

Experience of COVID-19 Vaccination among Primary Healthcare Workers in Hong Kong: A Qualitative Study



Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Research Team
2.3. Research Setting
2.4. Participant Recruitment
2.5. Data Collection
2.6. Data Analysis
2.7. Ethical Consideration
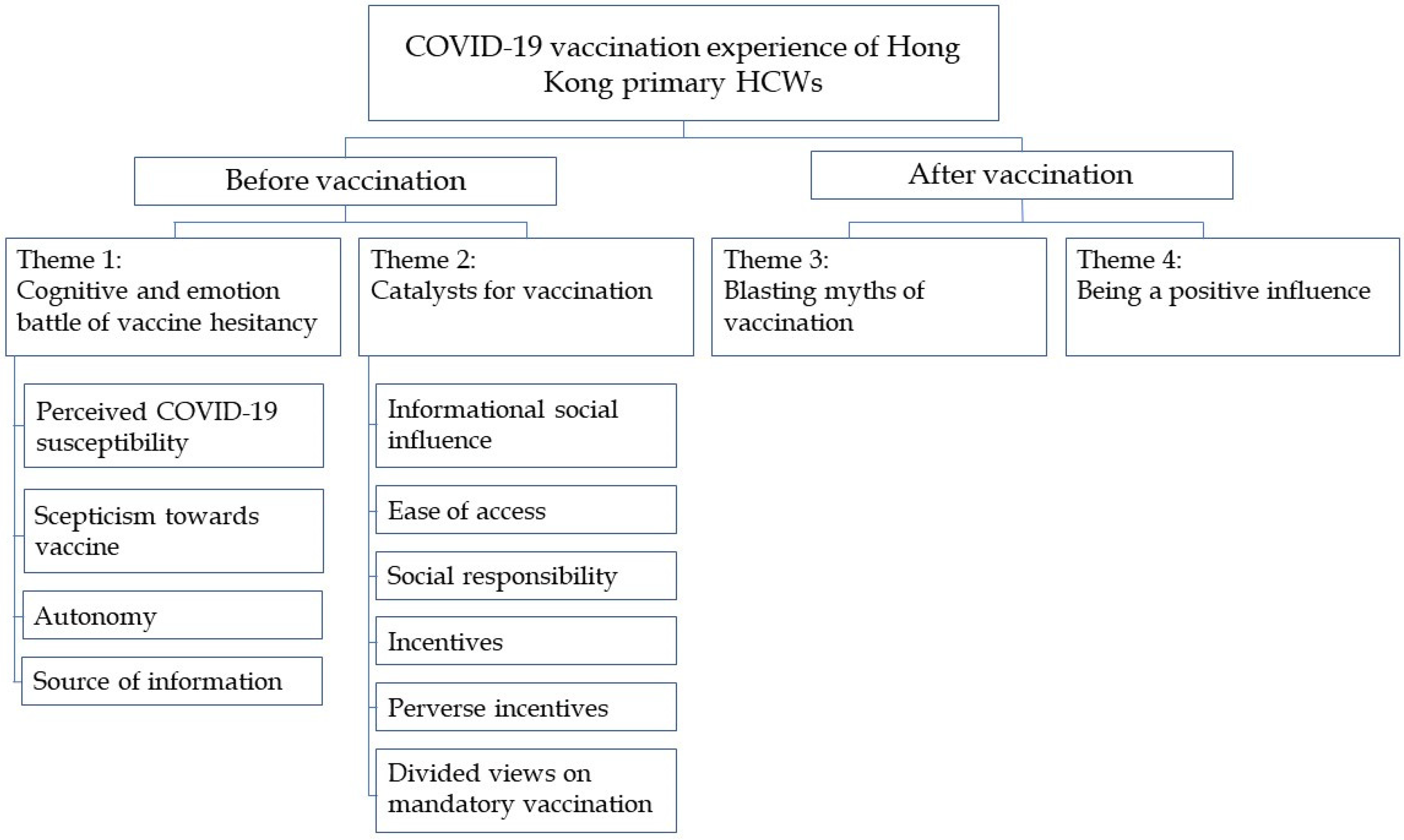
3. Results
3.1. Theme 1: Cognitive and Emotional Battle of Vaccine Hesitancy
3.1.1. Perceived COVID-19 Susceptibility
“I’m very concerned (of infection) at the moment, because of the Omicron variant and its severe outbreak in other countries. It seems we could not escape from it. …absolutely I need to vaccinate to prevent infection.”(Participant N8, 48-year-old, female, advanced practice nurse, 24 years of working experience)
“…healthcare workers should protect our patients, friends, and family members we encounter in daily life, and even more, if all of us are vaccinated, then we could protect our community, and the pandemic would end sooner.”(Participant D8, 30-year-old, female, GP resident trainee, 5 years of working experience)
3.1.2. Scepticism towards Vaccine
“I’m afraid, fear the side effects, because it did not follow conventional procedures and put into market.”(Participant S2, 35-year-old, male, clerical staff, 10 years of working experience)
“I took [deidentified] (an inactivated COVID-19 vaccine), which uses an established technology, … unlike [deidentified] (an mRNA COVID-19 vaccine) which is very new and there are lots of uncertainties.”(Participant N3, 45-year-old, female, registered nurse, 21 years of working experience)
“I think the vaccine is useless, as you can see people were still infected after receiving three doses of vaccine.”(Participant N6, 51-year-old, female, registered nurse, 26 years of working experience)
“…when the news reported that there were a lot of people got severe side effects, it stopped me from vaccination. …those sudden death, myocarditis during exercises, and stroke... It was in the news everyday.”(Participant N4, 32-year-old, female, registered nurse, 9 years of working experience)
3.1.3. Autonomy
“We have autonomy, especially healthcare workers. Each of us has our judgement on vaccination, to balance risks and benefits, and it should not be mandatory.”(Participant D2, 30-year-old, female, GP resident trainee, 7 years of working experience)
3.1.4. Source of Information
“In March 2021, there were many scientific papers published which were large-scale studies, especially the [deidentified international] study. I obtained information from those studies.”(Participant D10, 48-year-old, male, GP consultant, 23 years of working experience)
“I really had to find (information about the vaccines) by myself, as we didn’t have enough information.”(Participant S1, 55-year-old, female, patient care assistant, 10 years of working experience)
“I had (enough information about the vaccines), from news and my friend.”(Participant S8, patient care assistant, 59-year-old, female, 10 years of working experience)
“Frontline staff such as nurses and supporting staff may not have update from the latest study. Perhaps one could publish some pamphlets and newsletter to enhance their understanding on the disease and vaccines, so that they can make an appropriate choice.”(Participant D6, 42-year-old, male, associate GP consultant, 19 years of working experience)
