
Predictors of COVID-19 Vaccine Acceptance among Healthcare Workers in Nigeria

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Data Collection
2.2. Inclusion Criteria
2.3. Sampling
2.4. Power Analysis
2.5. Data Analysis
3. Measured Parameters
3.1. Sociodemographic of Respondents
3.2. Acceptance of COVID-19 Vaccine
3.3. Knowledge and Attitudes towards COVID-19 Vaccination
3.4. Risk Perception of COVID-19 Vaccine
4. Results
4.1. Descriptive Statistics and Multinomial Logistic Regression of Sociodemographic Characteristics and COVID-19 Vaccine Acceptance among HCWs in Nigeria
4.1.1. Descriptive Statistics
4.1.2. COVID-19 Vaccine Acceptance
4.1.3. Multinomial Logistic Regression
4.2. Multinomial Logistic Regression of COVID-19 Vaccine Acceptance and Attitudes/Knowledge of Respondents towards COVID-19 Vaccines
4.3. Multinomial Logistic Regression of COVID-19 Vaccine Acceptance across Risk Perception Characteristics
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malik, J.A.; Ahmed, S.; Mir, A.; Shinde, M.; Bender, O.; Alshmmari, F.; Ansari, M.; Anwar, S. The SARS-CoV-2 mutations versus vaccine effectiveness: New opportunities to new challenges. J. Infect. Public Health 2022, 15, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Patwary, M.M.; Alam, M.A.; Bardhan, M.; Disha, A.S.; Haque, M.Z.; Billah, S.M.; Kabir, M.P.; Browning, M.H.; Rahman, M.M.; Parsa, A.D. COVID-19 Vaccine Acceptance among Low-and Lower-Middle-Income Countries: A Rapid Systematic Review and Meta-Analysis. Vaccines 2022, 10, 427. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Vivion, M.; Sauvageau, C.; Gagneur, A. Nature does things well, why should we interfere? Vaccine hesitancy among mothers. Qual. Health Res. 2016, 26, 411–425. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Buckner, J.H.; Chowell, G.; Springborn, M.R. Dynamic prioritization of COVID-19 vaccines when social distancing is limited for essential workers. Proc. Natl. Acad. Sci. USA 2021, 118, e2025786118. [Google Scholar] [CrossRef]
- Glatman-Freedman, A.; Bromberg, M.; Dichtiar, R.; Hershkovitz, Y.; Keinan-Boker, L. The BNT162b2 vaccine effectiveness against new COVID-19 cases and complications of breakthrough cases: A nation-wide retrospective longitudinal multiple cohort analysis using individualized data. EBioMed. 2021, 72, 103574. [Google Scholar] [CrossRef]
- Arbel, R.; Sergienko, R.; Friger, M.; Peretz, A.; Beckenstein, T.; Yaron, S.; Netzer, D.; Hammerman, A. Effectiveness of a second BNT162b2 booster vaccine against hospitalization and death from COVID-19 in adults aged over 60 years. Nat. Med. 2022, 28, 1486–1490. [Google Scholar] [CrossRef]
