Magnesium, Oxidative Stress, Inflammation, and Cardiovascular Disease



Abstract

1. Introduction
2. Mg Deficiency Induces Metabolic Derangements
2.1. Mg Deficiency and Oxidative Stress
2.2. Mg Deficiency and Inflammation
2.3. Mg Deficiency and Insulin Resistance
3. Mg Supplementation as a Therapeutic Treatment for Cardiomyopathy
3.1. Mg Supplementation Improves HF
3.2. Mg Supplementation Shows Protective Effects against Arrhythmias
3.3. Mg Treatment of Other Cardiovascular Diseases
3.4. Gender Differences in Mg Therapy
4. Mg Treatment: Routes, Chemical Formulations, Doses, and Duration
5. Limitations and Controversial Reports of Mg Supplementation
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Liu, M.; Jeong, E.-M.; Liu, H.; Xie, A.; So, E.Y.; Shi, G.; Jeong, G.E.; Zhou, A.; Dudley, S.C., Jr. Magnesium supplementation improves diabetic mitochondrial and cardiac diastolic function. JCI Insight 2019, 4, e123182. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics-2019 update: A report from the American Heart Association. Circulation 2019, 139, E56–E528. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Underlying cause of death. In National Center for Health Statistics: 1999–2018; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. [Google Scholar]
- Douban, S.; Brodsky, M.A.; Whang, D.D.; Whang, R. Significance of magnesium in congestive heart failure. Am. Heart J. 1996, 132, 664–671. [Google Scholar] [CrossRef]
- Milionis, H.J.; Alexandrides, G.E.; Liberopoulos, E.N.; Bairaktari, E.T.; Goudevenos, J.; Elisaf, M.S. Hypomagnesemia and concurrent acid–base and electrolyte abnormalities in patients with congestive heart failure. Eur. J. Heart Fail. 2002, 4, 167–173. [Google Scholar] [CrossRef]
- Tangvoraphonkchai, K.; Davenport, A. Magnesium and cardiovascular disease. Adv. Chronic Kidney Dis. 2018, 25, 251–260. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; Liu, J.; O’Keefe, J.H. Magnesium for the prevention and treatment of cardiovascular disease. Open Heart 2018, 5, e000775. [Google Scholar] [CrossRef] [PubMed]
- Al Alawi, A.M.; Majoni, S.W.; Falhammar, H. Magnesium and human health: Perspectives and research directions. Int. J. Endocrinol. 2018, 2018, 9041694. [Google Scholar] [CrossRef] [PubMed]
- Schwinger, R.H.; Erdmann, E. Heart failure and electrolyte disturbances. Methods Find. Exp. Clin. Pharmacol. 1992, 14, 315–325. [Google Scholar]
- Ceremużyński, L.; Gębalska, J.; Wołk, R.; Makowska, E. Hypomagnesemia in heart failure with ventricular arrhythmias. Beneficial effects of magnesium supplementation. J. Intern. Med. 2000, 247, 78–86. [Google Scholar] [CrossRef]
- Gommers, L.M.; Hoenderop, J.G.; Bindels, R.J.; de Baaij, J.H. Hypomagnesemia in type 2 diabetes: A vicious circle? Diabetes 2016, 65, 3–13. [Google Scholar] [CrossRef]
- Shechter, M. Magnesium and cardiovascular system. Magnes. Res. 2010, 23, 60–72. [Google Scholar]
- Reffelmann, T.; Ittermann, T.; Dörr, M.; Völzke, H.; Reinthaler, M.; Petersmann, A.; Felix, S.B. Low serum magnesium concentrations predict cardiovascular and all-cause mortality. Atherosclerosis 2011, 219, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Severino, P.; Netti, L.; Mariani, M.V.; Maraone, A.; D’Amato, A.; Scarpati, R.; Infusino, F.; Pucci, M.; Lavalle, C.; Maestrini, V.; et al. Prevention of cardiovascular disease: Screening for magnesium deficiency. Cardiol. Res. Pract. 2019, 2019, 4874921. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, H.O.; Nicolson, D.J.; Campbell, F.; Cook, J.V.; Beyer, F.R.; Ford, G.A.; Mason, J. Magnesium supplementation for the management of essential hypertension in adults. Cochrane Database Syst. Rev. 2006. [Google Scholar] [CrossRef]
- Kass, L.; Weekes, J.; Carpenter, L. Effect of magnesium supplementation on blood pressure: A meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 411. [Google Scholar] [CrossRef]
- Altura, B.M.; Kostellow, A.B.; Zhang, A.; Li, W.; Morrill, G.A.; Gupta, R.K.; Altura, B.T. Expression of the nuclear factor-kB and proto-oncogenes c-fos and c-jun are induced by low extracellular Mg2+ in aortic and cerebral vascular smooth muscle cells: Possible links to hypertension, atherogenesis, and stroke. Am. J. Hypertens. 2003, 16, 701–707. [Google Scholar] [CrossRef]
- Zhao, B.; Hu, L.; Dong, Y.; Xu, J.; Wei, Y.; Yu, D.; Xu, J.; Zhang, W. The effect of magnesium intake on stroke incidence: A systematic review and meta-analysis with trial sequential analysis. Front. Neurol. 2019, 10, 852. [Google Scholar] [CrossRef]
- Volpe, S.L. Magnesium in disease prevention and overall health. Adv. Nutr. 2013, 4, 378S–383S. [Google Scholar] [CrossRef]
- De Baaij, J.H.; Hoenderop, J.G.; Bindels, R.J. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef]
- He, K.; Liu, K.; Daviglus, M.L.; Morris, S.J.; Loria, C.M.; Van Horn, L.; Jacobs, D.R., Jr.; Savage, P.J. Magnesium intake and incidence of metabolic syndrome among young adults. Circulation 2006, 113, 1675–1682. [Google Scholar] [CrossRef]
- Belin, R.J.; He, K. Magnesium physiology and pathogenic mechanisms that contribute to the development of the metabolic syndrome. Magnes. Res. 2007, 20, 107–129. [Google Scholar] [PubMed]
- Sjögren, A.; Florén, C.H.; Nilsson, A. Oral administration of magnesium hydroxide to subjects with insulin-dependent diabetes mellitus: Effects on magnesium and potassium levels and on insulin requirements. Magnesium 1988, 7, 117–122. [Google Scholar] [PubMed]
- Djurhuus, M.S.; Klitgaard, N.A.; Pedersen, K.K.; Blaabjerg, O.; Altura, B.M.; Altura, B.T.; Henriksen, J.E. Magnesium reduces insulin-stimulated glucose uptake and serum lipid concentrations in type 1 diabetes. Metabolism 2001, 50, 1409–1417. [Google Scholar] [CrossRef]
- Song, Y.; Manson, J.E.; Buring, J.E.; Liu, S. Dietary magnesium intake in relation to plasma insulin levels and risk of type 2 diabetes in women. Diabetes Care 2004, 27, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Martins, I.J. Magnesium deficiency and induction of NAFLD and type 3 diabetes in Australasia. Australas. Med. J. 2017, 10, 235–237. [Google Scholar] [CrossRef]
- Ascherio, A.; Rimm, E.B.; Giovannucci, E.L.; Colditz, G.A.; Rosner, B.; Willett, W.C.; Sacks, F.; Stampfer, M.J. A prospective study of nutritional factors and hypertension among US men. Circulation 1992, 86, 1475–1484. [Google Scholar] [CrossRef]
- Ascherio, A.; Hennekens, C.; Willett, W.C.; Sacks, F.; Rosner, B.; Manson, J.; Witteman, J.; Stampfer, M.J. Prospective study of nutritional factors, blood pressure, and hypertension among US women. Hypertension 1996, 27, 1065–1072. [Google Scholar] [CrossRef]
- Haigney, M.C.; Wei, S.; Kääb, S.; Griffiths, E.; Berger, R.; Tunin, R.; Kass, D.; Fisher, W.G.; Silver, B.; Silverman, H. Loss of cardiac magnesium in experimental heart failure prolongs and destabilizes repolarization in dogs. J. Am. Coll. Cardiol. 1998, 31, 701–706. [Google Scholar] [CrossRef]
- Schimatschek, H.F.; Rempis, R. Prevalence of hypomagnesemia in an unselected German population of 16,000 individuals. Magnes. Res. 2001, 14, 283–290. [Google Scholar]
- Guo, W.; Nazim, H.; Liang, Z.; Yang, D. Magnesium deficiency in plants: An urgent problem. Crop J. 2016, 4, 83–91. [Google Scholar] [CrossRef]
- Olza, J.; Aranceta-Bartrina, J.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, A. Reported dietary intake, disparity between the reported consumption and the level needed for adequacy and food sources of calcium, phosphorus, magnesium and vitamin D in the Spanish population: Findings from the ANIBES Study. Nutrients 2017, 9, 168. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.; Goldman, J.; Ahuja, J.; Rhodes, D.; Lacomb, R. What We Eat in America, NHANES 2005–2006, Usual Nutrient Intakes from Food and Water Compared to 1997 Dietary Reference Intakes for Vitamin D, Calcium, Phosphorus, and Magnesium. Available online: https://www.ars.usda.gov/research/publications/publication/?seqNo115=243279 (accessed on 30 July 2020).
- Costello, R.B.; Elin, R.J.; Rosanoff, A.; Wallace, T.C.; Guerrero-Romero, F.; Hruby, A.; Lutsey, P.L.; Nielsen, F.H.; Rodriguez-Moran, M.; Song, Y.; et al. Perspective: The case for an evidence-based reference interval for serum magnesium: The time has come. Adv. Nutr. 2016, 7, 977–993. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.H. Magnesium deficiency and increased inflammation: Current perspectives. J. Inflamm. Res. 2018, 11, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Mokdad, A.H. Dietary magnesium intake in a national sample of US adults. J. Nutr. 2003, 133, 2879–2882. [Google Scholar] [CrossRef] [PubMed]
- Corica, F.; Corsonello, A.; Ientile, R.; Cucinotta, D.; Di Benedetto, A.; Perticone, F.; Dominguez, L.J.; Barbagallo, M. Serum ionized magnesium levels in relation to metabolic syndrome in type 2 diabetic patients. J. Am. Coll. Nutr. 2006, 25, 210–215. [Google Scholar] [CrossRef]
- Taveira, T.H.; Ouellette, D.; Gulum, A.; Choudhary, G.; Eaton, C.B.; Liu, S.; Wu, W.C. Relation of magnesium intake with cardiac function and heart failure hospitalizations in black adults: The Jackson Heart Study. Circ. Heart Fail. 2016, 9, e002698. [Google Scholar] [CrossRef]
- Gottlieb, S.S. Importance of magnesium in congestive heart failure. Am. J. Cardiol. 1989, 63, 39g–42g. [Google Scholar] [CrossRef]
- Chrysant, S.G.; Chrysant, G.S. Association of hypomagnesemia with cardiovascular diseases and hypertension. Int. J. Cardiol. Hypertens. 2019, 1, 100005. [Google Scholar] [CrossRef]
- Perticone, F.; Adinolfi, L.; Bonaduce, D. Efficacy of magnesium sulfate in the treatment of torsade de pointes. Am. Heart J. 1986, 112, 847–849. [Google Scholar] [CrossRef]
- Gupta, A.; Lawrence, A.T.; Krishnan, K.; Kavinsky, C.J.; Trohman, R.G. Current concepts in the mechanisms and management of drug-induced QT prolongation and torsade de pointes. Am. Heart J. 2007, 153, 891–899. [Google Scholar] [CrossRef]
- Fernando, H.C.; Jaklitsch, M.T.; Walsh, G.L.; Tisdale, J.E.; Bridges, C.D.; Mitchell, J.D.; Shrager, J.B. The Society of Thoracic surgeons practice guideline on the prophylaxis and management of atrial fibrillation associated with general thoracic surgery: Executive summary. Ann. Thorac. Surg. 2011, 92, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Frendl, G.; Sodickson, A.C.; Chung, M.K.; Waldo, A.L.; Gersh, B.J.; Tisdale, J.E.; Calkins, H.; Aranki, S.; Kaneko, T.; Cassivi, S.; et al. 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. J. Thorac. Cardiovasc. Surg. 2014, 148, e153–e193. [Google Scholar] [CrossRef]
- Markovits, N.; Kurnik, D.; Halkin, H.; Margalit, R.; Bialik, M.; Lomnicky, Y.; Loebstein, R. Database evaluation of the association between serum magnesium levels and the risk of atrial fibrillation in the community. Int. J. Cardiol. 2016, 205, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Zehender, M.; Meinertz, T.; Faber, T.; Caspary, A.; Jeron, A.; Bremm, K.; Just, H. Antiarrhythmic effects of increasing the daily intake of magnesium and potassium in patients with frequent ventricular arrhythmias. Magnesium in Cardiac Arrhythmias (MAGICA) Investigators. J. Am. Coll. Cardiol. 1997, 29, 1028–1034. [Google Scholar] [CrossRef]
- Lutsey, P.; Chen, L.; Eaton, A.; Jaeb, M.; Rudser, K.; Neaton, J.; Alonso, A. A pilot randomized trial of oral magnesium supplementation on supraventricular arrhythmias. Nutrients 2018, 10, 884. [Google Scholar] [CrossRef]
- Horner, S.M. Efficacy of intravenous magnesium in acute myocardial infarction in reducing arrhythmias and mortality. Meta-analysis of magnesium in acute myocardial infarction. Circulation 1992, 86, 774–779. [Google Scholar] [CrossRef]
- Ferrari, R.; Albertini, A.; Curello, S.; Ceconi, C.; Di Lisa, F.; Raddino, R.; Visioli, O. Myocardial recovery during post-ischaemic reperfusion: Effects of nifedipine, calcium and magnesium. J. Mol. Cell. Cardiol. 1986, 18, 487–498. [Google Scholar] [CrossRef]
- Gout, E.; Rébeillé, F.; Douce, R.; Bligny, R. Interplay of Mg2+, ADP, and ATP in the cytosol and mitochondria: Unravelling the role of Mg2+ in cell respiration. Proc. Natl. Acad. Sci. USA 2014, 111, E4560–E4567. [Google Scholar] [CrossRef]
- Yamanaka, R.; Tabata, S.; Shindo, Y.; Hotta, K.; Suzuki, K.; Soga, T.; Oka, K. Mitochondrial Mg2+ homeostasis decides cellular energy metabolism and vulnerability to stress. Sci. Rep. 2016, 6, 30027. [Google Scholar] [CrossRef]
- Sreedhara, A.; Cowan, J.A. Structural and catalytic roles for divalent magnesium in nucleic acid biochemistry. BioMetals 2002, 15, 211–223. [Google Scholar] [CrossRef]
