
COVID-19 Pediatric Vaccine Hesitancy among Racially Diverse Parents in the United States


Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, J. Epidemiology of COVID-19 in Children Aged 5–11 Years; Epidemiology Task Force CDC COVID-19 Public Health Response; Advisory Committee on Immunization Practices (ACIP) Meeting, 2 November, 2021. Available online: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-11-2-3/03-Covid-Jefferson-508.pdf (accessed on 29 October 2021).
- Lee, E.H.; Kepler, K.L.; Geevarughese, A.; Paneth-Pollak, R.; Dorsinville, M.S.; Ngai, S.; Reilly, K.H. Race/Ethnicity Among Children With COVID-19–Associated Multisystem Inflammatory Syndrome. JAMA Netw. Open 2020, 3, e2030280. [Google Scholar] [CrossRef] [PubMed]
- Fraiman, Y.S.; Litt, J.S.; Davis, J.M.; Pursley, D.M. Racial and ethnic disparities in adult COVID-19 and the future impact on child health. Pediatr. Res. 2021, 89, 1052–1054. [Google Scholar] [CrossRef] [PubMed]
- Artiga, S.; Hill, L.; Ndugga, N. Racial Disparities in COVID-19 Impacts and Vaccinations for Children. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/racial-disparities-in-covid-19-impacts-and-vaccinations-for-children/# (accessed on 16 November 2021).
- FDA. FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Children 5 through 11 Years of Age; FDA: Silver Spring, MD, USA, 29 October 2021. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-pfizer-biontech-covid-19-vaccine-emergency-use-children-5-through-11-years-age (accessed on 2 November 2021).
- Murthy, B.P.; Zell, E.; Saelee, R.; Murthy, N.; Meng, L.; Meador, S.; Reed, K.; Shaw, L.; Gibbs-Scharf, L.; McNaghten, A. COVID-19 vaccination coverage among adolescents aged 12–17 years—United States, December 14, 2020–July 31, 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Goldman, R.D.; Staubli, G.; Cotanda, C.P.; Brown, J.C.; Hoeffe, J.; Seiler, M.; Gelernter, R.; Hall, J.E.; Griffiths, M.A.; Davis, A.L. Factors associated with parents’ willingness to enroll their children in trials for COVID-19 vaccination. Hum. Vaccines Immunother. 2021, 17, 1607–1611. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, K.M.; Wong, J.; Sweeney, C.F.; Avola, A.; Auger, A.; Macaluso, M.; Reidy, P. Parents’ Intentions to Vaccinate Their Children Against COVID-19. J. Pediatr. Health Care 2021, 35, 509–517. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Shah, M.D.; Delgado, J.R.; Thomas, K.; Vizueta, N.; Cui, Y.; Vangala, S.; Shetgiri, R.; Kapteyn, A. Parents’ intentions and perceptions about COVID-19 vaccination for their children: Results from a national survey. Pediatrics 2021, 148, e2021052335. [Google Scholar] [CrossRef]
- Teasdale, C.A.; Borrell, L.N.; Kimball, S.; Rinke, M.L.; Rane, M.; Fleary, S.A.; Nash, D. Plans to vaccinate children for COVID-19: A survey of US parents. Pediatrics 2021, 237, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Babicki, M.; Pokorna-Kałwak, D.; Doniec, Z.; Mastalerz-Migas, A. Attitudes of Parents with Regard to Vaccination of Children against COVID-19 in Poland. A Nationwide Online Survey. Vaccines 2021, 9, 1192. [Google Scholar] [CrossRef] [PubMed]
- Bagateli, L.E.; Saeki, E.Y.; Fadda, M.; Agostoni, C.; Marchisio, P.; Milani, G.P. COVID-19 Vaccine Hesitancy among Parents of Children and Adolescents Living in Brazil. Vaccines 2021, 9, 1115. [Google Scholar] [CrossRef]
- Choi, S.-H.; Jo, Y.H.; Jo, K.J.; Park, S.E. Pediatric and Parents’ Attitudes Towards COVID-19 Vaccines and Intention to Vaccinate for Children. J. Korean Med Sci. 2021, 36, e227. [Google Scholar] [CrossRef] [PubMed]
- Montalti, M.; Di Valerio, Z.; Rallo, F.; Squillace, L.; Costantino, C.; Tomasello, F.; Mauro, G.L.; Stillo, M.; Perrone, P.; Resi, D. Attitudes toward the SARS-CoV-2 and Influenza Vaccination in the Metropolitan Cities of Bologna and Palermo, Italy. Vaccines 2021, 9, 1200. [Google Scholar] [CrossRef]
- Zhang, M.-X.; Lin, X.-Q.; Chen, Y.; Tung, T.-H.; Zhu, J.-S. Determinants of parental hesitancy to vaccinate their children against COVID-19 in China. Expert Rev. Vaccines 2021, 20, 1339–1349. [Google Scholar] [CrossRef] [PubMed]
- Shiri, T.; Evans, M.; Talarico, C.A.; Morgan, A.R.; Mussad, M.; Buck, P.O.; McEwan, P.; Strain, W.D. Vaccinating Adolescents and Children Significantly Reduces COVID-19 Morbidity and Mortality across All Ages: A Popula-Tion-Based Modeling Study Using the UK as an Example. Vaccines 2021, 9, 1180. [Google Scholar] [CrossRef] [PubMed]
- Aschwanden, C. Five reasons why COVID herd immunity is probably impossible. Nature 2021, 591, 520–522. [Google Scholar] [CrossRef] [PubMed]
- Alfieri, N.L.; Kusma, J.D.; Heard-Garris, N.; Davis, M.M.; Golbeck, E.; Barrera, L.; Macy, M.L. Parental COVID-19 vaccine hesitancy for children: Vulnerability in an urban hotspot. BMC Public Health 2021, 21, 1662. [Google Scholar] [CrossRef] [PubMed]
- Shacham, E.; Little, G.; Scroggins, S.; Fredman, A.; Wray, R.; Charney, R. Intent to Vaccinate Children against COVID-19: Low levels of trust in public health agencies trust across rural communities. SocArXiv 2021. [Google Scholar] [CrossRef]
- Trujillo, K.; Pippert, C.; Lazer, D.; Baum, M.; Simonson, M.; Perlis, R.; Ognyanova, K.; Druckman, J.; Santillana, M.; Quintana, A.; et al. The COVID States Project COVID-19 Survey Report #68: Heightened Parental Concerns about COVID-19 Vaccinationd for Children. Report # 74. 2021. Available online: www.covidstates.org (accessed on 24 December 2021).
