
Effectiveness of COVID-19 Vaccination Mandates and Incentives in Europe

Abstract
:1. Introduction
2. Methods
2.1. Policy Interventions
2.2. Data Sources
2.3. Population
2.4. Outcome
2.5. Statistical Analysis
3. Results
3.1. Austria
3.2. Greece
3.3. Italy
3.4. Norway
3.5. Poland
3.6. Russia
3.7. Spain
3.8. United Kingdom
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dial Down the Vaccine Rhetoric. Springer Nat Ltd. Available online: https://www.nature.com/articles/d41586-021-00769-7 (accessed on 15 August 2022).
- Aljazeera. Anti-vaccine Protesters Rally in France, Germany, Austria, Italy. Available online: https://www.aljazeera.com/news/2022/1/9/more-than-100000-rally-in-france-against-covid-vaccine-rules (accessed on 15 August 2022).
- The Guardian. Italy Braced for Unrest as Covid Pass Becomes Mandatory for all Workers. Available online: https://www.theguardian.com/world/2021/oct/14/italy-braced-for-unrest-as-covid-pass-becomes-mandatory-for-all-workers (accessed on 15 August 2022).
- DW News. COVID Digest: Austria Lifts Lockdown for the Unvaccinated. Available online: https://www.dw.com/en/covid-digest-austria-lifts-lockdown-for-the-unvaccinated/a-60554450 (accessed on 15 August 2022).
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The unintended consequences of COVID-19 vaccine policy: Why mandates, passports and restrictions may cause more harm than good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing—29 June 2022. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing---29-june-2022 (accessed on 15 August 2022).
- Barcelona Institute for Global Health. How Can We Be Better Prepared for the Next Public Health Crisis? Lessons Learned from the COVID-19 Pandemic. An ISGlobal Policy Paper. Available online: https://www.isglobal.org/en/-/how-can-we-be-better-prepared-for-the-next-public-health-crisis-lessons-learned-from-the-covid-19-pandemic (accessed on 15 August 2022).
- World Health Organization. WHO Director-General Declares the Ongoing Monkeypox Outbreak a Public Health Emergency of International Concern. Available online: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern (accessed on 15 August 2022).
- World Health Organization. Severe Acute Hepatitis of Unknown Aetiology in Children—Multi-Country. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON394 (accessed on 15 August 2022).
- Kuznetsova, L.; Cortassa, G.; Trilla, A. Effectiveness of Mandatory and Incentive-Based Routine Childhood Immunization Programs in Europe: A Systematic Review of the Literature. Vaccines 2021, 9, 1173. [Google Scholar] [CrossRef] [PubMed]
- United Nations Children’s Fund. UNICEF and WHO Warn of “Perfect storm” of Conditions for Measles Outbreaks, Affecting Children. Available online: https://www.unicef.org/press-releases/unicef-and-who-warn-perfect-storm-conditions-measles-outbreaks-affecting-children (accessed on 15 August 2022).
- Mills, M.C.; Rüttenauer, T. The Effect of Mandatory COVID-19 Certificates on Vaccine Uptake: Synthetic-Control Modelling of Six Countries. Lancet Public Health 2022, 7, e15–e22. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Rabin, K.; Ratzan, S.C.; Leigh, J.P.; Hu, J.; El-Mohandes, A. Revisiting COVID-19 Vaccine Hesitancy Around the World Using Data from 23 Countries in 2021. Nat. Commun. 2022, 13, 3801. [Google Scholar] [CrossRef] [PubMed]
- Salomoni, M.G.; Di Valerio, Z.; Gabrielli, E.; Montalti, M.; Tedesco, D.; Guaraldi, F.; Gori, D. Hesitant or Not Hesitant? A Systematic Review on Global COVID-19 Vaccine Acceptance in Different Populations. Vaccines 2021, 9, 873. [Google Scholar] [CrossRef] [PubMed]
- Gallup, Inc. Over 1 Billion Worldwide Unwilling to Take COVID-19 Vaccine. Available online: https://news.gallup.com/poll/348719/billion-unwilling-COVID-vaccine.aspx (accessed on 15 August 2022).