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitpatrick, M.C.; et al. The impact of vaccination on coronavirus disease 2019 (COVID-19) outbreaks in the United States. Clin. Infect. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef]
- Afolabi, A.A.; Ilesanmi, O.S. Dealing with vaccine hesitancy in Africa: The prospective COVID-19 vaccine context. Pan Afr. Med. J. 2021, 38, 3. [Google Scholar] [CrossRef]
- Lancet. An African plan to control COVID-19 is urgently needed. Lancet 2020, 396, 1777. [Google Scholar] [CrossRef]
- Dzinamarira, T.; Nachipo, B.; Phiri, B.; Musuka, G. COVID-19 vaccine roll-out in South Africa and Zimbabwe: Urgent need to address community preparedness, fears and hesitancy. Vaccines 2021, 9, 250. [Google Scholar] [CrossRef] [PubMed]
- Diab, M.M.; Zimmerman, A.; Dixit, S.; Mao, W.; Bharali, I.; Kristoffersen, A.; Yamey, G.; Ogbuoji, O. The Cost of Procuring and Delivering COVID-19 Vaccines in Low-and Middle-Income Countries: A Model of Projected Resource Needs. EurPMC 2021, 309459. [Google Scholar]
- Paudel, S.; Palaian, S.; Shankar, P.R.; Subedi, N. Risk perception and hesitancy toward COVID-19 vaccination among healthcare workers and staff at a medical college in Nepal. Risk Manag. Healthc. Policy 2021, 14, 2253–2261. [Google Scholar] [CrossRef]
- Ditekemena, J.D.; Nkamba, D.M.; Mutwadi, A.; Mavoko, H.M.; Fodjo, J.N.S.; Luhata, C.; Obimpeh, M.; Hees, S.V.; Nachega, J.B.; Colebunders, R. COVID-19 Vaccine Acceptance in the Democratic Republic of Congo: A Cross-Sectional Survey. Vaccines 2021, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Ike, A.C.; Reward, E.E.; Mbaawuaga, E.M.; Nnabuife, O.O.; Orabueze, I.N.A. Current status and underlying problems of eradication of poliomyelitis in the remaining endemic countries. Eur. J. Prev. Med. 2018, 6, 23–28. [Google Scholar] [CrossRef][Green Version]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.B.; Miema, J.M.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmat. Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Adebisi, Y.A.; Alaran, A.J.; Bolarinwa, O.A.; Sholabi, W.A.; Lucero-Prisno III, D.E. When it is available, will we take it? Public perception of hypothetical COVID-19 vaccine in Nigeria. Pan Afr. J. 2021, 38, 230. [Google Scholar] [CrossRef]
- Tobin, E.A.; Okonofua, M.; Adeke, A.; Obi, A. Willingness to Accept a COVID-19 Vaccine in Nigeria: A Population-based Cross-sectional Study. Cent. Afr. J. Public Health 2021, 7, 53–60. [Google Scholar] [CrossRef]
- Shekhar, R.; Garg, I.; Pal, S.; Kottewar, S.; Sheikh, A.B. COVID-19 Vaccine Booster: To Boost or Not to Boost. Infect. Dis. Rep. 2021, 13, 924–929. [Google Scholar] [CrossRef]
- Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar]
- Malik A, Malik J, Ishaq U () Acceptance of COVID-19 vaccine in Pakistan among health care workers. PLoS ONE 2021, 16, e0257237.
- Njoga, E.O.; Mshelbwala, P.P.; Abah, K.O.; Awoyomi, O.J.; Wangdi, K.; Pewan, S.B.; Oyeleye, F.A.; Galadima, H.B.; Alhassan, S.A.; Okoli, C.E.; et al. COVID-19 Vaccine Hesitancy and Determinants of Acceptance among Healthcare Workers, Academics and Tertiary Students in Nigeria. Vaccines 2022, 10, 626. [Google Scholar] [CrossRef]
- Dubov, A.; Distelberg, B.J.; Abdul-Mutakabbir, J.C.; Beeson, W.L.; Loo, L.K.; Montgomery, S.B.; Chrissian, A.A. Predictors of COVID-19 Vaccine Acceptance and Hesitancy among Healthcare Workers in Southern California: Not Just “Anti” vs.“Pro” Vaccine. Vaccines 2021, 9, 1428. [Google Scholar] [CrossRef]
- Elharake, J.A.; Galal, B.; Alqahtani, S.A.; Kattan, R.F.; Barry, M.A.; Temsah, M.-H.; Malik, A.A.; McFadden, S.M.; Yildirim, I.; Khoshnood, K.; et al. COVID-19 vaccine acceptance among health care workers in the Kingdom of Saudi Arabia. Int. J. Infect. Dis. 2021, 109, 286–293. [Google Scholar] [CrossRef]
- Otu, A.; Ukpeh, I.; Okuzu, O.; Yaya, S. Leveraging mobile health applications to improve sexual and reproductive health services in Nigeria: Implications for practice and policy. Reprod. Health 2021, 18, 21. [Google Scholar] [CrossRef]
- Akinyemi, A.I.; Isiugo-Abanihe, U.C. Demographic dynamics and development in Nigeria. Afr. Popul. Stud. 2014, 27, 239–248. [Google Scholar] [CrossRef]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. COVID-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am. J. Infect. Control 2021, 49, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Elhadi, M.; Alsoufi, A.; Alhadi, A.; Hmeida, A.; Alshareea, E.; Dokali, M.; Abodabos, S.; Alsadiq, O.; Abdelkabir, M.; Ashini, A.; et al. Knowledge, attitude, and acceptance of healthcare workers and the public regarding the COVID-19 vaccine: A cross-sectional study. BMC Public Health 2021, 21, 955. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 vaccine acceptance among health care workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef] [PubMed]
- Jain, L.; Vij, J.; Satapathy, P.; Chakrapani, C.; Patro, B.; Kar, S.S.; Singh, R.; Pala, S.; Sankhe, L.; Modi, B.; et al. Factors Influencing COVID-19 Vaccination Intentions Among College Students: A Cross-Sectional Study in India. Front. Public Health 2018, 9, 735902. [Google Scholar] [CrossRef] [PubMed]
- Agha, S.; Chine, A.; Lalika, M.; Pandey, S.; Seth, A.; Wiyeh, A.; Seng, A.; Rao, N.; Badshah, A. Drivers of COVID-19 Vaccine Uptake amongst Healthcare Workers (HCWs) in Nigeria. Vaccines 2021, 9, 1162. [Google Scholar] [CrossRef]