- Teherani, M.; Banskota, S.; Camacho-Gonzalez, A.; Smith, A.G.; Anderson, E.J.; Kao, C.M.; Crepy D’Orleans, C.; Shane, A.L.; Lu, A.; Jaggi, P. Intent to Vaccinate SARS-CoV-2 Infected Children in US Households: A Survey. Vaccines 2021, 9, 1049. [Google Scholar] [CrossRef]
- Teasdale, C.A.; Borrell, L.N.; Shen, Y.; Kimball, S.; Rinke, M.L.; Fleary, S.A.; Nash, D.N. Parental plans to vaccinate children for COVID-19 in New York City. Vaccine 2021, 39, 5082–5086. [Google Scholar] [CrossRef]
- Temsah, M.-H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O. Parental Attitudes and Hesitancy About COVID-19 vs. Routine Childhood Vaccinations: A National Survey. Front. Public Health 2021, 9, 1513. [Google Scholar] [CrossRef] [PubMed]
- Flood, E.M.; Rousculp, M.D.; Ryan, K.J.; Beusterien, K.M.; Divino, V.M.; Toback, S.L.; Sasané, M.; Block, S.L.; Hall, M.C.; Mahadevia, P.J. Parents’ decision-making regarding vaccinating their children against influenza: A web-based survey. Clin. Ther. 2010, 32, 1448–1467. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Humiston, S.G.; Marcuse, E.K.; Zhao, Z.; Dorell, C.G.; Howes, C.; Hibbs, B. Parental delay or refusal of vaccine doses, childhood vaccination coverage at 24 months of age, and the Health Belief Model. Public Health Rep. 2011, 126, 135–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, H.J.; De Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The state of vaccine confidence 2016: Global insights through a 67-country survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Perez, S.; Shapiro, G.K.; Tatar, O.; Joyal-Desmarais, K.; Rosberger, Z. Development and validation of the human papillomavirus attitudes and beliefs scale in a National Canadian sample. Sex. Transm. Dis. 2016, 43, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, S.A.; Savas, L.S.; Baumler, E.; Nyitray, A.G.; Mullen, P.D.; Vernon, S.W.; Fernandez, M.E. Parental predictors of HPV vaccine initiation among low-income Hispanic females aged 11–17 years. Vaccine 2018, 36, 5084–5090. [Google Scholar] [CrossRef] [PubMed]
- Goss, M.D.; Temte, J.L.; Barlow, S.; Temte, E.; Bell, C.; Birstler, J.; Chen, G. An assessment of parental knowledge, attitudes, and beliefs regarding influenza vaccination. Vaccine 2020, 38, 1565–1571. [Google Scholar] [CrossRef]
- Cancer Treatment Centers of America. Cervical Cancer Risk Factors. 2021. Available online: https://www.cancer.org/cancer/cervical-cancer/causes-risks-prevention/risk-factors.html (accessed on 24 December 2021).
- Grinberg, K.; Sela, Y. What Affects Maternal Response to Measles Vaccinations? Examining the Health Beliefs Model (HBM). Sci 2021, 3, 20. [Google Scholar] [CrossRef]
- Montalti, M.; Rallo, F.; Guaraldi, F.; Bartoli, L.; Po, G.; Stillo, M.; Perrone, P.; Squillace, L.; Dallolio, L.; Pandolfi, P. Would Parents Get Their Children Vaccinated Against SARS-CoV-2? Rate and Predictors of Vaccine Hesitancy According to a Survey over 5000 Families from Bologna, Italy. Vaccines 2021, 9, 366. [Google Scholar] [CrossRef] [PubMed]
- Hamel, L.; Lopes, L.; Kearney, A.; Krizinger, A.; Sparks, G.; Stokes, M.; Brodie, M. KFF COVID-19 Vaccine Monitor: Parents and the Pandemic. Polling. 2021. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-parents-and-the-pandemic/ (accessed on 24 December 2021).