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus (accessed on 3 September 2022).
- European Centre for Disease Prevention and Control. COVID-19 Vaccine Tracker. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#age-group-tab (accessed on 15 August 2022).
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, A.L.; Dobbins, T.A.; Pearson, S.A. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: A guide for evaluating large-scale health interventions. BMC Med. Res. Methodol. 2021, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Achcar, J.A.; de Oliveira, R.P.; Barili, E. Use of Stochastic Volatility Models in Epidemiological Data: Application to a Dengue Time Series in São Paulo City, Brazil. J. Biostat. Epidemiol. 2020, 6, 19–29. [Google Scholar]
- GitHub. Data on COVID-19 Vaccinations by Our World in Data. Available online: https://github.com/owid/covid-19-data/tree/master/public/data/vaccinations (accessed on 15 August 2022).
- Desson, Z.; Kauer, L.; Otten, T.; Peters, J.W.; Paolucci, F. Finding the way forward: COVID-19 vaccination progress in Germany, Austria and Switzerland. Health Policy Technol. 2022, 11, 100584. [Google Scholar] [CrossRef] [PubMed]
- Kloiber, K.; Peichl, A.; William, H. “Schnitzel Scare” as a Boost for Vaccines? The Impact of 2G Rules and Lockdowns on Vaccination Rates in Austria. Ifo Schnelld. Digit. 2021, 18, 1–5. [Google Scholar]
- Liam Drew. Did COVID Vaccine Mandates Work? What the Data Say. Available online: https://www.nature.com/articles/d41586-022-01827-4 (accessed on 15 August 2022).
- Sky Tg24. Vaccino Covid, Terza Dose: Come Stanno Andando le Somministrazioni Nelle Regioni. Available online: https://tg24.sky.it/cronaca/2021/11/24/vaccino-covid-terza-dose (accessed on 3 September 2022).
- Sky Tg24. Vaccino Covid ai Bambini 5-11 Anni, Date di Prenotazione Regione per Regione e Cosa Sapere. Available online: https://tg24.sky.it/salute-e-benessere/2021/12/12/covid-vaccino-bambini-prenotazione-cosa-sapere (accessed on 3 September 2022).
- Karaivanov, A.; Kim, D.; Lu, S.E.; Shigeoka, H. COVID-19 vaccination mandates and vaccine uptake. Nat. Hum. Behav. 2022, 2, 1–10. [Google Scholar]
- Oliu, M.; Pradelski, B.S.R.; Woloszko, N.; Aghion, P.; Artus, P.; Fontanet, A. The Effect of COVID Certificates on Vaccine Uptake, Health Outcomes, and the Economy. Nat Commun. 2022, 13, 3942. [Google Scholar] [CrossRef] [PubMed]
- Folkehelseinstituttet. COVID-19 Vaccination Calendar. Available online: https://www.fhi.no/contentassets/71e97765e43c41ee8f059efbd4016ca8/vedlegg/2021.08.13-vaccination-calendar.pdf (accessed on 15 August 2022).
- Rzeczpospolita. Vaccination Points will be Closed. Fewer and Fewer People are Willing to be Vaccinated Against COVID-19. Available online: https://www.rp.pl/swiat/art56371-punkty-szczepien-beda-zamykane-coraz-mniej-chetnych-na-szczepienie-na-covid-19 (accessed on 15 August 2022).
- Barber, A.; West, J. Conditional cash lotteries increase COVID-19 vaccination rates. J. Health Econ. 2022, 81, 102578. [Google Scholar] [CrossRef] [PubMed]
- Dziennik Gazeta Prawna. Vaccines are Going from Poland to the East. Available online: https://serwisy.gazetaprawna.pl/zdrowie/artykuly/8208328,szczepionki-z-polski-partnerstwo-wschodnie-ukraina-gruzja.html (accessed on 15 August 2022).
- Interfax. The Authorities of St. Petersburg Obliged to Vaccinate 65% of Officials by August 15. Available online: https://www.interfax.ru/russia/772966 (accessed on 15 August 2022).