3.2. Theme 2: Catalysts for Vaccination
3.2.1. Informational Social Influence
“I observed other people for 7 months before I had the confidence to vaccinate.”(Participant N2, 46-year-old, female, registered nurse, 19 years of working experience)
“I planned to vaccinate once available, but then I changed my mind and observed first. When I noticed half of colleagues in my clinic got vaccinated, and they did not have many side effects, then I decided to vaccinate.”(Participant D8, 30-year-old, female, GP resident trainee, 5 years of working experience)
“Government officials and celebrities vaccinated first, to be a role model…is effective.”(Participant S7, 56-year-old, female, phlebotomist, 15 years of working experience)
3.2.2. Ease of Access
“It is convenient for me to vaccinate at [deidentified] Hospital (close to his workplace). If I vaccinated earlier, I would have to travel to community vaccination centre which was troublesome.”(Participant D2, 30-year-old, female, GP resident trainee, 7 years of working experience)
3.2.3. Social Responsibility
“Social responsibility (is a factor affecting vaccination), because I am a medical professional. I have to do it myself first in order to be role model for others especially the public. We are an important symbolic figure, and we should get the shot first in order to motivate them.”(Participant D10, 48-year-old, male, GP consultant, 23 years of working experience)
3.2.4. Incentives
“I vaccinated (in June 2021) because there was AVL.”(Participant S3, 23-year-old, female, clinic clerk, 2 years of working experience)
“The most important thing we concern about (the vaccines) is the efficacy in protection. Financial reward is just an additional benefit.”(Participant D7, 39-year-old, female, GP resident, 16 years of working experience)
“I don’t suggest using lucky draw to promote vaccination. It seems like you vaccinate because you want to get the prize, but not protection.”(Participant N3, 45-year-old, female, registered nurse, 21 years of working experience)
3.2.5. Perverse Incentives
“…and if I did not vaccinate by 1 September, we had to pay for the test. That’s a big concern and I decided to vaccinate.”(Participant N4, 32-year-old, female, registered nurse, 9 years of working experience)
“Yes, I did not vaccinate by June and therefore my supervisor asked me, when I would vaccinate, why I haven’t vaccinated, and I felt stressed. However, since I got the jab, there was no more stress.”(Participant N10, 29-year-old, female, registered nurse, 7 years of working experience)
“I vaccinated because of social convenience. If you don’t vaccinate, you can’t do a lot of things, such as entering some public venues.”(Participant N2, 46-year-old, female, registered nurse, 19 years of working experience)
3.2.6. Divided Views on Mandatory Vaccination
“The aim (of mandatory vaccination) is to fight the pandemic together. We are in the medical field, and if we don’t take the first step, then how can we lead our citizens? Therefore, I think it is acceptable.”(Participant N8, 48-year-old, female, advanced practice nurse, 24 years of working experience)
