
Association between Adverse Reactions and Humoral Immune Response No Longer Detectable after BNT162b2 Booster Vaccination
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. SARS-CoV-2 Binding Antibodies
2.3. SARS-CoV-2 Nucleocapsid Antibodies
2.4. Wild Type (Wuhan) Neutralization Test (NT)
2.5. Statistical Analysis
2.6. Ethical Issues
3. Results
3.1. Participants
3.2. Waning Immunity over Time and Immunogenicity of BNT162b2 Booster Vaccination
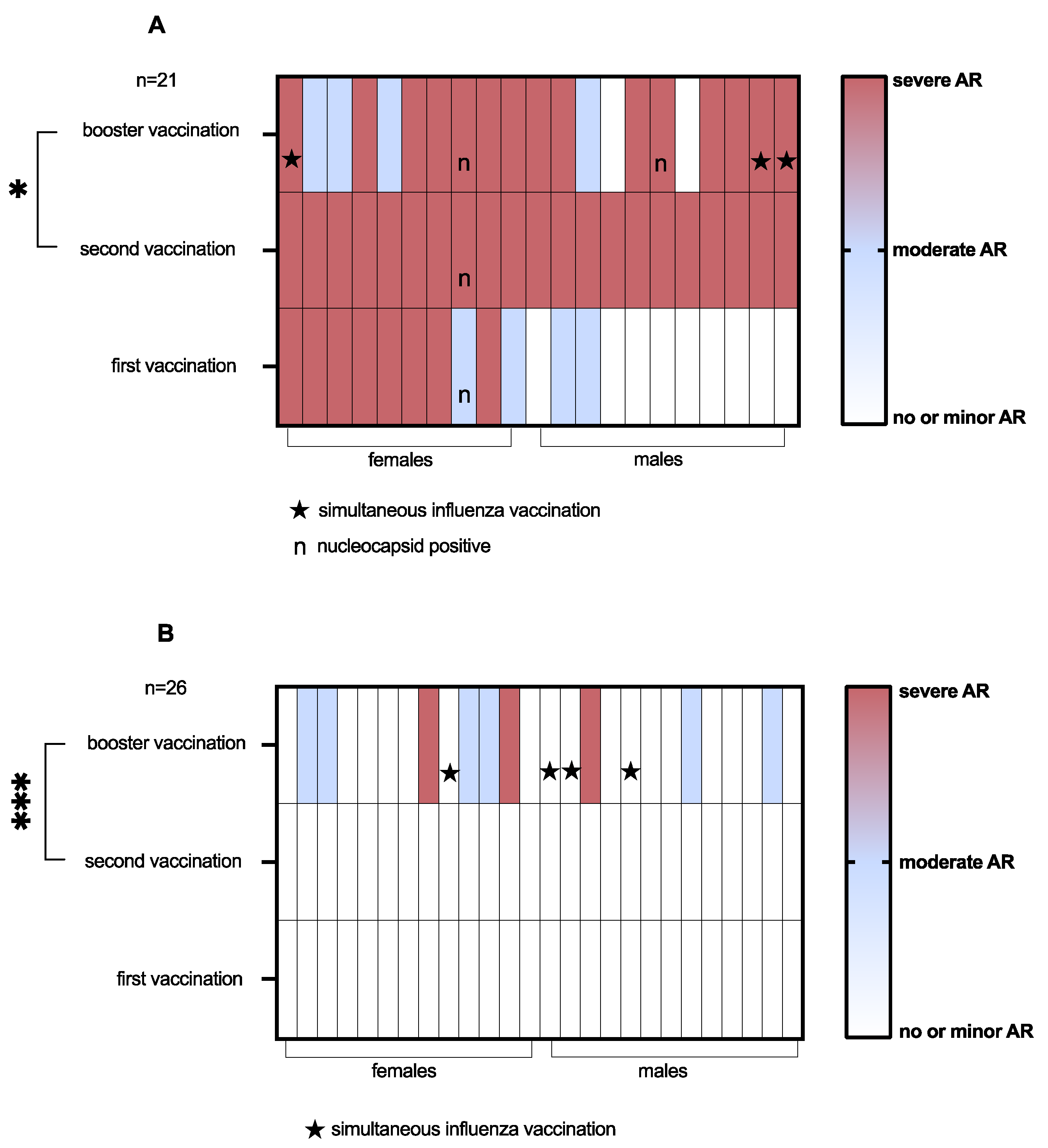
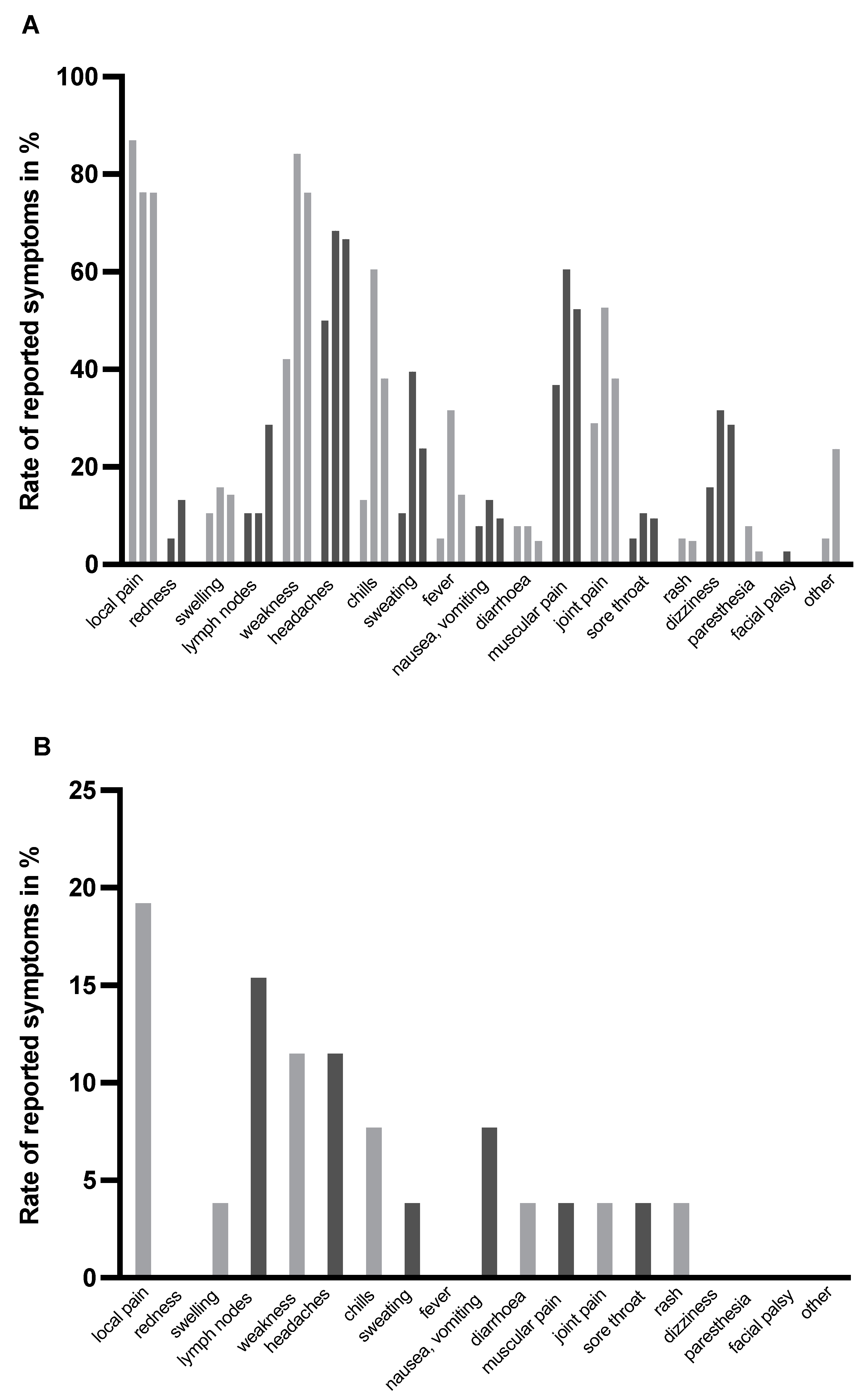
3.3. Reactogenicity of Vaccinations
3.4. Association of Immunogenicity and Reactogenicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FDA Pfizer-BioNTech COVID-19 Vaccine Emergency Use Authorization Review Memorandum. Available online: https://www.fda.gov/media/144416/download (accessed on 19 September 2022).
- European Commission Commission Implementing Decision of 21.12.2020 Granting a Conditional Marketing Authorisation under Regulation (EC) No 726/2004 of the European Parliament and of the Council for “Comirnaty—COVID-19 MRNA Vaccine (Nucleoside Modified)”, a Medicinal Product for Human Use. Available online: https://vaccinare-covid.gov.ro/wp-content/uploads/2020/12/Decizie_autorizare-vaccin-Comisia-Europeana.pdf (accessed on 19 September 2022).