- Federal Service for Surveillance on Consumer Rights Protection and Human Wellbeing. Preventive Vaccinations for Certain Groups of Population According to Epidemic Indications. Available online: https://77.rospotrebnadzor.ru/images/Postanovlenie_Andreevoy1506.PDF?p=1210&utm_source=google&utm_medium=organic&utm_startpage=kontur.ru%2Farticles%2F6071&utm_orderpage=kontur.ru%2Farticles%2F6071 (accessed on 15 August 2022).
- Information Portal of Sverdlovsk Region. Sverdlovsk Region Received a Record Amount of Vaccine. Available online: https://xn--b1ag8a.xn--p1ai/news/12767 (accessed on 15 August 2022).
- Izvestia. Vaccinate with an Iron Fist: Could Vaccination Become Mandatory? Available online: https://iz.ru/1247895/anastasiia-platonova/privit-zheleznoi-rukoi-mozhet-li-vaktcinatciia-stat-obiazatelnoi (accessed on 15 August 2022).
- TASS. Mandatory Vaccination for Residents over 60 Introduced in 12 Regions. Available online: https://tass.ru/obschestvo/12896903?utm_source=google.com&utm_medium=organic&utm_campaign=google.com&utm_referrer=google.com (accessed on 15 August 2022).
- Tvzvezda. The Ministry of Health Proposed to Encourage Doctors Involved in Vaccination. Available online: https://tvzvezda.ru/news/202111162136-mRHMx.html (accessed on 15 August 2022).
- Vesti. Covid Bans in the Regions of Russia: What You Need to Know before Planning a Vacation. Available online: https://www.vesti.ru/article/2658806 (accessed on 15 August 2022).
- El portal de las vacunas de la Asociación Española de Pediatría. Evolución de la Vacunación Frente a la COVID de Niños y Adolescentes en España. Available online: https://vacunasaep.org/profesionales/noticias/evolucion-de-la-vacunacion-frente-la-covid-de-ninos-y-adolescentes-en-espana-99#:~:text=La%20vacunaci%C3%B3n%20de%20los%20adolescentes,23%20de%20julio%20de%202021 (accessed on 15 August 2022).
- Las Provincias. La Vacunación Sin Cita Previa Arranca Con Colas Interminables en el Centro Comercial Arena de Valencia. Available online: https://www.lasprovincias.es/comunitat/vacunarse-cita-previa-20211210172829-nt.html (accessed on 15 August 2022).
- RTVE. El Pasaporte COVID Inyecta Ritmo a la Vacunación en España, que entra en las Navidades Subida a la Sexta ola. Available online: https://www.rtve.es/noticias/20211211/pasaporte-covid-vacunacion-dosis-espana-claves-datos/2237729.shtml (accessed on 15 August 2022).
- GOV.UK. JCVI Statement Regarding a COVID-19 Booster Vaccine Programme for Winter 2021 to 2022. Available online: https://www.gov.uk/government/publications/jcvi-statement-september-2021-covid-19-booster-vaccine-programme-for-winter-2021-to-2022/jcvi-statement-regarding-a-covid-19-booster-vaccine-programme-for-winter-2021-to-2022 (accessed on 15 August 2022).
- The Official UK Government Website for Data and Insights on COVID-19. Vaccinations in England. Available online: https://coronavirus.data.gov.uk/details/vaccinations?areaType=nation&areaName=England (accessed on 15 August 2022).
 Announcement of employees vaccine mandate (am1).
Announcement of employees vaccine mandate (am1).  Employees mandate in force (m1force).
Employees mandate in force (m1force).  Lockdown for unvaccinated (m2).
Lockdown for unvaccinated (m2).  Announcement of universal mandate with fines (am3).
Announcement of universal mandate with fines (am3).  Predicted values in absence of announcement of the universal vaccine mandate (am3).
Announcement of employees vaccine mandate (am1). Employees mandate in force (m1force). Lockdown for unvaccinated (m2). Announcement of universal mandate with fines (am3). Predicted values in absence of announcement of the universal vaccine mandate (am3).
Predicted values in absence of announcement of the universal vaccine mandate (am3).