- Mahase, E. COVID-19: Pfizer reports 100% vaccine efficacy in children aged 12 to 15. BMJ 2021, 373, n881. [Google Scholar] [CrossRef]
- Latkin, C.A.; Dayton, L.; Moran, M.; Strickland, J.C.; Collins, K. Behavioral and psychosocial factors associated with COVID-19 skepticism in the United States. Curr. Psychol. 2021, 40, 1–9. [Google Scholar] [CrossRef]
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. The Federal Retail Pharmacy Program for COVID-19 Vaccination. 2021. Available online: https://www.cdc.gov/vaccines/covid-19/retail-pharmacy-program/index.html (accessed on 24 December 2021).
- Kestenbaum, L.A.; Feemster, K.A. Identifying and Addressing Vaccine Hesitancy. Pediatr. Ann. 2015, 44, e71–e75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, N.E.; The SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- McClure, C.C.; Cataldi, J.R.; O’Leary, S.T. Vaccine Hesitancy: Where We Are and Where We Are Going. Clin. Ther. 2017, 39, 1550–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badr, H.; Zhang, X.; Oluyomi, A.; Woodard, L.D.; Adepoju, O.E.; Raza, S.A.; Amos, C.I. Overcoming COVID-19 Vaccine Hesitancy: Insights from an Online Population-Based Survey in the United States. Vaccines 2021, 9, 1100. [Google Scholar] [CrossRef] [PubMed]
- Ndugga, N.; Artiga, S. Disparities in Health and Health Care: 5 Key Questions and Answers. 2021. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/disparities-in-health-and-health-care-5-key-question-and-answers/ (accessed on 24 December 2021).
- King, W.C.; Rubinstein, M.; Reinhart, A.; Mejia, R.J. Time trends and factors related to COVID-19 vaccine hesitancy from January–May 2021 among US adults: Findings from a large-scale national survey. medRxiv 2021. Posted 25 October. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total Sample n = 400 | Yes or Probably Will n = 163 (40.75%) | Unsure n = 99 (24.75%) | No or Probably Not n = 138 (34.5%) | p-Value | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | ||
| Parent age, M (SD) | 35.83 (7.70) | 36.70 (6.53) | 35.54 (9.50) | 35.00 (7.47) | 0.15 |
| Education | 0.02 * | ||||
