


The Association between Socio-Demographics and Mental Distress Following COVID-19 Vaccination—Mediation of Vaccine Hesitancy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection Process
2.3. Questionnaire Development and Measures
2.4. Ethics Statement
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
3.2. Correlations among Demographics, Vaccine Hesitancy, and Mental Health
3.2.1. Correlation Analysis
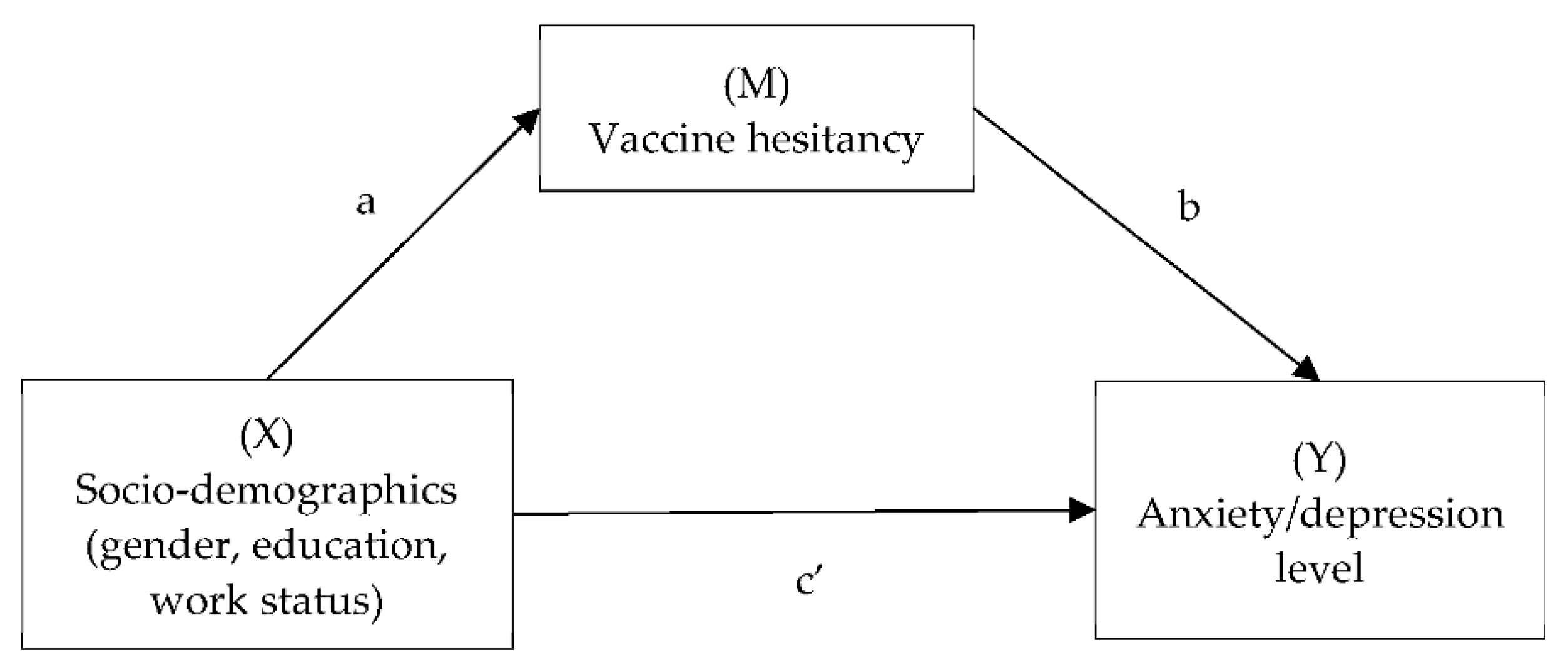
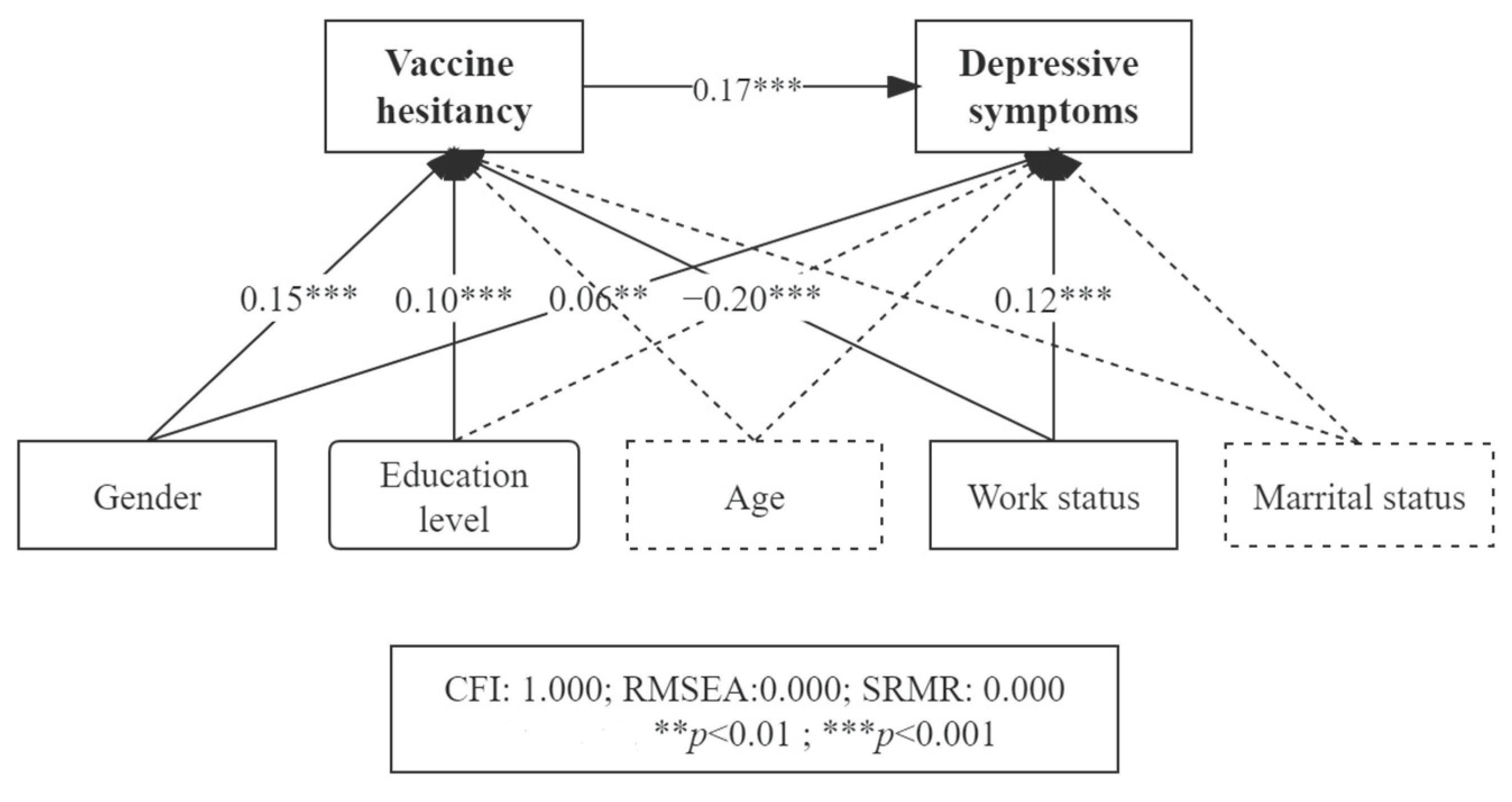
3.2.2. Factors of Depression and the Mechanism
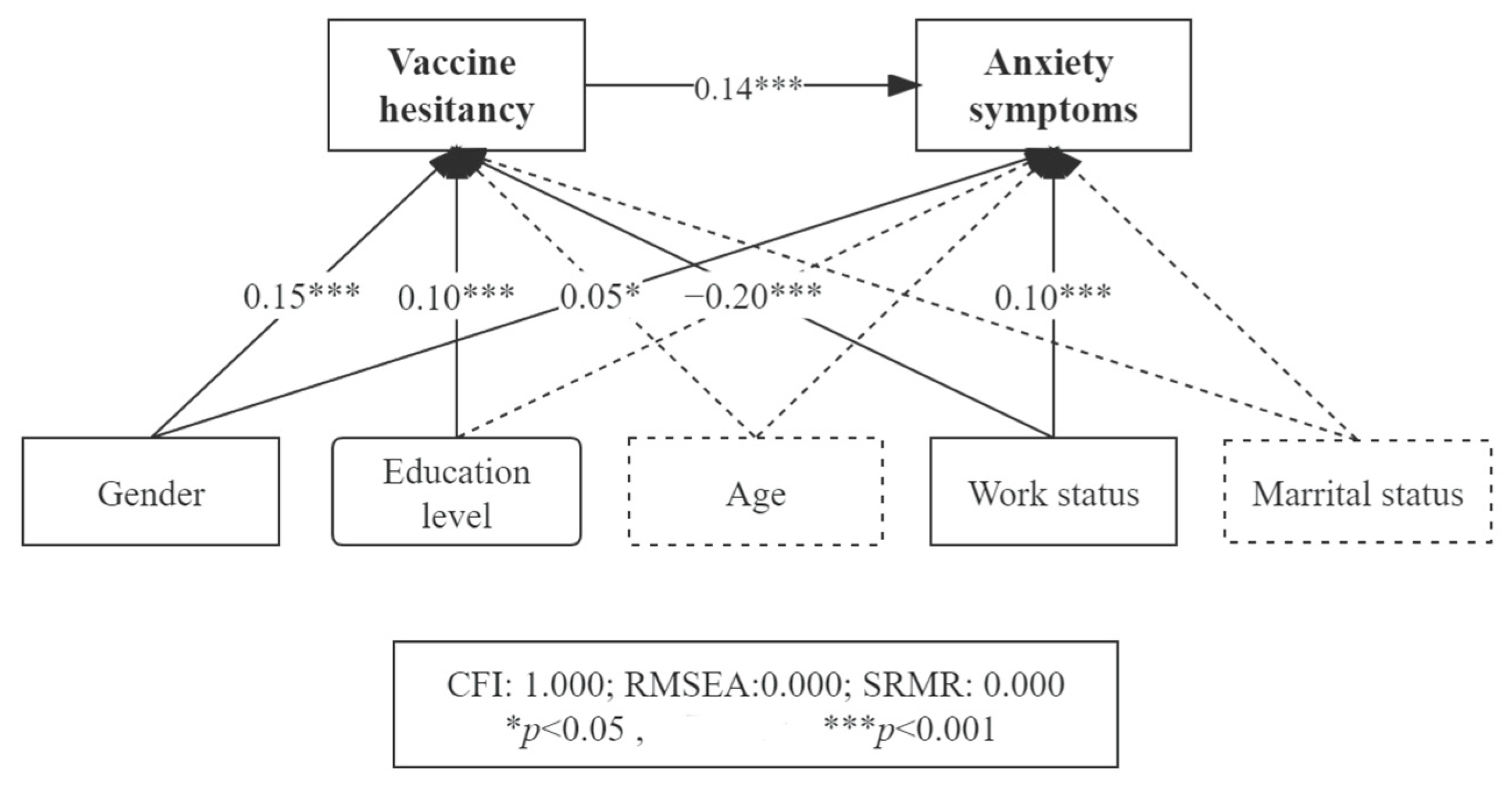
3.2.3. Factors for Anxiety and Mechanism
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Dattani, S.; Roser, M. Coronavirus Pandemic (COVID-19). Our World Data 2022, in press. [Google Scholar]
- Akhtar-Danesh, N.; Landeen, J. Relation between depression and sociodemographic factors. Int. J. Ment. Health Syst. 2007, 1, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Zhao, W.; Hu, F.; Hao, Q.; Hou, L.; Sun, X.; Zhang, G.; Yue, J.; Dong, B. Comorbid anxiety and depression, depression, and anxiety in comparison in multi-ethnic community of west China: Prevalence, metabolic profile, and related factors. J. Affect. Disord. 2021, 298, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Villarroel, M.A.; Terlizzi, E.P. Symptoms of Depression Among Adults: United States, 2019; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2020. [Google Scholar]
- Ren, X.; Yu, S.; Dong, W.; Yin, P.; Xu, X.; Zhou, M. Burden of depression in China, 1990–2017: Findings from the global burden of disease study 2017. J. Affect Disord. 2020, 268, 95–101. [Google Scholar] [CrossRef]