Announcement of employees vaccine mandate (am1). Employees mandate in force (m1force). Lockdown for unvaccinated (m2). Announcement of universal mandate with fines (am3). Predicted values in absence of announcement of the universal vaccine mandate (am3).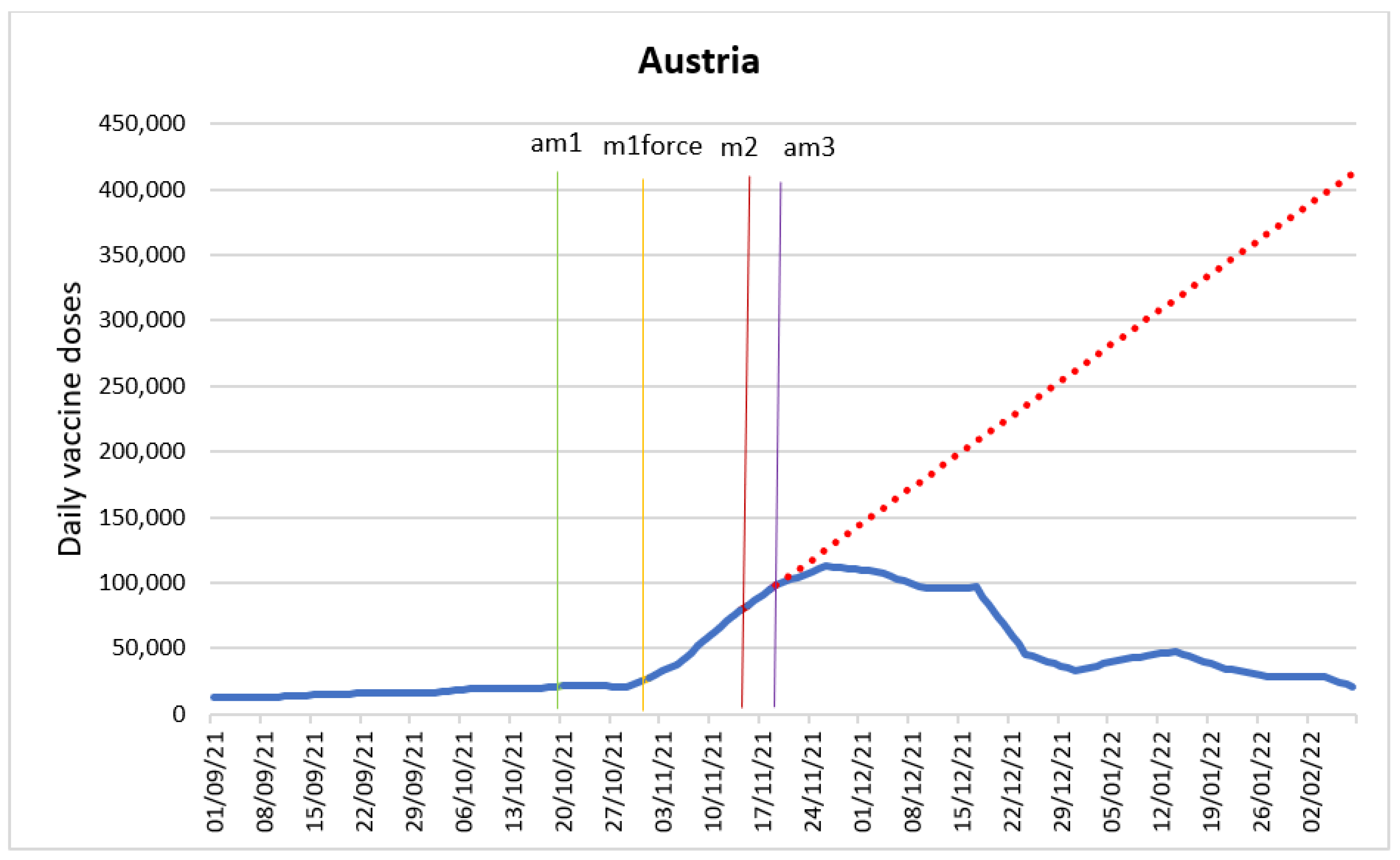
 Announcement of “freedom pass” (am1)
Announcement of “freedom pass” (am1)  Introduction of “freedom pass” (m1force)
Introduction of “freedom pass” (m1force)  Financial incentives for pharmacists and doctors (m2)
Financial incentives for pharmacists and doctors (m2)  Introduction of COVID certificates (m3)
Introduction of COVID certificates (m3)  Announcement of vaccine mandates for adults aged 60 and older (am4)
Announcement of vaccine mandates for adults aged 60 and older (am4)  Vaccine mandate for adults aged 60 and older in force (m4force)
Vaccine mandate for adults aged 60 and older in force (m4force)  Predicted values in absence of COVID certificates
Predicted values in absence of COVID certificates  Predicted values in absence of entry into force of the vaccine mandate for adults aged 60 and older.
