
Recurring Weakness in Rhabdomyolysis Following Pfizer–BioNTech Coronavirus Disease 2019 mRNA Vaccination


Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zimmerman, J.L.; Shen, M.C. Rhabdomyolysis. Chest 2013, 144, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Cabral, B.M.I.; Edding, S.N.; Portocarrero, J.P.; Lerma, E.V. Rhabdomyolysis. Dis Mon. 2020, 66, 101015. [Google Scholar] [CrossRef] [PubMed]
- Callado, R.B.; Carneiro, T.G.P.; Parahyba, C.C.C.; Lima, N.A.; Silva, G.B., Jr.; Daher, E.F. Rhabdomyolysis secondary to influenza A H1N1 vaccine resulting in acute kidney injury. Travel. Med. Infect. Dis. 2013, 11, 130–133. [Google Scholar] [CrossRef]
- Rajaratnam, N.; Govil, S.; Patel, R.; Ahmed, M.; Elias, S. Rhabdomyolysis after recombinant zoster vaccination: A rare adverse reaction. J. Community Hosp. Intern. Med. Perspect. 2021, 11, 145–146. [Google Scholar] [CrossRef]
- Hursitoglu, M.; Cikrikcioglu, M.A.; Gundogan, E.; Ozkan, O.; Cordan, I.; Yigit, Y.; Kara, O.; Soysal, P.; Rabus, S.A.; Celepkolu, T.; et al. Rhabdomyolysis secondary to tetanus toxoid administration in a patient following minor laceration. J. Clin. Pharmacol. 2011, 51, 110–111. [Google Scholar] [CrossRef]
- Kulkarni, H.; Lenzo, N.; McLean-Tooke, A. Causality of rhabdomyolysis and combined tetanus, diphtheria and acellular pertussis (Tdap) vaccine administration. J. Clin. Pharmacol. 2013, 53, 1099–1102. [Google Scholar] [CrossRef]
- Pereira, F.; Moraes, R.d.; Bavel, D.; Lorenzo, A.R.d.; Tibirica, E. Exertional Rhabdomyolysis after Military Training Paralleled by Systemic Microvascular Dysfunction and Plasma Cytokine Increase: A Case Report. Arq. Bras. Cardiol. 2019, 113, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.Y.; Pan, C.T.; Cheng, C.F.; Lin, C.Y.; Chang, S.N.; Chen, Y.C.; Wang, C.Y.; Chen, Y.F.; Chen, C.Y.; Ma, M.H.M.; et al. Combined intravenous immunoglobulin and baricitinib treatment for severe COVID-19 with rhabdomyolysis: A Case report. J. Formos. Med. Assoc. 2021, 120, 1777–1781. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Elias, C.; Cardoso, P.; Gonçalves, D.; Vaz, I.; Cardoso, L. Rhabdomyolysis Following Administration of Comirnaty®. Eur. J. Case Rep. Intern. Med. 2021, 8, 002796. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, B. Case Report: ANCA-Associated Vasculitis Presenting with Rhabdomyolysis and Pauci-Immune Crescentic Glomerulonephritis After Pfizer-BioNTech COVID-19 mRNA Vaccination. Front. Immunol. 2021, 12, 762006. [Google Scholar] [CrossRef] [PubMed]
- Nassar, M.; Chung, H.; Dhayaparan, Y.; Nyein, A.; Acevedo, B.J.; Chicos, C.; Zheng, D.; Barras, M.; Mohamed, M.; Alfishawy, M.; et al. COVID-19 vaccine induced rhabdomyolysis: Case report with literature review. Diabetes Metab. Syndr. 2021, 15, 102170. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Health and Human Services (DHHS); Public Health Service (PHS); Centers for Disease Control (CDC)/Food and Drug Administration (FDA); Vaccine Adverse Event Reporting System (VAERS). 1990–4/16/2021, CDC WONDER On-line Database. 2021. Available online: https://wonder.cdc.gov/vaers.html (accessed on 21 July 2021).
