
Glaucoma Cases Following SARS-CoV-2 Vaccination: A VAERS Database Analysis



Abstract
:1. Introduction
2. Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A Global Database of COVID-19 Vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control the Vaccine Adverse Event Reporting System (VAERS) Request. Available online: https://wonder.cdc.gov/vaers.html (accessed on 18 May 2022).
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The Pathophysiology and Treatment of Glaucoma: A Review. JAMA 2014, 311, 1901. [Google Scholar] [CrossRef] [PubMed]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040: A Systematic Review and Meta-Analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Nickells, R.W.; Howell, G.R.; Soto, I.; John, S.W.M. Under Pressure: Cellular and Molecular Responses During Glaucoma, a Common Neurodegeneration with Axonopathy. Annu. Rev. Neurosci. 2012, 35, 153–179. [Google Scholar] [CrossRef] [PubMed]
- Welcome to MedDRA|MedDRA. Available online: https://www.meddra.org/ (accessed on 18 May 2022).
- Centers for Disease Control and Prevention (CDC) CDC WONDER FAQs. Available online: https://wonder.cdc.gov/wonder/help/faq.html#8 (accessed on 18 May 2022).
- Centers for Disease Control and Prevention (CDC). The Vaccine Adverse Event Reporting System (VAERS) Data Request. Available online: https://wonder.cdc.gov/controller/datarequest/D8 (accessed on 7 June 2022).
- Fedak, K.M.; Bernal, A.; Capshaw, Z.A.; Gross, S. Applying the Bradford Hill Criteria in the 21st Century: How Data Integration Has Changed Causal Inference in Molecular Epidemiology. Emerg. Themes Epidemiol. 2015, 12, 14. [Google Scholar] [CrossRef]
- Savaskan, E.; Löffler, K.U.; Meier, F.; Müller-Spahn, F.; Flammer, J.; Meyer, P. Immunohistochemical Localization of Angiotensin-Converting Enzyme, Angiotensin II and AT1 Receptor in Human Ocular Tissues. Ophthalmic Res. 2004, 36, 312–320. [Google Scholar] [CrossRef]
- Igic, R.; Robinson, C.J.G.; Milosevic, Z. Activity of Renin and Angiotensin I Converting Enzyme in Retina and Ciliary Body. Lijec. Vjesn. 1977, 99, 482–484. [Google Scholar]
- Cullinane, A.B.; Leung, P.S.; Ortego, J.; Coca-Prados, M.; Harvey, B.J. Renin-Angiotensin System Expression and Secretory Function in Cultured Human Ciliary Body Non-Pigmented Epithelium. Br. J. Ophthalmol. 2002, 86, 676–683. [Google Scholar] [CrossRef]
- Angeli, F.; Spanevello, A.; Reboldi, G.; Visca, D.; Verdecchia, P. SARS-CoV-2 Vaccines: Lights and Shadows. Eur. J. Intern. Med. 2021, 88, 1–8. [Google Scholar] [CrossRef]
- Ozonoff, A.; Nanishi, E.; Levy, O. Bell’s Palsy and SARS-CoV-2 Vaccines. Lancet. Infect. Dis. 2021, 21, 450–452. [Google Scholar] [CrossRef]
- Fowler, N.; Mendez Martinez, N.R.; Pallares, B.V.; Maldonado, R.S. Acute-Onset Central Serous Retinopathy after Immunization with COVID-19 MRNA Vaccine. Am. J. Ophthalmol. Case Rep. 2021, 23, 101136. [Google Scholar] [CrossRef] [PubMed]
- Santovito, L.S.; Pinna, G. Acute Reduction of Visual Acuity and Visual Field after Pfizer-BioNTech COVID-19 Vaccine 2nd Dose: A Case Report. Inflamm. Res. 2021, 70, 931–933. [Google Scholar] [CrossRef] [PubMed]
