
Reduction of Precautionary Behaviour following Vaccination against COVID-19: A Test on a British Cohort


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Procedure
2.3. Measures
2.4. Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization COVID-19 Advice for the Public: Getting Vaccinated. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice (accessed on 9 July 2021).
- Hedlund, J. Risky Business: Safety Regulations, Risk Compensation, and Individual Behavior. Inj. Prev. 2000, 6, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Mantzari, E.; Rubin, G.J.; Marteau, T.M. Is Risk Compensation Threatening Public Health in the COVID-19 Pandemic? BMJ 2020, m2913. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Brainard, J.; Hunter, P.; Michie, S. Are People Letting down Their Guard Too Soon after COVID-19 Vaccination? Available online: https://blogs.bmj.com/bmj/2021/03/18/are-people-letting-down-their-guard-too-soon-after-covid-19-vaccination/?utm_source=twitter&utm_medium=social&utm_term=hootsuite&utm_content=sme&utm_campaign=usage (accessed on 9 June 2022).
- Scientific Pandemic Insights Group on Behaviours. SPI-B Possible Impact of the COVID-19 Vaccination Programme on Adherence to Rules and Guidance about Personal Protective Behaviours Aimed at Preventing Spread of the Virus, 17 December 2020, Published by the UK Government, London. Available online: https://www.gov.uk/government/publications/spi-b-possible-impact-of-the-covid-19-vaccination-programme-on-adherence-to-rules-and-guidance-about-personal-protective-behaviours-aimed-at-preventi (accessed on 9 June 2022).
- Trogen, B.; Caplan, A. Risk Compensation and COVID-19 Vaccines. Ann. Intern. Med. 2021, 174, 858–859. [Google Scholar] [CrossRef]
- Bernal, J.L.; Andrews, N.; Gower, C.; Stowe, J.; Robertson, C.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Early Effectiveness of COVID-19 Vaccination with BNT162b2 MRNA Vaccine and ChAdOx1 Adenovirus Vector Vaccine on Symptomatic Disease, Hospitalisations and Mortality in Older Adults in England. medRxiv 2021. [Google Scholar] [CrossRef]
- Hunter, P.R.; Brainard, J.S. Estimating the Effectiveness of the Pfizer COVID-19 BNT162b2 Vaccine after a Single Dose. A Reanalysis of a Study of’real-World’vaccination Outcomes from Israel. medRxiv 2021. [Google Scholar] [CrossRef]
- Brewer, N.T.; Cuite, C.L.; Herrington, J.E.; Weinstein, N.D. Risk Compensation and Vaccination: Can Getting Vaccinated Cause People to Engage in Risky Behaviors? Ann. Behav. Med. 2007, 34, 95–99. [Google Scholar] [CrossRef]
- Reiber, C.; Shattuck, E.C.; Fiore, S.; Alperin, P.; Davis, V.; Moore, J. Change in Human Social Behavior in Response to a Common Vaccine. Ann. Epidemiol. 2010, 20, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Kasting, M.L.; Shapiro, G.K.; Rosberger, Z.; Kahn, J.A.; Zimet, G.D. Tempest in a Teapot: A Systematic Review of HPV Vaccination and Risk Compensation Research. Hum. Vaccines Immunother. 2016, 12, 1435–1450. [Google Scholar] [CrossRef] [PubMed]
- Wright, L.; Steptoe, A.; Mak, H.W.; Fancourt, D. Do People Reduce Compliance with COVID-19 Guidelines Following Vaccination? A Longitudinal Analysis of Matched UK Adults. J. Epidemiol. Community Health 2022, 76, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Moussaoui, L.S.; Ofosu, N.D.; Desrichard, O. Social Psychological Correlates of Protective Behaviours in the COVID-19 Outbreak: Evidence and Recommendations from a Nationally Representative Sample. Appl. Psychol. Health Well-Being 2020, 12, 1183–1204. [Google Scholar] [CrossRef] [PubMed]
- Prolific. Available online: https://www.prolific.co (accessed on 3 June 2022).
- Risk Homeostasis, COVID-19 Vaccination, May 2021 (#67108). Available online: https://aspredicted.org/blind.php?x=8p9wh2 (accessed on 9 June 2022).