- Sharikabad, M.N.; Østbye, K.M.; Brørs, O. Increased [Mg2+] reduces Ca2+ influx and disruption of mitochondrial membrane potential during reoxygenation. Am. J. Physiol. Heart Circ. Physiol. 2001, 281, H2113–H2123. [Google Scholar] [CrossRef] [PubMed]
- Racay, P. Effect of magnesium on calcium-induced depolarisation of mitochondrial transmembrane potential. Cell Biol. Int. 2008, 32, 136–145. [Google Scholar] [CrossRef]
- Buda, S.; Stompor, T.; Sulowicz, W.; Kopec, J.; Szymczakiewicz-Multanowska, A.; Janion, M. The impact of changes in levels of calcium, phosphate and magnesium during hemodialysis on autonomic system reactivity as measured by heart rate variability analysis. Przegl. Lek. 2000, 57, 340–345. [Google Scholar]
- Mubagwa, K.; Gwanyanya, A.; Zakharov, S.; Macianskiene, R. Regulation of cation channels in cardiac and smooth muscle cells by intracellular magnesium. Arch. Biochem. Biophys. 2007, 458, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Almoznino-Sarafian, D.; Sarafian, G.; Berman, S.; Shteinshnaider, M.; Tzur, I.; Cohen, N.; Gorelik, O. Magnesium administration may improve heart rate variability in patients with heart failure. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Feng, R.; Shao, D.; Liu, S.; Lei, M.; Wang, H.; Sun, X.; Guo, F.; Hu, H.; Kameyama, M.; et al. Mg2+-dependent facilitation and inactivation of L-type Ca2+ channels in guinea pig ventricular myocytes. J. Pharmacol. Sci. 2015, 129, 143–149. [Google Scholar] [CrossRef]
- Finley, N.; Dvoretsky, A.; Rosevear, P.R. Magnesium-calcium exchange in cardiac troponin C bound to cardiac troponin I. J. Mol. Cell. Cardiol. 2000, 32, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.R.; Masino, L.; Bayley, P.M. Enhancement by Mg2+ of domain specificity in Ca2+-dependent interactions of calmodulin with target sequences. Protein Sci. 2000, 9, 2477–2488. [Google Scholar] [CrossRef]
- Carvil, P.; Cronin, J. Magnesium and implications on muscle function. Strenth Cond. J. 2010, 32, 48–54. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Del Gobbo, L.C.; Rosanoff, A.; Wang, J.; Zhang, W.; Song, Y. Effects of magnesium supplementation on blood pressure: A meta-analysis of randomized double-blind placebo-controlled trials. Hypertension 2016, 68, 324–333. [Google Scholar] [CrossRef]
- Romani, A.M.; Matthews, V.D.; Scarpa, A. Parallel stimulation of glucose and Mg2+ accumulation by insulin in rat hearts and cardiac ventricular myocytes. Circ. Res. 2000, 86, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Wang, H.; Jing, Z.; Wang, Y.; Cheng, Y.; Wang, W.; Sun, W. Role of magnesium in type 2 diabetes mellitus. Biol. Trace Elem. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Tucker, K.L.; Hannan, M.T.; Chen, H.; Cupples, L.A.; Wilson, P.W.; Kiel, D.P. Potassium, magnesium, and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women. Am. J. Clin. Nutr. 1999, 69, 727–736. [Google Scholar] [CrossRef]
- Rude, R.K.; Gruber, H.E.; Wei, L.Y.; Frausto, A.; Mills, B.G. Magnesium deficiency: Effect on bone and mineral metabolism in the mouse. Calcif. Tissue Int. 2003, 72, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Erem, S.; Atfi, A.; Razzaque, M.S. Anabolic effects of vitamin D and magnesium in aging bone. J. Steroid Biochem. Mol. Biol. 2019, 193, 105400. [Google Scholar] [CrossRef]
- Soar, J.; Perkins, G.D.; Abbas, G.; Alfonzo, A.; Barelli, A.; Bierens, J.J.; Brugger, H.; Deakin, C.D.; Dunning, J.; Georgiou, M.; et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution. Resuscitation 2010, 81, 1400–1433. [Google Scholar] [CrossRef]
- Pham, P.C.; Pham, P.A.; Pham, S.V.; Pham, P.T.; Pham, P.M.; Pham, P.T. Hypomagnesemia: A clinical perspective. Int. J. Nephrol. Renovasc. Dis. 2014, 7, 219–230. [Google Scholar] [CrossRef]
- Watanabe, M.; Konishi, M. Intracellular calibration of the fluorescent Mg2+ indicator furaptra in rat ventricular myocytes. Pflugers Arch. 2001, 442, 35–40. [Google Scholar] [CrossRef]
- Tashiro, M.; Inoue, H.; Konishi, M. Magnesium homeostasis in cardiac myocytes of Mg-deficient rats. PLoS ONE 2013, 8, e73171. [Google Scholar] [CrossRef]
- Touyz, R.M. Transient receptor potential melastatin 6 and 7 channels, magnesium transport, and vascular biology: Implications in hypertension. Am. J. Physiol. Heart Circ. Physiol. 2008, 294, H1103–H1118. [Google Scholar] [CrossRef]
- Tashiro, M.; Inoue, H.; Konishi, M. Physiological pathway of magnesium influx in rat ventricular myocytes. Biophys. J. 2014, 107, 2049–2058. [Google Scholar] [CrossRef] [PubMed]
- Arjona, F.J.; Chen, Y.X.; Flik, G.; Bindels, R.J.; Hoenderop, J.G. Tissue-specific expression and in vivo regulation of zebrafish orthologues of mammalian genes related to symptomatic hypomagnesemia. Pflug. Arch. 2013, 465, 1409–1421. [Google Scholar] [CrossRef] [PubMed]
- Kolisek, M.; Zsurka, G.; Samaj, J.; Weghuber, J.; Schweyen, R.J.; Schweigel, M. Mrs2p is an essential component of the major electrophoretic Mg2+ influx system in mitochondria. EMBO J. 2003, 22, 1235–1244. [Google Scholar] [CrossRef] [PubMed]
- Mastrototaro, L.; Smorodchenko, A.; Aschenbach, J.R.; Kolisek, M.; Sponder, G. Solute carrier 41A3 encodes for a mitochondrial Mg2+ efflux system. Sci. Rep. 2016, 6, 27999. [Google Scholar] [CrossRef]
- Pilchova, I.; Klacanova, K.; Tatarkova, Z.; Kaplan, P.; Racay, P. The involvement of Mg2+ in regulation of cellular and mitochondrial functions. Oxid. Med. Cell. Longev. 2017, 2017, 6797460. [Google Scholar] [CrossRef] [PubMed]
- Romani, A.M.P. Cellular magnesium homeostasis. Arch. Biochem. Biophys. 2011, 512, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Goytain, A.; Quamme, G.A. Functional characterization of human SLC41A1, a Mg2+ transporter with similarity to prokaryotic MgtE Mg2+ transporters. Physiol. Genom. 2005, 21, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Clapham, D.E. Mammalian MagT1 and TUSC3 are required for cellular magnesium uptake and vertebrate embryonic development. Proc. Natl. Acad. Sci. USA 2009, 106, 15750–15755. [Google Scholar] [CrossRef]
- Shahi, A.; Aslani, S.; Ataollahi, M.; Mahmoudi, M. The role of magnesium in different inflammatory diseases. Inflammopharmacology 2019, 27, 649–661. [Google Scholar] [CrossRef]
- Liu, M.; Liu, H.; Xie, A.; Kang, G.J.; Feng, F.; Zhou, X.; Zhao, Y.; Dudley, S.C., Jr. Magnesium deficiency causes reversible diastolic and systolic cardiomyopathy. Biophys. J. 2020, 118, 245a. [Google Scholar] [CrossRef]
- He, Y.; Yao, G.; Savoia, C.; Touyz, R.M. Transient receptor potential melastatin 7 ion channels regulate magnesium homeostasis in vascular smooth muscle cells: Role of angiotensin II. Circ. Res. 2005, 96, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Sontia, B.; Montezano Augusto, C.I.; Paravicini, T.; Tabet, F.; Touyz Rhian, M. Downregulation of renal TRPM7 and increased inflammation and fibrosis in aldosterone-infused mice. Hypertension 2008, 51, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Yogi, A.; Callera, G.E.; O’Connor, S.; Antunes, T.T.; Valinsky, W.; Miquel, P.; Montezano, A.C.I.; Perraud, A.-L.; Schmitz, C.; Shrier, A.; et al. Aldosterone signaling through transient receptor potential melastatin 7 cation channel (TRPM7) and its α-kinase domain. Cell. Signal. 2013, 25, 2163–2175. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Weglicki, W.; Quamme, G.; Tucker, K.; Haigney, M.; Resnick, L. Potassium, magnesium, and electrolyte imbalance and complications in disease management. Clin. Exp. Hypertens. 2005, 27, 95–112. [Google Scholar] [CrossRef]
- Liamis, G.; Rodenburg, E.M.; Hofman, A.; Zietse, R.; Stricker, B.H.; Hoorn, E.J. Electrolyte disorders in community subjects: Prevalence and risk factors. Am. J. Med. 2013, 126, 256–263. [Google Scholar] [CrossRef]
- Tham, Y.K.; Bernardo, B.C.; Ooi, J.Y.Y.; Weeks, K.L.; McMullen, J.R. Pathophysiology of cardiac hypertrophy and heart failure: Signaling pathways and novel therapeutic targets. Arch. Toxicol. 2015, 89, 1401–1438. [Google Scholar] [CrossRef]
- Panov, A.; Scarpa, A. Mg2+ control of respiration in isolated rat liver mitochondria. Biochemistry 1996, 35, 12849–12856. [Google Scholar] [CrossRef]
- Rodríguez-Zavala, J.S.; Moreno-Sánchez, R. Modulation of oxidative phosphorylation by Mg2+ in rat heart mitochondria. J. Biol. Chem. 1998, 273, 7850–7855. [Google Scholar] [CrossRef]
- Salaminia, S.; Sayehmiri, F.; Angha, P.; Sayehmiri, K.; Motedayen, M. Evaluating the effect of magnesium supplementation and cardiac arrhythmias after acute coronary syndrome: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2018, 18, 129. [Google Scholar] [CrossRef]
- Rayssiguier, Y.; Libako, P.; Nowacki, W.; Rock, E. Magnesium deficiency and metabolic syndrome: Stress and inflammation may reflect calcium activation. Magnes. Res. 2010, 23, 73–80. [Google Scholar] [CrossRef]
- Rayssiguier, Y.; Gueux, E.; Nowacki, W.; Rock, E.; Mazur, A. High fructose consumption combined with low dietary magnesium intake may increase the incidence of the metabolic syndrome by inducing inflammation. Magnes. Res. 2006, 19, 237–243. [Google Scholar] [PubMed]
- Bo, S.; Durazzo, M.; Guidi, S.; Carello, M.; Sacerdote, C.; Silli, B.; Rosato, R.; Cassader, M.; Gentile, L.; Pagano, G. Dietary magnesium and fiber intakes and inflammatory and metabolic indicators in middle-aged subjects from a population-based cohort. Am. J. Clin. Nutr. 2006, 84, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Tejero-Taldo, M.I.; Chmielinska, J.J.; Gonzalez, G.; Mak, I.T.; Weglicki, W.B. N-methyl-D-aspartate receptor blockade inhibits cardiac inflammation in the Mg2+-deficient rat. J. Pharmacol. Exp. Ther. 2004, 311, 8–13. [Google Scholar] [CrossRef]
- Hans, C.P.; Chaudhary, D.P.; Bansal, D.D. Magnesium deficiency increases oxidative stress in rats. Indian J. Exp. Biol. 2002, 40, 1275–1279. [Google Scholar]
- Guerrero-Romero, F.; Tamez-Perez, H.E.; González-González, G.; Salinas-Martínez, A.M.; Montes-Villarreal, J.; Treviño-Ortiz, J.H.; Rodríguez-Morán, M. Oral magnesium supplementation improves insulin sensitivity in non-diabetic subjects with insulin resistance. A double-blind placebo-controlled randomized trial. Diabetes Metab. 2004, 30, 253–258. [Google Scholar] [CrossRef]
- Liu, M.; Gu, L.; Sulkin, M.S.; Liu, H.; Jeong, E.M.; Greener, I.; Xie, A.; Efimov, I.R.; Dudley, S.C., Jr. Mitochondrial dysfunction causing cardiac sodium channel downregulation in cardiomyopathy. J. Mol. Cell. Cardiol. 2013, 54, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Dey, S.; DeMazumder, D.; Sidor, A.; Foster, D.B.; O’Rourke, B. Mitochondrial ROS drive sudden cardiac death and chronic proteome remodeling in heart failure. Circ. Res. 2018, 123, 356–371. [Google Scholar] [CrossRef]
- García, N.; Zazueta, C.; Aguilera-Aguirre, L. Oxidative stress and inflammation in cardiovascular disease. Oxid. Med. Cell. Longev. 2017, 2017, 5853238. [Google Scholar] [CrossRef] [PubMed]
- Pignatelli, P.; Menichelli, D.; Pastori, D.; Violi, F. Oxidative stress and cardiovascular disease: New insights. Kardiol. Pol. 2018, 76, 713–722. [Google Scholar] [CrossRef]
- Hashimoto, T.; Nishi, K.; Nagasao, J.; Tsuji, S.; Oyanagi, K. Magnesium exerts both preventive and ameliorating effects in an in vitro rat Parkinson disease model involving 1-methyl-4-phenylpyridinium (MPP+) toxicity in dopaminergic neurons. Brain Res. 2008, 1197, 143–151. [Google Scholar] [CrossRef]
- Das, U.N. Nutritional factors in the prevention and management of coronary artery disease and heart failure. Nutrition 2015, 31, 283–291. [Google Scholar] [CrossRef]
- Zheltova, A.A.; Kharitonova, M.V.; Iezhitsa, I.N.; Spasov, A.A. Magnesium deficiency and oxidative stress: An update. Biomedicine (Taipei) 2016, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.B.S.; Severo, J.S.; Santos, L.R.d.; de Sousa Melo, S.R.; de Oliveira Santos, R.; de Oliveira, A.R.S.; Cruz, K.J.C.; do Nascimento Marreiro, D. Role of magnesium in oxidative stress in individuals with obesity. Biol. Trace Elem. Res. 2017, 176, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Celik, N.; Andiran, N.; Yilmaz, A.E. The relationship between serum magnesium levels with childhood obesity and insulin resistance: A review of the literature. J. Pediatr. Endocrinol. Metab. 2011, 24, 675–678. [Google Scholar] [PubMed]