- Wasser, L.M.; Roditi, E.; Zadok, D.; Berkowitz, L.; Weill, Y. Keratoplasty Rejection After the BNT162b2 Messenger RNA Vaccine. Cornea 2021, 40, 1070–1072. [Google Scholar] [CrossRef]
- Phylactou, M.; Li, J.P.O.; Larkin, D.F.P. Characteristics of Endothelial Corneal Transplant Rejection Following Immunisation with SARS-CoV-2 Messenger RNA Vaccine. Br. J. Ophthalmol. 2021, 105, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Rallis, K.I.; Ting, D.S.J.; Said, D.G.; Dua, H.S. Corneal Graft Rejection Following COVID-19 Vaccine. Eye 2022, 36, 1319–1320. [Google Scholar] [CrossRef]
- Ivanov, K.; Garanina, E.; Rizvanov, A.; Khaiboullina, S. Inflammasomes as Targets for Adjuvants. Pathogens 2020, 9, 252. [Google Scholar] [CrossRef] [PubMed]
- Bayas, A.; Menacher, M.; Christ, M.; Behrens, L.; Rank, A.; Naumann, M. Bilateral Superior Ophthalmic Vein Thrombosis, Ischaemic Stroke, and Immune Thrombocytopenia after ChAdOx1 NCoV-19 Vaccination. Lancet 2021, 397, e11. [Google Scholar] [CrossRef]
- Papasavvas, I.; Herbort, C.P. Reactivation of Vogt-Koyanagi-Harada Disease under Control for More than 6 Years, Following Anti-SARS-CoV-2 Vaccination. J. Ophthalmic Inflamm. Infect. 2021, 11, 21. [Google Scholar] [CrossRef]
- Singh, R.B.; Parmar, U.P.S.; Kahale, F.; Agarwal, A.; Tsui, E. Vaccine-Associated Uveitis Following SARS-CoV-2 Vaccination: A CDC-VAERS Database Analysis. Ophthalmology 2022, 8, 27. [Google Scholar] [CrossRef]
- Wu, P.; Duan, F.; Luo, C.; Liu, Q.; Qu, X.; Liang, L.; Wu, K. Characteristics of Ocular Findings of Patients with Coronavirus Disease 2019 (COVID-19) in Hubei Province, China. JAMA Ophthalmol. 2020, 138, 1291. [Google Scholar] [CrossRef]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary Manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Li, J.P.O.; Lam, D.S.C.; Chen, Y.; Ting, D.S.W. Novel Coronavirus Disease 2019 (COVID-19): The Importance of Recognising Possible Early Ocular Manifestation and Using Protective Eyewear. Br. J. Ophthalmol. 2020, 104, 297–298. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Seo, M.H.; Choi, K.E.; Lee, S.; Choi, B.; Yun, C.; Kim, S.W.; Kim, Y.Y. Vision-Threatening Ocular Adverse Events after Vaccination against Coronavirus Disease 2019. J. Clin. Med. 2022, 11, 3318. [Google Scholar] [CrossRef] [PubMed]
- Behera, G.; Jossy, A.; Deb, A.K.; Neelakandan, S.; Basavarajegowda, A. Spontaneous Suprachoroidal Haemorrhage in Haemophilia Coincident with ChAdOx1 NCoV-19 Vaccine. Eur. J. Ophthalmol. 2022, 112067212210982. [Google Scholar] [CrossRef]
- Wagle, A.; Wu, B.; Gopal, L.; Sundar, G. Necrosis of Uveal Melanoma Post-COVID-19 Vaccination. Indian J. Ophthalmol. 2022, 70, 1837. [Google Scholar] [CrossRef]
- Wang, M.T.M.; Niederer, R.L.; McGhee, C.N.J.; Danesh-Meyer, H.V. COVID-19 Vaccination and the Eye. Am. J. Ophthalmol. 2022, 240, 79–98. [Google Scholar] [CrossRef]
- Health Insurance Portability and Accountability Act of 1996 (HIPAA)|CDC. Available online: https://www.cdc.gov/phlp/publications/topic/hipaa.html (accessed on 19 May 2022).




