
COVID-19 Vaccination Improved Psychological Distress (Anxiety and Depression Scores) in Chronic Kidney Disease Patients: A Prospective Study


 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.1.1. Participants
2.1.2. Instruments
- “Regarding the vaccine, what do you fear most?”
- “Regarding vaccine-related fears, what do you think helps you feel better?”
- “How do you think we can help you from the hospital/hemodialysis clinic?”
- “How would you describe your quality of life in general?”
2.1.3. Procedure
2.2. Sample Size Calculation
2.3. Data Analysis
3. Results
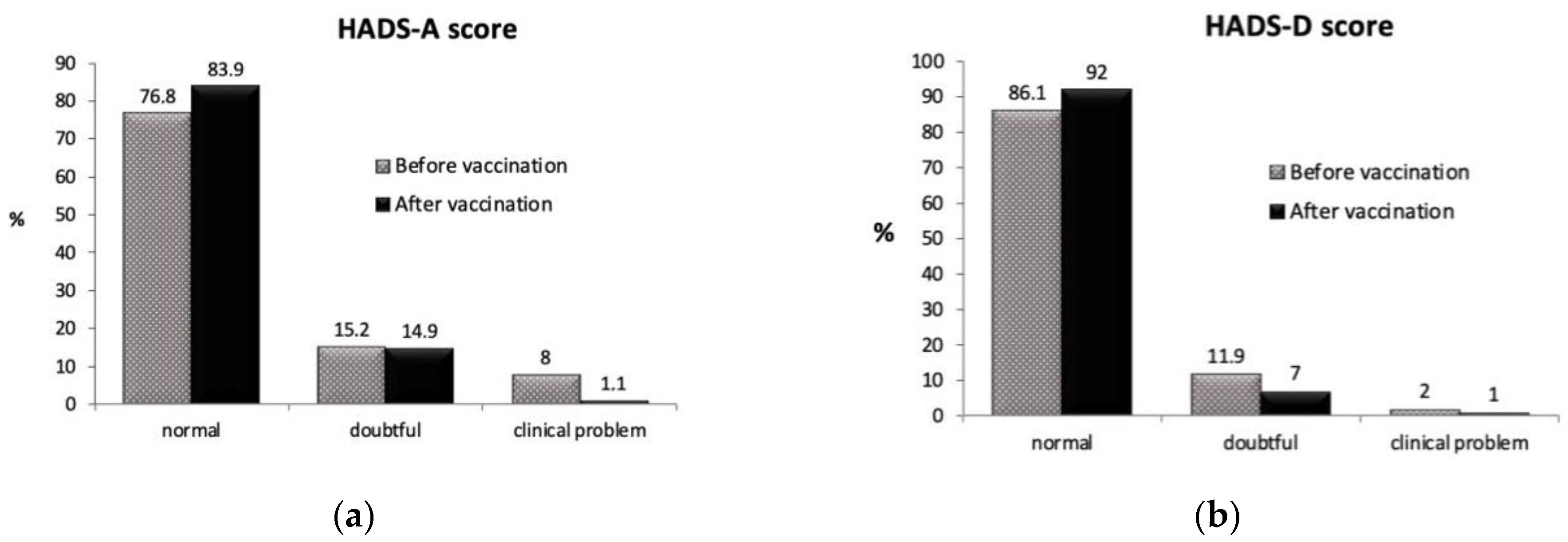
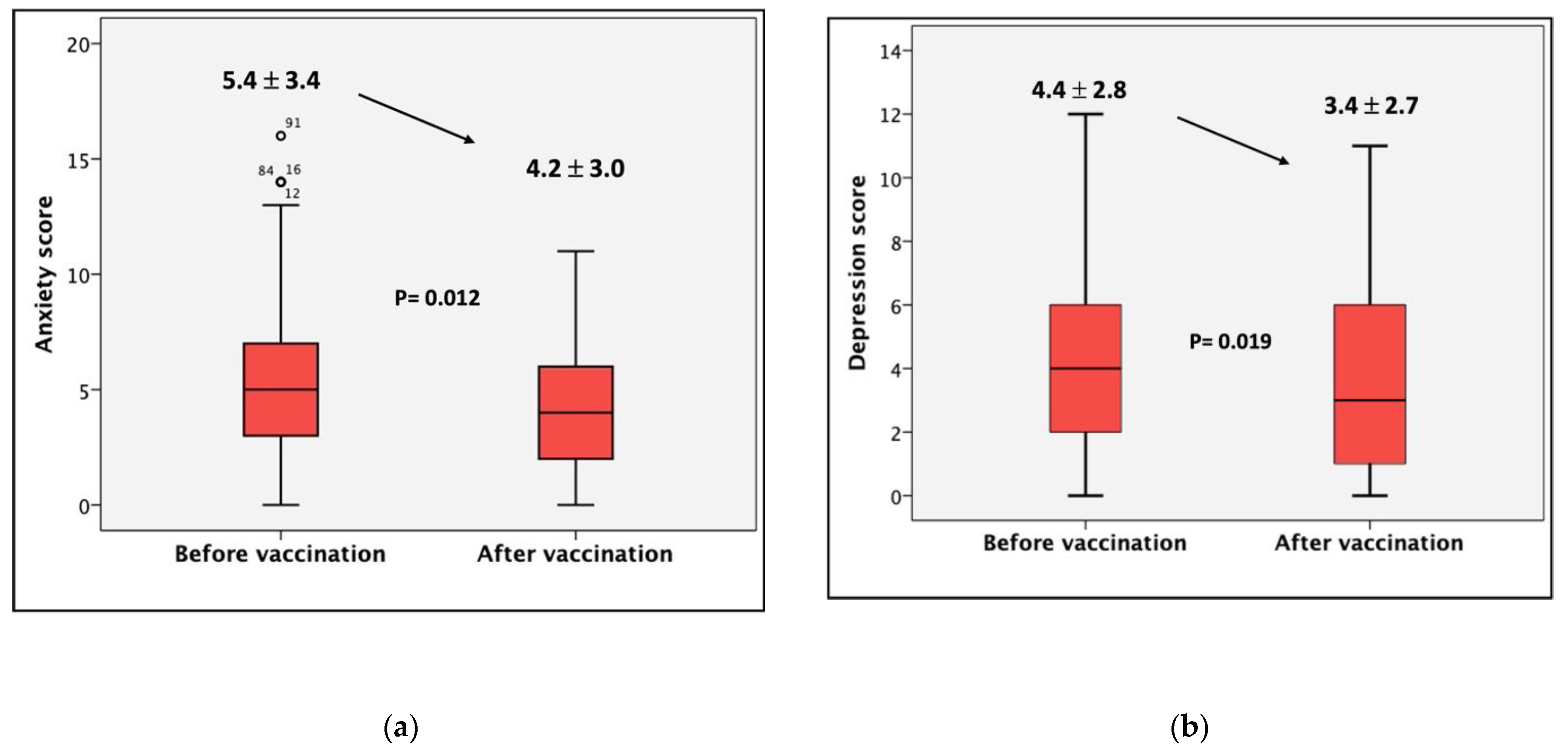
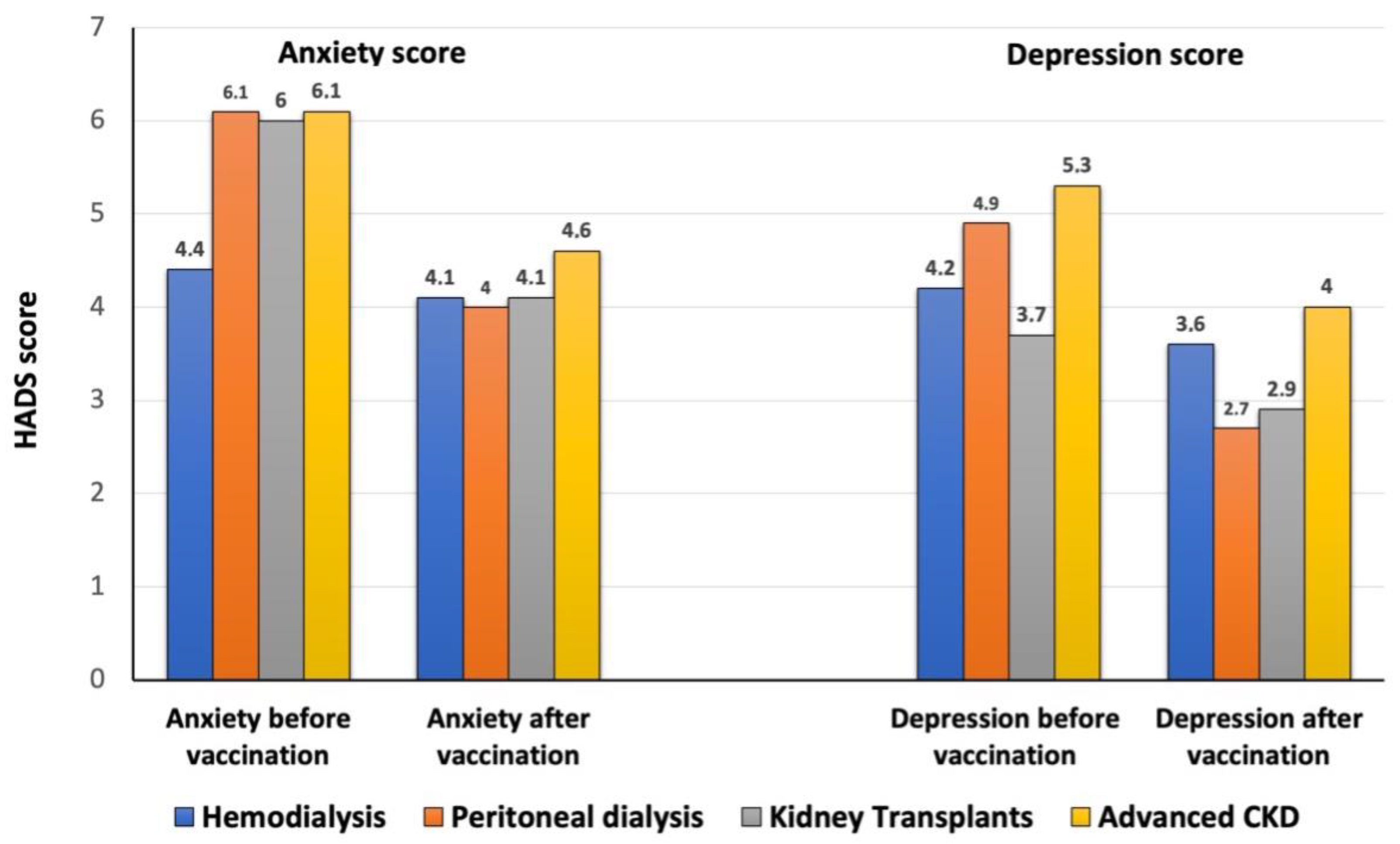
3.1. Psychological Distress and HRQOL Pre and Post Vaccination
3.2. Basal Descriptive Fears, Personal Coping Resources and Coping Resources Demanded of the Healthcare Team
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shelef, L.; Zalsman, G. The psychological impact of COVID-19 on mental health—Literature review. Harefuah 2020, 159, 320–325. [Google Scholar] [PubMed]
- Shafi, S.T.; Shafi, T. A comparison of anxiety and depression between pre-dialysis chronic kidney disease patients and hemodialysis patients using hospital anxiety and depression scale. Pak. J. Med. Sci. 2017, 33, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Zalai, D.; Szeifert, L.; Novak, M. Psychological distress and depression in patients with chronic kidney disease. Semin. Dial. 2012, 25, 428–438. [Google Scholar] [CrossRef]
- Chan, A.S.W.; Ho, J.M.C.; Li, J.S.F.; Tam, H.L.; Tang, P.M.K. Impacts of COVID-19 Pandemic on Psychological Well-Being of Older Chronic Kidney Disease Patients. Front. Med. 2021, 8, 666973. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Hoq, M.; Measey, M.A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2021, 21, e110. [Google Scholar] [CrossRef]