- Codoner-Franch, P.; Boix-Garcia, L.; Simo-Jorda, R.; Del Castillo-Villaescusa, C.; Maset-Maldonado, J.; Valls-Belles, V. Is obesity associated with oxidative stress in children? Int. J. Pediatr. Obes. 2010, 5, 56–63. [Google Scholar] [CrossRef]
- Kubota, T.; Shindo, Y.; Tokuno, K.; Komatsu, H.; Ogawa, H.; Kudo, S.; Kitamura, Y.; Suzuki, K.; Oka, K. Mitochondria are intracellular magnesium stores: Investigation by simultaneous fluorescent imagings in PC12 cells. Biochim. Biophys. Acta 2005, 1744, 19–28. [Google Scholar] [CrossRef]
- Jeong, E.M.; Chung, J.; Liu, H.; Go, Y.; Gladstein, S.; Farzaneh-Far, A.; Lewandowski, E.D.; Dudley, S.C. Role of mitochondrial oxidative stress in glucose tolerance, insulin resistance, and cardiac diastolic dysfunction. J. Am. Heart Assoc. 2016, 5, e003046. [Google Scholar] [CrossRef]
- Kramer, J.H.; Mišík, V.; Weglicki, W.B. Magnesium-deficiency potentiates free radical production associated with postischemic injury to rat hearts: Vitamin E affords protection. Free Radical. Biol. Med. 1994, 16, 713–723. [Google Scholar] [CrossRef]
- Shah, N.C.; Liu, J.-P.; Iqbal, J.; Hussain, M.; Jiang, X.-C.; Li, Z.; Li, Y.; Zheng, T.; Li, W.; Sica, A.C.; et al. Mg deficiency results in modulation of serum lipids, glutathione, and NO synthase isozyme activation in cardiovascular tissues: Relevance to de novo synthesis of ceramide, serum Mg and atherogenesis. Int. J. Clin. Exp. Med. 2011, 4, 103–118. [Google Scholar]
- Kumar, B.P.; Shivakumar, K. Depressed antioxidant defense in rat heart in experimental magnesium deficiency. Implications for the pathogenesis of myocardial lesions. Biol. Trace Elem. Res. 1997, 60, 139–144. [Google Scholar] [CrossRef]
- Canet-Avilés, R.M.; Wilson, M.A.; Miller, D.W.; Ahmad, R.; McLendon, C.; Bandyopadhyay, S.; Baptista, M.J.; Ringe, D.; Petsko, G.A.; Cookson, M.R. The Parkinson’s disease protein DJ-1 is neuroprotective due to cysteine-sulfinic acid-driven mitochondrial localization. Proc. Natl. Acad. Sci. USA 2004, 101, 9103–9108. [Google Scholar] [CrossRef] [PubMed]
- Björkblom, B.; Maple-Grødem, J.; Puno, M.R.; Odell, M.; Larsen, J.P.; Møller, S.G. Reactive oxygen species-mediated DJ-1 monomerization modulates intracellular trafficking involving karyopherin β2. Mol. Cell. Biol. 2014, 34, 3024–3040. [Google Scholar] [CrossRef]
- Blomeyer, C.A.; Bazil, J.N.; Stowe, D.F.; Dash, R.K.; Camara, A.K.S. Mg2+ differentially regulates two modes of mitochondrial Ca2+ uptake in isolated cardiac mitochondria: Implications for mitochondrial Ca2+ sequestration. J. Bioenerg. Biomembr. 2016, 48, 175–188. [Google Scholar] [CrossRef]
- Sponder, G.; Abdulhanan, N.; Frohlich, N.; Mastrototaro, L.; Aschenbach, J.R.; Rontgen, M.; Pilchova, I.; Cibulka, M.; Racay, P.; Kolisek, M. Overexpression of Na+/Mg2+ exchanger SLC41A1 attenuates pro-survival signaling. Oncotarget 2018, 9, 5084–5104. [Google Scholar] [CrossRef] [PubMed]
- Salvi, M.; Bozac, A.; Toninello, A. Gliotoxin induces Mg2+ efflux from intact brain mitochondria. Neurochem. Int. 2004, 45, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wei, X.; Yan, P.; Han, Y.; Sun, S.; Wu, K.; Fan, D. Human mitochondrial Mrs2 protein promotes multidrug resistance in gastric cancer cells by regulating p27, cyclin D1 expression and cytochrome C release. Cancer Biol. Ther. 2009, 8, 607–614. [Google Scholar] [CrossRef]
- Bednarczyk, P.; Dolowy, K.; Szewczyk, A. Matrix Mg2+ regulates mitochondrial ATP-dependent potassium channel from heart. FEBS Lett. 2005, 579, 1625–1632. [Google Scholar] [CrossRef] [PubMed]
- Beavis, A.D.; Powers, M.F. On the regulation of the mitochondrial inner membrane anion channel by magnesium and protons. J. Biol. Chem. 1989, 264, 17148–17155. [Google Scholar]
- Zoratti, M.; Szabò, I. The mitochondrial permeability transition. Biochim. Biophys. Acta 1995, 1241, 139–176. [Google Scholar] [CrossRef]
- Seo, Y.W.; Shin, J.N.; Ko, K.H.; Cha, J.H.; Park, J.Y.; Lee, B.R.; Yun, C.W.; Kim, Y.M.; Seol, D.W.; Kim, D.W.; et al. The molecular mechanism of Noxa-induced mitochondrial dysfunction in p53-mediated cell death. J. Biol. Chem. 2003, 278, 48292–48299. [Google Scholar] [CrossRef]
- Gorgoglione, V.; Laraspata, D.; Piana, G.L.; Marzulli, D.; Lofrumento, N.E. Protective effect of magnesium and potassium ions on the permeability of the external mitochondrial membrane. Arch. Biochem. Biophys. 2007, 461, 13–23. [Google Scholar] [CrossRef] [PubMed]
- La Piana, G.; Gorgoglione, V.; Laraspata, D.; Marzulli, D.; Lofrumento, N.E. Effect of magnesium ions on the activity of the cytosolic NADH/cytochrome C electron transport system. FEBS J. 2008, 275, 6168–6179. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-Y.; Hsieh, Y.-L.; Ju, D.-T.; Lin, C.-C.; Kuo, C.-H.; Liou, Y.-F.; Ho, T.-J.; Tsai, C.-H.; Tsai, F.-J.; Lin, J.-Y. Attenuation of magnesium sulfate on CoCl2-induced cell death by activating ERK1/2/MAPK and inhibiting HIF-1a via mitochondrial apoptotic signaling suppression in a neuronal cell line. Chin. J. Physiol. 2015, 58, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Boelens, A.D.; Pradhan, R.K.; Blomeyer, C.A.; Camara, A.K.S.; Dash, R.K.; Stowe, D.F. Extra-matrix Mg2+ limits Ca2+ uptake and modulates Ca2+ uptake–independent respiration and redox state in cardiac isolated mitochondria. J. Bioenerg. Biomembr. 2013, 45, 203–218. [Google Scholar] [CrossRef][Green Version]
- Li, Y.; Wang, J.; Yue, J.; Wang, Y.; Yang, C.; Cui, Q. High magnesium prevents matrix vesicle-mediated mineralization in human bone marrow-derived mesenchymal stem cells via mitochondrial pathway and autophagy. Cell Biol. Int. 2018, 42, 205–215. [Google Scholar] [CrossRef]
- Piskacek, M.; Zotova, L.; Zsurka, G.; Schweyen, R.J. Conditional knockdown of hMRS2 results in loss of mitochondrial Mg(2+) uptake and cell death. J. Cell. Mol. Med. 2009, 13, 693–700. [Google Scholar] [CrossRef]
- Merolle, L.; Sponder, G.; Sargenti, A.; Mastrototaro, L.; Cappadone, C.; Farruggia, G.; Procopio, A.; Malucelli, E.; Parisse, P.; Gianoncelli, A.; et al. Overexpression of the mitochondrial Mg channel MRS2 increases total cellular Mg concentration and influences sensitivity to apoptosis. Metallomics 2018, 10, 917–928. [Google Scholar] [CrossRef]
- De Baaij, J.H.; Arjona, F.J.; van den Brand, M.; Lavrijsen, M.; Lameris, A.L.; Bindels, R.J.; Hoenderop, J.G. Identification of SLC41A3 as a novel player in magnesium homeostasis. Sci. Rep. 2016, 6, 28565. [Google Scholar] [CrossRef]
- Goytain, A.; Quamme, G.A. Identification and characterization of a novel mammalian Mg2+ transporter with channel-like properties. BMC Genom. 2005, 6, 48. [Google Scholar] [CrossRef]
- Pearson, P.J.; Evora, P.R.; Seccombe, J.F.; Schaff, H.V. Hypomagnesemia inhibits nitric oxide release from coronary endothelium: Protective role of magnesium infusion after cardiac operations. Ann. Thorac. Surg. 1998, 65, 967–972. [Google Scholar] [CrossRef]
- Tamura, M.; Kanno, M.; Kai, T. Destabilization of neutrophil NADPH oxidase by ATP and other trinucleotides and its prevention by Mg2+. Biochim. Biophys. Acta 2001, 1510, 270–277. [Google Scholar] [CrossRef]
- Weglicki, W.B.; Phillips, T.M.; Freedman, A.M.; Cassidy, M.M.; Dickens, B.F. Magnesium-deficiency elevates circulating levels of inflammatory cytokines and endothelin. Mol. Cell. Biochem. 1992, 110, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Bussiere, F.I.; Gueux, E.; Rock, E.; Mazur, A.; Rayssiguier, Y. Protective effect of calcium deficiency on the inflammatory response in magnesium-deficient rats. Eur. J. Nutr. 2002, 41, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Maier, J.A.M.; Malpuech-Brugère, C.; Zimowska, W.; Rayssiguier, Y.; Mazur, A. Low magnesium promotes endothelial cell dysfunction: Implications for atherosclerosis, inflammation and thrombosis. Biochim. Biophys. Acta 2004, 1689, 13–21. [Google Scholar] [CrossRef]
- Song, Y.; Li, T.Y.; van Dam, R.M.; Manson, J.E.; Hu, F.B. Magnesium intake and plasma concentrations of markers of systemic inflammation and endothelial dysfunction in women. Am. J. Clin. Nutr. 2007, 85, 1068–1074. [Google Scholar] [CrossRef]
- Tejero-Taldo, M.I.; Kramer, J.H.; Mak Iu, T.; Komarov, A.M.; Weglicki, W.B. The nerve-heart connection in the pro-oxidant response to Mg-deficiency. Heart Fail. Rev. 2006, 11, 35–44. [Google Scholar] [CrossRef]
- Nielsen, F.H. Magnesium, inflammation, and obesity in chronic disease. Nutr. Rev. 2010, 68, 333–340. [Google Scholar] [CrossRef]
- Almoznino-Sarafian, D.; Berman, S.; Mor, A.; Shteinshnaider, M.; Gorelik, O.; Tzur, I.; Alon, I.; Modai, D.; Cohen, N. Magnesium and C-reactive protein in heart failure: An anti-inflammatory effect of magnesium administration? Eur. J. Nutr. 2007, 46, 230–237. [Google Scholar] [CrossRef]
- Giacconi, R.; Muti, E.; Malavolta, M.; Cipriano, C.; Costarelli, L.; Bernardini, G.; Gasparini, N.; Mariani, E.; Saba, V.; Boccoli, G.; et al. The +838 C/G MT2A polymorphism, metals, and the inflammatory/immune response in carotid artery stenosis in elderly people. Mol. Med. 2007, 13, 388–395. [Google Scholar] [CrossRef]
- Blache, D.; Devaux, S.; Joubert, O.; Loreau, N.; Schneider, M.; Durand, P.; Prost, M.; Gaume, V.; Adrian, M.; Laurant, P.; et al. Long-term moderate magnesium-deficient diet shows relationships between blood pressure, inflammation and oxidant stress defense in aging rats. Free Radic. Biol. Med. 2006, 41, 277–284. [Google Scholar] [CrossRef]
- Adrian, M.; Chanut, E.; Laurant, P.; Gaume, V.; Berthelot, A. A long-term moderate magnesium-deficient diet aggravates cardiovascular risks associated with aging and increases mortality in rats. J. Hypertens. 2008, 26, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Castiglioni, S.; Cazzaniga, A.; Maier, J.A. Potential interplay between NFκB and PPARγ in human dermal microvascular endothelial cells cultured in low magnesium. Magnes. Res. 2014, 27, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Altura, B.M.; Shah, N.C.; Shah, G.J.; Zhang, A.; Li, W.; Zheng, T.; Perez-Albela, J.L.; Altura, B.T. Short-term Mg deficiency upregulates protein kinase C isoforms in cardiovascular tissues and cells; relation to NF-kB, cytokines, ceramide salvage sphingolipid pathway and PKC-zeta: Hypothesis and review. Int. J. Clin. Exp. Med. 2014, 7, 1–21. [Google Scholar]
- Chacko, S.A.; Song, Y.; Nathan, L.; Tinker, L.; de Boer, I.H.; Tylavsky, F.; Wallace, R.; Liu, S. Relations of dietary magnesium intake to biomarkers of inflammation and endothelial dysfunction in an ethnically diverse cohort of postmenopausal women. Diabetes Care 2010, 33, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Weglicki, W.B.; Mak, I.T.; Stafford, R.E.; Dickens, B.F.; Cassidy, M.M.; Phillips, T.M. Neurogenic peptides and the cardiomyopathy of magnesium-deficiency: Effects of substance P-receptor inhibition. Mol. Cell. Biochem. 1994, 130, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Rude, R.K.; Gruber, H.E.; Norton, H.J.; Wei, L.Y.; Frausto, A.; Kilburn, J. Reduction of dietary magnesium by only 50% in the rat disrupts bone and mineral metabolism. Osteoporos. Int. 2006, 17, 1022–1032. [Google Scholar] [CrossRef]
- Weglicki, W.B.; Mak, I.T.; Phillips, T.M. Blockade of cardiac inflammation in Mg2+ deficiency by substance P receptor inhibition. Circ. Res. 1994, 74, 1009–1013. [Google Scholar] [CrossRef]
- Zghoul, N.; Alam-Eldin, N.; Mak, I.T.; Silver, B.; Weglicki, W.B. Hypomagnesemia in diabetes patients: Comparison of serum and intracellular measurement of responses to magnesium supplementation and its role in inflammation. Diabetes Metab. Syndr. Obes. 2018, 11, 389–400. [Google Scholar] [CrossRef]
- Mak, I.T.; Kramer, J.H.; Weglicki, W.B. Suppression of neutrophil and endothelial activation by substance P receptor blockade in the Mg-deficient rat. Magnes. Res. 2003, 16, 91–97. [Google Scholar]
- Guerrero-Romero, F.; Rodríguez-Morán, M. Hypomagnesemia, oxidative stress, inflammation, and metabolic syndrome. Diabetes Metab. Res. Rev. 2006, 22, 471–476. [Google Scholar] [CrossRef]
- Ahokas, R.A.; Sun, Y.; Bhattacharya, S.K.; Gerling, I.C.; Weber, K.T. Aldosteronism and a proinflammatory vascular phenotype: Role of Mg2+, Ca2+, and H2O2 in peripheral blood mononuclear cells. Circulation 2005, 111, 51–57. [Google Scholar] [CrossRef]
- Malpuech-Brugère, C.; Rock, E.; Astier, C.; Nowacki, W.; Mazur, A.; Rayssiguier, Y. Exacerbated immune stress response during experimental magnesium deficiency results from abnormal cell calcium homeostasis. Life Sci. 1998, 63, 1815–1822. [Google Scholar] [CrossRef]