Announcement of “freedom pass” (am1) Introduction of “freedom pass” (m1force) Financial incentives for pharmacists and doctors (m2) Introduction of COVID certificates (m3) Announcement of vaccine mandates for adults aged 60 and older (am4) Vaccine mandate for adults aged 60 and older in force (m4force) Predicted values in absence of COVID certificates Predicted values in absence of entry into force of the vaccine mandate for adults aged 60 and older.
Predicted values in absence of entry into force of the vaccine mandate for adults aged 60 and older.
Announcement of “freedom pass” (am1) Introduction of “freedom pass” (m1force) Financial incentives for pharmacists and doctors (m2) Introduction of COVID certificates (m3) Announcement of vaccine mandates for adults aged 60 and older (am4) Vaccine mandate for adults aged 60 and older in force (m4force) Predicted values in absence of COVID certificates Predicted values in absence of entry into force of the vaccine mandate for adults aged 60 and older.
 Introduction of “Green pass” mandate for employees (m1)
Introduction of “Green pass” mandate for employees (m1)  Introduction of vaccine mandate for adults aged 50 and older (m2)
Introduction of vaccine mandate for adults aged 50 and older (m2)  Predicted values in absence of entry into force of the vaccine mandate for adults aged 50 and older.
Introduction of “Green pass” mandate for employees (m1) Introduction of vaccine mandate for adults aged 50 and older (m2) Predicted values in absence of entry into force of the vaccine mandate for adults aged 50 and older.
Predicted values in absence of entry into force of the vaccine mandate for adults aged 50 and older.
Introduction of “Green pass” mandate for employees (m1) Introduction of vaccine mandate for adults aged 50 and older (m2) Predicted values in absence of entry into force of the vaccine mandate for adults aged 50 and older.
 Introduction of COVID certificates (m1).
Introduction of COVID certificates (m1).
Introduction of COVID certificates (m1).
Introduction of COVID certificates (m1).
 Start of national lottery and municipality competitions (m1).
Start of national lottery and municipality competitions (m1).
Start of national lottery and municipality competitions (m1).
Start of national lottery and municipality competitions (m1).
 Introduction of employees vaccine mandate (m1)
Introduction of employees vaccine mandate (m1)  Lottery for the vaccinated (m2)
Lottery for the vaccinated (m2)  Announcement of the introduction of COVID certificates (am3)
Announcement of the introduction of COVID certificates (am3)  COVID certificates in force (m3force)
COVID certificates in force (m3force)  Predicted values in absence of the announcement of COVID certificates.
Introduction of employees vaccine mandate (m1) Lottery for the vaccinated (m2) Announcement of the introduction of COVID certificates (am3) COVID certificates in force (m3force) Predicted values in absence of the announcement of COVID certificates.
Predicted values in absence of the announcement of COVID certificates.
Introduction of employees vaccine mandate (m1) Lottery for the vaccinated (m2) Announcement of the introduction of COVID certificates (am3) COVID certificates in force (m3force) Predicted values in absence of the announcement of COVID certificates.
 Announcement of the introduction of COVID certificates (m1)
Announcement of the introduction of COVID certificates (m1)  COVID certificates in force (m2).
Announcement of the introduction of COVID certificates (m1) COVID certificates in force (m2).
