
Evaluation of the Humoral Immune Response of a Heterologous Vaccination between BBIBP-CorV and BNT162b2 with a Temporal Separation of 7 Months, in Peruvian Healthcare Workers with and without a History of SARS-CoV-2 Infection

 ,
,  , , , , ,
, , , , ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
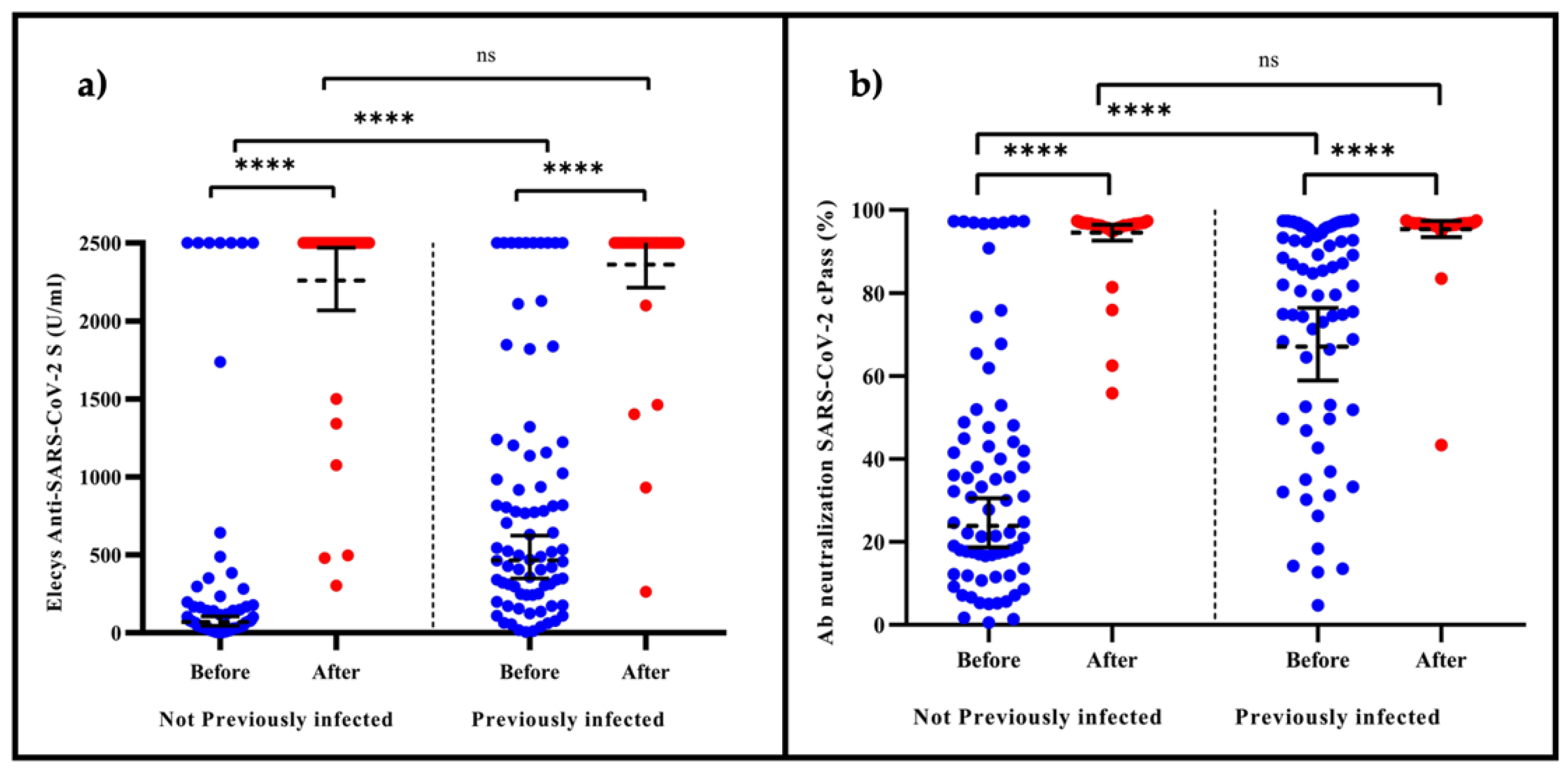
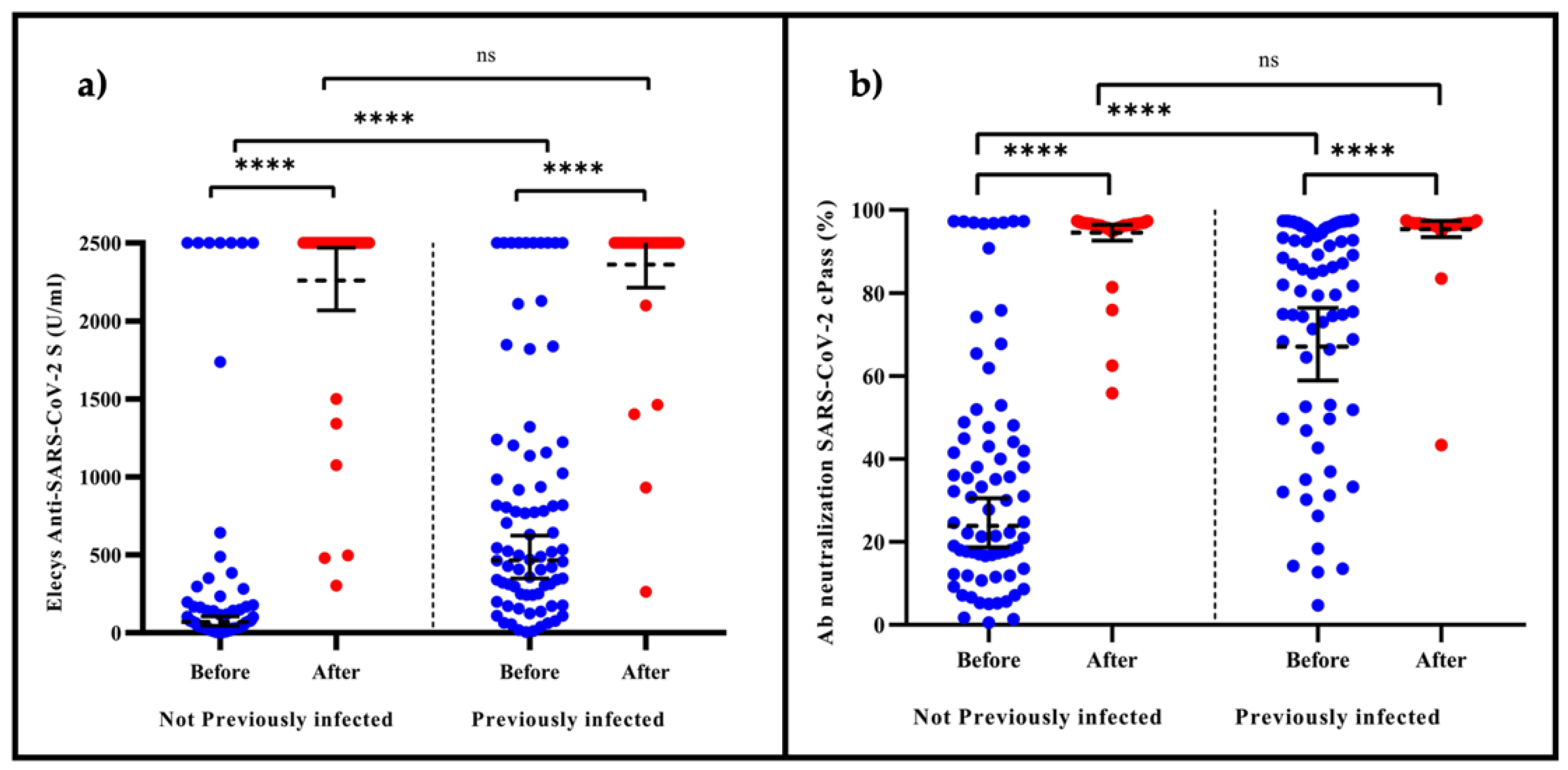
3.1. Elecsys® Anti-SARS-CoV-2 S (Anti-S-RBD IgG)
3.2. cPass™ SARS-CoV-2 Neutralization Antibody
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization WHO Lists 9th COVID-19 Vaccine for Emergency Use with Aim to Increase Access to Vaccination in Lower-Income Countries. Available online: https://www.who.int/news/item/17-12-2021-who-lists-9th-covid-19-vaccine-for-emergency-use-with-aim-to-increase-access-to-vaccination-in-lower-income-countries (accessed on 14 February 2022).