- Li, F.Y.; Chaigne-Delalande, B.; Kanellopoulou, C.; Davis, J.C.; Matthews, H.F.; Douek, D.C.; Cohen, J.I.; Uzel, G.; Su, H.C.; Lenardo, M.J. Second messenger role for Mg2+ revealed by human T-cell immunodeficiency. Nature 2011, 475, 471–476. [Google Scholar] [CrossRef]
- Mazur, A.; Maier, J.A.; Rock, E.; Gueux, E.; Nowacki, W.; Rayssiguier, Y. Magnesium and the inflammatory response: Potential physiopathological implications. Arch. Biochem. Biophys. 2007, 458, 48–56. [Google Scholar] [CrossRef]
- Zierler, S.; Sumoza-Toledo, A.; Suzuki, S.; Dúill, F.Ó.; Ryazanova, L.V.; Penner, R.; Ryazanov, A.G.; Fleig, A. TRPM7 kinase activity regulates murine mast cell degranulation. J. Physiol. 2016, 594, 2957–2970. [Google Scholar] [CrossRef]
- Libako, P.; Nowacki, W.; Rock, E.; Rayssiguier, Y.; Mazur, A. Phagocyte priming by low magnesium status: Input to the enhanced inflammatory and oxidative stress responses. Magnes. Res. 2010, 23, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ferrè, S.; Baldoli, E.; Leidi, M.; Maier, J.A.M. Magnesium deficiency promotes a pro-atherogenic phenotype in cultured human endothelial cells via activation of NFkB. Biochim. Biophys. Acta 2010, 1802, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Bernardini, D.; Nasulewic, A.; Mazur, A.; Maier, J.A. Magnesium and microvascular endothelial cells: A role in inflammation and angiogenesis. Front. Biosci. 2005, 10, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Rochelson, B.; Dowling, O.; Schwartz, N.; Metz, C.N. Magnesium sulfate suppresses inflammatory responses by human umbilical vein endothelial cells (HuVECs) through the NFkappaB pathway. J. Reprod. Immunol. 2007, 73, 101–107. [Google Scholar] [CrossRef]
- Kohli, P.; Levy, B.D. Resolvins and protectins: Mediating solutions to inflammation. Br. J. Pharmacol. 2009, 158, 960–971. [Google Scholar] [CrossRef]
- Bussière, F.I.; Gueux, E.; Rock, E.; Girardeau, J.P.; Tridon, A.; Mazur, A.; Rayssiguier, Y. Increased phagocytosis and production of reactive oxygen species by neutrophils during magnesium deficiency in rats and inhibition by high magnesium concentration. Br. J. Nutr. 2002, 87, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Bussière, F.I.; Mazur, A.; Fauquert, J.L.; Labbe, A.; Rayssiguier, Y.; Tridon, A. High magnesium concentration in vitro decreases human leukocyte activation. Magnes. Res. 2002, 15, 43–48. [Google Scholar] [PubMed]
- Montell, C. Mg2+ homeostasis: The Mg2+nificent TRPM chanzymes. Curr. Biol. 2003, 13, R799–R801. [Google Scholar] [CrossRef] [PubMed]
- Bates-Withers, C.; Sah, R.; Clapham, D.E. TRPM7, the Mg2+ inhibited channel and kinase. In Transient Receptor Potential Channels; Islam, M.S., Ed.; Springer: Dordrecht, The Netherlands, 2011; pp. 173–183. [Google Scholar] [CrossRef]
- Schlingmann, K.P.; Gudermann, T. A critical role of TRPM channel-kinase for human magnesium transport. J. Physiol. 2005, 566, 301–308. [Google Scholar] [CrossRef]
- Yogi, A.; Callera, G.E.; Antunes, T.T.; Tostes, R.C.; Touyz, R.M. Transient receptor potential melastatin 7 (TRPM7) cation channels, magnesium and the vascular system in hypertension. Circ. J. 2011, 75, 237–245. [Google Scholar] [CrossRef]
- Chokshi, R.; Matsushita, M.; Kozak, J.A. Detailed examination of Mg2+ and pH sensitivity of human TRPM7 channels. Am. J. Physiol. Cell Physiol. 2012, 302, C1004–C1011. [Google Scholar] [CrossRef]
- Kozak, J.A.; Matsushita, M.; Nairn, A.C.; Cahalan, M.D. Charge screening by internal pH and polyvalent cations as a mechanism for activation, inhibition, and rundown of TRPM7/MIC channels. J. Gen. Physiol. 2005, 126, 499–514. [Google Scholar] [CrossRef]
- Rios, F.J.; Zou, Z.-G.; Harvey, A.P.; Harvey, K.Y.; Nosalski, R.; Anyfanti, P.; Camargo, L.L.; Lacchini, S.; Ryazanov, A.G.; Ryazanova, L.; et al. Chanzyme TRPM7 protects against cardiovascular inflammation and fibrosis. Cardiovasc. Res. 2019, 116, 721–735. [Google Scholar] [CrossRef]
- Schilling, T.; Miralles, F.; Eder, C. TRPM7 regulates proliferation and polarisation of macrophages. J. Cell Sci. 2014, 127, 4561–4566. [Google Scholar] [CrossRef]
- Li, F.Y.; Lenardo, M.J.; Chaigne-Delalande, B. Loss of MAGT1 abrogates the Mg2+ flux required for T cell signaling and leads to a novel human primary immunodeficiency. Magnes. Res. 2011, 24, S109–S114. [Google Scholar] [CrossRef]
- Matsuda-Lennikov, M.; Biancalana, M.; Zou, J.; Ravell, J.C.; Zheng, L.; Kanellopoulou, C.; Jiang, P.; Notarangelo, G.; Jing, H.; Masutani, E.; et al. Magnesium transporter 1 (MAGT1) deficiency causes selective defects in N-linked glycosylation and expression of immune-response genes. J. Biol. Chem. 2019, 294, 13638–13656. [Google Scholar] [CrossRef] [PubMed]
- Kostov, K.; Halacheva, L. Role of magnesium deficiency in promoting atherosclerosis, endothelial dysfunction, and arterial stiffening as risk factors for hypertension. Int. J. Mol. Sci. 2018, 19, 1724. [Google Scholar] [CrossRef] [PubMed]
- Sanui, H.; Rubin, A.H. Membrane bound and cellular cationic changes associated with insulin stimulation of cultured cells. J. Cell. Physiol. 1978, 96, 265–278. [Google Scholar] [CrossRef] [PubMed]
- Jamilian, M.; Samimi, M.; Faraneh, A.E.; Aghadavod, E.; Shahrzad, H.D.; Chamani, M.; Mafi, A.; Asemi, Z. Magnesium supplementation affects gene expression related to insulin and lipid in patients with gestational diabetes. Magnes. Res. 2017, 30, 71–79. [Google Scholar] [CrossRef]
- Solaimani, H.; Soltani, N.; MaleKzadeh, K.; Sohrabipour, S.; Zhang, N.; Nasri, S.; Wang, Q. Modulation of GLUT4 expression by oral administration of Mg2+ to control sugar levels in STZ-induced diabetic rats. Can. J. Physiol. Pharmacol. 2014, 92, 438–444. [Google Scholar] [CrossRef]
- Van Laecke, S.; Caluwe, R.; Huybrechts, I.; Nagler, E.V.; Vanholder, R.; Peeters, P.; Van Vlem, B.; Van Biesen, W. Effect of magnesium supplements on insulin secretion after kidney transplantation: A randomized controlled trial. Ann. Transplant. 2017, 22, 524–531. [Google Scholar] [CrossRef]
- Rodríguez-Morán, M.; Guerrero-Romero, F. Insulin secretion is decreased in non-diabetic individuals with hypomagnesaemia. Diabetes Metab. Res. Rev. 2011, 27, 590–596. [Google Scholar] [CrossRef]
- Wright, E., Jr.; Scism-Bacon, J.L.; Glass, L.C. Oxidative stress in type 2 diabetes: The role of fasting and postprandial glycaemia. Int. J. Clin. Pract. 2006, 60, 308–314. [Google Scholar] [CrossRef]
- Cunha, A.R.; Umbelino, B.; Correia, M.L.; Neves, M.F. Magnesium and vascular changes in hypertension. Int. J. Hypertens. 2012, 2012, 754250. [Google Scholar] [CrossRef]
- Kamran, M.; Kharazmi, F.; Malekzadeh, K.; Talebi, A.; Khosravi, F.; Soltani, N. Effect of long-term administration of oral magnesium sulfate and insulin to reduce streptozotocin-induced hyperglycemia in rats: The role of Akt2 and IRS1 gene expressions. Biol. Trace Elem. Res. 2019, 190, 396–404. [Google Scholar] [CrossRef]
- Barbagallo, M.; Dominguez, L.J.; Tagliamonte, M.R.; Resnick, L.M.; Paolisso, G. Effects of vitamin E and glutathione on glucose metabolism: Role of magnesium. Hypertension 1999, 34, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, L.; Garfinkel, D. Magnesium regulation of the glycolytic pathway and the enzymes involved. Magnesium 1985, 4, 60–72. [Google Scholar] [PubMed]
- Denton, R.M.; Randle, P.J.; Bridges, B.J.; Cooper, R.H.; Kerbey, A.L.; Pask, H.T.; Severson, D.L.; Stansbie, D.; Whitehouse, S. Regulation of mammalian pyruvate dehydrogenase. Mol. Cell. Biochem. 1975, 9, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.P.; Diggle, T.A.; Denton, R.M. Sensitivity of pyruvate dehydrogenase phosphate phosphatase to magnesium ions. Similar effects of spermine and insulin. Biochem. J. 1986, 238, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Mastrototaro, L.; Tietjen, U.; Sponder, G.; Vormann, J.; Aschenbach, J.R.; Kolisek, M. Insulin modulates the Na+/Mg2+ exchanger SLC41A1 and influences Mg2+ efflux from intracellular stores in transgenic HEK293 cells. J. Nutr. 2015, 145, 2440–2447. [Google Scholar] [CrossRef] [PubMed]
- Kolisek, M.; Launay, P.; Beck, A.; Sponder, G.; Serafini, N.; Brenkus, M.; Froschauer, E.M.; Martens, H.; Fleig, A.; Schweigel, M. SLC41A1 is a novel mammalian Mg2+ carrier. J. Biol. Chem. 2008, 283, 16235–16247. [Google Scholar] [CrossRef] [PubMed]
- Abbott, L.G.; Rude, R.K. Clinical manifestations of magnesium deficiency. Miner. Electrolyte Metab. 1993, 19, 314–322. [Google Scholar]
- Shafiq, A.; Goyal, A.; Jones, P.G.; Sahil, S.; Hoffman, M.; Qintar, M.; Buchanan, D.M.; Kosiborod, M.; Arnold, S.V. Serum magnesium levels and in-hospital mortality in acute myocardial infarction. J. Am. Coll. Cardiol. 2017, 69, 2771–2772. [Google Scholar] [CrossRef]
- Woods, K.L.; Fletcher, S.; Roffe, C.; Haider, Y. Intravenous magnesium sulphate in suspected acute myocardial infarction: Results of the second Leicester Intravenous Magnesium Intervention Trial (LIMIT-2). Lancet 1992, 339, 1553–1558. [Google Scholar] [CrossRef]
- Woods, K.L.; Fletcher, S. Long-term outcome after intravenous magnesium sulphate in suspected acute myocardial infarction: The second Leicester Intravenous Magnesium Intervention Trial (LIMIT-2). Lancet 1994, 343, 816–819. [Google Scholar] [CrossRef]
- Ince, C.; Schulman, S.P.; Quigley, J.F.; Berger, R.D.; Kolasa, M.; Ferguson, R.; Silver, B.; Haigney, M.C. Usefulness of magnesium sulfate in stabilizing cardiac repolarization in heart failure secondary to ischemic cardiomyopathy. Am. J. Cardiol. 2001, 88, 224–229. [Google Scholar] [CrossRef]
- Bashir, Y.; Sneddon, J.F.; Staunton, H.A.; Haywood, G.A.; Simpson, I.A.; McKenna, W.J.; Camm, A.J. Effects of long-term oral magnesium chloride replacement in congestive heart failure secondary to coronary artery disease. Am. J. Cardiol. 1993, 72, 1156–1162. [Google Scholar] [CrossRef]
- Gottlieb, S.S.; Fisher, M.L.; Pressel, M.D.; Patten, R.D.; Weinberg, M.; Greenberg, N. Effects of intravenous magnesium sulfate on arrhythmias in patients with congestive heart failure. Am. Heart J. 1993, 125, 1645–1650. [Google Scholar] [CrossRef]
- Stepura, O.B.; Martynow, A.I. Magnesium orotate in severe congestive heart failure (MACH). Int. J. Cardiol. 2009, 131, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Terzi, A.; Furlan, G.; Chiavacci, P.; Dal Corso, B.; Luzzani, A.; Dalla Volta, S. Prevention of atrial tachyarrhythmias after non-cardiac thoracic surgery by infusion of magnesium sulfate. Thorac. Cardiovasc. Surg. 1996, 44, 300–303. [Google Scholar] [CrossRef]
- He, D.; Aggarwal, N.; Zurakowski, D.; Jonas, R.A.; Berul, C.I.; Hanumanthaiah, S.; Moak, J.P. Lower risk of postoperative arrhythmias in congenital heart surgery following intraoperative administration of magnesium. J. Thorac. Cardiovasc. Surg. 2018, 156, 763–770.e1. [Google Scholar] [CrossRef]
- Tzivoni, D.; Banai, S.; Schuger, C.; Benhorin, J.; Keren, A.; Gottlieb, S.; Stern, S. Treatment of torsade de pointes with magnesium sulfate. Circulation 1988, 77, 392–397. [Google Scholar] [CrossRef]
- Baker, W.L. Treating arrhythmias with adjunctive magnesium: Identifying future research directions. Eur. Heart J. Cardiovasc. Pharmacother. 2017, 3, 108–117. [Google Scholar] [CrossRef][Green Version]
- Ho, K.M. Intravenous magnesium for cardiac arrhythmias: Jack of all trades. Magnes. Res. 2008, 21, 65–68. [Google Scholar]
- Ho, K.M.; Sheridan, D.J.; Paterson, T. Use of intravenous magnesium to treat acute onset atrial fibrillation: A meta-analysis. Heart 2007, 93, 1433–1440. [Google Scholar] [CrossRef]
- Lomivorotov, V.V.; Efremov, S.M.; Karaskov, A.M. Pharmacokinetics of magnesium in cardiac surgery: Implications for prophylaxis against atrial fibrillation. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1295–1296. [Google Scholar] [CrossRef] [PubMed]
- Shiga, T.; Wajima, Z.; Inoue, T.; Ogawa, R. Magnesium prophylaxis for arrhythmias after cardiac surgery: A meta-analysis of randomized controlled trials. Am. J. Med. 2004, 117, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Biesenbach, P.; Mårtensson, J.; Lucchetta, L.; Bangia, R.; Fairley, J.; Jansen, I.; Matalanis, G.; Bellomo, R. Pharmacokinetics of magnesium bolus therapy in cardiothoracic surgery. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Davey, M.J.; Teubner, D. A randomized controlled trial of magnesium sulfate, in addition to usual care, for rate control in atrial fibrillation. Ann. Emerg. Med. 2005, 45, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Zaman, A.G.; Alamgir, F.; Richens, T.; Williams, R.; Rothman, M.T.; Mills, P.G. The role of signal averaged P wave duration and serum magnesium as a combined predictor of atrial fibrillation after elective coronary artery bypass surgery. Heart 1997, 77, 527–531. [Google Scholar] [CrossRef]