COVID certificates in force (m2).
Announcement of the introduction of COVID certificates (m1) COVID certificates in force (m2).
 Introduction of discounts and vouchers for the vaccinated (m1).
Introduction of discounts and vouchers for the vaccinated (m1).
Introduction of discounts and vouchers for the vaccinated (m1).
Introduction of discounts and vouchers for the vaccinated (m1).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Measure Description | Announced | Introduced | Suspended | Selected Sources |
|---|---|---|---|---|---|
| Austria | Introduction of a general requirement for ‘3G’ proof to enter the workplace. The ‘3Gs’ are ‘geimpft, genesen oder getestet’ (abbreviated as 3G as all three words start with a G in German) meaning vaccinated, recovered or tested. | 20 October 2021 | 1 November 2021 | March 2022 | https://www.thelocal.at/20220223/austria-to-lift-3g-requirement-for-workplaces/ (accessed on 15 August 2022) |
| Lockdown for the unvaccinated. Unvaccinated people in Austria will be allowed to leave their homes only for work, food shopping or emergencies. | 15 November 2021 | 15 November 2021 | 19 November 2021 | https://www.bbc.com/news/world-europe-59343650 (accessed on 15 August 2022) https://www.npr.org/sections/coronavirus-live-updates/2021/11/15/1055839727/austria-and-germany-impose-restrictions-on-unvaccinated-people-as-covid-cases-su (accessed on 15 August 2022) | |
| Universal mandate with fines announced. Those over the age of 18 who decline to take a jab face penalty of up to 3600 EUR, unless they are pregnant or severely ill. | 19 November 2021 | February 2022 | March 2022 | https://www.theguardian.com/world/2022/mar/09/austria-suspends-mandatory-covid-vaccination-law (accessed on 15 August 2022) https://www.bnnbloomberg.ca/austria-suspends-vaccine-mandate-as-omicron-questions-policy-1.1734807 (accessed on 15 August 2022) | |
| Greece | “Freedom pass”—150 EUR voucher offered to people 18–25 years old who get vaccinated. | 28 June 2021 | 20 July 2021 | 31 December 2021 | https://news.gtp.gr/2021/07/23/greece-pushes-covid-19-vaccination-new-incentives-laws/ (accessed on 15 August 2022) https://emvolio.gov.gr/freedompass-datapass (accessed on 15 August 2022) |
| Financial incentives for pharmacists and doctors which include subsidies for booked vaccination appointments as well as for in-home vaccinations. | 23 July 2021 | 23 July 2021 | https://news.gtp.gr/2021/07/23/greece-pushes-covid-19-vaccination-new-incentives-laws/ (accessed on 15 August 2022) | ||
| Those vaccinated against COVID-19 have to present their vaccination certificates, while unvaccinated people are required to present a negative COVID-19 test to enter all shops, banks and public indoor areas, as well as outdoor restaurants and cafes. Exceptions were made for food shops, pharmacies, and places of worship. | 2 November 2021 | 6 November 2021 | 1 May 2022 | https://abcnews.go.com/Health/wireStory/greece-toughens-restrictions-unvaccinated-cases-spike-80927971 (accessed on 15 August 2022) https://www.reuters.com/world/europe/unvaccinated-greece-face-new-restrictions-covid-cases-soar-2021-11-06/ (accessed on 15 August 2022) https://news.gtp.gr/2022/04/12/greece-suspend-covid-19-vaccination-and-recovery-certificates-next-month/ (accessed on 15 August 2022) | |
| Vaccination mandate for all residents of Greece over the age of 60. The unvaccinated would be fined 100 EUR for every month they remain unvaccinated. | 1 December 2021 | 17 January 2022 | 15 April 2022 | https://abcnews.go.com/Health/wireStory/greece-approves-mandatory-vaccination-aged-60-81500213 (accessed on 15 August 2022) https://www.bbc.com/news/world-europe-59474808 (accessed on 15 August 2022) https://greekcitytimes.com/2022/04/15/over-60s-in-greece-ends-as-of-today/ (accessed on 15 August 2022) | |