| Did not attend college | 107 (26.8%) | 32 (19.6%) | 34 (34.3%) | 41 (29.7%) | |
| Some college or higher | 293 (73.3%) | 131 (80.4%) | 65 (65.7%) | 97 (70.3%) | |
| Annual household income | 0.004 * | ||||
| Less than $20,000 | 156 (39%) | 51 (31.3%) | 49 (49.5%) | 56 (40.6%) | |
| Between $20,000 and $50,999 | 178 (44.5%) | 75 (46%) | 39 (39.4%) | 64 (46.4%) | |
| Between $51,000 and $79,999 | 49 (12.3%) | 27 (16.6%) | 5 (5.1%) | 17 (12.3%) | |
| Preferred not to answer | 17 (4.3%) | 10 (6.1%) | 6 (6.1%) | 1 (0.7%) | |
| Financial security | 0.01 * | ||||
| Cannot make ends meet | 90 (22.5%) | 25 (15.3%) | 30 (30.3%) | 35 (25.4%) | |
| Have just enough or comfortable | 310 (77.5%) | 138 (84.7%) | 69 (69.7%) | 103 (74.6%) | |
| Region of residence | 0.17 | ||||
| Northeast | 66 (16.5%) | 29 (17.8%) | 15 (15.2%) | 22 (15.9%) | |
| Midwest | 132 (33%) | 53 (32.5%) | 41 (41.4%) | 38 (27.5%) | |
| South | 110 (27.5%) | 40 (24.5%) | 29 (29.3%) | 41 (29.7%) | |
| West | 92 (23%) | 41 (25.2%) | 14 (14.1%) | 37 (26.8%) | |
| Parent vaccination status | <0.001 * | ||||
| No | 173 (43.3%) | 19 (11.7%) | 51 (51%) | 103 (74.6%) | |
| Yes | 227 (56.8%) | 144 (88.3%) | 48 (48.5%) | 35 (25.4%) | |
| Parent previously tested for COVID-19 | 0.71 | ||||
| No | 191 (47.8%) | 81 (49.7%) | 44 (44.4%) | 66 (47.8%) | |
| Yes | 209 (52.3%) | 82 (50.3%) | 55 (55.6%) | 72 (52.2%) | |
| Child’s age,M (SD) | 7.66 (1.70) | 7.94 (1.68) | 7.49 (1.62) | 7.46 (1.74) | 0.12 |
| 5 to 7 years old | 194 (48.5%) | 69 (42.3%) | 52 (52.5%) | 73 (52.9%) | |
| 8 to 10 years old | 206 (51.5%) | 94 (57.7%) | 47 (47.5%) | 64 (47.1%) | |
| Child’s gender | 0.16 | ||||
| Male | 214 (53.5) | 77 (47.2%) | 61 (61.6%) | 76 (55.1%) | |
| Female | 185 (46.3) | 85 (52.1%) | 38 (38.4%) | 62 (44.9%) | |
| Gender nonbinary | 1 (0.3) | 1 (0.6%) | 0% | 0% | |
| Child previously tested for COVID-19 | 0.81 | ||||
| No | 200 (50%) | 80 (49.1%) | 49 (49.5%) | 71 (51.4%) | |
| Yes | 196 (49%) | 81 (49.7%) | 50 (50.5%) | 65 (47.1%) | |
| I don’t know | 4 (1%) | 2 (1.2%) | 0% | 2 (1.4%) | |
| Child previously had COVID-19 | 0.34 | ||||