{kind=link}
{kind=link}
{kind=link}
| Frequency (n) | % | |
|---|---|---|
| Mean Age (in years) | 60.41 ± 17.56 | |
| Age Range | ||
| 10–19 | 2 | 1.2 |
| 20–29 | 9 | 5.6 |
| 30–39 | 9 | 5.6 |
| 40–49 | 9 | 5.6 |
| 50–59 | 42 | 26.1 |
| 60–69 | 21 | 13.0 |
| 70–79 | 38 | 23.6 |
| 80–89 | 16 | 9.9 |
| 90+ | 4 | 2.5 |
| Unknown | 11 | 6.8 |
| Sex | ||
| Female | 109 | 67.7 |
| Male | 51 | 31.7 |
| Unknown | 1 | 0.6 |
| Origin | ||
| Australia | 1 | 0.6 |
| Asia | 18 | 11.2 |
| Europe | 86 | 53.4 |
| United States | 48 | 29.8 |
| Foreign (nonspecific) | 3 | 1.9 |
| Unknown | 5 | 3.1 |
| Frequency (n) | % | |
|---|---|---|
| Type of Vaccine | ||
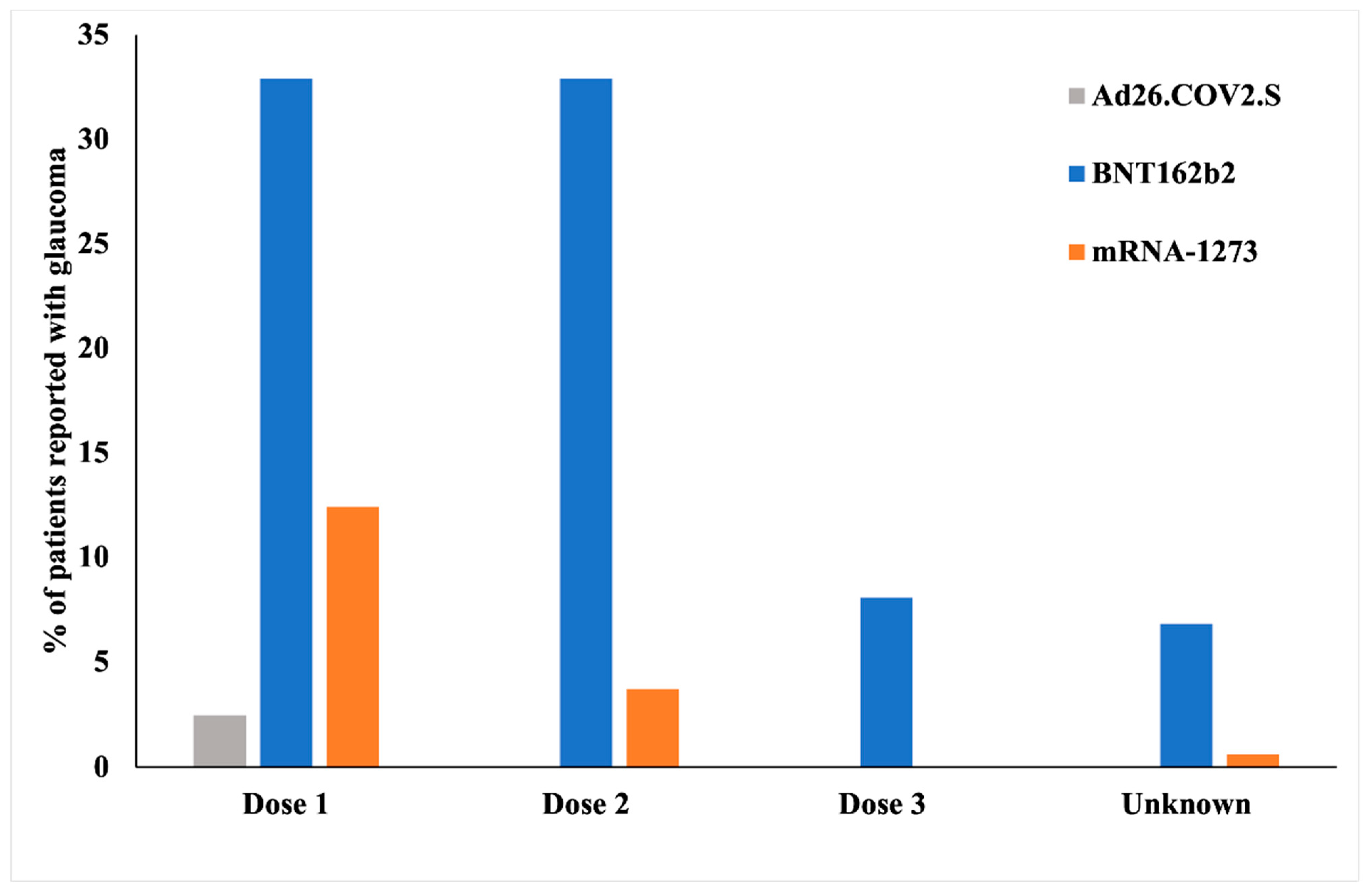
| Ad26.COV2.S | 4 | 2.5 |
| BNT162b2 | 130 | 80.7 |
| mRNA-1273 | 27 | 16.8 |
| Dosage | ||
| 1 | 77 | 47.8 |
| 2 | 59 | 36.6 |
| 3 | 13 | 8.1 |
| Unknown | 12 | 7.5 |
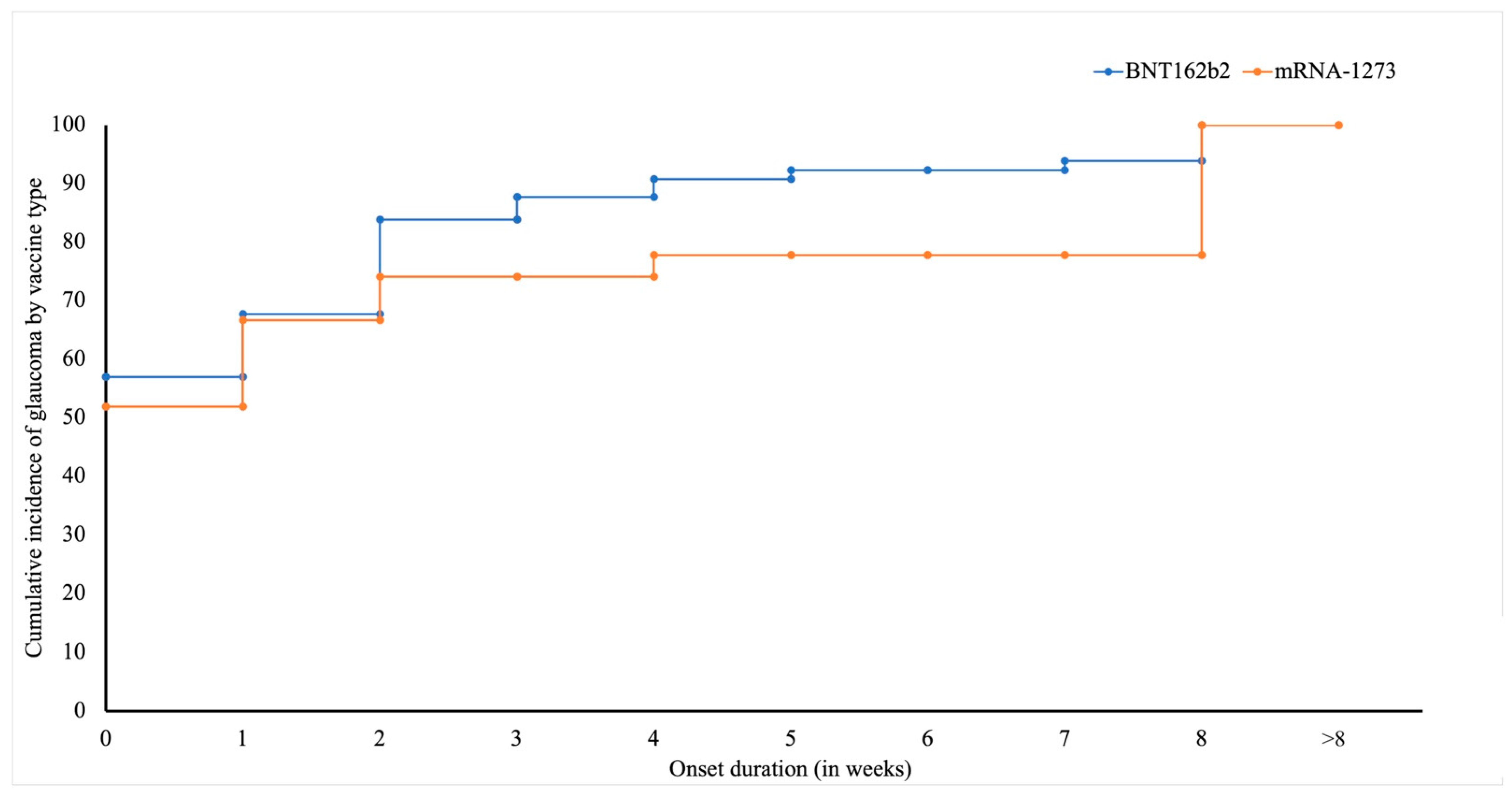
| Median Onset Interval (in days) | 4 | |
| Onset Interval Post-Vaccination | ||
| Day 0 | 29 | 18.0 |
| Days 1–7 | 62 | 38.5 |
| Days 8–14 | 18 | 11.2 |
| Days 15–21 | 9 | 5.6 |
| Days 22–28 | 5 | 3.1 |
| Days 29–35 | 5 | 3.1 |
| Days 36–42 | 2 | 1.2 |
| Days 42–49 | 0 | 0.0 |
| Days 50–56 | 2 | 1.2 |
| Days 56+ | 14 | 8.7 |
| Unknown | 15 | 9.3 |
| Frequency | % | |
|---|---|---|
| History of COVID-19 | 5 | 3.1 |
| Glaucoma Diagnosis | ||
| Open-angle glaucoma | 105 | 65.2 |
| Angle-closure glaucoma | 45 | 27.6 |
| Unknown | 11 | 6.8 |
| Ocular Presentations | ||
| Flashes | 6 | 3.7 |
| Floaters | 5 | 3.1 |
| High IOP | 48 | 29.8 |
| Ocular pain | 60 | 37.3 |
| Photophobia | 5 | 3.1 |