- Asher, M.; Asnaani, A.; Aderka, I.M. Gender differences in social anxiety disorder: A review. Clin. Psychol. Rev. 2017, 56, 1–12. [Google Scholar] [CrossRef]
- Rusu, A.; Chiriac, D.; Sălăgean, N.; Hojbotă, A. Job search self-efficacy as mediator between employment status and symptoms of anxiety. Rom. J. Appl. Psychol. 2013, 15, 69–75. [Google Scholar]
- Verma, S.; Mishra, A. Depression, anxiety, and stress and socio-demographic correlates among general Indian public during COVID-19. Int. J. Soc. Psychiatry 2020, 66, 756–762. [Google Scholar] [CrossRef]
- Hiswåls, A.-S.; Walander, A.; Soares, J.; Macassa, G. Employment Status, Anxiety and Depression in a Municipal Context. Res. Health Sci. 2017, 2, 12. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.; Lambe, S.; Freeman, D.; Cipriani, A. COVID-19 vaccines, hesitancy and mental health. Evid.-Based Ment. Health 2021, 24, 47–48. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 Vaccine Acceptance in Saudi Arabia: A Web-Based National Survey. J. Multidiscip. Health 2020, 13, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Machida, M.; Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; et al. Acceptance of a COVID-19 Vaccine in Japan during the COVID-19 Pandemic. Vaccines 2021, 9, 210. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Willis, D.E.; Selig, J.P.; Andersen, J.A.; Hall, S.; Hallgren, E.; Williams, M.; Bryant-Moore, K.; McElfish, P.A. Hesitant but vaccinated: Assessing COVID-19 vaccine hesitancy among the recently vaccinated. J. Behav. Med. 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.L.; Mishel, M.H. Uncertainty in childhood illness: A synthesis of the parent and child literature. Sch. Inq. Nurs. Pract. 2000, 14, 299–319. [Google Scholar]