“Some colleagues are physically unfit for vaccination, and therefore you cannot make it a mandate. Do you count it as injury on-duty if adverse effects happen after vaccination?”(Participant N3, 45-year-old, female, registered nurse, 21 years of working experience)
3.3. Theme 3: Blasting Myths of Vaccination
“The process was smooth. Basically, the waiting time was short, and I did not have much paperwork to do, and therefore, after the staff scanned my QR code and checked my name, I was ready to vaccinate.”(Participant D5, 42-year-old, male, associate GP consultant, 19 years of working experience)
“I had some malaise and some injection site pain, and there was no fever. I worked and exercised as usual. I didn’t know there could be myocarditis at that moment, and I just kept running and hiking without any problem.”(Participant D10, 48-year-old, male, GP consultant, 23 years of working experience)
“The side effects weren’t as severe as circulated in public.”(Participant N2, 46-year-old, female, registered nurse, 19 years of working experience)
3.4. Theme 4: Being a Positive Influence
“I felt less feared (after vaccination). Previously I was concerned about infection and complications (of COVID-19), and now it was prevented.”(Participant D2, 30-year-old, female, GP resident trainee, 7 years of working experience)
“…when I know my colleagues and friends aren’t vaccinated, I’ll remind them about the urgency of vaccination, as the most important reason for vaccination to protect themselves.”(Participant S5, 41-year-old, female, patient care assistant, 6 years of working experience)
“(After vaccination myself,) I am more confident in encouraging patients in getting jabs.”(Participant S1, 55-year-old, female, patient care assistant, 10 years of working experience)
“I took the booster dose much earlier because the last 2 doses were unremarkable.”(Participant N7, 51-year-old, female, registered nurse, 25 years of working experience)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Wilde, J.A.; McMillan, J.A.; Serwint, J.; Butta, J.; O’Riordan, M.A.; Steinhoff, M.C. Effectiveness of influenza vaccine in health care professionals: A randomized trial. JAMA 1999, 281, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Salgado, C.D.; Giannetta, E.T.; Hayden, F.G.; Farr, B.M. Preventing nosocomial influenza by improving the vaccine acceptance rate of clinicians. Infect. Control Hosp. Epidemiol. 2004, 25, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Willems, L.D.; Dyzel, V.; Sterkenburg, P.S. COVID-19 Vaccination Intentions amongst Healthcare Workers: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 10192. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9407815/ (accessed on 2 September 2022). [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef] [PubMed]
- Hospital Authority. Press Release. Hospital Authority: Hong Kong. 2021. Available online: https://www.ha.org.hk/haho/ho/pad/60976c.pdf (accessed on 26 September 2021).
- Gagneux-Brunon, A.; Botelho-Nevers, E.; Bonneton, M.; Peretti-Watel, P.; Verger, P.; Launay, O.; Ward, J.K. Public opinion on a mandatory COVID-19 vaccination policy in France: A cross-sectional survey. Clin. Microbiol. Infect. 2022, 28, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Hospital Authority. Press Release. Hospital Authority: Hong Kong. 2021. Available online: https://www.ha.org.hk/haho/ho/pad/210802Eng2.pdf (accessed on 26 September 2021).