| Reduced/blurry vision | 47 | 29.2 |
| Vision loss/blindness | 35 | 21.7 |
| Ocular History | ||
| Conjunctivitis | 4 | 2.5 |
| Glaucoma (controlled) | 28 | 17.3 |
| Hemorrhage | 3 | 1.9 |
| Herpes zoster ophthalmicus | 5 | 3.1 |
| Keratitis | 2 | 1.2 |
| Ocular ischemic syndrome | 1 | 0.6 |
| Optic ischemic neuropathy | 1 | 0.6 |
| Retinal artery occlusion | 1 | 0.6 |
| Retinal vein occlusion | 6 | 3.7 |
| Uveitis | 7 | 4.3 |
| Vitreous detachment | 2 | 1.2 |
| Systemic Presentation | ||
| Headache | 48 | 29.8 |
| Pain | 17 | 10.6 |
| Nausea | 12 | 7.5 |
| Palpitations | 4 | 2.5 |
| High blood pressure | 8 | 5.0 |
| Vaccine site induration/rash | 6 | 3.7 |
| Systemic History | ||
| Allergies | 9 | 5.6 |
| Cardiovascular disorders (MI, CAD, Afib, tachyarrhythmia, heart failure) | 33 | 20.5 |
| Cerebrovascular disorders | 3 | 1.9 |
| Diabetes | 9 | 5.6 |
| Hypercholesterolemia/Dyslipidemia | 7 | 4.3 |
| Hypertension | 13 | 8.1 |
| Hypothyroidism | 11 | 6.8 |
| Pulmonary disorders (COPD, embolism) | 4 | 2.5 |
| Renal disorders | 5 | 3.1 |
| Percentage (n) | Mean Onset Interval (in Days) | Median Onset Interval (in Days) | p-Value | |
|---|---|---|---|---|
| Vaccine * | ||||
| BNT162b2 | 80.7% (130/161) | 14.7 ± 2.42 | 5 | 0.013 * |
| mRNA-1273 | 16.7% (27/161) | 37.07 ± 12.71 | 7 | |
| Ad26.COV2.S | 2.5% (4/161) | 5.5 ± 3.2 | 3 | |
| Sex * | ||||
| Female | 67.7% (109/161) | 15.17 ± 2.98 | 4 | 0.196 |
| Male | 31.7% (51/161) | 24.6 ± 6.65 | 9 | |
| Age * | ||||
| 10–19 | 1.86% (3/161) | 32 ± 31.03 | 1 | 0.565 |
| 20–29 | 5.6% (9/161) | 21.88 ± 17.74 | 1 | |