- Ekwebene, O.C.; Obidile, V.C.; Azubuike, P.C.; Nnamani, C.P.; Dankano, N.E.; Egbuniwe, M.C. COVID-19 Vaccine Knowledge and Acceptability among Healthcare Providers in Nigeria. Int. J. Trop. Dis. Health 2021, 42, 51–60. [Google Scholar] [CrossRef]
- Onwe, R.O.; Nnaemeka, V.C.; Ekwedike, A.L.; Ihedioha, J.I.; Ahamefule, C.S.; Nnabuife, O.O.; Ike, A.C. COVID-19 vaccine: Vaccine acceptance, risk perception, and attitude towards vaccination among college students and staff in the southeastern universities, Nigeria. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Guidry, J.P.D.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Berrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. willingness to get the COVID-19 vaccine with and without emergency use authorization. Am. J. Infect. Control 2021, 49, 137–142. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Yilma, D.; Mohammed, R.; Abdela, S.G.; Enbiale, W.; Seifu, F.; Pareyn, M.; Liesenborghs, L.; van Griensven, J.; van Henten, S. COVID-19 vaccine acceptability among healthcare workers in Ethiopia: Do we practice what we preach? Trop. Med. Int. Health 2022, 27, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.W.C.; Tan, H.M.; Lee, W.H.; Mathews, J.; Young, D. COVID-19 vaccine booster hesitancy among healthcare workers: A retrospective observational study in Singapore. Vaccines 2022, 10, 464. [Google Scholar] [CrossRef]
- Larson, H.J.; Broniatowski, D.A. Volatility of vaccine confidence. Science 2021, 371, 1289. [Google Scholar] [CrossRef]
- Ledford, H. COVID vaccines and blood clots: Five key questions. Nature 2021, 592, 495–496. [Google Scholar] [CrossRef] [PubMed]
- Sønderskov, K.M.; Dinesen, P.T.; Østergaard, S.D. Sustained COVID-19 vaccine willingness after safety concerns over the Oxford-AstraZeneca vaccine. Dan Med. J. 2021, 68, A03210292. [Google Scholar] [PubMed]
- Kayode, O.R.; Babatunde, O.A.; Adekunle, O.; Igbalajobi, M.; Abiodun, A.K. COVID-19 Vac-cine Hesitancy: Maximizing the Extending Roles of Community Pharmacists in Nigeria in Driving Behavioural Changes in Public Health Interventions. J. Infect. Dis. Epidemiol. 2021, 7, 205. [Google Scholar]
- Magadmi, R.M.; Kamel, F.O. Beliefs and barriers associated with COVID-19 vaccination among the general population in Saudi Arabia. BMC Public Health 2021, 21, 1438. [Google Scholar] [CrossRef]
- Barry, M.; Temsah, M.-H.; Alhuzaimi, A.; Alamro, N.; Al-Eyadhy, A.; Aljamaan, F.; Saddik, B.; Alhaboob, A.; Alsohime, F.; Alhasan, K.; et al. COVID-19 vaccine confidence and hesitancy among health care workers: A cross-sectional survey from a MERS-CoV experienced nation. PLoS ONE 2021, 16, e0244415. [Google Scholar] [CrossRef]