- Israeli, E.; Agmon-Levin, N.; Blank, M.; Shoenfeld, Y. Adjuvants and autoimmunity. Lupus 2009, 18, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.P.; Kozoriz, M.G.; Ahmadi, A.A.; Kelsall, J.; Paquette, K.; Onrot, J.M. Post-vaccination myositis and myocarditis in a previously healthy male. Allergy Asthma Clin. Immunol. 2016, 12, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Rasbi, S.; Al-Maqbali, J.S.; Al-Farsi, R.; Shukaili, M.A.A.; Al-Riyami, M.H.; Falahi, Z.A.; Farhan, H.A.; Alawi, A.M.A. Myocarditis, Pulmonary Hemorrhage, and Extensive Myositis with Rhabdomyolysis 12 Days After First Dose of Pfizer-BioNTech BNT162b2 mRNA COVID-19 Vaccine: A Case Report. Am. J. Case Rep. 2022, 23, e934399. [Google Scholar] [CrossRef]
- Tan, A.; Stepien, K.M.; Narayana, S.T.K. Carnitine palmitoyltransferase II deficiency and post-COVID vaccination rhabdomyolysis. QJM 2021, 114, 596–597. [Google Scholar] [CrossRef]
- Gelbenegger, G.; Cacioppo, F.; Firbas, C.; Jilma, B. Rhabdomyolysis following Ad26.COV2.S COVID-19 Vaccination. Vaccines 2021, 9, 956. [Google Scholar] [CrossRef]
- Arunachalam, P.S.; Scott, M.K.D.; Hagan, T.; Li, C.; Feng, Y.; Wimmers, F.; Grigoryan, L.; Trisal, M.; Edara, V.V.; Lai, L.; et al. Systems Vaccinology of the BNT162b2 mRNA Vaccine in Humans. Nature 2021, 596, 410–416. [Google Scholar] [CrossRef]