- Hervé, C.; Laupèze, B.; Del Giudice, G.; Didierlaurent, A.M.; Tavares Da Silva, F. The how’s and what’s of vaccine reactogenicity. Npj Vaccines 2019, 4, 39. [Google Scholar] [CrossRef]
- Bauernfeind, S.; Salzberger, B.; Hitzenbichler, F.; Scigala, K.; Einhauser, S.; Wagner, R.; Gessner, A.; Koestler, J.; Peterhoff, D. Association between reactogenicity and immunogenicity after vaccination with BNT162b2. Vaccines 2021, 9, 1089. [Google Scholar] [CrossRef]
- Uwamino, Y.; Kurafuji, T.; Sato, Y.; Tomita, Y.; Shibata, A.; Tanabe, A.; Yatabe, Y.; Noguchi, M.; Arai, T.; Ohno, A.; et al. Young age, female sex, and presence of systemic adverse reactions are associated with high post-vaccination antibody titer after two doses of BNT162b2 MRNA SARS-CoV-2 vaccination: An observational study of 646 Japanese Healthcare workers and university staff. Vaccine 2022, 40, 1019–1025. [Google Scholar] [CrossRef]
- Lin, T.-Y.; Hung, N.-K.; Hung, S.-C. Association of reactogenicity with immunogenicity of the ChAdOx1 NCoV-19 vaccine in patients undergoing hemodialysis. Vaccines 2022, 10, 1366. [Google Scholar] [CrossRef]
- Kanizsai, A.; Molnar, T.; Varnai, R.; Zavori, L.; Tőkés-Füzesi, M.; Szalai, Z.; Berecz, J.; Csecsei, P. Fever after vaccination against SARS-CoV-2 with MRNA-based vaccine associated with higher antibody levels during 6 months follow-up. Vaccines 2022, 10, 447. [Google Scholar] [CrossRef]
- Rechavi, Y.; Shashar, M.; Lellouche, J.; Yana, M.; Yakubovich, D.; Sharon, N. Occurrence of BNT162b2 vaccine adverse reactions is associated with enhanced SARS-CoV-2 IgG antibody response. Vaccines 2021, 9, 977. [Google Scholar] [CrossRef]
- Jubishi, D.; Okamoto, K.; Hamada, K.; Ishii, T.; Hashimoto, H.; Shinohara, T.; Yamashita, M.; Wakimoto, Y.; Otani, A.; Hisasue, N.; et al. The Association between adverse reactions and immune response against SARS-CoV-2 spike protein after vaccination with BNT162b2 among healthcare workers in a single healthcare system: A prospective observational cohort study. Hum. Vaccines Immunother. 2022, 18, 1–10. [Google Scholar] [CrossRef]
- Dickerson, J.A.; Englund, J.A.; Wang, X.; Brown, J.C.; Zerr, D.M.; Strelitz, B.; Klein, E.J. Higher antibody concentrations in U.S. health care workers associated with greater reactogenicity post-vaccination. Vaccines 2022, 10, 601. [Google Scholar] [CrossRef]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- Yamamoto, S.; Fukunaga, A.; Tanaka, A.; Takeuchi, J.S.; Inoue, Y.; Kimura, M.; Maeda, K.; Ueda, G.; Mizoue, T.; Ujiie, M.; et al. Association between reactogenicity and SARS-CoV-2 antibodies after the second dose of the BNT162b2 COVID-19 vaccine. Vaccine 2022, 40, 1924–1927. [Google Scholar] [CrossRef]
- Takeuchi, M.; Higa, Y.; Esaki, A.; Nabeshima, Y.; Nakazono, A. Does reactogenicity after a second injection of the BNT162b2 vaccine predict spike IgG antibody levels in healthy Japanese subjects? PLoS ONE 2021, 16, e0257668. [Google Scholar] [CrossRef]
- Coggins, S.A.; Laing, E.D.; Olsen, C.H.; Goguet, E.; Moser, M.; Jackson-Thompson, B.M.; Samuels, E.C.; Pollett, S.D.; Tribble, D.R.; Davies, J.; et al. Adverse effects and antibody titers in response to the BNT162b2 MRNA COVID-19 vaccine in a prospective study of healthcare workers. Open Forum Infect. Dis. 2022, 9, ofab575. [Google Scholar] [CrossRef]
- Hwang, Y.H.; Song, K.-H.; Choi, Y.; Go, S.; Choi, S.-J.; Jung, J.; Kang, C.K.; Choe, P.G.; Kim, N.-J.; Park, W.B.; et al. Can reactogenicity predict immunogenicity after COVID-19 vaccination? Korean J. Intern. Med. 2021, 36, 1486–1491. [Google Scholar] [CrossRef]
- Brown, C.M.; Vostok, J.; Johnson, H.; Burns, M.; Gharpure, R.; Sami, S.; Sabo, R.T.; Hall, N.; Foreman, A.; Schubert, P.L.; et al. Outbreak of SARS-CoV-2 infections, including COVID-19 vaccine breakthrough infections, associated with large public gatherings—Barnstable county, Massachusetts, July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1059–1062. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. Covid-19 vaccine effectiveness in New York state. N. Engl. J. Med. 2022, 386, 116–127. [Google Scholar] [CrossRef]