- Chen, F.; Zhu, S.; Dai, Z.; Hao, L.; Luan, C.; Guo, Q.; Meng, C.; Zhang, Y. Effects of COVID-19 and mRNA vaccines on human fertility. Hum. Reprod. 2020, 37, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Schaler, L.; Wingfield, M. COVID-19 vaccine—can it affect fertility? Ir. J. Med. Sci. 2021, 191, 2185–2187. [Google Scholar] [CrossRef]
- Vassallo, A.; Shajahan, S.; Harris, K.; Hallam, L.; Hockham, C.; Womersley, K.; Woodward, M.; Sheel, M. Sex and gender in COVID-19 vaccine research: Substantial evidence gaps remain. Front. Glob. Womens Health 2021, 2, 761511. [Google Scholar] [CrossRef] [PubMed]
- Eh-Mohandes, A.; White, T.M.; Wyka, K.; Rauh, L.; Rabin, K.; Kimball, S.H.; Ratzan, S.C.; Lazarus, J.V. COVID-19 vaccine acceptance among adults in four major US metropolitan areas and nationwide. Sci. Rep. 2021, 11, 21844. [Google Scholar] [CrossRef] [PubMed]
- Ilesanmi, O.; Afolabi, A.; Uchendu, O. The prospective COVID-19 vaccine willingness to pay and perception of community members in Ibadan, Nigeria. PeerJ 2021, 9, e11153. [Google Scholar] [CrossRef]
- Chou, W.Y.S.; Budenz, A. Considering emotion in COVID-19 vaccine communication: Addressing vaccine hesitancy and fostering vaccine confidence. Health Comm. 2020, 35, 1718–1722. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Eepidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Benneth, K.; Mason, L.; Gibson-Miller, J. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Comm. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Enitan, S.S.; Oyekale, A.O.; Akele, R.Y.; Olawuyi, K.A.; Olabisi, E.O.; Nwankiti, A.J.; Enitan, C.B. Assessment of knowledge, perception and readiness of Nigerians to participate in the COVID-19 vaccine trial. Int. J. Vacc. Immunol. 2020, 4, 1–13. [Google Scholar]
- Qiao, S.; Tam, C.C.; Li, X. Risk exposures, risk perceptions, negative attitudes toward general vaccination, and COVID-19 vaccine acceptance among college students in South Carolina. MedRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.L.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. E. Clin. Med. 2020, 26, 100495. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) | COVID-19 Vaccine Acceptance (Total = 418/705; 59.3% n (%)) | OR | p-Value | 95% CI |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 281 (39.6%) | 188 (66.9%) | 2.8 | <0.001 | 1.7–4.6 |
| Female | 429 (60.4%) | 232 (54.1%) | Ref | ||
| Age | |||||
| 15–25 | 308 (43.4%) | 163 (52.8%) | 0.6 | 0.5 | 0.1–2.9 |
| 26–36 | 202 (28.5%) | 126 (62.4%) | 0.8 | 0.8 | 0.7–4.0 |
| 37–47 | 102(14.3%) | 70 (68.6%) | 0.7 | 0.6 | 0.1–3.3 |