- Guerra, F.; Di Giacomo, D.; Ranieri, J.; Tunno, M.; Piscitani, L.; Ferri, C. Chronic Kidney Disease and Its Relationship with Mental Health: Allostatic Load Perspective for Integrated Care. J. Pers. Med. 2021, 11, 1367. [Google Scholar] [CrossRef]
- De Pasquale, C.; Pistorio, M.L.; Veroux, M.; Indelicato, L.; Biffa, G.; Bennardi, N.; Zoncheddu, P.; Martinelli, V.; Giaquinta, A.; Veroux, P. Psychological and Psychopathological Aspects of Kidney Transplantation: A Systematic Review. Front. Psychiatry 2020, 11, 106. [Google Scholar] [CrossRef] [Green Version]
- Iida, H.; Fujimoto, S.; Wakita, T.; Yanagi, M.; Suzuki, T.; Koitabashi, K.; Yazawa, M.; Kawarazaki, H.; Ishibashi, Y.; Shibagaki, Y.; et al. Psychological Flexibility and Depression in Advanced CKD and Dialysis. Kidney Med. 2020, 2, 684–691. [Google Scholar] [CrossRef]
- Villanego, F.; Mazuecos, A.; Pérez-Flores, I.M.; Moreso, F.; Andrés, A.; Jiménez-Martín, C.; Molina, M.; Canal, C.; Sanchez-Camara, L.A.; Zarraga, S.; et al. Predictors of severe COVID-19 in kidney transplant recipients in the different epidemic waves: Analysis of the Spanish Registry. Am. J. Transplant. 2021, 21, 2573–2582. [Google Scholar] [CrossRef]
- Nakanishi, T.; Pigazzini, S.; Degenhardt, F.; Cordioli, M.; Butler-Laporte, G.; Maya-Miles, D.; Bujanda, L.; Bouysran, Y.; Niemi, M.E.; Palom, A.; et al. Age-dependent impact of the major common genetic risk factor for COVID-19 on severity and mortality. J. Clin. Investig. 2021, 131, e152386. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Untas, A.; Aguirrezabal, M.; Chauveau, P.; Leguen, E.; Combe, C.; Rascle, N. Anxiety and depression in hemodialysis: Validation of the Hospital Anxiety and Depression Scale (HADS). Nephrol. Ther. 2009, 5, 193–200. [Google Scholar] [CrossRef]