- Kohno, H.; Koyanagi, T.; Kasegawa, H.; Miyazaki, M. Three-day magnesium administration prevents atrial fibrillation after coronary artery bypass grafting. Ann. Thorac. Surg. 2005, 79, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Banai, S.; Tzivoni, D. Drug therapy for torsade de pointes. J. Cardiovasc. Electrophysiol. 1993, 4, 206–210. [Google Scholar] [CrossRef]
- Zipes, D.P.; Camm, A.J.; Borggrefe, M.; Buxton, A.E.; Chaitman, B.; Fromer, M.; Gregoratos, G.; Klein, G.; Moss, A.J.; Myerburg, R.J.; et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death--executive summary: A report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death) Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Eur. Heart J. 2006, 27, 2099–2140. [Google Scholar] [CrossRef]
- Chinushi, M.; Sugiura, H.; Komura, S.; Hirono, T.; Izumi, D.; Tagawa, M.; Furushima, H.; Aizawa, Y. Effects of intravenous magnesium in a prolonged QT interval model of polymorphic ventricular tachycardia focus on transmural ventricular repolarization. Pacing Clin. Electrophysiol. 2005, 28, 844–850. [Google Scholar] [CrossRef]
- Bailie, D.S.; Inoue, H.; Kaseda, S.; Ben-David, J.; Zipes, D.P. Magnesium suppression of early afterdepolarizations and ventricular tachyarrhythmias induced by cesium in dogs. Circulation 1988, 77, 1395–1402. [Google Scholar] [CrossRef]
- Ford, E.S. Serum magnesium and ischaemic heart disease: Findings from a national sample of US adults. Int. J. Epidemiol. 1999, 28, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Freedman, A.M.; Cassidy, M.M.; Weglicki, W.B. Magnesium-deficient myocardium demonstrates an increased susceptibility to an in vivo oxidative stress. Magnes. Res. 1991, 4, 185–189. [Google Scholar] [PubMed]
- Shi, B.; Heavner, J.E.; Boylan, L.M.; Wang, M.J.; Spallholz, J.E. Dietary magnesium deficiency increases Giα levels in the rat heart after myocardial infarction. Cardiovasc. Res. 1995, 30, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Morton, B.C.; Nair, R.C.; Smith, F.M.; McKibbon, T.G.; Poznanski, W.J. Magnesium therapy in acute myocardial infarction--a double-blind study. Magnesium 1984, 3, 346–352. [Google Scholar]
- Rasmussen, H.S.; McNair, P.; Norregard, P.; Backer, V.; Lindeneg, O.; Balslev, S. Intravenous magnesium in acute myocardial infarction. Lancet 1986, 1, 234–236. [Google Scholar] [CrossRef]
- Smith, L.F.; Heagerty, A.M.; Bing, R.F.; Barnett, D.B. Intravenous infusion of magnesium sulphate after acute myocardial infarction: Effects on arrhythmias and mortality. Int. J. Cardiol. 1986, 12, 175–183. [Google Scholar] [CrossRef]
- Abraham, A.S.; Rosenmann, D.; Kramer, M.; Balkin, J.; Zion, M.M.; Farbstien, H.; Eylath, U. Magnesium in the prevention of lethal arrhythmias in acute myocardial infarction. Arch. Intern. Med. 1987, 147, 753–755. [Google Scholar] [CrossRef]
- Shechter, M.; Hod, H.; Rabinowitz, B.; Boyko, V.; Chouraqui, P. Long-term outcome of intravenous magnesium therapy in thrombolysis-ineligible acute myocardial infarction patients. Cardiology 2003, 99, 205–210. [Google Scholar] [CrossRef]
- Shen, A.C.; Jennings, R.B. Myocardial calcium and magnesium in acute ischemic injury. Am. J. Pathol. 1972, 67, 417–440. [Google Scholar]
- Vormann, J.; Fischer, G.; Classen, H.G.; Thöni, H. Influence of decreased and increased magnesium supply on the cardiotoxic effects of epinephrine in rats. Arzneimittelforschung 1983, 33, 205–210. [Google Scholar]
- Parikka, H.; Toivonen, L.; Naukkarinen, V.; Tierala, I.; Pohjola-Sintonen, S.; Heikkilä, J.; Nieminen, M.S. Decreases by magnesium of QT dispersion and ventricular arrhythmias in patients with acute myocardial infarction. Eur. Heart J. 1999, 20, 111–120. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Benz, I.; Kohlhardt, M. Modulation of single cardiac Na+ channels by cytosolic Mg++ ions. Eur. Biophys. J. 1991, 20, 223–228. [Google Scholar] [CrossRef] [PubMed]
- White, R.E.; Hartzell, H.C. Effects of intracellular free magnesium on calcium current in isolated cardiac myocytes. Science 1988, 239, 778–780. [Google Scholar] [CrossRef]
- Hartzell, H.C.; White, R.E. Effects of magnesium on inactivation of the voltage-gated calcium current in cardiac myocytes. J. Gen. Physiol. 1989, 94, 745–767. [Google Scholar] [CrossRef] [PubMed]
- Agus, Z.S.; Kelepouris, E.; Dukes, I.; Morad, M. Cytosolic magnesium modulates calcium channel activity in mammalian ventricular cells. Am. J. Physiol. 1989, 256, C452–C455. [Google Scholar] [CrossRef]
- Wu, J.Y.; Lipsius, S.L. Effects of extracellular Mg2+ on T- and L-type Ca2+ currents in single atrial myocytes. Am. J. Physiol. 1990, 259, H1842–H1850. [Google Scholar] [CrossRef]
- Wei, S.K.; Quigley, J.F.; Hanlon, S.U.; O’Rourke, B.; Haigney, M.C. Cytosolic free magnesium modulates Na/Ca exchange currents in pig myocytes. Cardiovasc. Res. 2002, 53, 334–340. [Google Scholar] [CrossRef]
- Wei, S.K.; Hanlon, S.U.; Haigney, M.C. Beta-adrenergic stimulation of pig myocytes with decreased cytosolic free magnesium prolongs the action potential and enhances triggered activity. J. Cardiovasc. Electrophysiol. 2002, 13, 587–592. [Google Scholar] [CrossRef]
- Duchatelle-Gourdon, I.; Hartzell, H.C.; Lagrutta, A.A. Modulation of the delayed rectifier potassium current in frog cardiomyocytes by beta-adrenergic agonists and magnesium. J. Physiol. 1989, 415, 251–274. [Google Scholar] [CrossRef]
- Duchatelle-Gourdon, I.; Lagrutta, A.A.; Hartzell, H.C. Effects of Mg2+ on basal and beta-adrenergic-stimulated delayed rectifier potassium current in frog atrial myocytes. J. Physiol. 1991, 435, 333–347. [Google Scholar] [CrossRef]
- Ishihara, K.; Mitsuiye, T.; Noma, A.; Takano, M. The Mg2+ block and intrinsic gating underlying inward rectification of the K+ current in guinea-pig cardiac myocytes. J. Physiol. 1989, 419, 297–320. [Google Scholar] [CrossRef] [PubMed]
- Hartzell, H.C.; Duchatelle-Gourdon, I. Regulation of the cardiac delayed rectifier K current by neurotransmitters and magnesium. Cardiovasc. Drugs Ther. 1993, 7 (Suppl. 3), 547–554. [Google Scholar] [CrossRef] [PubMed]
- Hirahara, K.; Matsubayashi, T.; Matsuura, H.; Ehara, T. Intracellular Mg2+ depletion depresses the delayed rectifier K+ current in guinea pig ventricular myocytes. Jpn. J. Physiol. 1998, 48, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Findlay, I. ATP-sensitive K+ channels in rat ventricular myocytes are blocked and inactivated by internal divalent cations. Pflug. Arch. 1987, 410, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Chung, C.; Vizcaychipi, M. Magnesium: The neglected electrolyte? A clinical review. Pharmacol. Pharm. 2014, 5, 11. [Google Scholar] [CrossRef]
- Dunnett, J.; Nayler, W.G. Calcium efflux from cardiac sarcoplasmic reticulum: Effects of calcium and magnesium. J. Mol. Cell. Cardiol. 1978, 10, 487–498. [Google Scholar] [CrossRef]
- Laver, D.R.; Baynes, T.M.; Dulhunty, A.F. Magnesium inhibition of ryanodine-receptor calcium channels: Evidence for two independent mechanisms. J. Membr. Biol. 1997, 156, 213–229. [Google Scholar] [CrossRef]
- Laver, D.R.; Honen, B.N. Luminal Mg2+, a key factor controlling RYR2-mediated Ca2+ release: Cytoplasmic and luminal regulation modeled in a tetrameric channel. J. Gen. Physiol. 2008, 132, 429–446. [Google Scholar] [CrossRef]
- Bara, M.; Guiet-Bara, A.; Durlach, J. Regulation of sodium and potassium pathways by magnesium in cell membranes. Magnes. Res. 1993, 6, 167–177. [Google Scholar]
- Ishihara, K.; Sarai, N.; Asakura, K.; Noma, A.; Matsuoka, S. Role of Mg2+ block of the inward rectifier K+ current in cardiac repolarization reserve: A quantitative simulation. J. Mol. Cell. Cardiol. 2009, 47, 76–84. [Google Scholar] [CrossRef]
- Choudhary, G.; Dudley, S.C., Jr. Heart failure, oxidative stress, and ion channel modulation. Congest. Heart Fail. 2002, 8, 148–155. [Google Scholar] [CrossRef]
- Ayoub, K.F.; Pothineni, N.V.K.; Rutland, J.; Ding, Z.; Mehta, J.L. Immunity, inflammation, and oxidative stress in heart failure: Emerging molecular targets. Cardiovasc. Drugs Ther. 2017, 31, 593–608. [Google Scholar] [CrossRef]
- Dudley, S.C.; Hoch, N.E.; McCann, L.A.; Honeycutt, C.; Diamandopoulos, L.; Fukai, T.; Harrison, D.G.; Dikalov, S.I.; Langberg, J. Atrial fibrillation increases production of superoxide by the left atrium and left atrial appendage: Role of the NADPH and xanthine oxidases. Circulation 2005, 112, 1266–1273. [Google Scholar] [CrossRef] [PubMed]
- Hanna, I.R.; Heeke, B.; Bush, H.; Brosius, L.; King-Hageman, D.; Dudley, S.C.; Beshai, J.F.; Langberg, J.J. Lipid-lowering drug use is associated with reduced prevalence of atrial fibrillation in patients with left ventricular systolic dysfunction. Heart Rhythm 2006, 3, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Gao, G.; Dudley, S.C., Jr. Redox regulation, NF-kB, and atrial fibrillation. Antioxid. Redox Signal. 2009, 11, 2265–2277. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.K.; Martin, D.O.; Sprecher, D.; Wazni, O.; Kanderian, A.; Carnes, C.A.; Bauer, J.A.; Tchou, P.J.; Niebauer, M.J.; Natale, A.; et al. C-reactive protein elevation in patients with atrial arrhythmias: Inflammatory mechanisms and persistence of atrial fibrillation. Circulation 2001, 104, 2886–2891. [Google Scholar] [CrossRef]
- Aviles, R.J.; Martin, D.O.; Apperson-Hansen, C.; Houghtaling, P.L.; Rautaharju, P.; Kronmal, R.A.; Tracy, R.P.; Van Wagoner, D.R.; Psaty, B.M.; Lauer, M.S.; et al. Inflammation as a risk factor for atrial fibrillation. Circulation 2003, 108, 3006–3010. [Google Scholar] [CrossRef]
- Liu, M.; Liu, H.; Dudley, S.C., Jr. Reactive oxygen species originating from mitochondria regulate the cardiac sodium channel. Circ. Res. 2010, 107, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Jeong, E.M.; Liu, M.; Sturdy, M.; Gao, G.; Sovari, A.A.; Dudley, J. Metabolic stress, reactive oxygen species, and arrhythmia. J. Mol. Cell. Cardiol. 2011, 52, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Shi, G.; Yang, K.C.; Gu, L.; Kanthasamy, A.G.; Anantharam, V.; Dudley, J. Role of protein kinase C in metabolic regulation of the cardiac Na+ channel. Heart Rhythm 2017, 14, 440–447. [Google Scholar] [CrossRef]
- Nakajima, T.; Davies, S.S.; Matafonova, E.; Potet, F.; Amarnath, V.; Tallman, K.A.; Serwa, R.A.; Porter, N.A.; Balser, J.R.; Kupershmidt, S.; et al. Selective g-ketoaldehyde scavengers protect Nav1.5 from oxidant-induced inactivation. J. Mol. Cell. Cardiol. 2010, 48, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Xie, Y.; Wen, H.; Xiao, D.; Allen, C.; Fefelova, N.; Dun, W.; Boyden, P.A.; Qu, Z.; Xie, L.H. Role of the transient outward potassium current in the genesis of early afterdepolarizations in cardiac cells. Cardiovasc. Res. 2012, 95, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Coetzee, W.A.; Opie, L.H. Effects of oxygen free radicals on isolated cardiac myocytes from guinea-pig ventricle: Electrophysiological studies. J. Mol. Cell. Cardiol. 1992, 24, 651–663. [Google Scholar] [CrossRef]
- Fearon, I.M.; Palmer, A.C.V.; Balmforth, A.J.; Ball, S.G.; Varadi, G.; Peers, C. Modulation of recombinant human cardiac L-type Ca2+ channel a1C subunits by redox agents and hypoxia. J. Physiol. 1999, 514, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Hool, L.C.; Di Maria, C.A.; Viola, H.M.; Arthur, P.G. Role of NAD(P)H oxidase in the regulation of cardiac L-type Ca2+ channel function during acute hypoxia. Cardiovasc. Res. 2005, 67, 624–635. [Google Scholar] [CrossRef]
- DeSantiago, J.; Bare, D.J.; Varma, D.; Solaro, R.J.; Arora, R.; Banach, K. Loss of p21-activated kinase 1 (Pak1) promotes atrial arrhythmic activity. Heart Rhythm 2018, 15, 1233–1241. [Google Scholar] [CrossRef]
- Cherednichenko, G.; Zima, A.V.; Feng, W.; Schaefer, S.; Blatter, L.A.; Pessah, I.N. NADH oxidase activity of rat cardiac sarcoplasmic reticulum regulates calcium-induced calcium release. Circ. Res. 2004, 94, 478–486. [Google Scholar] [CrossRef]
- Gao, L.; Li, Y.; Schultz, H.D.; Wang, W.Z.; Wang, W.; Finch, M.; Smith, L.M.; Zucker, I.H. Downregulated Kv4.3 expression in the RVLM as a potential mechanism for sympathoexcitation in rats with chronic heart failure. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, H945–H955. [Google Scholar] [CrossRef]