| 48–58 | 75 (10.5%) | 42 (65.3%) | 0.8 | 0.8 | 0.1–4.4 |
| 59–69 | 22 (3.1%) | 13 (59.1%) | Ref | ||
| Zone in Nigeria | |||||
| North | 307(43.2%) | 169 (55.1%) | 0.4 | 0.004 | 0.2–0.8 |
| East | 202 (28.5%) | 85 (42.1%) | 0.1 | <0.001 | 0.1– 0.3 |
| West | 201 (28.3%) | 167 (83.0%) | Ref | ||
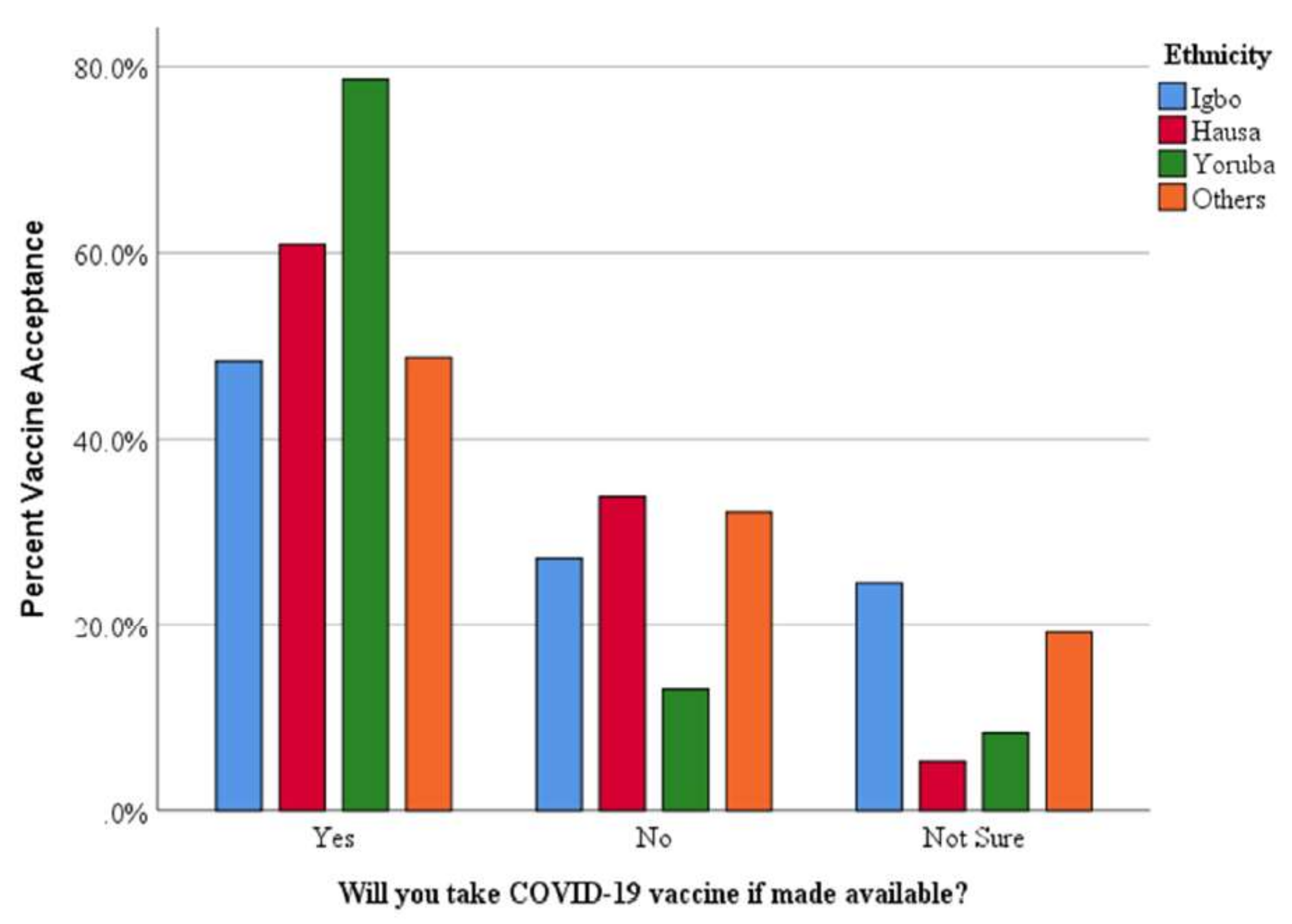
| Ethnicity | |||||
| Igbo | 229 (32.5%) | 110 (48.2%) | 0.8 | 0.357 | 0.5–1.3 |
| Hausa | 135 (19.2%) | 82 (60.9%) | 4.5 | <0.001 | 1.8–10.9 |
| Yoruba | 193 (27.4%) | 152 (78.6%) | 3.5 | <0.001 | 1.8–7.1 |
| Others | 147 (20.9%) | 71 (48.6%) | Ref | ||
| Location | |||||
| Urban | 421 (60.0%) | 269 (63.9%) | 2.4 | 0.004 | 1.5–4.8 |
| Suburban | 192 (27.4%) | 98 (51.1%) | 1.1 | 0.7 | 0.3–1.4 |
| Rural | 89 (12.7%) | 48 (53.9%) | Ref | ||
| Facility | |||||
| Teaching Hospital | 119 (17.0%) | 55.9 (47.0%) | 0.364 | 1.442 | 0.7–3.2 |
| Federal Medical Centre | 228(32.5%) | 132 (57.9%) | 0.083 | 1.733 | 0.9–3.2 |
| Private Hospital | 138 (19.7%) | 91 (65.7%) | 1.7 | <0.020 | 0.8–3.7 |
| Primary Healthcare | 103 (14.7%) | 86 (83.2%) | 4.4 | <0.004 | 1.6–12.3 |
| Others | 114 (16.2%) | 52 (45.6%) | Ref | ||
| Ward | |||||
| Respiratory Unit | 53 (7.6%) | 29 (54.7%) | 2.9 | 0.1 | 0.6–3.8 |
| Emergency Unit | 104 (14.9%) | 67 (64.4%) | 2.0 | 0.17 | 0.3–2.0 |
| Intensive Unit | 106(15.2%) | 71 (67.0%) | 2.0 | 0.18 | 0.3–2.0 |
| Medical Imaging | 28 (4.0) | 19 (66.7%) | 2.5 | 0.2 | 0.2–2.4 |
| Medical Laboratory Unit | 41 (5.9%) | 23 (56.5%) | 1.4 | 0.5 | 0.5–2.3 |
| Others | 367 (52.5%) | 197 (53.7%) | Ref | ||
| Cohort | |||||
| Physician | 111(15.7%) | 69 (62.4%) | 2.4 | 0.031 | 1.1–5.4 |
| Nurse | 46(6.5%) | 29 (62.2%) | 2.0 | 0.9 | 0.4–2.2 |
| Pharmacist | 157(22.2%) | 101 (64.1%) | 1.2 | 0.5 | 0.7–2.2 |
| Physiotherapist | 20(2.8%) | 15 (75.0%) | 4.8 | 0.1 | 0.6–37.8 |
| Scientist | 114(16.1%) | 50 (43.9%) | 0.6 | 0.2 | 0.3–1.2 |
| Radiographer | 27(3.8%) | 21 (76.9%) | 3.2 | 0.1 | 0.7–14.4 |
| Administrative Staff | 50(7.0%) | 35 (70.0%) | 2.8 | 0.7 | 0.9–8.5 |
| Others | 181 (25.5%) | 100 (55.2%) | Ref | ||
| Chronic Illness | |||||
| Yes | 128 (18.0%) | 79 (61.4%) | 1.1 | 0.8 | 0.670–1.665 |
| No | 578(81.9%) | 339 (58.7%) | Ref |
| Knowledge and Attitude towards COVID-19 Vaccination | n % | COVID-19 Vaccine Acceptance | OR | p-Value | 95% CI | |
|---|---|---|---|---|---|---|
| Have you taken any other vaccine apart from the COVID-19 vaccine in the past three years? | Yes No NS | 328 (46.7%) 330 (46.9%) 45(6.4%) | 235 71.6%) 162 (49.1%) 19 (42.2%) | 3.1 Ref. | 0.027 | 1.1–8.3 |
| Will you recommend the COVID-19 vaccine to your patient? | Yes Not NS | 438 (62.8%) 155(22.2%) 105 (15.0%) | 364 (83.1%) 30 (19.4%) 18 (17.1%) | 24.9 Ref. | <0.001 | 12.6–49.3 |