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/covid-cases (accessed on 14 February 2022).
- Al Kaabi, N.; Zhang, Y.; Xia, S.; Yang, Y.; Al Qahtani, M.M.; Abdulrazzaq, N.; Al Nusair, M.; Hassany, M.; Jawad, J.S.; Abdalla, J.; et al. Effect of 2 Inactivated SARS-CoV-2 Vaccines on Symptomatic COVID-19 Infection in Adults: A Randomized Clinical Trial. JAMA 2021, 326, 35. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing Antibody Levels Are Highly Predictive of Immune Protection from Symptomatic SARS-CoV-2 Infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune Correlates Analysis of the MRNA-1273 COVID-19 Vaccine Efficacy Trial; Science: New York, NY, USA, 2021. [Google Scholar]
- Marot, S.; Malet, I.; Leducq, V.; Zafilaza, K.; Sterlin, D.; Planas, D.; Gothland, A.; Jary, A.; Dorgham, K.; Bruel, T.; et al. Rapid Decline of Neutralizing Antibodies against SARS-CoV-2 among Infected Healthcare Workers. Nat. Commun. 2021, 12, 844. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; Navaratnam, A.M.D.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.L.E.; Patel, P.; Kovar, J.; et al. Spike-Antibody Waning after Second Dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, Risk of Hospital Admission, and Vaccine Effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Robles-Fontán, M.M.; Nieves, E.G.; Cardona-Gerena, I.; Irizarry, R.A. Effectiveness estimates of three COVID-19 vaccines based on observational data from Puerto Rico. Lancet Reg. Health Am. 2021, 9, 100212. [Google Scholar] [CrossRef]
- El Peruano Aplicación de Tercera Dosis Contra Virus se Iniciará el 15 de Octubre. Available online: https://elperuano.pe/noticia/130662-aplicacion-de-tercera-dosis-contra-virus-se-iniciara-el-15-de-octubre (accessed on 14 February 2022).
- CPass SARS-CoV-2 Neutralization Antibody Detection Kit—Instructions for Use. 50. Available online: https://www.fda.gov/media/143583/download (accessed on 14 February 2022).
- Riester, E.; Findeisen, P.; Hegel, J.K.; Kabesch, M.; Ambrosch, A.; Rank, C.M.; Pessl, F.; Laengin, T.; Niederhauser, C. Performance Evaluation of the Roche Elecsys Anti-SARS-CoV-2 S Immunoassay. J. Virol. Methods 2021, 297, 114271. [Google Scholar] [CrossRef]
- World Health Organization Guidelines on Clinical Evaluation of Vaccines: Regulatory Expectations. Available online: https://www.who.int/publications/m/item/WHO-TRS-1004-web-annex-9 (accessed on 14 February 2022).
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and Immunogenicity of Seven COVID-19 Vaccines as a Third Dose (Booster) Following Two Doses of ChAdOx1 NCov-19 or BNT162b2 in the UK (COV-BOOST): A Blinded, Multicentre, Randomised, Controlled, Phase 2 Trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Barros-Martins, J.; Hammerschmidt, S.I.; Cossmann, A.; Odak, I.; Stankov, M.V.; Morillas Ramos, G.; Dopfer-Jablonka, A.; Heidemann, A.; Ritter, C.; Friedrichsen, M.; et al. Immune Responses against SARS-CoV-2 Variants after Heterologous and Homologous ChAdOx1 NCoV-19/BNT162b2 Vaccination. Nat. Med. 2021, 27, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to Covid-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef] [PubMed]