- Dong, D.; Liu, Y.; Zhou, Y.; Song, W.; Wang, H.; Yang, B. Decreases of voltage-dependent K+ currents densities in ventricular myocytes of guinea pigs by chronic oxidant stress. Acta Pharmacol. Sin. 2004, 25, 751–755. [Google Scholar]
- Sunagawa, T.; Shimizu, T.; Matsumoto, A.; Tagashira, M.; Kanda, T.; Shirasawa, T.; Nakaya, H. Cardiac electrophysiological alterations in heart/muscle-specific manganese-superoxide dismutase-deficient mice: Prevention by a dietary antioxidant polyphenol. BioMed Res. Int. 2014, 2014, 704291. [Google Scholar] [CrossRef]
- Yalta, T.; Yalta, K. Systemic inflammation and arrhythmogenesis: A review of mechanistic and clinical perspectives. Angiology 2018, 69, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Korantzopoulos, P.; Letsas, K.P.; Tse, G.; Fragakis, N.; Goudis, C.A.; Liu, T. Inflammation and atrial fibrillation: A comprehensive review. J. Arrhythmia 2018, 34, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; He, K.; Levitan, E.B.; Manson, J.E.; Liu, S. Effects of oral magnesium supplementation on glycaemic control in type 2 diabetes: A meta-analysis of randomized double-blind controlled trials. Diabet. Med. 2006, 23, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Bertinato, J.; Xiao, C.W.; Ratnayake, W.M.; Fernandez, L.; Lavergne, C.; Wood, C.; Swist, E. Lower serum magnesium concentration is associated with diabetes, insulin resistance, and obesity in South Asian and white Canadian women but not men. Food Nutr. Res. 2015, 59, 25974. [Google Scholar] [CrossRef] [PubMed]
- Schutten, J.C.; Gomes-Neto, A.W.; Navis, G.; Gansevoort, R.T.; Dullaart, R.P.F.; Kootstra-Ros, J.E.; Danel, R.M.; Goorman, F.; Gans, R.O.B.; de Borst, M.H.; et al. Lower plasma magnesium, measured by nuclear magnetic resonance spectroscopy, is associated with increased risk of developing type 2 diabetes mellitus in women: Results from a Dutch prospective cohort study. J. Clin. Med. 2019, 8, 169. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendía, L.E.; Sahebkar, A.; Rodríguez-Morán, M.; Guerrero-Romero, F. A systematic review and meta-analysis of randomized controlled trials on the effects of magnesium supplementation on insulin sensitivity and glucose control. Pharmacol. Res. 2016, 111, 272–282. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Simental-Mendía, L.E.; Hernández-Ronquillo, G.; Rodriguez-Morán, M. Oral magnesium supplementation improves glycaemic status in subjects with prediabetes and hypomagnesaemia: A double-blind placebo-controlled randomized trial. Diabetes Metab. 2015, 41, 202–207. [Google Scholar] [CrossRef]
- Hatzistavri, L.S.; Sarafidis, P.A.; Georgianos, P.I.; Tziolas, I.M.; Aroditis, C.P.; Zebekakis, P.E.; Pikilidou, M.I.; Lasaridis, A.N. Oral magnesium supplementation reduces ambulatory blood pressure in patients with mild hypertension. Am. J. Hypertens. 2009, 22, 1070–1075. [Google Scholar] [CrossRef]
- Shechter, M.; Merz, C.N.; Rude, R.K.; Paul Labrador, M.J.; Meisel, S.R.; Shah, P.K.; Kaul, S. Low intracellular magnesium levels promote platelet-dependent thrombosis in patients with coronary artery disease. Am. Heart J. 2000, 140, 212–218. [Google Scholar] [CrossRef]
- Rayssiguier, Y.; Noé, L.; Etienne, J.; Gueux, E.; Cardot, P.; Mazur, A. Effect of magnesium deficiency on post-heparin lipase activity and tissue lipoprotein lipase in the rat. Lipids 1991, 26, 182–186. [Google Scholar] [CrossRef]
- Bussière, L.; Mazur, A.; Gueux, E.; Nowacki, W.; Rayssiguier, Y. Triglyceride-rich lipoproteins from magnesium-deficient rats are more susceptible to oxidation by cells and promote proliferation of cultured vascular smooth muscle cells. Magnes. Res. 1995, 8, 151–157. [Google Scholar] [PubMed]
- Martínez-Revelles, S.; García-Redondo, A.B.; Avendaño, M.S.; Varona, S.; Palao, T.; Orriols, M.; Roque, F.R.; Fortuño, A.; Touyz, R.M.; Martínez-González, J.; et al. Lysyl oxidase induces vascular oxidative stress and contributes to arterial stiffness and abnormal elastin structure in hypertension: Role of p38MAPK. Antioxid. Redox Signal. 2017, 27, 379–397. [Google Scholar] [CrossRef] [PubMed]
- Gotru, S.K.; Chen, W.; Kraft, P.; Becker, I.C.; Wolf, K.; Stritt, S.; Zierler, S.; Hermanns, H.M.; Rao, D.; Perraud, A.L.; et al. TRPM7 kinase controls calcium responses in arterial thrombosis and stroke in mice. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Lazard, E.M. A preliminary report on the intravenous use of magnesium sulphate in puerperal eclampsia. Am. J. Obstet. Gynecol. 1925, 9, 178–188. [Google Scholar] [CrossRef]
- Gabbe, S.G. Classic pages from the American Journal of obstetrics and Genecology: A preliminary report on the intravenous use of magnesium sulphate in puerperal eclampsia. Am. J. Obstet. Gynecol. 1996, 174, 1390–1391. [Google Scholar] [CrossRef]
- Zuspan, F.P. Treatment of severe preeclampsia and eclampsia. Clin. Obstet. Gynecol. 1966, 9, 954–972. [Google Scholar] [CrossRef]
- Altman, D.; Carroli, G.; Duley, L.; Farrell, B.; Moodley, J.; Neilson, J.; Smith, D. Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: A randomised placebo-controlled trial. Lancet 2002, 359, 1877–1890. [Google Scholar] [CrossRef]
- Duley, L.; Gülmezoglu, A.M.; Henderson-Smart, D.J.; Chou, D. Magnesium sulphate and other anticonvulsants for women with pre-eclampsia. Cochrane Database Syst. Rev. 2010, 2010, Cd000025. [Google Scholar] [CrossRef]
- Lu, J.F.; Nightingale, C.H. Magnesium sulfate in eclampsia and pre-eclampsia: Pharmacokinetic principles. Clin. Pharmacokinet. 2000, 38, 305–314. [Google Scholar] [CrossRef]
- Okusanya, B.O.; Oladapo, O.T.; Long, Q.; Lumbiganon, P.; Carroli, G.; Qureshi, G.; Duley, L.; Souza, J.P.; Gülmezoglu, A.M. Clinical pharmacokinetic properties of magnesium sulphate in women with pre-eclampsia and eclampsia. BJOG 2016, 123, 356–366. [Google Scholar] [CrossRef]
- Lox, C.D.; Dorsett, M.M.; Hampton, R.M. Observations on clotting activity during pre-eclampsia. Clin. Exp. Hypertens. B 1983, 2, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Ariza, A.C.; Bobadilla, N.; Díaz, L.; Avila, E.; Larrea, F.; Halhali, A. Placental gene expression of calcitonin gene-related peptide and nitric oxide synthases in preeclampsia: Effects of magnesium sulfate. Magnes. Res. 2009, 22, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Fei, X.; Hongxiang, Z.; Qi, C.; Daozhen, C. Maternal plasma levels of endothelial dysfunction mediators including AM, CGRP, sICAM-1 and tHcy in pre-eclampsia. Adv. Clin. Exp. Med. 2012, 21, 573–579. [Google Scholar]
- Chiuve, S.E.; Korngold, E.C.; Januzzi, J.L., Jr.; Gantzer, M.L.; Albert, C.M. Plasma and dietary magnesium and risk of sudden cardiac death in women. Am. J. Clin. Nutr. 2011, 93, 253–260. [Google Scholar] [CrossRef]
- Zhang, W.; Iso, H.; Ohira, T.; Date, C.; Tamakoshi, A. Associations of dietary magnesium intake with mortality from cardiovascular disease: The JACC study. Atherosclerosis 2012, 221, 587–595. [Google Scholar] [CrossRef]
- Ye, H.; Cao, P.; Zhang, X.; Lin, J.; Guo, Q.; Mao, H.; Yu, X.; Yang, X. Serum magnesium and cardiovascular mortality in peritoneal dialysis patients: A 5-year prospective cohort study. Br. J. Nutr. 2018, 120, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Sun, Y.; Xu, T.; Zhang, Y. Magnesium intake and cardiovascular disease mortality: A meta-analysis of prospective cohort studies. Int. J. Cardiol. 2013, 167, 3044–3047. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, E.H.; Frost, L.; Andreasen, F.; Mortensen, P.; Thomsen, P.E.; Pedersen, A.K. Dose-related cardiac electrophysiological effects of intravenous magnesium. A double-blind placebo-controlled dose-response study in patients with paroxysmal supraventricular tachycardia. Europace 2000, 2, 320–326. [Google Scholar] [CrossRef]
- Ranade, V.V.; Somberg, J.C. Bioavailability and pharmacokinetics of magnesium after administration of magnesium salts to humans. Am. J. Ther. 2001, 8, 345–357. [Google Scholar] [CrossRef]
- Coudray, C.; Rambeau, M.; Feillet-Coudray, C.; Gueux, E.; Tressol, J.C.; Mazur, A.; Rayssiguier, Y. Study of magnesium bioavailability from ten organic and inorganic Mg salts in Mg-depleted rats using a stable isotope approach. Magnes. Res. 2005, 18, 215–223. [Google Scholar]
- Firoz, M.; Graber, M. Bioavailability of US commercial magnesium preparations. Magnes. Res. 2001, 14, 257–262. [Google Scholar] [PubMed]
- Baker, W.L.; Kluger, J.; White, C.M.; Dale, K.M.; Silver, B.B.; Coleman, C.I. Effect of magnesium L-lactate on blood pressure in patients with an implantable cardioverter defibrillator. Ann. Pharmacother. 2009, 43, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, M.A.; Orlov, M.V.; Capparelli, E.V.; Allen, B.J.; Iseri, L.T.; Ginkel, M.; Orlov, Y.S.K. Magnesium therapy in new-onset atrial fibrillation. Am. J. Cardiol. 1994, 73, 1227–1229. [Google Scholar] [CrossRef]
- Ingemansson, M.P.; Smideberg, B.; Olsson, S.B. Intravenous MgSO4 alone and in combination with glucose, insulin and potassium (GIK) prolong the atrial cycle length in chronic atrial fibrillation. Europace 2000, 2, 106–114. [Google Scholar] [CrossRef]
- Ceremuzyński, L.; Jurgiel, R.; Kulakowski, P.; Gebalska, J. Threatening arrhythmias in acute myocardial infarction are prevented by intravenous magnesium sulfate. Am. Heart J. 1989, 118, 1333–1334. [Google Scholar] [CrossRef]
- Winters, S.L.; Sachs, R.G.; Curwin, J.H. Nonsustained polymorphous ventricular tachycardia during amiodarone therapy for atrial fibrillation complicating cardiomyopathy. Management with intravenous magnesium sulfate. Chest 1997, 111, 1454–1457. [Google Scholar] [CrossRef][Green Version]
- Sarisoy, O.; Babaoglu, K.; Tugay, S.; Barn, E.; Gokalp, A.S. Efficacy of magnesium sulfate for treatment of ventricular tachycardia in amitriptyline intoxication. Pediatr. Emerg. Care 2007, 23, 646–648. [Google Scholar] [CrossRef]
- Rasmussen, H.S.; Thomsen, P.E. The electrophysiological effects of intravenous magnesium on human sinus node, atrioventricular node, atrium, and ventricle. Clin. Cardiol. 1989, 12, 85–90. [Google Scholar] [CrossRef]
- England, M.R.; Gordon, G.; Salem, M.; Chernow, B. Magnesium administration and dysrhythmias after cardiac surgery. A placebo-controlled, double-blind, randomized trial. JAMA 1992, 268, 2395–2402. [Google Scholar] [CrossRef]
- Colquhoun, I.W.; Berg, G.A.; el-Fiky, M.; Hurle, A.; Fell, G.S.; Wheatley, D.J. Arrhythmia prophylaxis after coronary artery surgery. A randomised controlled trial of intravenous magnesium chloride. Eur. J. Cardiothorac. Surg. 1993, 7, 520–523. [Google Scholar] [CrossRef]
- Li, S.; Tian, H. Oral low-dose magnesium gluconate preventing pregnancy induced hypertension. Chin. J. Obstet. Gynecol. 1997, 32, 613–615. [Google Scholar]
- Manz, M.; Jung, W.; Lüderitz, B. Effect of magnesium on sustained ventricular tachycardia. Herz 1997, 22 (Suppl. 1), 51–55. [Google Scholar] [CrossRef] [PubMed]
- Caron, M.F.; Kluger, J.; Tsikouris, J.P.; Ritvo, A.; Kalus, J.S.; White, C.M. Effects of intravenous magnesium sulfate on the QT interval in patients receiving ibutilide. Pharmacotherapy 2003, 23, 296–300. [Google Scholar] [CrossRef]
- Kalus, J.S.; Spencer, A.P.; Tsikouris, J.P.; Chung, J.O.; Kenyon, K.W.; Ziska, M.; Kluger, J.; White, C.M. Impact of prophylactic i.v. magnesium on the efficacy of ibutilide for conversion of atrial fibrillation or flutter. Am. J. Health Syst. Pharm. 2003, 60, 2308–2312. [Google Scholar] [CrossRef] [PubMed]
- Leor, J.; Kloner, R.A. An experimental model examining the role of magnesium in the therapy of acute myocardial infarction. Am. J. Cardiol. 1995, 75, 1292–1293. [Google Scholar] [CrossRef]
- Barr, C.S.; Lang, C.C.; Hanson, J.; Arnott, M.; Kennedy, N.; Struthers, A.D. Effects of adding spironolactone to an angiotensin-converting enzyme inhibitor in chronic congestive heart failure secondary to coronary artery disease. Am. J. Cardiol. 1995, 76, 1259–1265. [Google Scholar] [CrossRef]
- Netzer, T.; Knauf, H.; Mutschler, E. Modulation of electrolyte excretion by potassium retaining diuretics. Eur. Heart J. 1992, 13 (Suppl. G), 22–27. [Google Scholar] [CrossRef]
- Schwinger, R.H.; Antoni, D.H. Triamterene may preserve lymphocyte magnesium and potassium in patients with congestive heart failure. Magnes. Res. 1992, 5, 29–32. [Google Scholar]
- Magnesium—Fact Sheet for Health Professionals. Available online: https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/ (accessed on 3 June 2020).