- OSF. Available online: https://osf.io/nxt6q/?view_only=6844f507c3884cc99e5da03a7b9be8a1 (accessed on 9 June 2022).
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Cardilli, L.; Reed, J.L.; Saunders, T.J.; Kite, C.; Douillette, K.; Fournier, K.; Buckley, J.P. A Comparison of Self-Reported and Device Measured Sedentary Behaviour in Adults: A Systematic Review and Meta-Analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 31. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Liu, J.; Koleva, Y.; Fonseca, V.; Kalsekar, A.; Pawaskar, M. Concordance of Adherence Measurement Using Self-Reported Adherence Questionnaires and Medication Monitoring Devices. PharmacoEconomics 2010, 28, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Howard, M.; Agarwal, G.; Lytwyn, A. Accuracy of Self-Reports of Pap and Mammography Screening Compared to Medical Record: A Meta-Analysis. Cancer Causes Control 2009, 20, 1. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Vaccination Status (Row Percent) | ||||||
|---|---|---|---|---|---|---|
| All | 0 Dose | 1 Dose < 14 Days | 1 Dose ≥ 14 Days | 2 Doses < 14 Days | 2 Doses ≥ 14 Days | |
| N (%) * | 765 (100%) | 178 (23.4) | 48 (6.5) | 176 (23.1) | 108 (23.1) | 251 (33) |
| Age years | ||||||
| Mean (SD) | 48.1 (14.6) | 36 (13.4) | 35 (6.9) | 48 (9.93) | 54.5 (9.23) | 56.4 (13.4) |
| Sex | ||||||