| No | 437 (86.8%) | 144 (88.3%) | 88 (88.9%) | 115 (83.3%) | |
| Yes | 0% | 0% | 0% | 0% | |
| I don’t know | 54 (13.3%) | 19 (11.7%) | 11 (11.1%) | 23 (16.7%) | |
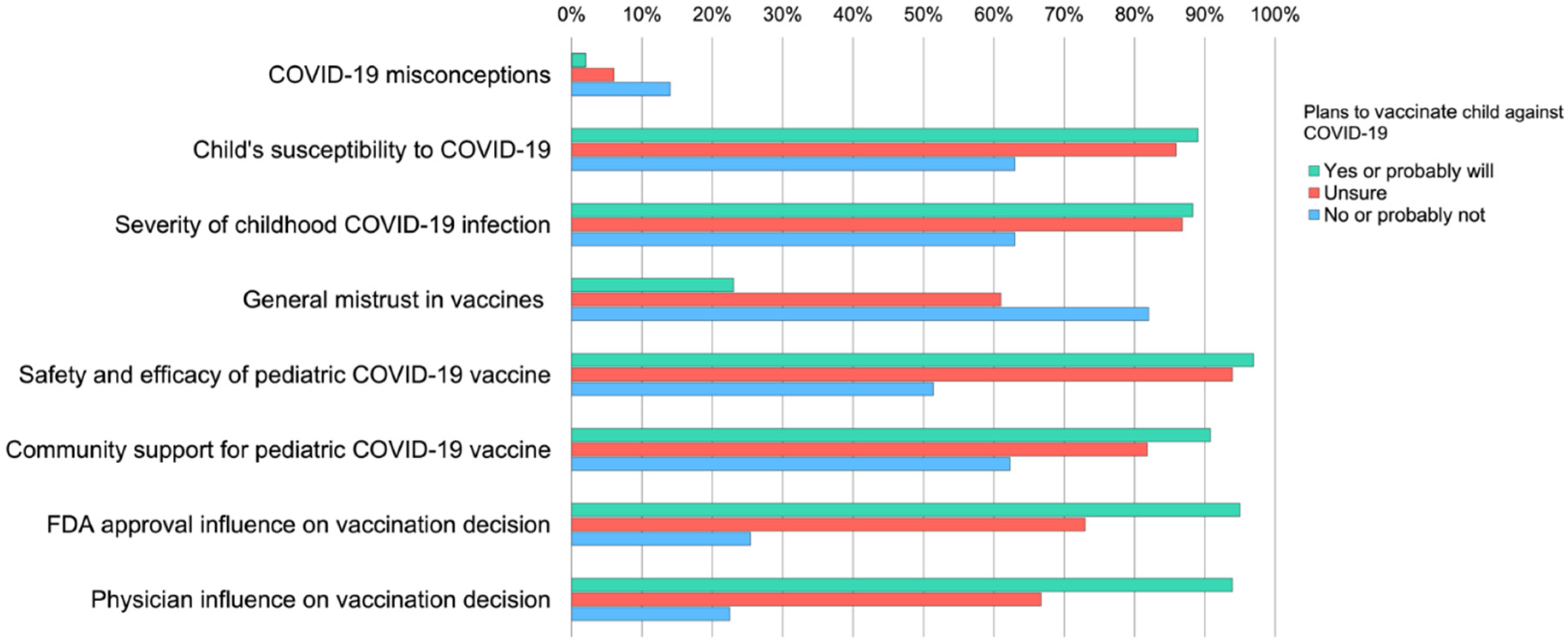
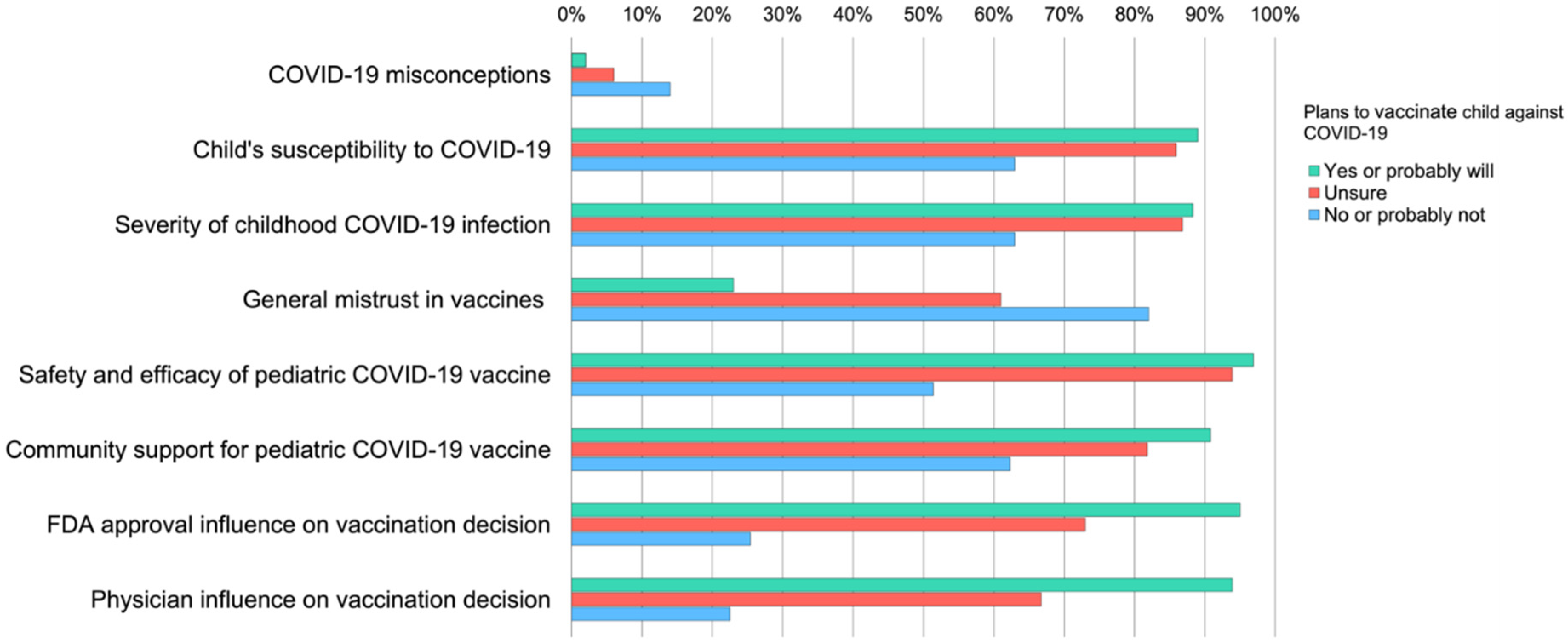
| COVID-19 misconceptions | <0.001 * | ||||
| M (SD) | 1.47 (1.65) | .88 (1.23) | 1.30 (1.51) | 2.28 (1.85) | |
| More COVID-19 misconceptions | 29 (7.2%) | 3 (1.8%) | 6 (6.1%) | 20 (14.5%) | |
| Less COVID-19 misconceptions | 371 (92.8%) | 160 (98.2%) | 93 (93.9%) | 118 (85.5%) | |
| Child’s susceptibility to COVID-19 | <0.001 * | ||||
| M (SD) | 4.06 (1.33) | 4.39 (1.06) | 4.37 (1.22) | 3.45 (1.49) | |
| Greater perceived susceptibility | 317 (79.3%) | 145 (89%) | 85 (85.9%) | 87 (63%) | |
| Less perceived susceptibility | 83 (20.8%) | 18 (11%) | 14 (14.1%) | 51 (37%) | |
| Severity of childhood COVID-19 infection | <0.001 * | ||||
| M (SD) | 3.87 (1.06) | 4.17 (.96) | 4.03 (.96) | 3.41 (1.09) | |
| Greater perceived severity | 317 (79.3%) | 144 (88.3%) | 86 (86.9%) | 87 (63%) | |
| Less perceived severity | 83 (20.8%) | 19 (11.7%) | 13 (13.1%) | 51 (37%) | |
| General mistrust in vaccines | <0.001 * | ||||
| M (SD) | 3.17 (1.24) | 2.41 (1.03) | 3.25 (.89) | 4.01 (1.14) | |
| Greater mistrust in vaccines | 211 (52.8%) | 38 (23.3%) | 60 (60.6%) | 113 (81.9%) | |
| Less mistrust in vaccines | 189 (47.3%) | 125 (76.7%) | 39 (39.4%) | 25 (18.1%) | |
| Safety and efficacy of pediatric COVID-19 vaccine | <0.001 * | ||||
| M (SD) | 3.96 (1.19) | 4.79 (.89) | 3.97 (.80) | 2.98 (.95) | |
| Greater perceived safety and efficacy | 322 (80.5%) | 158 (96.6%) | 93 (93.9%) | 71 (51.4%) | |
| Less perceived safety and efficacy | 78 (19.5%) | 5 (3.1%) | 6 (6.1%) | 67 (48.6%) | |
| Community support for pediatric COVID-19 vaccination | <0.001 * | ||||
| M (SD) | 3.26 (0.94) | 3.68 (0.86) | 3.23 (0.81) | 2.78 (0.89) | |
| Greater perceived community support | 315 (78.8%) | 148 (90.8%) | 81 (81.8%) | 86 (62.3%) | |
| Less perceived community support | 85 (21.3%) | 15 (9.2%) | 18 (18.2%) | 52 (37.7%) | |
| FDA approval influence on vaccination decision | <0.001 * | ||||