- Saciuk, Y.; Kertes, J.; Shamir Stein, N.; Ekka Zohar, A. Effectiveness of a Third Dose of BNT162b2 MRNA Vaccine. J. Infect. Dis. 2022, 225, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Efectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J Med. 2022. Available online: https://doi.org/10.1056/NEJMoa2119451 (accessed on 14 February 2022). [CrossRef] [PubMed]
- Vályi-Nagy, I.; Matula, Z.; Gönczi, M.; Tasnády, S.; Bekő, G.; Réti, M.; Ajzner, É.; Uher, F. Comparison of antibody and T cell responses elicited by BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) vaccines against SARS-CoV-2 in healthy adult humans. Geroscience 2021, 43, 2321–2331. [Google Scholar] [CrossRef]
- Moghnieh, R.; Mekdashi, R.; El-Hassan, S.; Abdallah, D.; Jisr, T.; Bader, M.; Jizi, I.; Sayegh, M.H.; Rahman Bizri, A. Immunogenicity and reactogenicity of BNT162b2 booster in BBIBP-CorV-vaccinated individuals compared with homologous BNT162b2 vaccination: Results of a pilot prospective cohort study from Lebanon. Vaccine 2021, 39, 6713–6719. [Google Scholar] [CrossRef]
- Liu, Y.; Zeng, Q.; Deng, C.; Li, M.; Li, L.; Liu, D.; Liu, M.; Ruan, X.; Mei, J.; Mo, R.; et al. Robust Induction of B Cell and T Cell Responses by a Third Dose of Inactivated SARS-CoV-2 Vaccine. Cell Discov. 2022, 8, 10. [Google Scholar] [CrossRef]
- Costa Clemens, S.A.; Weckx, L.; Clemens, R.; Almeida Mendes, A.V.; Ramos Souza, A.; Silveira, M.B.V.; da Guarda, S.N.F.; de Nobrega, M.M.; de Moraes Pinto, M.I.; Gonzalez, I.G.S.; et al. Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): A phase 4, non-inferiority, single blind, randomised study. Lancet 2022, 399, 521–529. [Google Scholar] [CrossRef]
- Keskin, A.U.; Bolukcu, S.; Ciragil, P.; Topkaya, A.E. SARS-CoV-2 specific antibody responses after third CoronaVac or BNT162b2 vaccine following two-dose CoronaVac vaccine regimen. J. Med. Virol. 2022, 94, 39–41. [Google Scholar] [CrossRef]
- Çağlayan, D.; Süner, A.F.; Şiyve, N.; Güzel, I.; Irmak, Ç.; Işik, E.; Appak, Ö.; Çelik, M.; Öztürk, G.; Alp Çavuş, S.; et al. An analysis of antibody response following the second dose of CoronaVac and humoral response after booster dose with BNT162b2 or CoronaVac among healthcare workers in Turkey. J. Med. Virol. 2022, 11, 27620. [Google Scholar] [CrossRef] [PubMed]
- Yorsaeng, R.; Suntronwong, N.; Phowatthanasathian, H.; Assawakosri, S.; Kanokudom, S.; Thongmee, T.; Vichaiwattana, P.; Auphimai, C.; Wongsrisang, L.; Srimuan, D.; et al. Immunogenicity of a Third Dose Viral-Vectored COVID-19 Vaccine after Receiving Two-Dose Inactivated Vaccines in Healthy Adults. Vaccine 2022, 40, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Then, E.; Lucas, C.; Monteiro, V.S.; Miric, M.; Brache, V.; Cochon, L.; Vogels, C.B.F.; De la Cruz, E.; Jorge, A.; De los Santos, M.; et al. Immunogenicity of Heterologous BNT162b2 Booster in Fully Vaccinated Individuals with CoronaVac against SARS-CoV-2 Variants Delta and Omicron: The Dominican Republic Experience. Available online: https://www.medrxiv.org/content/10.1101/2021.12.27.21268459v1 (accessed on 14 January 2022).