| Male (%) | 353 (47.6) | 85 (24.4) | 27 (7.8) | 86 (24.7) | 46 (13.2) | 104 (29.9) |
| Female (%) | 388 (52.4) | 84 (21.8) | 19 (4.9) | 85 (22.1) | 57 (14.8) | 140 (36.4) |
| Comorbidities | ||||||
| Yes (%) | 137 (17.9) | 16 (11.7) | 1 (0.7) | 28 (20.4) | 18 (13.1) | 74 (54) |
| No (%) | 628 (82.1) | 162 (26) | 47 (7.5) | 147 (23.6) | 90 (14.4) | 177 (28.4) |
| COVID-19 Status ** | ||||||
| 1 (%) | 461 (61.1) | 88 (19.2) | 28 (6.1) | 107 (23.4) | 56 (12.2) | 179 (39.1) |
| 2 (%) | 135 (17.9) | 37 (27.8) | 10 (7.5) | 27 (20.3) | 28 (21.1) | 31 (23.3) |
| 3 (%) | 83 (11) | 22 (26.5) | 7 (8.4) | 22 (26.5) | 13 (15.7) | 19 (22.9) |
| 4 (%) | 75 (9.9) | 28 (37.3) | 3 (4) | 17 (22.7) | 9 (12) | 18 (24) |
| Perceived protection | ||||||
| Mean (SD) | 41.2 (34) | 48.8 (21.9) | 53.8 (17.3) | 70.8 (16.4) | 79.4 (14.8) | |
| Educational Level | ||||||
| 1 (%) | 10 (1.3) | 3 (30) | 0 (0) | 2 (20) | 2 (20) | 3 (30) |
| 2 (%) | 100 (13.4) | 13 (13.3) | 2 (2) | 31 (31.6) | 16 (16.3) | 36 (36.7) |
| 3 (%) | 126 (16.9) | 50 (40) | 9 (7.2) | 20 (16.0) | 17 (13.6) | 29 (23.2) |
| 4 (%) | 99 (13.3) | 16 (16.3) | 0 (0) | 24 (24.5) | 14 (14.3) | 44 (44.9) |
| 5 (%) | 269 (36.2) | 65 (24.4) | 18 (6.8) | 58 (21.8) | 38 (14.3) | 87 (32.7) |
| 6 (%) | 119 (16.0) | 22 (18.6) | 14 (11.9) | 30 (25.4) | 15 (12.7) | 37 (31.4) |
| 7 (%) | 21 (2.8) | 2 (9.5) | 3 (14.3) | 6 (28.6) | 2 (9.5) | 8 (38.1) |
| Simple Effects of Time of Measurement | |||||||