- Teo, L.M.; Smith, H.E.; Lwin, M.O.; Tang, W.E. Attitudes and perception of influenza vaccines among older people in Singapore: A qualitative study. Vaccine 2019, 37, 6665–6672. [Google Scholar] [CrossRef] [PubMed]
- Keske, Ş.; Mutters, N.T.; Tsioutis, C.; Ergönül, Ö.; EUCIC influenza vaccination survey team. Influenza vaccination among infection control teams. A EUCIC survey prior to COVID-19 pandemic. Vaccine 2020, 38, 8357–8361. [Google Scholar] [CrossRef] [PubMed]
- Hospital Authority. Clinical Services Plan for the New Territories West Cluster 2017; Hospital Authority: Hong Kong, China, 2017; 132p. [Google Scholar]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0208601 (accessed on 1 October 2021). [CrossRef] [PubMed]
- QSR International Pty Ltd. NVivo (Version 12). 2018. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 1 February 2022).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- American Psychological Association. APA Dictionary of Psychology; Americal Psychological Association: Washington, DC, USA; Available online: https://dictionary.apa.org/informational-influence (accessed on 7 May 2022).
- Al-Hasan, A.; Khuntia, J.; Yim, D. Does Seeing What Others Do Through Social Media Influence Vaccine Uptake and Help in the Herd Immunity Through Vaccination? A Cross-Sectional Analysis. Front. Public Health 2021, 9, 715931. Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2021.715931/full (accessed on 7 May 2022). [CrossRef] [PubMed]
- Toth-Manikowski, S.M.; Swirsky, E.S.; Gandhi, R.; Piscitello, G. COVID-19 vaccination hesitancy among health care workers, communication and policy-making. Am. J. Infect. Control. 2022, 50, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Ganti, L.; Graham, E.W.; Shah, D.; Aleksandrovskiy, I.; Al-Bassam, M.; Fraunfelter, F.; Falgiani, M.; Leon, L.; Lopez-Ortiz, C. COVID-19 Vaccine Hesitancy Among Healthcare Providers. Health Psychol. Res. 2022, 10, 34128. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9239370/ (accessed on 2 September 2022). [CrossRef] [PubMed]
- Manby, L.; Dowrick, A.; Karia, A.; Maio, L.; Buck, C.; Singleton, G.; Lewis-Jackson, S.; Uddin, I.; Vanderslott, S.; Martin, S.; et al. Healthcare workers’ perceptions and attitudes towards the UK’s COVID-19 vaccination programme: A rapid qualitative appraisal. BMJ Open 2022, 12, e051775. [Google Scholar] [CrossRef] [PubMed]
- Elwy, A.R.; Clayman, M.L.; LoBrutto, L.; Miano, D.; Ann Petrakis, B.; Javier, S.; Erhardt, T.; Midboe, A.M.; Carbonaro, R.; Jasuja, G.K.; et al. Vaccine hesitancy as an opportunity for engagement: A rapid qualitative study of patients and employees in the, U.S. Veterans Affairs healthcare system. Vaccine 2021, 9, 100116. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, S.; Salmanton-Garcia, J.; Cornely, O.A.; Mellinghoff, S.C. Increasing influenza coverage in healthcare workers: A review on campaign strategies and their effect. Infection 2021, 49, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Brauer, E.; Choi, K.; Chang, J.; Luo, Y.; Lewin, B.; Munoz-Plaza, C.; Bronstein, D.; Bruxvoort, K. Health Care Providers’ Trusted Sources for Information About COVID-19 Vaccines: Mixed Methods Study. JMIR Infodemiology 2021, 1, e33330. [Google Scholar] [CrossRef] [PubMed]
- Aci, O.S.; Kackin, O.; Karaaslan, S.; Ciydem, E. Qualitative examination of the attitudes of healthcare workers in Turkey regarding COVID-19 vaccines. Int. J. Nurs. Knowl. 2021, 33, 136–146. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Topic | Question(s) | Probes/Prompts |
|---|---|---|
| Introduction | What comes to mind when you first hear the term “COVID-19 vaccines”? | |
| Factors affecting vaccination | Please tell me the factors affecting your intention to vaccinate. | How at risk did you think you were of contracting COVID-19? Considering your risk, did you think you were indicated for COVID-19 vaccination? Please elaborate. |
| Did your confidence in COVID-19 vaccine affect your decision to vaccinate? Please elaborate. | ||
| Were there any barriers for you to receive a COVID-19 vaccines? Please elaborate. | ||