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y.; et al. Dietary magnesium intake and the risk of cardiovascular disease, type 2 diabetes, and all-cause mortality: A dose-response meta-analysis of prospective cohort studies. BMC Med. 2016, 14, 210. [Google Scholar] [CrossRef]
- Best Diets for Healthy Eating. Available online: https://health.usnews.com/best-diet/best-healthy-eating-diets (accessed on 11 September 2020).
- Your Guide to Lowering Your Blood Pressure with DASH. Available online: https://www.nhlbi.nih.gov/files/docs/public/heart/new_dash.pdf (accessed on 16 September 2020).
- Oesterle, A.; Weber, B.; Tung, R.; Choudhry, N.K.; Singh, J.P.; Upadhyay, G.A. Preventing postoperative atrial fibrillation after noncardiac surgery: A meta-analysis. Am. J. Med. 2018, 131, 795–804.e5. [Google Scholar] [CrossRef]
- Haigney, M.C.; Berger, R.; Schulman, S.; Gerstenblith, G.; Tunin, C.; Silver, B.; Silverman, H.S.; Tomaselli, G.; Calkins, H. Tissue magnesium levels and the arrhythmic substrate in humans. J. Cardiovasc. Electrophysiol. 1997, 8, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Farouque, H.M.; Sanders, P.; Young, G.D. Intravenous magnesium sulfate for acute termination of sustained monomorphic ventricular tachycardia associated with coronary artery disease. Am. J. Cardiol. 2000, 86, 1270–1272. [Google Scholar] [CrossRef]
- Baker, W.L.; Kluger, J.; Coleman, C.I.; White, C.M. Impact of magnesium L-lactate on occurrence of ventricular arrhythmias in patients with implantable cardioverter defibrillators: A randomized, placebo-controlled trial. Open Cardiovasc. Med. J. 2015, 9, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Feldstedt, M.; Boesgaard, S.; Bouchelouche, P.; Svenningsen, A.; Brooks, L.; Lech, Y.; Aldershvile, J.; Skagen, K.; Godtfredsen, J. Magnesium substitution in acute ischaemic heart syndromes. Eur. Heart J. 1991, 12, 1215–1218. [Google Scholar] [CrossRef] [PubMed]
- Eichhorn, E.J.; Tandon, P.K.; DiBianco, R.; Timmis, G.C.; Fenster, P.E.; Shannon, J.; Packer, M. Clinical and prognostic significance of serum magnesium concentration in patients with severe chronic congestive heart failure: The PROMISE Study. J. Am. Coll. Cardiol. 1993, 21, 634–640. [Google Scholar] [CrossRef]
- Bouida, W.; Beltaief, K.; Msolli, M.A.; Azaiez, N.; Ben Soltane, H.; Sekma, A.; Trabelsi, I.; Boubaker, H.; Grissa, M.H.; Methemem, M.; et al. Low-dose Magnesium Sulfate Versus High Dose in the Early Management of Rapid Atrial Fibrillation: Randomized Controlled Double-blind Study (LOMAGHI Study). Acad. Emerg. Med. 2019, 26, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Adams, N. Magnesium for atrial fibrillation. Emerg. Med. Australas. 2019, 31, 493. [Google Scholar] [CrossRef] [PubMed]






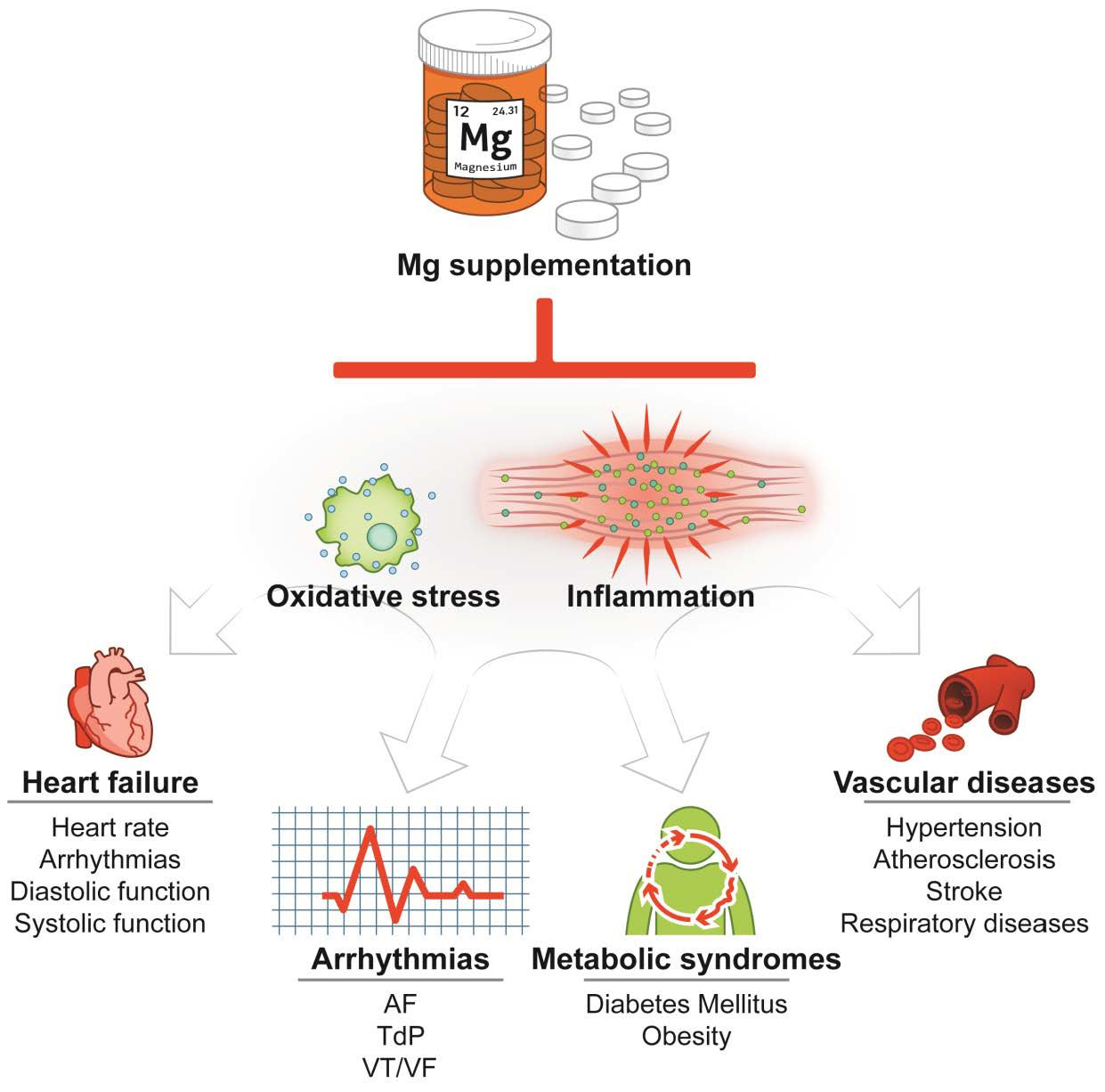{kind=link}
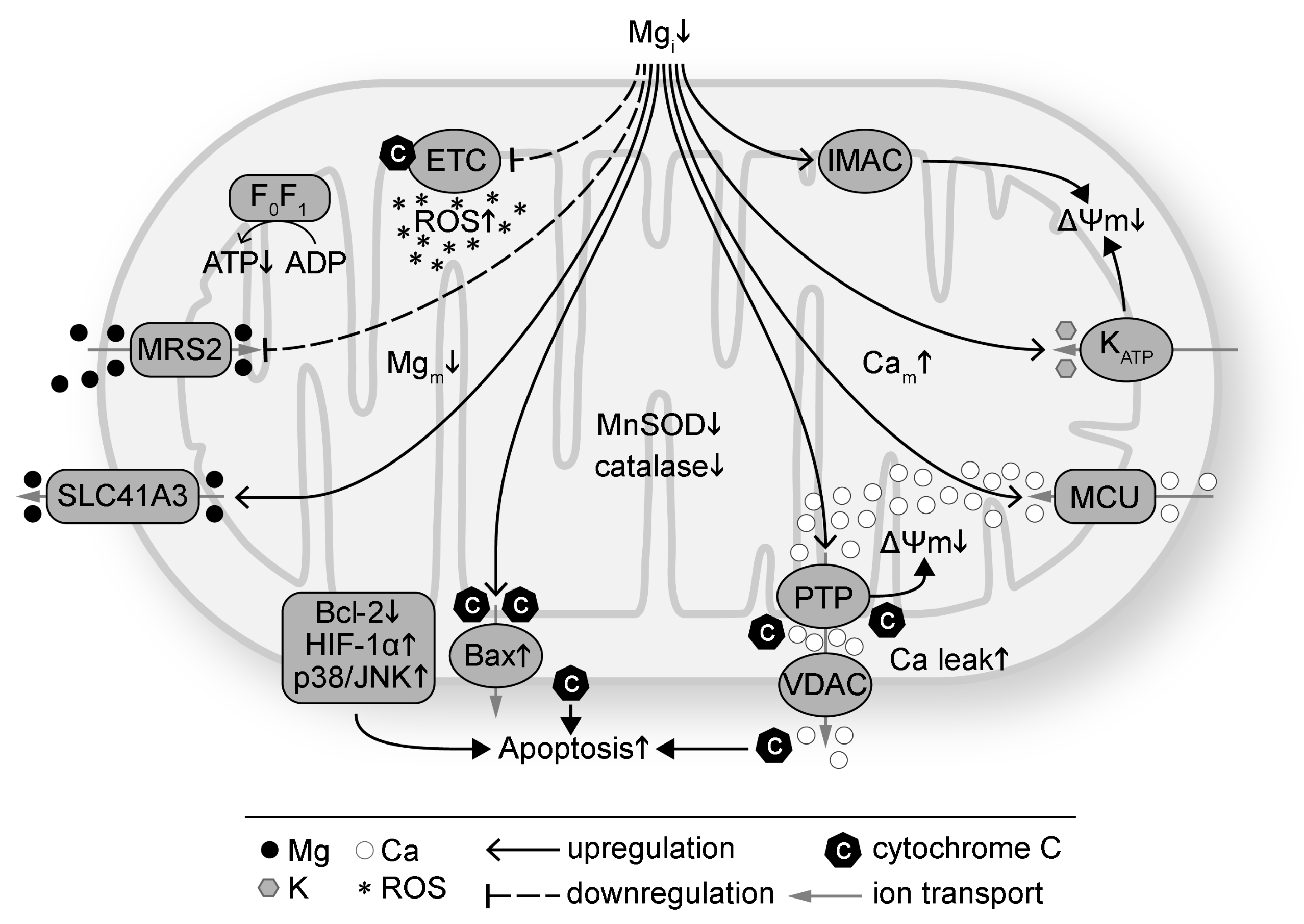{kind=link}
{kind=link}
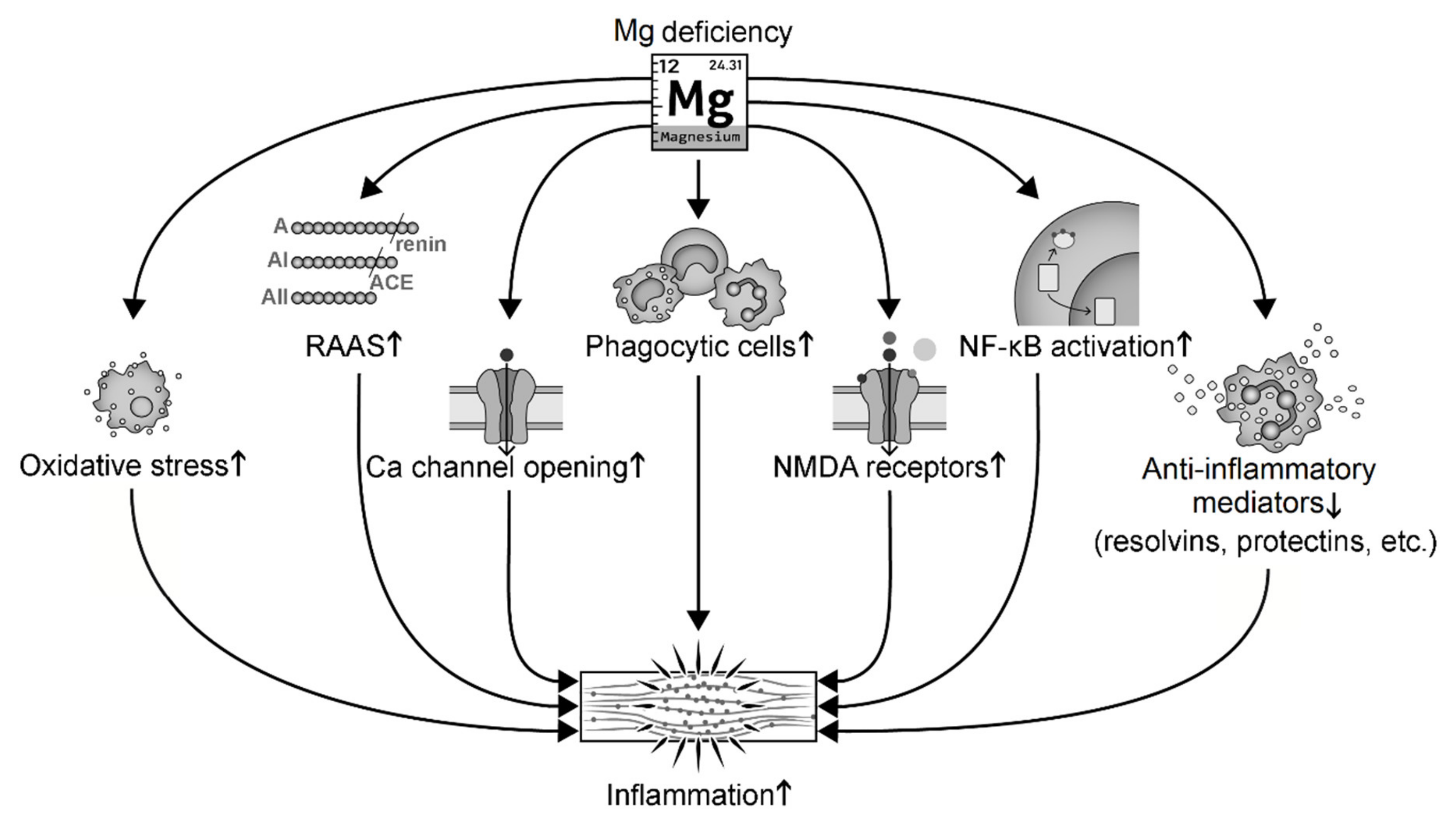{kind=link}
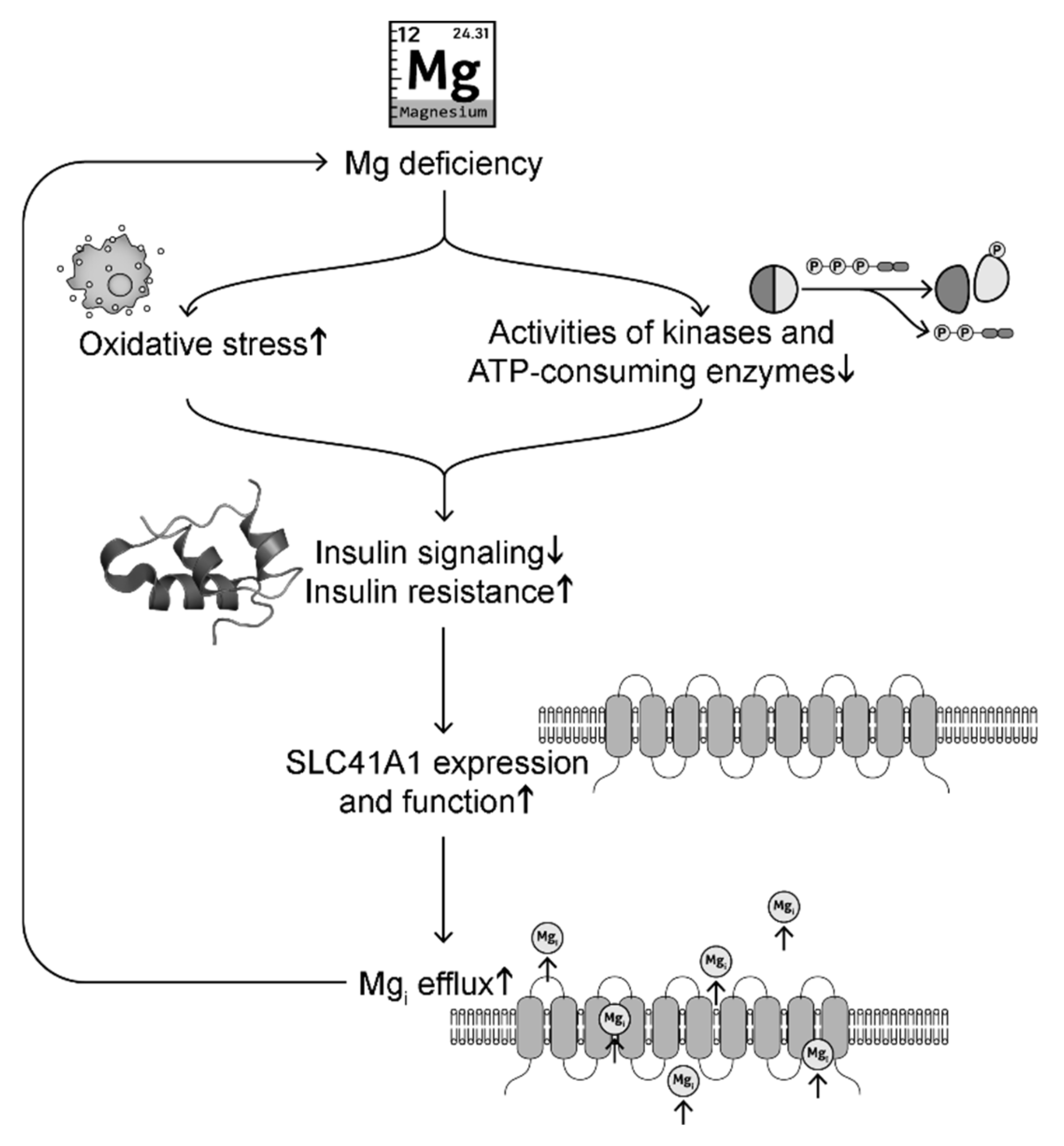{kind=link}
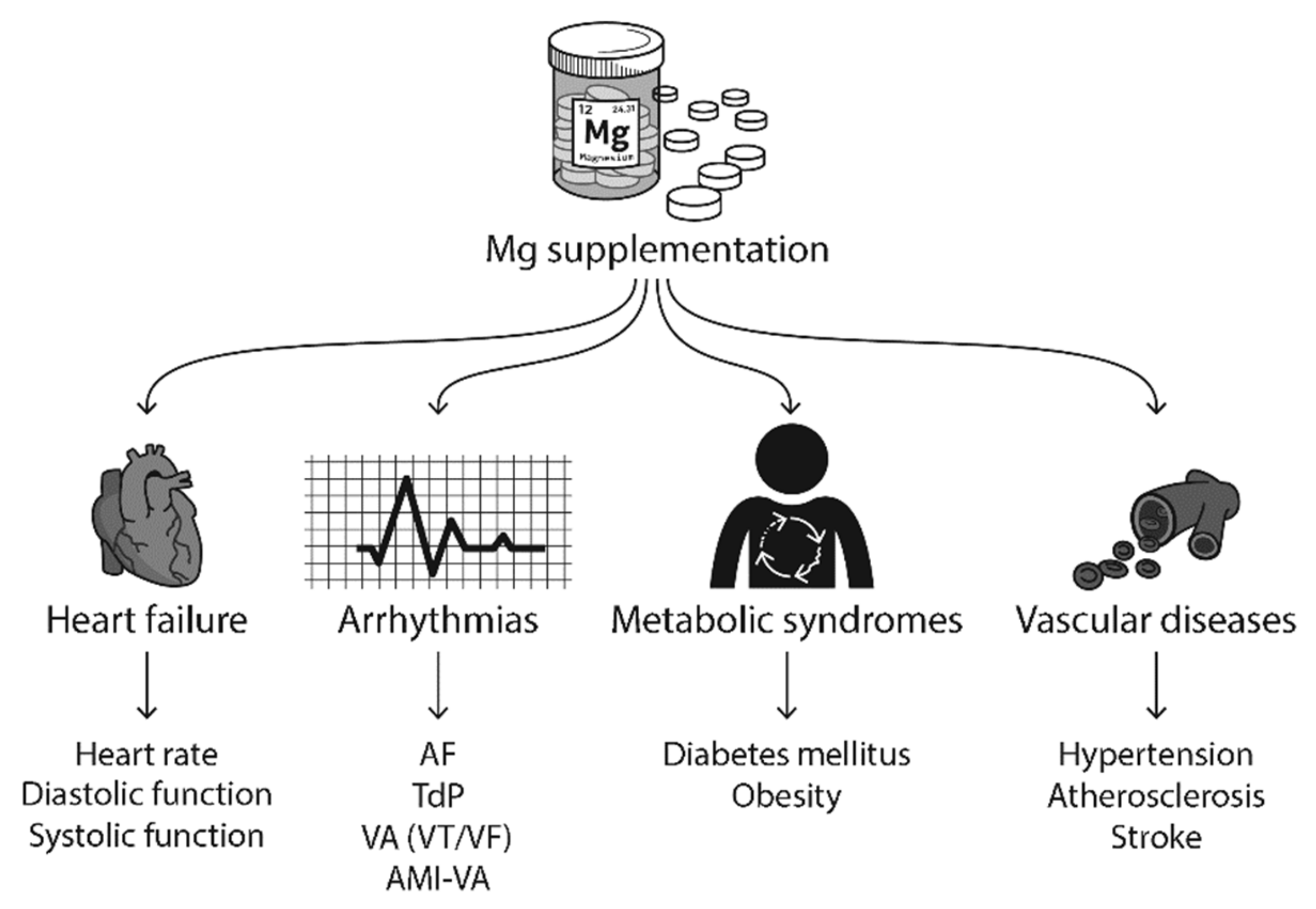{kind=link}
| Increased Inflammatory Markers | Tested Targets | Reference |
|---|---|---|
| CRP | Human HF | [140] |
| Postmenopausal women | [146] | |
| MCP-1 | Human carotid artery stenosis | [141] |
| Human dermal microvascular cells | [144] | |
| Mouse hearts | Our unpublished work | |
| substance P | Rats | [147,148] |
| Rats with cardiomyopathic lesions | [149] | |
| Mouse megakaryocytes and lymphocytes | [66] | |
| IL-1 | Human umbilical vein endothelial cells | [136] |
| Mouse osteoclasts | [66] | |
| Hamsters and rats with cardiac lesions | [134] | |
| Rat bone cells | [148] | |
| IL-6 | Postmenopausal women | [146] |
| Aging rats with CVD | [142,143] | |
| Hamsters and rats with cardiac lesions | [134] | |
