 0.465 |
| Therapeutic specialty, n (%) | ||||
| Family medicine with pediatric focus | 0 (0) | 1 (2.9) | 1 (1.5) | 0.222 |
| Family medicine | 31 (93.9) | 28 (80.0) | 59 (86.8) | |
| General practice | 1 (3.0) | 5 (14.3) | 6 (8.8 | |
| Type of practice, n (%) | ||||
| Solo | 11 (33.3) | 14 (40.0) | 25 (36.8) | 0.621 |
| Group | 22 (66.7) | 21 (60.0) | 43 (63.2) | |
| Years in practice | ||||
| Mean ± SD | 18.0 ± 13.2 | 15.6 ± 10.3 | 16.8 ± 11.8 | 0.654 |
| Median (range) | 15.0 (1–47) | 13.0 (2–40) | 13.0 (1–47) | |
| Days per week in active clinical practice | ||||
| Mean ± SD | 5.0 ± 0.8 | 4.9 ± 1.1 | 4.9 ± 1.0 | 0.815 |
| Median (range) | 5.0 (3-6) | 5.0 (2–6) | 5.0 (2–6) | |
| Number of patients seen in practice | ||||
| Mean ± SD | 1769 ± 850 | 1856 ± 824 | 1814 ± 831 | 0.499 |
| Median (range) | 1500 (200–4000) | 1700 (200–4009) | 1600 (200–4009) | |
| Percentage of infants 6 through 23 months seen for healthy baby visits per month | ||||
| Mean ± SD | 14.2 ± 20.6 | 17.2 ± 21.3 | 15.8 ± 20.8 | 0.714 |
| Median (range) | 10.0 (1–90) | 10.0 (1–80) | 10.0 (1–90) | |
| Approximate percentage of patients 6 through 11 months of age | ||||
| Mean ± SD | 6.4 ± 6.5 | 5.7 ± 5.9 | 6.0 ± 6.2 | 0.707 |
| Median (range) | 5.0 (1–20) | 5.0 (1–20) | 5.0 (1–20) | |
| Approximate percentage of patients 12 through 23 months of age | ||||
| Mean ± SD | 6.8 ± 5.9 | 6.3 ± 6.0 | 6.5 ± 5.9 | 0.506 |
| Median (range) | 5.0 (1–20) | 5.0 (1–20) | 5.0 (1–20) | |
| Socioeconomic status of physician practice region | ||||
| Low, n (%) | 2 (6.1) | 2 (5.7) | 4 (5.9) | 0.997 |
| Moderate, n (%) | 12 (36.4) | 13 (37.1) | 25 (36.8) | |
| High, n (%) | 19 (57.6) | 20 (57.1) | 39 (57.4) | |
| Percentage of children aged 6 through 23 months vaccinated in practice with routine pediatric vaccines | ||||
| Publicly funded vaccines per month, mean ± SD | 67.9 ± 39.6 | 67.1 ± 40.7 | 67.5 ± 39.8 | 0.475 |
| Privately paid vaccines per month, mean ± SD | 3.4 ± 6.3 | 4.7 ± 6.5 | 4.0 ± 6.4 | 0.807 |
| Percentage of children aged 6 through 23 months vaccinated in practice with the seasonal influenza vaccine during last influenza season, mean ± SD | 26.2 ± 20.6 | 26.4 ± 24.3 | 26.3 ± 22.4 | 0.711 |
| Immunization management practices | ||||
| Stock and administer vaccines in the clinic, n (%) | 31 (93.9) | 34 (97.1) | 65 (95.6) | 0.583 |
| Typically initiate discussions with parents on routine pediatric vaccinations, n (%) | 33 (100) | 38 (100) | 68 (100) | NA |
| Typically initiate discussions with parents on seasonal influenza vaccinations, n (%) | 28 (84.8) | 33 (94.3) | 61 (89.7) | 0.252 |
| Covariate | Beta ± SE | OR (95% CI) | p Value |
|---|---|---|---|
| Intercept | −0.103 ± 0.207 | 0.90 (0.60 to 1.36) | 0.620 |
| Exposure | |||
| Control group | Ref. | — | — |
| CME group | 0.418 ± 0.170 | 1.52 (1.09 to 2.12) | 0.014 |
| Socioeconomic status | |||
| Low | 0.467 ± 0.416 | 1.60 (0.71 to 3.61) | 0.261 |
| Medium | 0.136 ± 0.177 | 1.15 (0.81 to 1.62) | 0.440 |
| High | Ref. | — | — |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fisher, W.A.; Gilca, V.; Murti, M.; Orth, A.; Garfield, H.; Roumeliotis, P.; Rampakakis, E.; Brown, V.; Yaremko, J.; Van Buynder, P.; et al. Continuing Medical Education Improves Physician Communication Skills and Increases Likelihood of Pediatric Vaccination: Findings from the Pediatric Influenza Vaccination Optimization Trial (PIVOT)—II. Vaccines 2023, 11, 17. https://doi.org/10.3390/vaccines11010017
Fisher WA, Gilca V, Murti M, Orth A, Garfield H, Roumeliotis P, Rampakakis E, Brown V, Yaremko J, Van Buynder P, et al. Continuing Medical Education Improves Physician Communication Skills and Increases Likelihood of Pediatric Vaccination: Findings from the Pediatric Influenza Vaccination Optimization Trial (PIVOT)—II. Vaccines. 2023; 11(1):17. https://doi.org/10.3390/vaccines11010017
Chicago/Turabian StyleFisher, William A., Vladimir Gilca, Michelle Murti, Alison Orth, Hartley Garfield, Paul Roumeliotis, Emmanouil Rampakakis, Vivien Brown, John Yaremko, Paul Van Buynder, and et al. 2023. "Continuing Medical Education Improves Physician Communication Skills and Increases Likelihood of Pediatric Vaccination: Findings from the Pediatric Influenza Vaccination Optimization Trial (PIVOT)—II" Vaccines 11, no. 1: 17. https://doi.org/10.3390/vaccines11010017
APA StyleFisher, W. A., Gilca, V., Murti, M., Orth, A., Garfield, H., Roumeliotis, P., Rampakakis, E., Brown, V., Yaremko, J., Van Buynder, P., Boikos, C., & Mansi, J. A. (2023). Continuing Medical Education Improves Physician Communication Skills and Increases Likelihood of Pediatric Vaccination: Findings from the Pediatric Influenza Vaccination Optimization Trial (PIVOT)—II. Vaccines, 11(1), 17. https://doi.org/10.3390/vaccines11010017