| M (SD) | 3.99 (1.70) | 5.20 (.99) | 4.04 (1.17) | 2.52 (1.52) | |
| Greater influence of FDA approval | 261 (65.3%) | 154 (94.5%) | 72 (72.7%) | 35 (25.4%) | |
| Less influence of FDA approval | 139 (34.8%) | 9 (5.5%) | 27 (27.3%) | 103 (74.6%) | |
| Physician influence on vaccination decision | <0.001 * | ||||
| M (SD) | 3.88 (1.69) | 5.06 (.99) | 3.99 (1.30) | 2.39 (1.43) | |
| Greater influence of physician recommendation | 250 (62.5%) | 153 (93.6%) | 66 (66.7%) | 31 (22.5%) | |
| Less influence of physician recommendation | 150 (37.5%) | 10 (6.1%) | 33 (33.3%) | 107 (77.5%) | |
| Total Sample (n = 400) | Non-Hispanic Asian (n = 100) | Non-Hispanic Black (n = 100) | Hispanic/ Latinx (n = 100) | Non-Hispanic White (n = 100) | p-Value | |
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Parent age, M (SD) | 35.83 (7.70) | 36.13 (5.74) | 35.90 (8.02) | 33.91 (7.24) | 37.37 (9.10) | 0.01 * |
| Education | 0.25 | |||||
| Did not attend college | 107 (26.8%) | 19% | 30% | 29% | 29% | |
| Some college or higher | 293 (73.3%) | 81% | 70% | 71% | 71% | |
| Annual household income | <0.001 * | |||||
| Less than $20,000 | 156 (39%) | 31% | 52% | 31% | 42% | |
| Between $20,000 and $50,999 | 178 (44.5%) | 43% | 41% | 54% | 40% | |
| Between $51,000 and $79,999 | 49 (12.3%) | 15% | 4% | 14% | 16% | |
| Preferred not to answer | 17 (4.3%) | 11% | 3% | 1% | 2% | |
| Financial security | 0.04 | |||||
| Cannot make ends meet | 90 (22.5%) | 15% | 32% | 21% | 22% | |
| Have just enough or comfortable | 310 (77.5%) | 85% | 68% | 79% | 78% | |
| Region of residence | 0.23 | |||||
| Northeast | 66 (16.5%) | 14% | 13% | 15% | 24% | |
| Midwest | 132 (33%) | 34% | 34% | 36% | 28% | |
| South | 110 (27.5%) | 23% | 35% | 25% | 27% | |
| West | 92 (23%) | 29% | 18% | 24% | 21% | |
| Parent vaccination status | <0.001 * | |||||
| No | 173 (43.3%) | 23% | 56% | 42% | 52% | |
| Yes | 227 (56.8%) | 77% | 44% | 58% | 48% | |
| Parent previously tested for COVID-19 | 0.15 | |||||
| No | 191 (47.8%) | 53% | 46% | 39% | 53% | |
| Yes | 209 (52.3%) | 47% | 54% | 61% | 47% | |
| Child’s age,M (SD) | 7.66 (1.70) | 7.88 (1.59) | 7.81 (1.72) | 7.81 (1.73) | 7.14 (1.67) | <0.001 * |