- Quintana, J.M.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the psychometric characteristics of the Spanish version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, P.L.; Emont, S.L.; Newmann, J.M.; Danko, H.; Moss, A.H. ESRD patient quality of life: Symptoms, spiritual beliefs, psychosocial factors, and ethnicity. Am. J. Kidney Dis. 2003, 42, 713–721. [Google Scholar] [CrossRef]
- Schouten, R.W.; Nadort, E.; van Ballegooijen, W.; Loosman, W.L.; Honig, A.; Siegert, C.E.H.; Meuleman, Y.; Broekman, B.F.P. General distress and symptoms of anxiety and depression: A factor analysis in two cohorts of dialysis patients. Gen. Hosp. Psychiatry 2020, 65, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Kader, K.; Unruh, M.L.; Weisbord, S.D. Sympton burden, depression and quality of life in chronic and end-stage kidney disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 1057–1064. [Google Scholar] [CrossRef]
- Rodríguez-Fructuoso, M.; Castro, R.; Oliveira, I.; Prata, C.; Morgado, T. Quality of life in chronic kidney disease. Nefrología 2011, 31, 91–96. [Google Scholar] [CrossRef]
- Justo-Alonso, A.; García-Dantas, A.; González-Vázquez, A.I.; Sánchez-Martín, M.; del Río-Casanova, L. How did Different Generations Cope with the COVID-19 Pandemic? Early Stages of the Pandemic in Spain. Psicothema 2021, 32, 490–500. [Google Scholar]
- Fernández-Ballesteros, R.; Sánchez-Izquierdo Alonso, M. Impacto del COVID-19 en personas mayores en España: Algunos resultados y reflexiones. Clínica Salud 2020, 31, 165–169. [Google Scholar] [CrossRef]
- García-Llana, H.; Remor, E.; del Peso, G.; Celadilla, O.; Selgas, R. Motivational Interviewing promotes adherence and improves wellbeing in pre-dyalisis patients with Advanced Chronic Kidney Disease. J. Clin. Psychol. Med. Setting 2014, 21, 103–115. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Strand, H.; Parker, D. Effects of multidisciplinary models of care for adult pre-dialysis patients with chronic kidney disease: A systematic review. Int. J. Evid.-Based Healthc. 