|---|---|---|---|---|---|---|---|
| Outcomes | Main Effect of Time of Measurement | Time of Measurement * Number of Doses | 0 Dose | 1 < 14 Days | 1 ≥ 14 Days | 2 < 14 Days | 2 ≥ 14 Days |
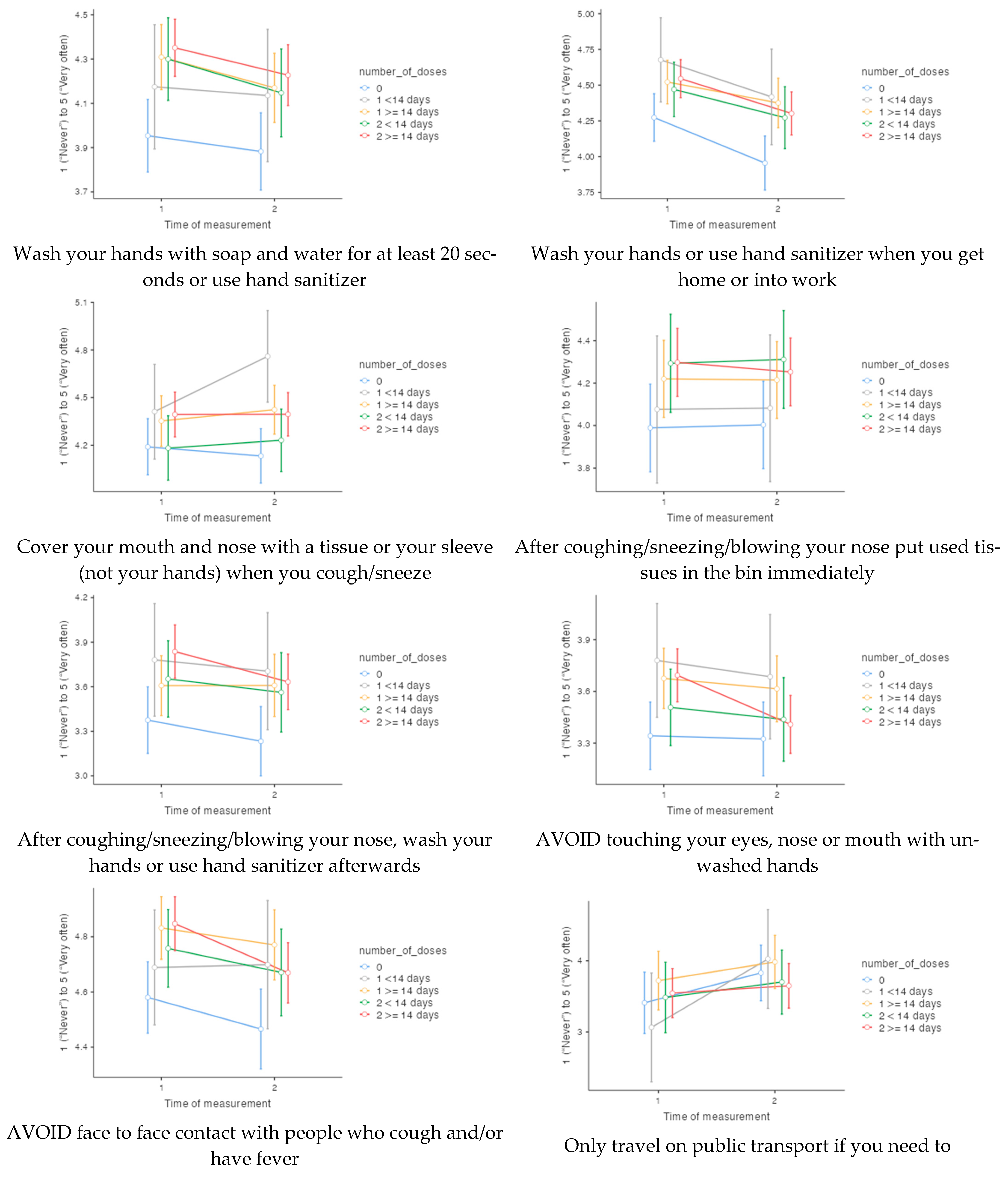
| Wash your hands with soap and water for at least 20 s or use hand sanitizer | p = 0.0012 η2p = 0.015 * (−) | p = 0.9322 η2p = 0.001 | p = 0.3845 | p = 0.7783 | p = 0.0578 | p = 0.1013 | p = 0.0554 |
| Wash your hands or use hand sanitizer when you get home or into work | p = 0.0001 η2p = 0.051 * (−) | p = 0.6112 η2p = 0.004 | p = 0.0003 * (−) | p = 0.0992 | p = 0.0718 | p = 0.0520 | p = 0.0006 * (−) |
| Cover your mouth and nose with a tissue or your sleeve (not your hands) when you cough/sneeze | p = 0.1947 η2p = 0.003 | p = 0.1669 η2p = 0.010 | p = 0.5389 | p = 0.0274 | p = 0.3996 | p = 0.6531 | p = 0.9867 |
| After coughing/ sneezing/blowing your nose put used tissues in the bin immediately | p = 0.9541 η2p = 0.000 | p = 0.9854 η2p = 0.001 | p = 0.8888 | p = 0.9718 | p = 0.9537 | p = 0.8696 | p = 0.5620 |
| After coughing/sneezing/ blowing your nose, wash your hands or use hand sanitizer afterwards | p = 0.0107 η2p = 0.010 | p = 0.4376 η2p = 0.006 | p = 0.1507 | p = 0.6488 | p = 0.9888 | p = 0.4262 | p = 0.0101 * (−) |
| AVOID touching your eyes, nose or mouth with unwashed hands | p = 0.0008 η2p = 0.016 * (−) | p = 0.1296 η2p = 0.010 | p = 0.8462 | p = 0.5520 | p = 0.4733 | p = 0.5128 | p = 0.0001 * (−) |