- Laczkó, D.; Hogan, M.J.; Toulmin, S.A.; Hicks, P.; Lederer, K.; Gaudette, B.T.; Castaño, D.; Amanat, F.; Muramatsu, H.; Oguin, T.H., 3rd; et al. A Single Immunization with Nucleoside-Modified MRNA Vaccines Elicits Strong Cellular and Humoral Immune Responses against SARS-CoV-2 in Mice. Immunity 2020, 53, 724–732.e7. [Google Scholar] [CrossRef]
- Lamminen, A.E.; Hekali, P.E.; Tiula, E.; Suramo, I.; Korhola, O.A. Acute rhabdomyolysis: Evaluation with magnetic resonance imaging compared with computed tomography and ultrasonography. Br. J. Radiol. 1989, 62, 326–330. [Google Scholar] [CrossRef]
- Faissner, S.; Richter, D.; Ceylan, U.; Schneider-Gold, C.; Gold, R. COVID-19 mRNA vaccine induced rhabdomyolysis and fasciitis. J. Neurol. 2022, 269, 1774–1775. [Google Scholar] [CrossRef] [PubMed]
- Kamura, Y.; Terao, T.; Akao, S.; Kono, Y.; Honma, K.; Matsue, K. Fatal thrombotic microangiopathy with rhabdomyolysis as an initial symptom after the first dose of mRNA-1273 vaccine: A Case Report. Int. J. Infect. Dis. 2022, 117, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Shintani, S.; Shiigai, T. Repeat MRI in acute rhabdomyolysis: Correlation with clinicopathological findings. J. Comput. Assist. Tomogr. 1993, 17, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.H.; Tsang, Y.M.; Yu, C.W.; Wu, M.Z.; Hsu, C.Y.; Shih, T.T.F. Rhabdomyolysis: Magnetic Resonance Imaging and Computed Tomography Findings. J. Comput. Assist. Tomogr. 2007, 31, 368–374. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
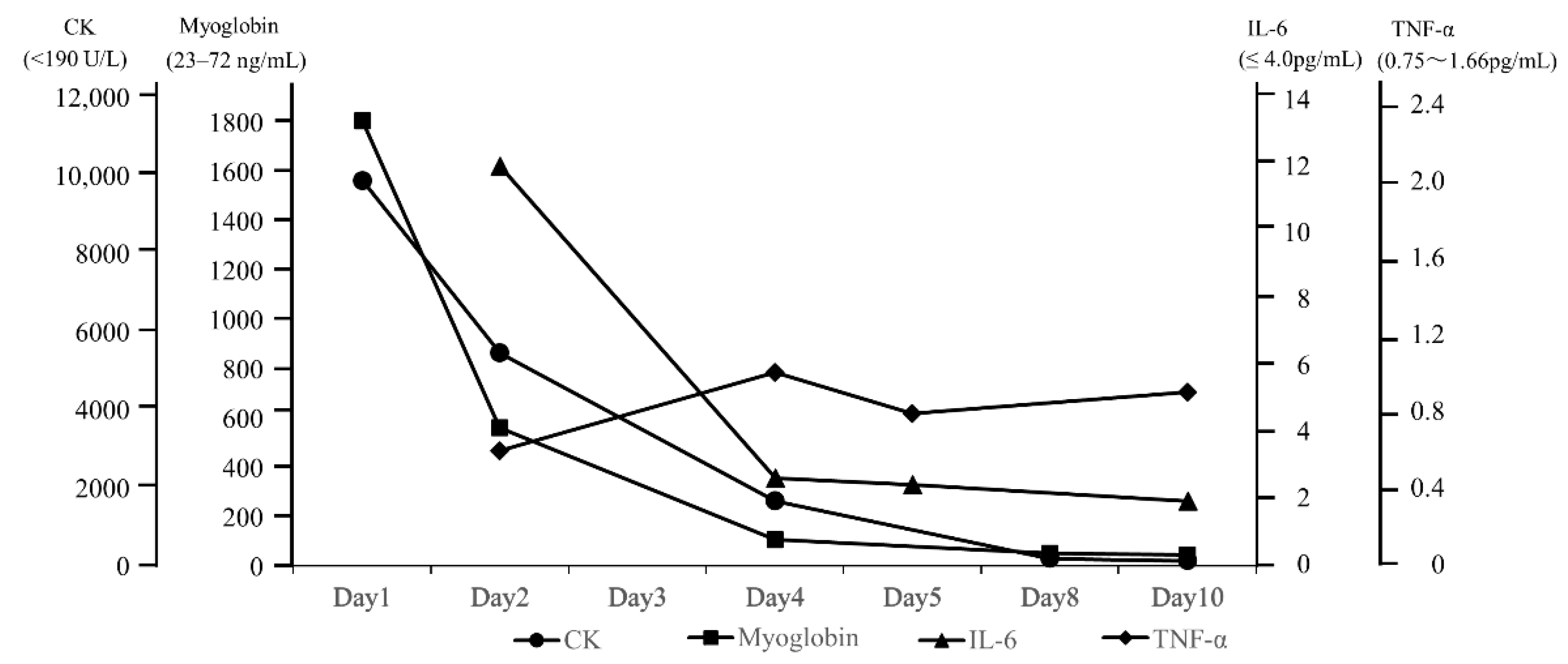
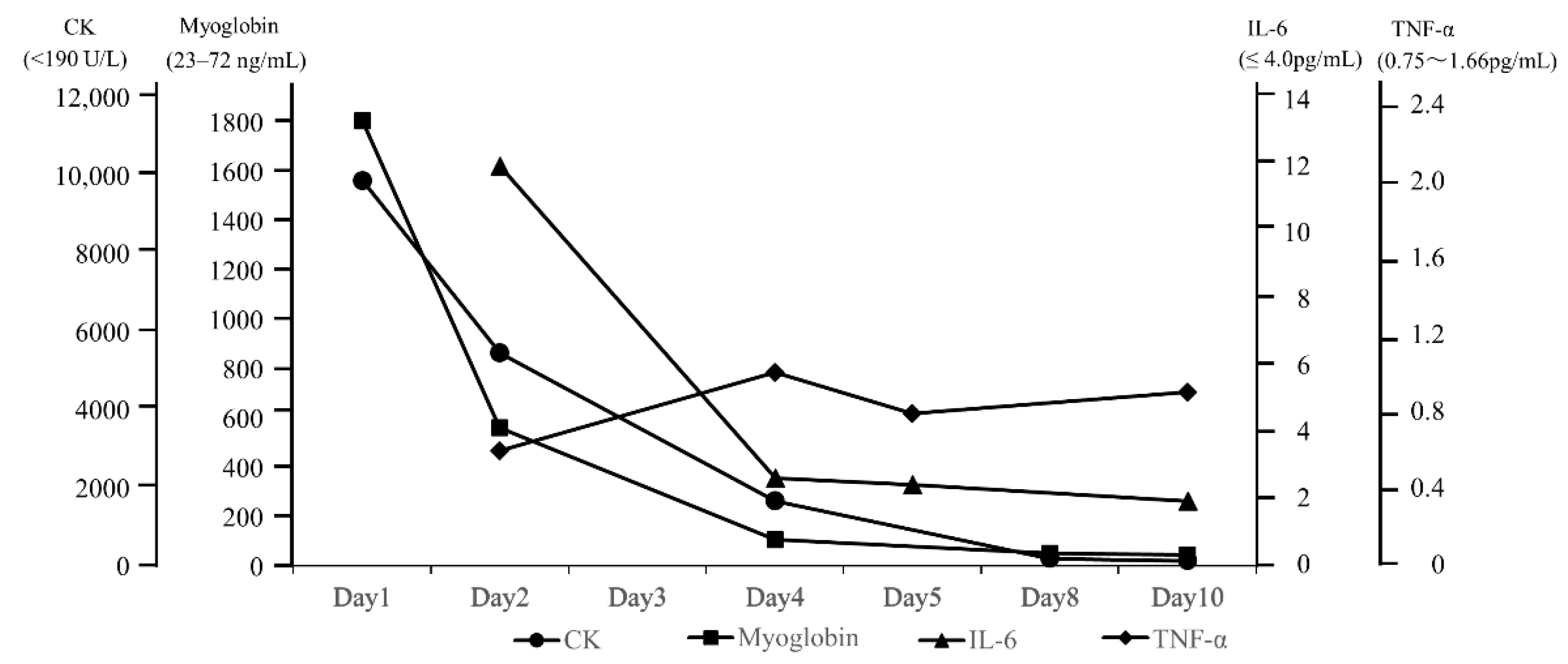