2012, 10, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Arshad, M.S.; Hussain, I.; Mahmood, T.; Hayat, K.; Majeed, A.; Imran, I.; Saeed, H.; Iqbal, M.O.; Uzair, M.; Rehman, A.U.; et al. A National Survey to Assess the COVID-19 Vaccine-Related Conspiracy Beliefs, Acceptability. Preference, and willingness to pay among the General population of Pakistan. Vaccines 2021, 9, 720. [Google Scholar] [CrossRef] [PubMed]
- El-Elimat, T.; Abu AlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and attitudes toward COVID-19 vaccines: A crosssectional study from Jordan. PLoS ONE 2021, 16, e0250555. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| HD | PD | KT | CKD 4/5 | p | |
|---|---|---|---|---|---|
| Age | 70 (65–76.2) | 71 (57.5–76) | 60 (53–71.7) | 65 (56.7–73) | 0.32 |
| Sex (male) n (%) | 34 (68) | 11 (84.6) | 21 (65.6) | 13 (59.1) | 0.47 |
| Previous COVID-19 | 4 (8) | 1 (7.7) | 2 (6.5) | 0 | 0.69 |
| Type 2 diabetes mellitus | 20 (60) | 5 (38.5) | 7 (21.9) | 8 (36.4) | 0.38 |
| Hypertension | 42 (84) | 11 (84.6) | 27 (84.4) | 17 (77.3) | 0.89 |
| Cardiopathy | 18 (36) | 6 (46) | 3 (9.4) | 3 (13.6) | 0.08 |
| Liver disease | 4 (8) | 0 | 0 | 0 | 0.13 |
| Dialysis vintage | 35 (14–66) | 10 (2–20.5) | 48.5 (25–84) | 65 (56.7–73) | 0.89 |
| Kidney transplant vintage | 29 (14–38.5) |
| “Regarding Vaccine, What Do You Fear Most?” | n (%) |
|---|---|
| Nothing Adverse effects (i.e., thrombus) | 44 (44.9) 34 (34.7) |
| Not having access to vaccine and get infected Lack of information | 12 (12.2) 5 (5.1) |
| Vaccine brand | 3 (3.1) |
| “Regarding Vaccine Related Fears, What Do You Think Helps You Feel Better?” | n (%) |
|---|---|
| Family and friends The vaccine itself | 47 (46.5) 15 (14.9) |
| Music, books and watching TV series Nature and walks | 12 (11.9) 9 (8.9) |
| Trust in my healthcare team Physical activity No listening to the news Work | 6 (5.9) 6 (5.9) 4 (4) 2 (2) |