| 5 to 7 years old | 194 (48.5%) | 44% | 43% | 40% | 67% | |
| 8 to 10 years old | 206 (51.5%) | 56% | 57% | 60% | 33% | |
| Child’s gender | 0.16 | |||||
| Male | 214 (53.5) | 44% | 54% | 62% | 54% | |
| Female | 185 (46.3) | 55% | 46% | 38% | 46% | |
| Gender nonbinary | 1 (0.3) | 1% | 0% | 0% | 0% | |
| Child previously tested for COVID-19 | 0.44 | |||||
| No | 200 (50%) | 58% | 46% | 45% | 51% | |
| Yes | 196 (49%) | 42% | 52% | 54% | 48% | |
| I don’t know | 4 (1%) | 0% | 2% | 1% | 1% | |
| Child previously had COVID-19 | 0.03 * | |||||
| No | 437 (86.8%) | 94% | 89% | 81% | 83% | |
| Yes | 0% | 0% | 0% | 0% | 0% | |
| I don’t know | 54 (13.3%) | 6% | 11% | 18% | 17% | |
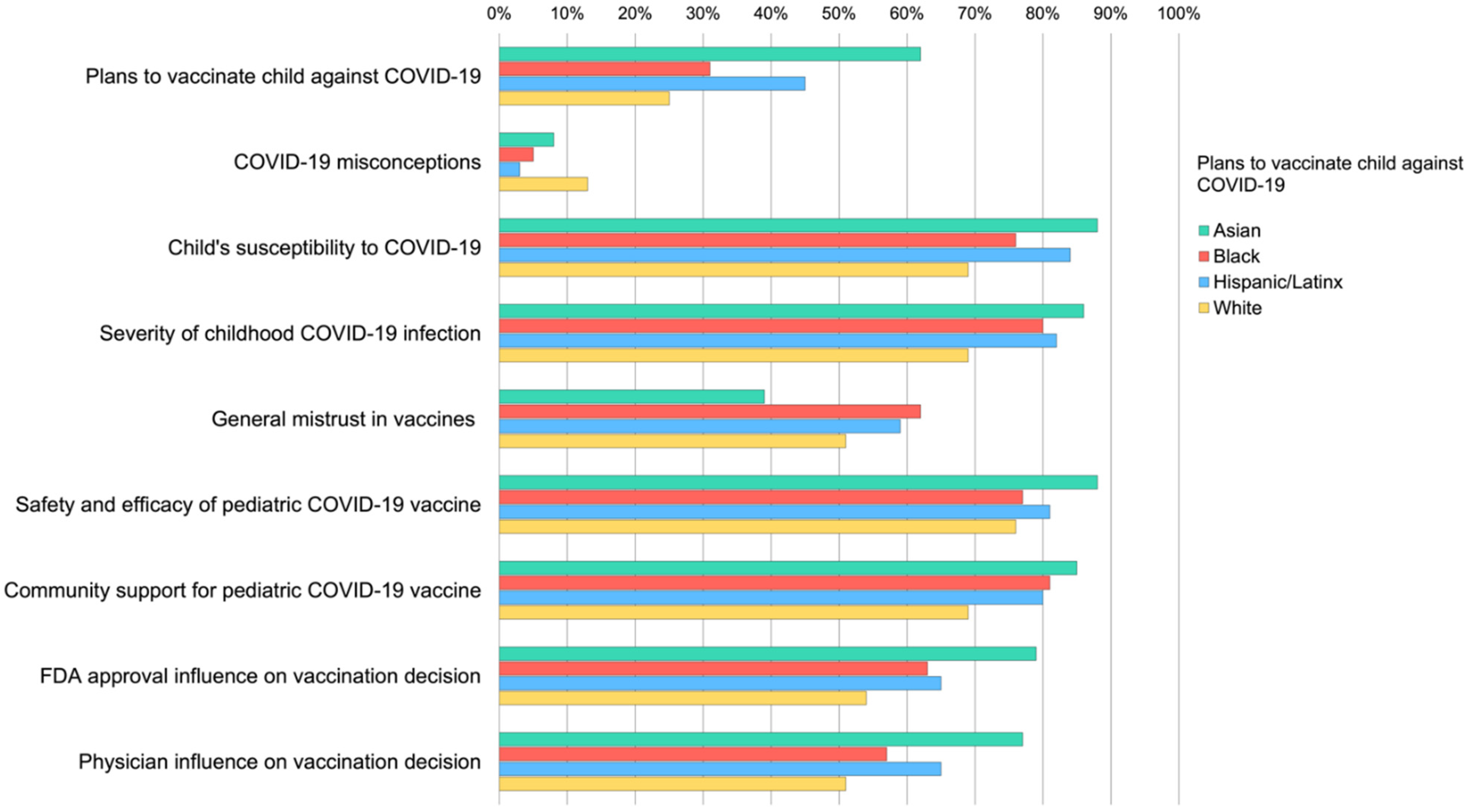
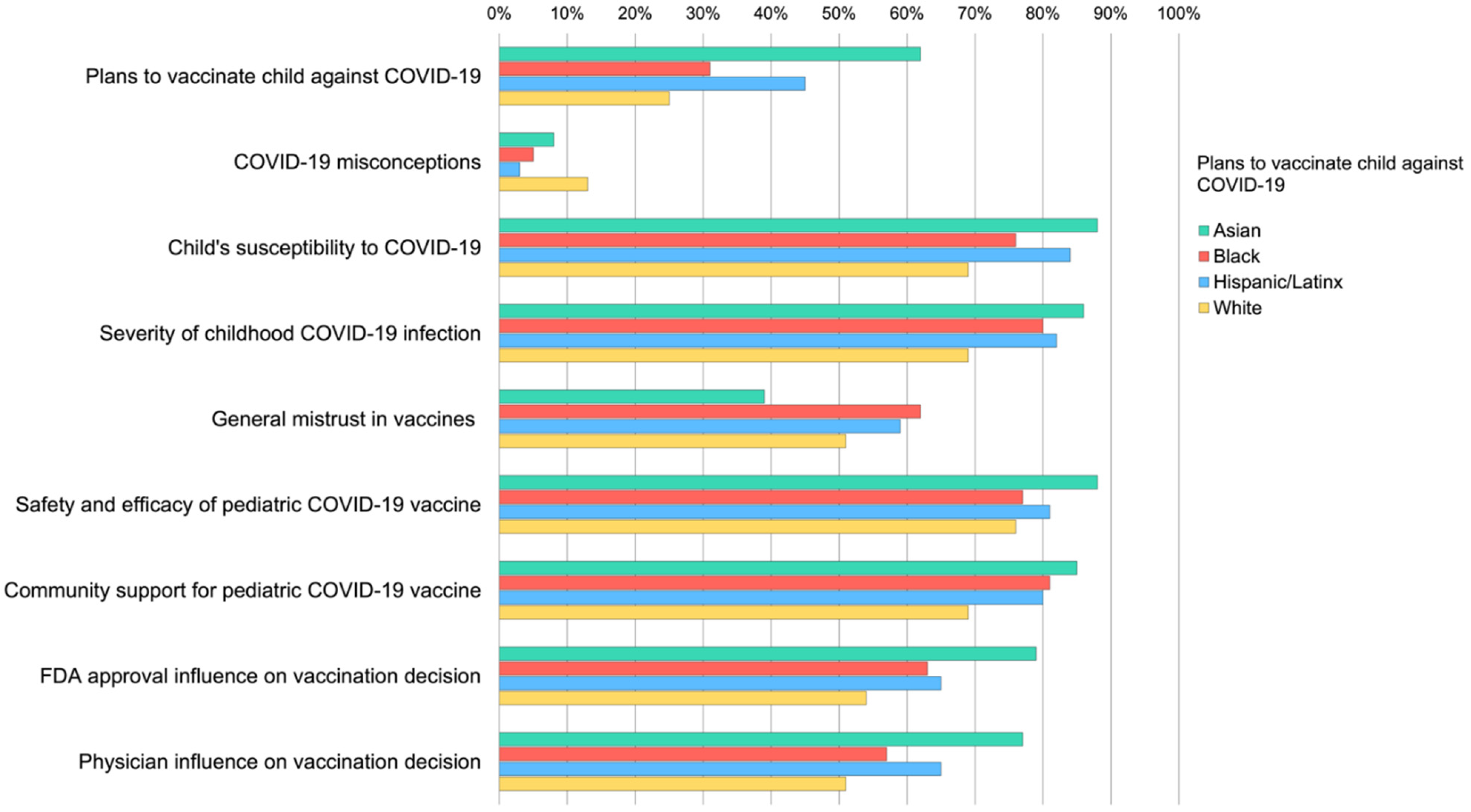
| Plans to vaccinate child against COVID-19 | <0.001 * | |||||
| No or probably not | 138 (34.5%) | 22% | 34% | 32% | 50% | |
| Unsure | 99 (24.8%) | 16% | 35% | 23% | 25% | |
| Yes or probably will | 163 (40.8%) | 62% | 31% | 45% | 25% | |
| COVID-19 misconceptions | 0.04 * | |||||
| M (SD) | 1.47 (1.65) | 1.41 (1.78) | 1.29 (1.48) | 1.40 (1.40) | 1.77 (1.88) | |
| More COVID-19 misconceptions | 29 (7.2%) | 8% | 5% | 3% | 13% | |
| Less COVID-19 misconceptions | 371 (92.8%) | 92% | 95% | 97% | 87% | |
| Child’s susceptibility to COVID-19 | 0.01 * | |||||
| M (SD) | 4.06 (1.33) | 4.37 (1.15) | 4.10 (1.31) | 4.25 (1.31) | 3.51 (1.41) | |
| Greater perceived susceptibility | 317 (79.3%) | 88% | 76% | 84% | 69% | |
| Less perceived susceptibility | 83 (20.8%) | 12% | 24% | 16% | 31% | |
| Severity of childhood COVID-19 infection | 0.02 * | |||||
| M (SD) | 3.87 (1.06) | 4.05 (.93) | 3.86 (1.19) | 4.07 (1.01) | 3.51 (1.01) | |
| Greater perceived severity | 317 (79.3%) | 86% | 80% | 82% | 69% | |
| Less perceived severity | 83 (20.8%) | 14% | 20% | 18% | 31% | |
| General vaccine mistrust | 0.01 * | |||||
| M (SD) | 3.17 (1.24) | 2.81 (1.20) | 3.38 (1.13) | 3.32 (1.34) | 3.18 (1.23) | |
| Greater vaccine mistrust | 211 (52.8%) | 39% | 62% | 59% | 51% | |
| Less vaccine mistrust | 189 (47.3%) | 61% | 38% | 41% | 49% | |