- Peterhoff, D.; Glück, V.; Vogel, M.; Schuster, P.; Schütz, A.; Neubert, P.; Albert, V.; Frisch, S.; Kiessling, M.; Pervan, P.; et al. A highly specific and sensitive serological assay detects SARS-CoV-2 antibody levels in COVID-19 patients that correlate with neutralization. Infection 2021, 49, 75–82. [Google Scholar] [CrossRef]
- Einhauser, S.; Peterhoff, D.; Niller, H.H.; Beileke, S.; Günther, F.; Steininger, P.; Burkhardt, R.; Heid, I.M.; Pfahlberg, A.B.; Überla, K.; et al. Spectrum bias and individual strengths of SARS-CoV-2 Serological tests—A population-based evaluation. Diagnostics 2021, 11, 1843. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex Differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Niesen, M.J.M.; Pawlowski, C.; O’Horo, J.C.; Challener, D.W.; Silvert, E.; Donadio, G.; Lenehan, P.J.; Virk, A.; Swift, M.D.; Speicher, L.L.; et al. Surveillance of safety of 3 doses of COVID-19 MRNA vaccination using electronic health records. JAMA Netw. Open 2022, 5, e227038. [Google Scholar] [CrossRef]
- Hause, A.M.; Baggs, J.; Marquez, P.; Myers, T.R.; Su, J.R.; Blanc, P.G.; Gwira Baumblatt, J.A.; Woo, E.J.; Gee, J.; Shimabukuro, T.T.; et al. Safety monitoring of COVID-19 vaccine booster doses among adults—United States, September 22, 2021–February 6, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect. Dis. 2022, 22, 1002–1010. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and heterologous Covid-19 booster vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- Moreira, E.D.; Kitchin, N.; Xu, X.; Dychter, S.S.; Lockhart, S.; Gurtman, A.; Perez, J.L.; Zerbini, C.; Dever, M.E.; Jennings, T.W.; et al. Safety and efficacy of a third dose of BNT162b2 Covid-19 vaccine. N. Engl. J. Med. 2022, 386, 1910–1921. [Google Scholar] [CrossRef]
- Falsey, A.R.; Frenck, R.W.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 neutralization with BNT162b2 vaccine dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| After Second Vaccination | Before Booster Vaccination | After Booster Vaccination | |
|---|---|---|---|
| Total number of participants | 76 | 65 | 47 |
| Age—years (median, range) | 43 (23–64) | 44 (23–64) | 44 (23–64) |
| Sex—n (%) females | 36 (47.4) | 32 (49.2) | 23 (48.9) |
| Any chronic disease—n (%) | 19 (25.0) | 18 (27.7) | 15 (31.9) |
| Smoking—n (%) | 5 (6.6) | 5 (7.7) | 5 (10.6) |
| Body-mass index (median, range) | 24.4 (17.6–35.9) | 24.6 (17.6–35.9) | 24.5 (17.6–32.1) |
| Nucleocapsid positive—n (%) | 3 (3.9) | 3 (4.6) | 2 (4.3) |
| Simultaneous influenza vaccination | 7 (14.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bauernfeind, S.; Einhauser, S.; Tydykov, L.; Mader, A.-L.; Salzberger, B.; Hitzenbichler, F.; Mohr, A.; Burkhardt, R.; Wagner, R.; Peterhoff, D. Association between Adverse Reactions and Humoral Immune Response No Longer Detectable after BNT162b2 Booster Vaccination. Vaccines 2022, 10, 1608. https://doi.org/10.3390/vaccines10101608
Bauernfeind S, Einhauser S, Tydykov L, Mader A-L, Salzberger B, Hitzenbichler F, Mohr A, Burkhardt R, Wagner R, Peterhoff D. Association between Adverse Reactions and Humoral Immune Response No Longer Detectable after BNT162b2 Booster Vaccination. Vaccines. 2022; 10(10):1608. https://doi.org/10.3390/vaccines10101608
Chicago/Turabian StyleBauernfeind, Stilla, Sebastian Einhauser, Leonid Tydykov, Anna-Lena Mader, Bernd Salzberger, Florian Hitzenbichler, Arno Mohr, Ralph Burkhardt, Ralf Wagner, and David Peterhoff. 2022. "Association between Adverse Reactions and Humoral Immune Response No Longer Detectable after BNT162b2 Booster Vaccination" Vaccines 10, no. 10: 1608. https://doi.org/10.3390/vaccines10101608
APA StyleBauernfeind, S., Einhauser, S., Tydykov, L., Mader, A.-L., Salzberger, B., Hitzenbichler, F., Mohr, A., Burkhardt, R., Wagner, R., & Peterhoff, D. (2022). Association between Adverse Reactions and Humoral Immune Response No Longer Detectable after BNT162b2 Booster Vaccination. Vaccines, 10(10), 1608. https://doi.org/10.3390/vaccines10101608