{kind=link}
| Variable | Total (n = 152) | Previously Infected (n = 79) | Not Previously Infected (n = 73) | p-Value |
|---|---|---|---|---|
| Age, years * (IQR) | 34.0 (28–42) | 34 (27–40) | 34 (28–43) | 0.455 a |
| Sex (%) | 0.952 b | |||
| 119 (78.3) | 62 (52.10) | 57 (47.90) | |
| 33 (21.7) | 17 (51.52) | 16 (48.48) | |
| Humoral response rates | ||||
| 7 months after second dose | ||||
| 109 (71.7) | 73 (92.4) | 36 (49.3) | <0.001 c |
| 151 (99.3) | 79 (100) | 72 (98.6) | 0.480 c |
| 40.85 (34.90–47.81) | 67.07 (58.89–76.38) | 23.89 (18.70–30.50) | <0.001 a |
| 186.26 (138.63–250.25) | 466.11 (349.02–622.49) | 69.02 (44.91–106.07) | <0.001 a |
| 21 days after booster | ||||
| 152 (100) | 79 (100) | 73 (100) | 0.999 c |
| 152 (100) | 79 (100) | 73 (100) | 0.999 c |
| 94.99 (93.63–96.36) | 95.40 (93.46–97.38) | 94.54 (92.64–96.48) | 0.520 a |
| 2312.03 (2191.30–2439.42) | 2360.69 (2213.49–2517.67) | 2260 (2068.72–2470.09) | 0.340 a |
| Ab Neutralization SARS-CoV-2 cPass™ after Booster BNT162b2 | ||||
|---|---|---|---|---|
| Variable | Crude β (95% IC) | p-Value | Adjusted β (95% IC) | p-Value |
| Male | 1.564 (−0.939 to 4.068) | 0.219 | 1.569 (−0.937 to 4.076) | 0.218 |
| Previously infected | 0.859 (−1.213 to 2.931) | 0.414 | 0.865 (−1.203 to 2.934) | 0.410 |
| Elecsys® anti-SARS-CoV-2 S after Booster BNT162b2 | ||||
| Variable | Crude β (95% IC) | p-Value | Adjusted β (95% IC) | p-Value |
| Male | 135.669 (−23.051 to 294.390) | 0.093 | 135.989 (−22.914 to 924.892) | 0.093 |
| Previously infected | 54.002 (−77.925 to 185.930) | 0.420 | 54.544 (−76.581 to 185.670) | 0.412 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hueda-Zavaleta, M.; Gómez de la Torre, J.C.; Cáceres-Del Aguila, J.A.; Muro-Rojo, C.; De La Cruz-Escurra, N.; Arenas Siles, D.; Minchón-Vizconde, D.; Copaja-Corzo, C.; Bardales-Silva, F.; Benites-Zapata, V.A.; et al. Evaluation of the Humoral Immune Response of a Heterologous Vaccination between BBIBP-CorV and BNT162b2 with a Temporal Separation of 7 Months, in Peruvian Healthcare Workers with and without a History of SARS-CoV-2 Infection. Vaccines 2022, 10, 502. https://doi.org/10.3390/vaccines10040502
Hueda-Zavaleta M, Gómez de la Torre JC, Cáceres-Del Aguila JA, Muro-Rojo C, De La Cruz-Escurra N, Arenas Siles D, Minchón-Vizconde D, Copaja-Corzo C, Bardales-Silva F, Benites-Zapata VA, et al. Evaluation of the Humoral Immune Response of a Heterologous Vaccination between BBIBP-CorV and BNT162b2 with a Temporal Separation of 7 Months, in Peruvian Healthcare Workers with and without a History of SARS-CoV-2 Infection. Vaccines. 2022; 10(4):502. https://doi.org/10.3390/vaccines10040502
Chicago/Turabian StyleHueda-Zavaleta, Miguel, Juan C. Gómez de la Torre, José Alonso Cáceres-Del Aguila, Cecilia Muro-Rojo, Nathalia De La Cruz-Escurra, Daniella Arenas Siles, Diana Minchón-Vizconde, Cesar Copaja-Corzo, Fabrizzio Bardales-Silva, Vicente A. Benites-Zapata, and et al. 2022. "Evaluation of the Humoral Immune Response of a Heterologous Vaccination between BBIBP-CorV and BNT162b2 with a Temporal Separation of 7 Months, in Peruvian Healthcare Workers with and without a History of SARS-CoV-2 Infection" Vaccines 10, no. 4: 502. https://doi.org/10.3390/vaccines10040502
APA StyleHueda-Zavaleta, M., Gómez de la Torre, J. C., Cáceres-Del Aguila, J. A., Muro-Rojo, C., De La Cruz-Escurra, N., Arenas Siles, D., Minchón-Vizconde, D., Copaja-Corzo, C., Bardales-Silva, F., Benites-Zapata, V. A., & Rodriguez-Morales, A. J. (2022). Evaluation of the Humoral Immune Response of a Heterologous Vaccination between BBIBP-CorV and BNT162b2 with a Temporal Separation of 7 Months, in Peruvian Healthcare Workers with and without a History of SARS-CoV-2 Infection. Vaccines, 10(4), 502. https://doi.org/10.3390/vaccines10040502