| Safety and efficacy of pediatric COVID-19 vaccine | 0.13 | |||||
| M (SD) | 3.96 (1.19) | 4.27 (1.05) | 3.82 (1.18) | 4.00 (1.25) | 3.76 (1.200) | |
| Greater perceived safety and efficacy | 322 (80.5%) | 88% | 77% | 81% | 76% | |
| Less perceived safety and efficacy | 78 (19.5%) | 12% | 23% | 19% | 24% | |
| Community support for pediatric COVID-19 vaccination | 0.04 * | |||||
| M (SD) | 3.26 (0.94) | 3.50 (0.99) | 3.22 (0.83) | 3.33 (0.96) | 2.99 (0.93) | |
| Greater perceived community support | 315 (78.8%) | 85% | 81% | 80% | 69% | |
| Less perceived community support | 85 (21.3%) | 15% | 19% | 20% | 31% | |
| FDA approval influence on vaccination decision | 0.003 * | |||||
| M (SD) | 3.99 (1.70) | 4.58 (1.49) | 3.89 (1.66) | 3.99 (1.68) | 3.50 (1.79) | |
| Greater influence of FDA approval | 261 (65.3%) | 79% | 63% | 65% | 54% | |
| Less influence of FDA approval | 139 (34.8%) | 21% | 37% | 35% | 46% | |
| Physician influence on vaccination decision | 0.001 * | |||||
| M (SD) | 3.88 (1.69) | 4.42 (1.58) | 3.62 (1.66) | 4.00 (1.65) | 3.46 (1.72) | |
| Greater influence of physician recommendation | 250 (62.5%) | 77% | 57% | 65% | 51% | |
| Less influence of physician recommendation | 150 (37.5%) | 23% | 43% | 35% | 49% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fisher, C.B.; Gray, A.; Sheck, I. COVID-19 Pediatric Vaccine Hesitancy among Racially Diverse Parents in the United States. Vaccines 2022, 10, 31. https://doi.org/10.3390/vaccines10010031
Fisher CB, Gray A, Sheck I. COVID-19 Pediatric Vaccine Hesitancy among Racially Diverse Parents in the United States. Vaccines. 2022; 10(1):31. https://doi.org/10.3390/vaccines10010031
Chicago/Turabian StyleFisher, Celia B., Aaliyah Gray, and Isabelle Sheck. 2022. "COVID-19 Pediatric Vaccine Hesitancy among Racially Diverse Parents in the United States" Vaccines 10, no. 1: 31. https://doi.org/10.3390/vaccines10010031
APA StyleFisher, C. B., Gray, A., & Sheck, I. (2022). COVID-19 Pediatric Vaccine Hesitancy among Racially Diverse Parents in the United States. Vaccines, 10(1), 31. https://doi.org/10.3390/vaccines10010031