| “How Do You Think We Can Help You from the Hospital/Hemodialysis Clinic?” | n (%) |
|---|---|
| They are already doing it Personalized information, kindness, and close communication | 53 (50) 31 (29.2) |
| Facilitating vaccine access Research | 14 (13.2) 8 (7.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Llana, H.; Panizo, N.; Gandía, L.; Orti, M.; Giménez-Civera, E.; Forquet, C.; D’Marco, L.; Puchades, M.J.; Sargsyan, M.; Sanchís, I.; et al. COVID-19 Vaccination Improved Psychological Distress (Anxiety and Depression Scores) in Chronic Kidney Disease Patients: A Prospective Study. Vaccines 2022, 10, 299. https://doi.org/10.3390/vaccines10020299
Garcia-Llana H, Panizo N, Gandía L, Orti M, Giménez-Civera E, Forquet C, D’Marco L, Puchades MJ, Sargsyan M, Sanchís I, et al. COVID-19 Vaccination Improved Psychological Distress (Anxiety and Depression Scores) in Chronic Kidney Disease Patients: A Prospective Study. Vaccines. 2022; 10(2):299. https://doi.org/10.3390/vaccines10020299
Chicago/Turabian StyleGarcia-Llana, Helena, Nayara Panizo, Lorena Gandía, Marisa Orti, Elena Giménez-Civera, Claudia Forquet, Luis D’Marco, Maria Jesús Puchades, Mari Sargsyan, Irina Sanchís, and et al. 2022. "COVID-19 Vaccination Improved Psychological Distress (Anxiety and Depression Scores) in Chronic Kidney Disease Patients: A Prospective Study" Vaccines 10, no. 2: 299. https://doi.org/10.3390/vaccines10020299
APA StyleGarcia-Llana, H., Panizo, N., Gandía, L., Orti, M., Giménez-Civera, E., Forquet, C., D’Marco, L., Puchades, M. J., Sargsyan, M., Sanchís, I., Ribera, C., Marco, M. I., Ferrá, C. M., Pérez-Baylach, C. M., Bonilla, B., Moncho Francés, F., Perez-Bernat, E., Sancho, A., & Górriz, J. L. (2022). COVID-19 Vaccination Improved Psychological Distress (Anxiety and Depression Scores) in Chronic Kidney Disease Patients: A Prospective Study. Vaccines, 10(2), 299. https://doi.org/10.3390/vaccines10020299