| Did you feel you have adequate information to decide whether to have the COVID-19 vaccine? If not, what sort of information did you lack? Please elaborate. | ||
| Some people vaccinate because they want to protect others. What is your view? | ||
| Are they any other reasons that affect | ||
| When did you decide to receive the COVID-19 vaccine? How did you make up your mind at that moment? | ||
| Vaccination experience | Please tell me your experience of receiving the vaccination. | Where were you vaccinated? |
| How did you make the appointment? | ||
| Did you vaccinate during or outside work hours? | ||
| How did you feel about the arrangement at your vaccination venue? | ||
| What suggestions do you have for improving the vaccination experience? | ||
| Effects of vaccination | Please tell me your experience after vaccination. | Did you experience any side effects? If yes, what are they and how long did they last? |
| Did vaccination change your daily life? If yes, how | Did vaccination have impact on your work? | |
| Did vaccination have impact on your social life? | ||
| Did vaccination have impact on your health? | ||
| Considering your experience, would you recommend COVID-19 vaccination to others? | ||
| Attitudes on vaccination promotion strategies | What vaccination promotion strategies do you know that targeted healthcare workers in Hong Kong? What are your views on these strategies? | What are your views on promotion from social media/authorised vaccination leave/lucky draw for vaccinated people? |
| Some countries employed mandatory vaccination policies for healthcare workers. What is your opinion on such strategy? | ||
| Do you have any suggestion for vaccination promotion strategy targeting healthcare workers? |
| Participant ID | Ranking | Gender | Age | Working Experience (Years) | Time between Vaccination and Launch of Vaccination Programme (Months) |
|---|---|---|---|---|---|
| D1 | GP resident specialist | Male | 39 | 14 | 0 |
| D2 | GP resident trainee | Female | 30 | 7 | 3 |
| D3 | GP associate consultant | Male | 44 | 19 | 0 |
| D4 | GP resident | Male | 52 | 29 | 1 |
| D5 | GP associate consultant | Male | 42 | 19 | 0 |
| D6 | GP associate consultant | Male | 42 | 19 | 0 |
| D7 | GP resident | Female | 39 | 16 | 2 |
| D8 | GP resident trainee | Female | 30 | 5 | 1 |
| D9 | GP resident trainee | Female | 28 | 5 | 1 |
| D10 | GP consultant | Male | 48 | 23 | 0 |
| N1 | Registered nurse | Female | 44 | 19 | 4 |
| N2 | Registered nurse | Female | 46 | 19 | 7 |
| N3 | Registered nurse | Female | 45 | 21 | 2 |
| N4 | Registered nurse | Female | 32 | 9 | 4 |
| N5 | Registered nurse | Female | 64 | 42 | 4 |
| N6 | Registered nurse | Female | 51 | 26 | 4 |
| N7 | Registered nurse | Female | 51 | 25 | 0 |
| N8 | Advanced practice nurse | Female | 48 | 24 | 1 |
| N9 | Registered nurse | Female | 32 | 9 | 1 |
| N10 | Registered nurse | Female | 29 | 7 | 4 |
| S1 | Patient care assistant | Female | 55 | 10 | 3 |
| S2 | Clinic clerk | Male | 35 | 10 | 3 |
| S3 | Clinic clerk | Female | 23 | 2 | 3 |
| S4 | Patient care assistant | Female | 46 | 10 | 3 |
| S5 | Patient care assistant | Female | 41 | 6 | 3 |
| S6 | Patient care assistant | Female | 59 | 19 | 3 |
| S7 | Phlebotomist | Female | 56 | 15 | 0 |
| S8 | Patient care assistant | Female | 59 | 10 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, K.M.; Chu, T.K.; Lau, P. Experience of COVID-19 Vaccination among Primary Healthcare Workers in Hong Kong: A Qualitative Study. Vaccines 2022, 10, 1531. https://doi.org/10.3390/vaccines10091531
Ng KM, Chu TK, Lau P. Experience of COVID-19 Vaccination among Primary Healthcare Workers in Hong Kong: A Qualitative Study. Vaccines. 2022; 10(9):1531. https://doi.org/10.3390/vaccines10091531
Chicago/Turabian StyleNg, Kai Man, Tsun Kit Chu, and Phyllis Lau. 2022. "Experience of COVID-19 Vaccination among Primary Healthcare Workers in Hong Kong: A Qualitative Study" Vaccines 10, no. 9: 1531. https://doi.org/10.3390/vaccines10091531
APA StyleNg, K. M., Chu, T. K., & Lau, P. (2022). Experience of COVID-19 Vaccination among Primary Healthcare Workers in Hong Kong: A Qualitative Study. Vaccines, 10(9), 1531. https://doi.org/10.3390/vaccines10091531