- McEvoy, P.M.; Mahoney, A.E. Achieving certainty about the structure of intolerance of uncertainty in a treatment-seeking sample with anxiety and depression. J. Anxiety Disord. 2011, 25, 112–122. [Google Scholar] [CrossRef]
- Asaoka, H.; Koido, Y.; Kawashima, Y.; Ikeda, M.; Miyamoto, Y.; Nishi, D. Longitudinal change in depressive symptoms among healthcare professionals with and without COVID-19 vaccine hesitancy from October 2020 to June 2021 in Japan. Ind. Health 2021, 60, 387–394. [Google Scholar] [CrossRef]
- Palgi, Y.; Bergman, Y.S.; Ben-David, B.; Bodner, E. No psychological vaccination: Vaccine hesitancy is associated with negative psychiatric outcomes among Israelis who received COVID-19 vaccination. J. Affect. Disord. 2021, 287, 352–353. [Google Scholar] [CrossRef]
- Hagger, M.S.; Hankonen, N.; Kangro, E.; Lintunen, T.; Pagaduan, J.; Polet, J.; Ries, F.; Hamilton, K. Trait Self-Control, Social Cognition Constructs, and Intentions: Correlational Evidence for Mediation and Moderation Effects in Diverse Health Behaviours. Appl. Psychol. Health Well-Being 2019, 11, 407–437. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Yu, Y.; She, R.; Luo, S.; Xin, M.; Li, L.; Wang, S.; Ma, L.; Tao, F.; Zhang, J.; Zhao, J.; et al. Factors Influencing Depression and Mental Distress Related to COVID-19 among University Students in China: Online Cross-sectional Mediation Study. JMIR Ment. Health 2021, 8, e22705. [Google Scholar] [CrossRef] [PubMed]
- Mehra, K.; Markoulakis, R.; Kodeeswaran, S.; Redelmeier, D.; Sinyor, M.; MacKillop, J.; Cheung, A.; Levitt, E.E.; Addison, T.; Levitt, A. The impact of mental health and substance use issues on COVID-19 vaccine readiness: A cross sectional community-based survey in Ontario, Canada. medRxiv 2021. [Google Scholar] [CrossRef]