| AVOID face to face contact with people who cough and/or have fever | p = 0.0351 η2p = 0.007 | p = 0.6073 η2p = 0.004 | p = 0.1674 | p = 0.9398 | p = 0.4004 | p = 0.3326 | p = 0.0046 * (−) |
| Only travel on public transport if you need to | p = 0.0026 η2p = 0.023 * (+) | p = 0.5008 η2p = 0.008 | p = 0.0826 | p = 0.0251 | p = 0.2557 | p = 0.4349 | p = 0.5954 |
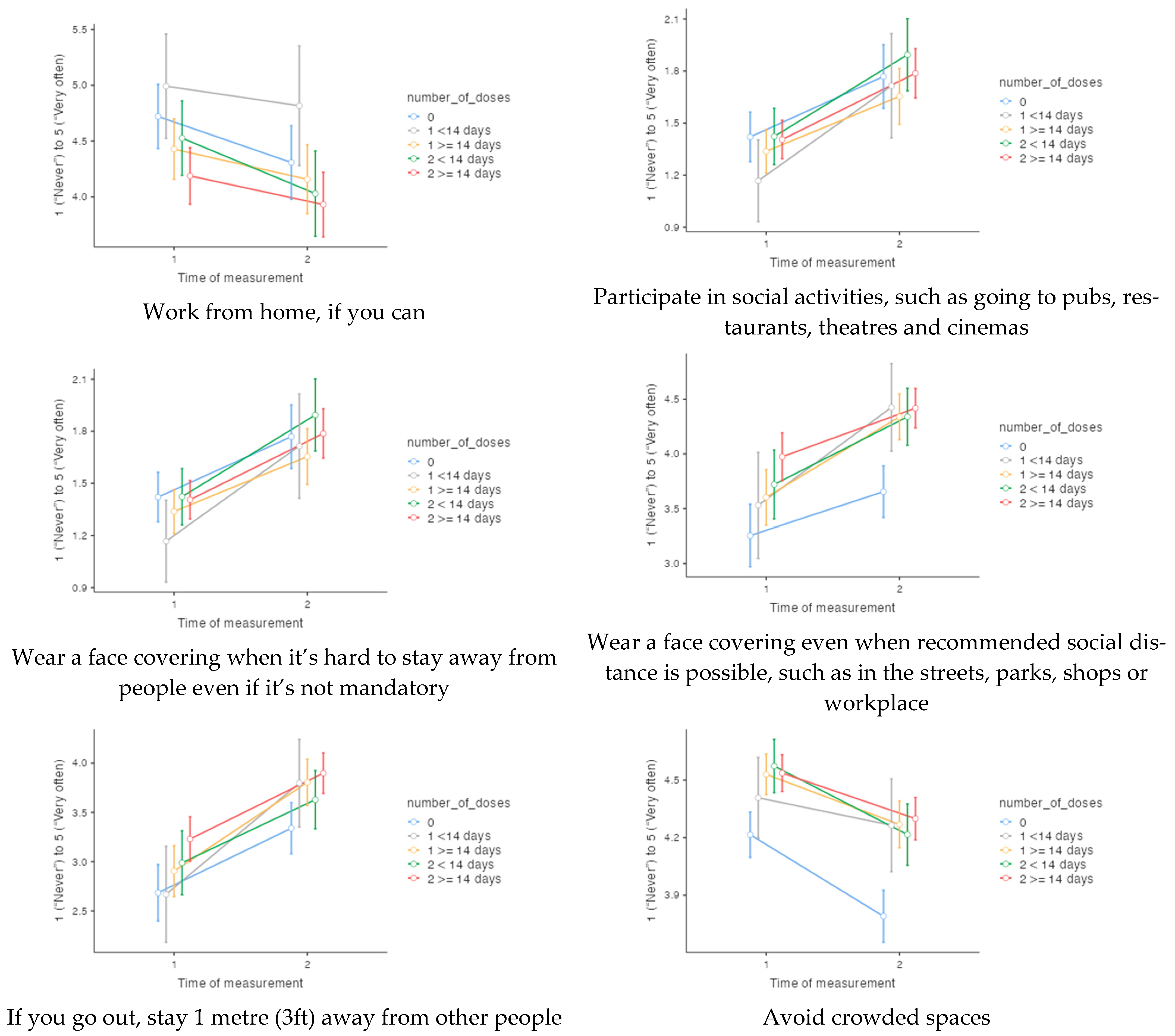
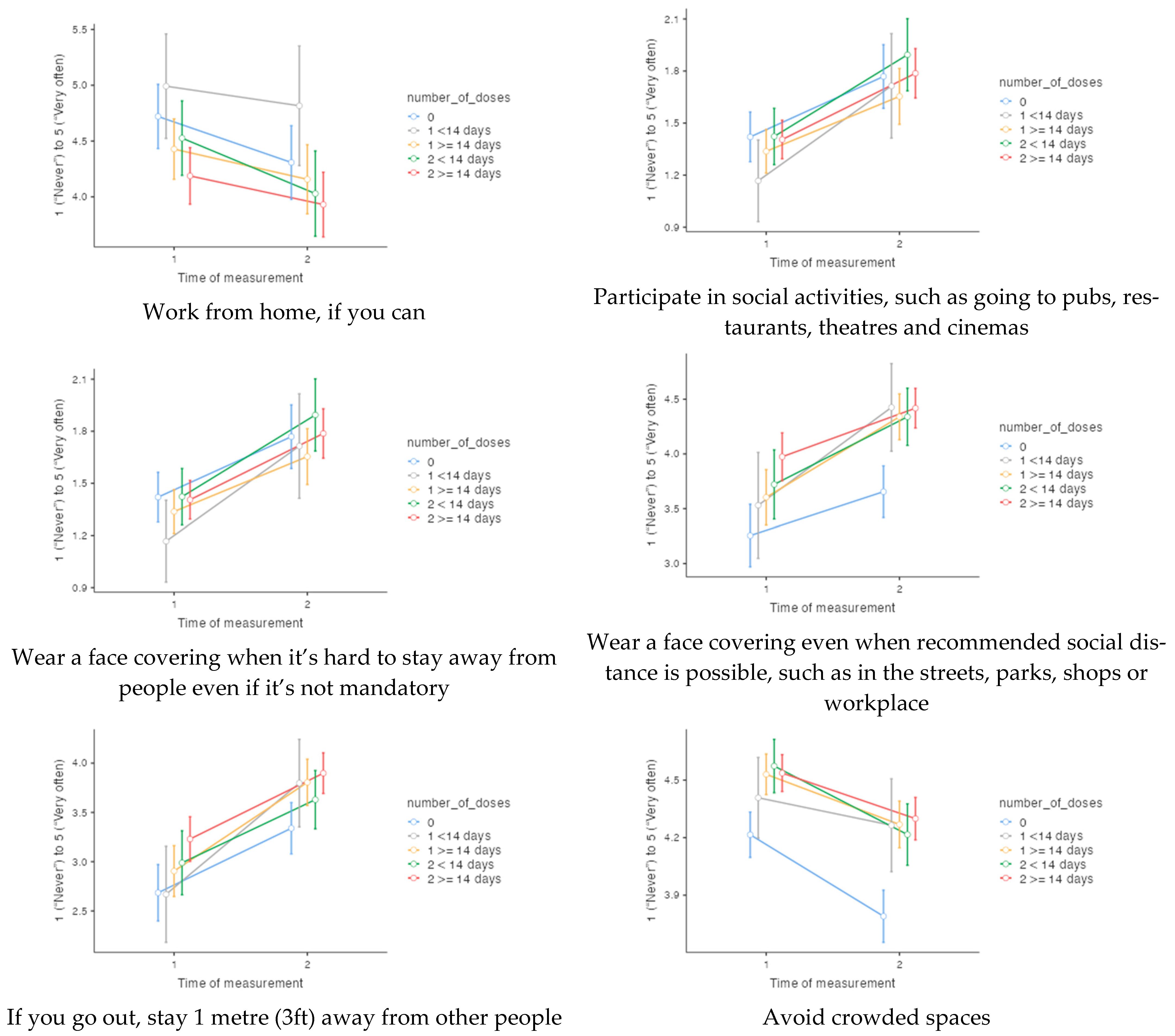
| Work from home, if you can | p = 0.0005 η2p = 0.032 * (−) | p = 0.5656 η2p = 0.000 | p = 0.0043 * (−) | p = 0.4535 | p = 0.0457 | p = 0.0030 * (−) | p = 0.0429 |
| Participate in social activities, such as going to pubs, restaurants, theatres and cinemas | p < 0.0001 η2p = 0.128 * (+) | p = 0.4464 η2p = 0.006 | p < 0.0001 * (+) | p = 0.0001 * (+) | p < 0.0001 * (+) | p < 0.0001 * (+) | p < 0.0001 * (+) |
| Wear a face covering when it’s hard to stay away from people even if it’s not mandatory | p < 0.0001 η2p = 0.143 * (+) | p = 0.0807 η2p = 0.013 | p = 0.0043 * (+) | p = 0.0002 * (+) | p < 0.0001 * (+) | p < 0.0001 * (+) | p < 0.0001 * (+) |
| Wear a face covering even when recommended social distance is possible, such as in the streets, parks, shops or workplace | p < 0.0001 η2p = 0.168 * (+) | p = 0.2748 η2p = 0.008 | p < 0.0001 * (+) | p < 0.0001 * (+) | p < 0.0001 * (+) | p = 0.0003 * (+) | p < 0.0001 * (+) |