| Italy | Workers cannot access any place of work in Italy without a ‘Green Pass’, which is issued if the holder has been fully vaccinated against COVID-19, received a negative result from a rapid or antigen test in the previous 48 h or recovered from COVID-19 in the previous six months. | September 2021 | 15 October 2021 | May 2022 | https://www.theguardian.com/world/2021/oct/14/italy-braced-for-unrest-as-covid-pass-becomes-mandatory-for-all-workers (accessed on 15 August 2022) https://www.gazzettaufficiale.it/eli/id/2022/03/24/22G00034/sg (accessed on 15 August 2022) https://www.reuters.com/world/europe/italy-readies-law-make-covid-health-pass-mandatory-all-workers-2021-09-16/ (accessed on 15 August 2022) |
| Italy extends COVID-19 vaccine mandate to everyone over 50. The fine for non-compliance is 100 EUR. | 5 January 2022 | 5 January 2022 | 15 June 2022 | https://www.reuters.com/world/europe/italy-make-covid-jab-mandatory-over-50s-tighten-curbs-draft-2022-01-05/ (accessed on 15 August 2022) https://www.normattiva.it/uri-res/N2Ls?urn:nir:stato:decreto.legge:2022-01-07;1 (accessed on 15 August 2022) https://www.ilsole24ore.com/art/in-arrivo-nuova-stretta-anti-omicron-obbligo-vaccino-gli-over-60-AEOd2T6 (accessed on 15 August 2022) | |
| Norway | Domestic use of COVID-19 certificates for coastal cruises and events, as well as authority for municipalities to regulate, e.g., opening of closed businesses using COVID-19 certificates. | 20 June 2021 | 25 September 2021 | https://www.regjeringen.no/no/dokumenter/prop.-10-l-20212022/id2880813/?ch=5 (accessed on 15 August 2022) | |
| Russia | Mandatory vaccination for employees in a wide range of sectors, covering most of employees in the country. | 1 July 2021 | May 2022 | https://abcnews.go.com/Health/wireStory/russian-regions-make-vaccines-mandatory-workers-78334612 (accessed on 15 August 2022) https://www.loc.gov/item/global-legal-monitor/2021-06-22/russian-federation-unvaccinated-employees-can-be-suspended-without-pay/ (accessed on 15 August 2022) | |
| Lotteries for the vaccinated. Four draws of total 2000 cash prizes, 100,000 RUB each. | 1 September 2021 | 30 November 2021 | https://xn--80abehgib9bifaxh1a8l.xn--p1ai/ (accessed on 15 August 2022) | ||
| Introduction of COVID-19 certificates in most regions, nationwide digital passes showing proof of vaccination or recent recovery from COVID-19 to enter public areas and events. | 22 October 2021 | 8 November 2021 | March 2022 | https://www.themoscowtimes.com/2021/11/02/russia-imposes-digital-covid-passes-amid-virus-surge-a75461 (accessed on 15 August 2022) | |
| Poland | Lottery for the vaccinated. Every day from July 1, every 500th participant to receive a cash prize of PLN200 (222 EUR) while every 2000th person was to win PLN500 and every week for three months until the end of September, the government gave several automobiles, five prizes of 50,000 PLN and 720 electric scooters. The government engaged municipalities all over Poland by launching a competition with numerous financial prizes. The commune with the highest percentage of the vaccinated will receive 2 million PLN. The first 500 municipalities that will vaccinate 67 percent will receive 100,000 PLN. | 1 July 2021 | 30 September 2021 (lottery) | https://www.intellinews.com/poland-kicks-off-covid-19-vaccination-lottery-214644/?source=poland (accessed on 15 August 2022)https://www.gov.pl/web/loteria/zasady-i-regulamin2 (accessed on 15 August 2022) https://www.gov.pl/web/szczepimysie/do-wygarnia-zdrowie-i-miliony-zlotych-ruszaja-konkursy-dla-gmin (accessed on 15 August 2022) | |