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, Y.; Long, S.; Fu, X.; Zhang, X.; Zhao, S.; Xiu, S.; Wang, X.; Lu, B.; Jin, H. Non-EPI Vaccine Hesitancy among Chinese Adults: A Cross-Sectional Study. Vaccines 2021, 9, 772. [Google Scholar] [CrossRef]
- Marzo, R.R.; Sami, W.; Alam, Z.; Acharya, S.; Jermsittiparsert, K.; Songwathana, K.; Pham, N.T.; Respati, T.; Faller, E.M.; Baldonado, A.M.; et al. Hesitancy in COVID-19 vaccine uptake and its associated factors among the general adult population: A cross-sectional study in six Southeast Asian countries. Trop. Med. Health 2022, 50, 1–10. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Fairchild, A.J.; MacKinnon, D.P. A General Model for Testing Mediation and Moderation Effects. Prev. Sci. 2009, 10, 87–99. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Wang, W.; Bian, Q.; Zhao, Y.; Li, X.; Wang, W.; Du, J.; Zhang, G.; Zhou, Q.; Zhao, M. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2014, 36, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Bi, Y.; Lao, L.; Jiang, S. Application of GAD-7 in population screening for generalized anxiety disorder. Chin. J. Gen. Pract. 2018, 17, 735–737. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kirzinger, A.; Hamel, L.; Sparks, G.; Brodie, M. KFF COVID-19 Vaccine Monitor: In Their Own Words; Kaiser Family Foundation: San Francisco, CA, USA, 2021. [Google Scholar]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- GBD Results Tool (Anxiety Disorders) [Internet]. 2019. Available online: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/d780dffbe8a381b25e1416884959e88b (accessed on 9 September 2022).