| If you go out, stay 1 metre (3ft) away from other people | p < 0.0001 η2p = 0.087 * (+) | p = 0.1014 η2p = 0.011 | p < 0.0001 * (+) | p = 0.1963 | p < 0.0001 * (+) | p < 0.0001 * (+) | p < 0.0001 * (+) |
| Avoid crowded spaces | p ≤ 0.0001 η2p = 0.083 * (−) | p = 0.5227 η2p = 0.005 | p = 0.0001 * (−) | p = 0.0821 | p = 0.0044 * (−) | p = 0.0003 * (−) | p < 0.0001 * (−) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Desrichard, O.; Moussaoui, L.; Ofosu, N. Reduction of Precautionary Behaviour following Vaccination against COVID-19: A Test on a British Cohort. Vaccines 2022, 10, 936. https://doi.org/10.3390/vaccines10060936
Desrichard O, Moussaoui L, Ofosu N. Reduction of Precautionary Behaviour following Vaccination against COVID-19: A Test on a British Cohort. Vaccines. 2022; 10(6):936. https://doi.org/10.3390/vaccines10060936
Chicago/Turabian StyleDesrichard, Olivier, Lisa Moussaoui, and Nana Ofosu. 2022. "Reduction of Precautionary Behaviour following Vaccination against COVID-19: A Test on a British Cohort" Vaccines 10, no. 6: 936. https://doi.org/10.3390/vaccines10060936
APA StyleDesrichard, O., Moussaoui, L., & Ofosu, N. (2022). Reduction of Precautionary Behaviour following Vaccination against COVID-19: A Test on a British Cohort. Vaccines, 10(6), 936. https://doi.org/10.3390/vaccines10060936