| 30–39 | 6.8% (11/161) | 29.81 ± 23.54 | 5 | |
| 40–49 | 8% (13/161) | 12.46 ± 4.95 | 5 | |
| 50–59 | 32.3% (52/161) | 14.90 ± 3.65 | 3.5 | |
| 60–69 | 13% (21/161) | 27.04 ± 8.62 | 8 | |
| 70–79 | 21.7% (35/161) | 15.57 ± 5.23 | 6 | |
| 80–89 | 8.7% (14/161) | 20.71 ± 12.13 | 10 | |
| 90+ | 1.86% (3/161) | 12 ± 10.51 | 2 | |
| Dosage * | ||||
| 1 | 47.8% (77/161) | 15.34 ± 4.26 | 4 | 0.268 |
| 2 | 36.6% (59/161) | 23.64 ± 5.60 | 9 | |
| 3 | 8.07% (13/161) | 17.61 ± 6.35 | 6 | |
| Unknown | 7.45% (12/161) | |||
| History of COVID-19 ** | ||||
| Yes | 3.1% (5/161) | 54.2 ± 32.5 | 33 | 0.08 |
| No | 96.27% (155/161) | 17.18 ± 2.86 | 5 | |
| Unknown | 0.62% (1/161) | |||
| BNT162b2 (Pfizer BioNTech) | mRNA-1273 | Ad26.COV2.S | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unknown | 1 | 2 | 3 | χ2 | p-value | Unknown | 1 | 2 | χ2 | p-value | Unknown | 1 | χ2 | p-value | |
| Age (in years) | 19.17 | 0.742 | 26.2 | 0.047 * | 1.333 | 0.995 | |||||||||
| 10–19 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 1 | ||||||
| 20–29 | 0 | 2 | 4 | 0 | 0 | 1 | 0 | 0 | 0 | ||||||
| 30–39 | 2 | 6 | 2 | 0 | 1 | 1 | 0 | 0 | 0 | ||||||
| 40–49 | 1 | 5 | 4 | 1 | 0 | 1 | 0 | 0 | 0 | ||||||
| 50–59 | 4 | 16 | 16 | 4 | 0 | 0 | 1 | 0 | 2 | ||||||
| 60–69 | 0 | 4 | 7 | 3 | 0 | 9 | 1 | 0 | 1 | ||||||
| 70–79 | 1 | 14 | 13 | 4 | 0 | 5 | 2 | 0 | 0 | ||||||
| 80–89 | 3 | 5 | 4 | 1 | 0 | 3 | 0 | 0 | 0 | ||||||
| 90+ | 0 | 1 | 1 | 0 | 0 | 0 | 2 | 0 | 0 | ||||||
| Sex | 0.555 | 0.906 | 0.905 | 0.636 | 1.333 | 0.248 | |||||||||
| Male | 3 | 16 | 15 | 5 | 0 | 8 | 3 | 0 | 2 | ||||||
| Female | 8 | 37 | 38 | 8 | 1 | 12 | 3 | 0 | 2 | ||||||