- Yu, W.; Singh, S.S.; Calhoun, S.; Zhang, H.; Zhao, X.; Yang, F. Generalized anxiety disorder in urban China: Prevalence, awareness, and disease burden. J. Affect. Disord. 2018, 234, 89–96. [Google Scholar] [CrossRef]
- Zhang, Y.; Bao, X.; Yan, J.; Miao, H.; Guo, C. Anxiety and Depression in Chinese Students During the COVID-19 Pandemic: A Meta-Analysis. Front. Public Health 2021, 9, 697642. [Google Scholar] [CrossRef]
- Bareeqa, S.B.; Ahmed, S.I.; Samar, S.S.; Yasin, W.; Zehra, S.; Monese, G.M.; Gouthro, R.V. Prevalence of depression, anxiety and stress in china during COVID-19 pandemic: A systematic review with meta-analysis. Int. J. Psychiatry Med. 2020, 56, 210–227. [Google Scholar] [CrossRef]
- Li, J.; Yang, Z.Q.; Wang, Y.; Jian, L.; Ji, J.; Li, K. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry 2020, 19, 249–250. [Google Scholar] [CrossRef]
- Eyllon, M.; Dang, A.P.; Ben Barnes, J.; Buresh, J.; Peloquin, G.D.; Hogan, A.C.; Shimotsu, S.T.; Sama, S.R.; Nordberg, S.S. Associations between psychiatric morbidity and COVID-19 vaccine hesitancy: An analysis of electronic health records and patient survey. Psychiatry Res. 2021, 307, 114329. [Google Scholar] [CrossRef]
- Pan, A.; Franco, O.H.; Wang, Y.-F.; Yu, Z.-J.; Ye, X.-W.; Lin, X. Prevalence and geographic disparity of depressive symptoms among middle-aged and elderly in China. J. Affect. Disord. 2008, 105, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; He, Y.; Wang, J.; Miao, J.; Zheng, H.; Zeng, Q. Epidemiology of depression at Traditional Chinese Medicine Hospital in Shanghai, China. Compr. Psychiatry 2016, 65, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; Sage Publications: New York, NY, USA, 2017. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number (n), % | Mean (SD) |
|---|---|---|
| Age (years) | ||
| 18–25 | 63.26% | |
| 26–40 | 26.70% | |
| >40 | 10.04% | |
| Gender | ||
| Female | 53.60% | |
| Male | 46.40% | |
| Education level | ||
| <High school | 10.75% | |
| ≥High school | 89.25% | |
| Employment status | ||
| Employed | 31.30% | |
| Unemployed (including students) | 68.70% | |
| Marital status | ||
| Unmarried | 78.08% | |
| Married | 20.93% | |
| Divorced or widowed | 0.99% | |
| Areas of living | ||
| Urban | 91.05% | |
| Non-urban | 8.95% | |
| Hesitancy | ||
| Not hesitant at all | 30.87% | |
| Merely hesitant | 33.76% | |
| Neutral | 2.08% | |
| Somewhat hesitant | 31.82% | |
| Very much | 1.47% | |
| Depression | ||
| No depression (0–4) | 84.52% | |
| Mild depression (5–9) | 11.74% | |
| Moderate or major (≥10) | 3.74% | |
| Depression (continuous) | 1.95 (3.65) | |
| Anxiety | ||
| No anxiety (0–4) | 86.93% | |
| Mild anxiety (5–9) | 10.27% | |
| Moderate or major anxiety (≥10) | 2.79% | |
| Anxiety (continuous) | 1.51 (3.04) |