| Spain | Introduction of COVID-19 certificates in 10 regions and 2 cities. Required in bars, restaurants, nursing homes, health establishments as well as to access events. | 22 November 2021 | 6 December 2021 | https://elpais.com/sociedad/2021-11-26/certificado-covid-que-comunidades-han-aprobado-su-uso-y-para-que-actividades.html (accessed on 15 August 2022) https://www.abc.es/sociedad/abci-estas-son-comunidades-necesitar-pasaporte-covid-navidad-nsv-202112171646_noticia.html (accessed on 15 August 2022) | |
| United Kingdom | Food, clothes, transportation and leisure discounts and vouchers for the vaccinated. | 1 August 2021 | 1 August 2021 | https://abcnews.go.com/Health/wireStory/pizza-shots-uk-targets-young-vaccine-incentives-79200767 (accessed on 15 August 2022) https://www.bbc.com/news/uk-58044088 (accessed on 15 August 2022) |
| Intervention | Type of Change | Time Period | Change in Number of Daily Administered Doses Total (95% CI)/Per Million Capita | Gain in Number of Doses Over a Time Period (Based on Counterfactual Analysis) |
|---|---|---|---|---|
| Announcement of cash incentive (“Freedom pass” in Greece) | Pulse | Immediate | 12,354 (11,755–12,954)/1197 | |
| Financial incentives for pharmacists and doctors (Greece) | Pulse | Immediate | 1546 (1215–1878)/150 | |
| Lottery and municipalities competition (Poland) | Pulse | Immediate | 25,196 (15,023–35,371)/667 | |
| Lottery (Russia) | Pulse | Immediate | 9766 (4003–15,530)/67 | |
| Introduction of COVID-19 certificates (Greece) | Step | Over 1 month | 1500 (1284–1716)/145 immediately | 830,956 |
| Introduction of COVID-19 certificates (Russia) | Pulse and step | Over 1 month | −42,718 (−78,256–7180)/−293 and 43,775 (8201–79,349)/300 immediately | 17,149,679 |
| Introduction of COVID-19 certificates (Spain) | Pulse | Over 3 days | 212,306/4544 | |
| Introduction of COVID-19 certificates (Norway) | Gradual step | 5 days | 1308 (228–2388)/237 on day 4 −1399 (−2482–315)/−254 on day 5 | |
| Introduction of employee vaccine mandate (Russia) | Pulse | Over 1,5 months | −43,429 (−78,063–8797)/−298 immediately | |
| Announcement of the universal vaccine mandate (Austria) | Step | Over 1 month | −3010 (−3592–2428)/−332 immediately | −1,696,266 (“missed” doses due to the policy change) |
| Introduction of the vaccine mandate for adults aged 60 and older (Greece) | Step | Immediate | −1932 (−2066–1798)/−187 | |
| Introduction of vaccine mandate for adults 50 and older (Italy) | Pulse and step | Over 4 days | −43,358 (−53,057–33,659)/−720 on day 1 89,729 (76,849–102,610)/1489 on day 2 17,920 (8321–27,518)/297 on day 3 −76,621 (−86,530–66,712)/−1272 on day 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuznetsova, L.; Diago-Navarro, E.; Mathu, R.; Trilla, A. Effectiveness of COVID-19 Vaccination Mandates and Incentives in Europe. Vaccines 2022, 10, 1714. https://doi.org/10.3390/vaccines10101714
Kuznetsova L, Diago-Navarro E, Mathu R, Trilla A. Effectiveness of COVID-19 Vaccination Mandates and Incentives in Europe. Vaccines. 2022; 10(10):1714. https://doi.org/10.3390/vaccines10101714
Chicago/Turabian StyleKuznetsova, Lidia, Elizabeth Diago-Navarro, Rachel Mathu, and Antoni Trilla. 2022. "Effectiveness of COVID-19 Vaccination Mandates and Incentives in Europe" Vaccines 10, no. 10: 1714. https://doi.org/10.3390/vaccines10101714
APA StyleKuznetsova, L., Diago-Navarro, E., Mathu, R., & Trilla, A. (2022). Effectiveness of COVID-19 Vaccination Mandates and Incentives in Europe. Vaccines, 10(10), 1714. https://doi.org/10.3390/vaccines10101714