| Do you know the different COVID-19 vaccines currently in use in Nigeria? | Yes No NS | 458 (66.4%) 157 (22.8%) 75 (10.9%) | 315 (68.8%) 59 (45.7%) 35 (8.6%) | 1.6 Ref. | 0.024 | 0.5–5.2 |
| Is the timing for the current COVID-19 vaccine appropriate | Yes No NS | 378 (53.8%) 120 (17.1%) 204 (29.1) | 299 (79.1) 52 (43.3%) 66 (32.4%) | 4.4 Ref | <0.001 | 2.4– 8.0 |
| Do you think COVID-19 vaccines should be made mandatory? | Yes No NS | 224 (32.3%) 376 (54.2%) 94 (13.5%) | 203 (90.6%) 151(40.3%) 56 (59.6%) | 7.6 Ref. | <0.001 | 3.3–17.8 |
| Risk Perceptions and COVID-19 Vaccination | n% | COVID-19 Vaccine Acceptance | OR | p-Value | 95% CI | |
|---|---|---|---|---|---|---|
| Are you concerned about the side effects of COVID-19 vaccines? | Yes No | 569 (81.2%) 132 (18.8%) | 348 (61.2%) 67 (50.8%) | 1.5 Ref | 0.3 | 0.8- 2.8 |
| Do you think the current COVID-19 vaccines have passed full clinical trials? | Yes No NS | 364 (51.8%) 206 (29.5%) 133 (18.9%) | 317 (87.1%) 57 (27.7%) 43 (32.3%) | 6.1 1.4 Ref | <0.001 0.3 | 3.1–12.2 0.7–2.6 |
| Do you think the COVID-19 vaccine contains dangerous substances? | Yes No NS | 229 (33%) 253 (36.2%) 694 (30.8%) | 123 (53.7%) 206 (81.4%) 409 (58.9%) | 1.7 4.5 Ref | 0.106 <0.001 | 0.9–3.1 2.0–10.1 |
| Do you think COVID-19 vaccine is safe? | Yes No NS | 337 (47.9%) 138 (19.5) 228 (32.8%) | 305 (90.5%) 40 (29.0%) 72 (31.6%) | 5.2 0.7 Ref | <0.001 0.8 | 2.50–10.92 0.4–1.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nnaemeka, V.C.; Onwe, R.O.; Ekwedike, A.L.; Oyedele, O.E.; Tsiterimam, T.S.; Ochepo, O.E.; Nwokoye, N.N.; Ike, A.C. Predictors of COVID-19 Vaccine Acceptance among Healthcare Workers in Nigeria. Vaccines 2022, 10, 1645. https://doi.org/10.3390/vaccines10101645
Nnaemeka VC, Onwe RO, Ekwedike AL, Oyedele OE, Tsiterimam TS, Ochepo OE, Nwokoye NN, Ike AC. Predictors of COVID-19 Vaccine Acceptance among Healthcare Workers in Nigeria. Vaccines. 2022; 10(10):1645. https://doi.org/10.3390/vaccines10101645
Chicago/Turabian StyleNnaemeka, Victory Chizaram, Reuben Ogba Onwe, Adaku Lydia Ekwedike, Oluwakemi Elizabeth Oyedele, Thomas Sambo Tsiterimam, Ogbole Emmanuel Ochepo, Nkiru Nenye Nwokoye, and Anthony Chibuogwu Ike. 2022. "Predictors of COVID-19 Vaccine Acceptance among Healthcare Workers in Nigeria" Vaccines 10, no. 10: 1645. https://doi.org/10.3390/vaccines10101645
APA StyleNnaemeka, V. C., Onwe, R. O., Ekwedike, A. L., Oyedele, O. E., Tsiterimam, T. S., Ochepo, O. E., Nwokoye, N. N., & Ike, A. C. (2022). Predictors of COVID-19 Vaccine Acceptance among Healthcare Workers in Nigeria. Vaccines, 10(10), 1645. https://doi.org/10.3390/vaccines10101645