| Onset Interval (in days) | 21.08 | 0.275 | 16.78 | 0.157 | 1.333 | 0.987 | |||||||||
| 0 | 1 | 9 | 13 | 2 | 0 | 4 | 0 | 0 | 0 | ||||||
| 1–7 | 3 | 25 | 16 | 5 | 1 | 9 | 0 | 0 | 3 | ||||||
| 8–14 | 1 | 4 | 8 | 1 | 0 | 2 | 2 | 0 | 0 | ||||||
| 15–21 | 4 | 10 | 6 | 1 | 0 | 2 | 0 | 0 | 1 | ||||||
| 22–28 | 1 | 1 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | ||||||
| 29–35 | 1 | 1 | 2 | 0 | 0 | 0 | 1 | 0 | 0 | ||||||
| 36–42 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | ||||||
| 43–49 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||||||
| 49–56 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | ||||||
| 56+ | 0 | 2 | 5 | 1 | 0 | 3 | 3 | 0 | 0 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, R.B.; Parmar, U.P.S.; Cho, W.; Ichhpujani, P. Glaucoma Cases Following SARS-CoV-2 Vaccination: A VAERS Database Analysis. Vaccines 2022, 10, 1630. https://doi.org/10.3390/vaccines10101630
Singh RB, Parmar UPS, Cho W, Ichhpujani P. Glaucoma Cases Following SARS-CoV-2 Vaccination: A VAERS Database Analysis. Vaccines. 2022; 10(10):1630. https://doi.org/10.3390/vaccines10101630
Chicago/Turabian StyleSingh, Rohan Bir, Uday Pratap Singh Parmar, Wonkyung Cho, and Parul Ichhpujani. 2022. "Glaucoma Cases Following SARS-CoV-2 Vaccination: A VAERS Database Analysis" Vaccines 10, no. 10: 1630. https://doi.org/10.3390/vaccines10101630
APA StyleSingh, R. B., Parmar, U. P. S., Cho, W., & Ichhpujani, P. (2022). Glaucoma Cases Following SARS-CoV-2 Vaccination: A VAERS Database Analysis. Vaccines, 10(10), 1630. https://doi.org/10.3390/vaccines10101630