| Parameter | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 8 | Day 10 |
|---|---|---|---|---|---|---|---|
| CK (<190 U/L) | 9816 | 5416 | - | 1630 | - | 164 | 101 |
| Myoglobin (23–72 ng/mL) | 1802 | 559 | - | 106 | - | 52 | 44 |
| IL-6 (≤4.0 pg/mL) | - | 11.9 | - | 2.6 | 2.4 | - | 1.9 |
| IL-1β (≤ 10 pg/mL) | - | ≤10 | - | ≤10 | ≤10 | - | ≤10 |
| TNF-α (0.75–1.66 pg/mL) | - | 0.59 | - | 0.99 | 0.78 | - | 0.89 |
| MRC | iliopsoas 4/4 | iliopsoas 5–/4 | all 5/5 | all 5/5 | supraspinatus and deltoid muscle 5/4 | supraspinatus and deltoid muscle 5/5– | all 5/5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimura, M.; Niwa, J.-I.; Doyu, M. Recurring Weakness in Rhabdomyolysis Following Pfizer–BioNTech Coronavirus Disease 2019 mRNA Vaccination. Vaccines 2022, 10, 935. https://doi.org/10.3390/vaccines10060935
Kimura M, Niwa J-I, Doyu M. Recurring Weakness in Rhabdomyolysis Following Pfizer–BioNTech Coronavirus Disease 2019 mRNA Vaccination. Vaccines. 2022; 10(6):935. https://doi.org/10.3390/vaccines10060935
Chicago/Turabian StyleKimura, Motoya, Jun-Ichi Niwa, and Manabu Doyu. 2022. "Recurring Weakness in Rhabdomyolysis Following Pfizer–BioNTech Coronavirus Disease 2019 mRNA Vaccination" Vaccines 10, no. 6: 935. https://doi.org/10.3390/vaccines10060935
APA StyleKimura, M., Niwa, J.-I., & Doyu, M. (2022). Recurring Weakness in Rhabdomyolysis Following Pfizer–BioNTech Coronavirus Disease 2019 mRNA Vaccination. Vaccines, 10(6), 935. https://doi.org/10.3390/vaccines10060935