| Age | Gender | Education | Employment Status | Marital Status | Vaccine Hesitancy | Anxiety | Depression | |
|---|---|---|---|---|---|---|---|---|
| Age | 1.00 | |||||||
| Gender | 0.05 * | 1.00 | ||||||
| Education | 0.07 * | 0.10 * | 1.00 | |||||
| Employment status | −0.64 * | −0.04 | −0.00 | 1.00 | ||||
| Marital status | 0.76 * | 0.05 * | −0.10 * | −0.53 * | 1.00 | |||
| Vaccine hesitancy | 0.17 * | 0.16 * | 0.11 * | −0.22 * | 0.14 * | 1.00 | ||
| Anxiety | −0.11 * | 0.12 * | 0.09 * | 0.12 * | −0.12 * | 0.15 * | 1.00 | |
| Depression | −0.13 * | 0.12 * | 0.09 * | 0.12 * | −0.14 * | 0.15 * | 0.74 * | 1.00 |
| X→M | M→Y | X→Y | Sobel Test | RIT (Indirect Effect/Total Effect) | RID (Indirect Effect/Direct Effect) | |
|---|---|---|---|---|---|---|
| Gender | B = 0.374, p = 0.000 | B = 0.481, p = 0.000 | B = 0.472, p = 0.003 | B = 0.180, p = 0.000 | 0.276 | 0.381 |
| Employment status | B = −0.529, p = 0.000 | B = 0.481, p = 0.000 | B = 0.914, p = 0.000 | B = −0.254, p = 0.000 | 0.385 | 0.278 |
| Education level | B = 0.135, p = 0.000 | B = 0.481, p = 0.000 | B = 0.017, p = 0.842 | B = 0.065, p = 0.000 | 0.788 | 3.715 |
| X→M | M→Y | X→Y | Sobel Test | RIT (Indirect Effect/Total Effect) | RID (Indirect Effect/Direct Effect) | |
|---|---|---|---|---|---|---|
| Gender | B = 0.374, p = 0.000 | B = 0.342, p = 0.000 | B = 0.299, p = 0.023 | B = 0.128, p = 0.000 | 0.299 | 0.427 |
| Employment status | B = −0.529, p = 0.000 | B = 0.342, p = 0.000 | B = 0.636, p = 0.023 | B = −0.181, p = 0.000 | 0.397 | 0.284 |
| Education level | B = 0.135, p = 0.000 | B = 0.342, p = 0.000 | B = 0.073, p = 0.321 | B = 0.046, p = 0.000 | 0.386 | 0.629 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Shen, J.; Li, M.; Shi, Y.; Wang, Q.; Chen, F.; Qin, H.; Zhao, X. The Association between Socio-Demographics and Mental Distress Following COVID-19 Vaccination—Mediation of Vaccine Hesitancy. Vaccines 2022, 10, 1697. https://doi.org/10.3390/vaccines10101697
Zhang X, Shen J, Li M, Shi Y, Wang Q, Chen F, Qin H, Zhao X. The Association between Socio-Demographics and Mental Distress Following COVID-19 Vaccination—Mediation of Vaccine Hesitancy. Vaccines. 2022; 10(10):1697. https://doi.org/10.3390/vaccines10101697
Chicago/Turabian StyleZhang, Xiaoying, Junwei Shen, Ming Li, Yijian Shi, Qing Wang, Fazhan Chen, Hongyun Qin, and Xudong Zhao. 2022. "The Association between Socio-Demographics and Mental Distress Following COVID-19 Vaccination—Mediation of Vaccine Hesitancy" Vaccines 10, no. 10: 1697. https://doi.org/10.3390/vaccines10101697
APA StyleZhang, X., Shen, J., Li, M., Shi, Y., Wang, Q., Chen, F., Qin, H., & Zhao, X. (2022). The Association between Socio-Demographics and Mental Distress Following COVID-19 Vaccination—Mediation of Vaccine Hesitancy. Vaccines, 10(10), 1697. https://doi.org/10.3390/vaccines10101697