| IL-8 | Human dermal microvascular cells | [144] |
| Hamsters and rats with cardiac lesions | [134] | |
| TNF-α | Type 2 diabetes patients | [150] |
| Postmenopausal women | [146] | |
| Aging rats with CVD | [142,143] | |
| Hamsters and rats with cardiac lesions | [134] | |
| Rat bone cells | [148] | |
| Mouse osteoclasts | [66] | |
| elevated cytokines, leukocyte and macrophage activation | Rats | [93,135] |
| Salts | Route | Dose | Treatment Duration | Treating Diseases | Serum Mg (mmol/L) | Reference | |
|---|---|---|---|---|---|---|---|
| Before Treatment | After Treatment | ||||||
| MgSO4 | Oral IV | 5.9 mmol/day MgCO3 22 mmol/h | 8 days 12 h on day 9 | NYHA II-IV HF-VA | 0.66 ± 0.14 | 0.74 ± 0.13 | [10] |
| IV | 0.1 mmol/h | 1 h | NYHA II-IV HF-VA | 0.74 ± 0.0 | 1.15 ± 0.16 | [196] | |
| IV | 1.67 mmol/h | 24 h | NYHA II-III HF-QT variability, ischemic HF | 0.85 ± 0.02 1 | 1.09 ± 0.07 1 | [194] | |
| IV | 1st bolus 30 mmol/h 2nd bolus 5 mmol/h | 20 min 2 h | AF | 0.85 ± 0.10 | NA | [207] | |
| IV | 1st bolus 66 mmol/h 2nd bolus 11 mmol/h | 15 min 6 h | New-onset AF | 1.1 ± 0.4 1 | NA | [296] | |
| IV | 0.15 mmol/kg BW 0.10 mmol/kg BW | 10 min 10 h | Chronic AF | 0.90 ± 0.09 | 1.62 ± 0.29 | [297] | |
| IV | 12–40 mmol total | 20 min–24 h | Acute onset AF | normal | NA | [203] | |
| IV | 24 mmol/h | 20 min, twice in 6 h for 3 days | Postoperative AT | 0.85 ± 0.08 | 0.95 ± 0.09 | [198] | |
| IV | 2.7 mmol/h | 24 h | AMI-VA and mortality | 0.80 ± 0.01 1 | 1.51 ± 0.03 1 | [219] | |
| IV | 2.8 mmol/h | 24 h | AMI-VT | 0.8 ± 0.2 | 1.0 ± 0.1 | [298] | |
| IV | 3.8 mmol/h | 48 h | AMI-HF and mortality | NA | NA | [221] | |
| IV | 60 mmol/h | 20 min | AMI-VA | 0.92 ± 0.02 1 | 1.07 ± 0.02 1 | [220] | |
| IV | 1st 48 mmol/h, 2nd 2.6 mmol/h | 10 min 24 h | AMI-VA | 0.78 (0.61–0.93) 2 | 1.30 (1.11–1.74) 2 | [224] | |
| IV | 1st 96 mmol/h 2nd 2.7 mmol/h | 5 min 24 h | AMI-HF and mortality | 0.80 ± 0.10 | 1.55 ± 0.10 1.80 ± 0.15 | [192] | |
| IV | 1.5–10 mmol/h | 1.7–11.1 h | TdP | 0.94 ± 0.08 | 1.56 ± 0.43 | [200] | |
| IV | 25 mmol/h 15 mmol/h | 2 h 1.5 h, twice a day for 3–4 days | TdP | 0.98 ± 0.11 | 1.08 ± 0.08 | [41] | |
| IV | 1st day 20 mmol/h then 5 mmol/h | ~50 min 50 min, once a day for 3–4 days | TdP | normal | NA | [299] | |
| IV | 33 mmol/h 1.5 mmol/h | 30 min 24 h | VT | NA | NA | [300] | |
| IV | 0.21–0.42 mmol/kg BW | intraoperation | Postoperative arrhythmias | NA | NA | [199] | |
| MgCl2 | Oral | 15.8 mmol/day | 6 w | NYHA II-IV HF-VA | 0.87 ± 0.05 | 0.92 ± 0.05 | [195] |
| IV | 1st bolus 5 mmol/h 2nd bolus 1.1 mmol/h 3rd bolus 0.5 mmol/h | 6 h 18 h 24 h | AMI-VA and mortality | 0.75 (0.56–0.98) 2 | 1.23 (0.77–2.27) 2 | [218] | |
| IV | 72 mmol/h | 10 min | SVA | 0.78 ± 0.03 1 | 1.52 ± 0.08 1 | [301] | |
| IV | 42 mmol/h | 30 min | Postoperative VA | 0.82 ± 0.02 | NA | [302] | |
| IV | 1 mmol/h | 48 h | Postoperative SVA | 0.82 ± 0.05 | 1.20 ± 0.25 | [303] | |
| Mg oxide | Oral | 9.9 mmol/day | 12 w | AF | 0.87 ± 0.06 | 0.90 ± 0.06 | [47] |
| Mg citrate | Oral | 1.4 mmol/day | 5 w | HF – heart rate variation | 0.78 ± 0.04 | 0.89 ± 0.06 | [57] |
| Mg gluconate | Oral | 7.2 mmol/day | ~10 w | Pregnancy-induced hypertension | NA | NA | [304] |
| Mg glutamate | IV | 2.6 mmol | twice | TdP | 0.79 ± 0.10 | 1.87 ± 0.50 | [305] |
| Mg-DL-hydrogen-aspartate | Oral | 6 mmol/day | 3 w | VA | 0.85 ± 0.03 | 0.88 ± 0.04 | [46] |
| Mg L-lactate | Oral | 21 mmol/day | 12–24 w | Hypertension of ICD patients | 0.91 ± 0.08 | 0.99 ± 0.08 | [295] |
| Mg orotate | Oral | 1.00 ± 0.04 mmol/day | 1 year | NYHY IV HF-survival and symptoms | NA | NA | [197] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, M.; Dudley, S.C., Jr. Magnesium, Oxidative Stress, Inflammation, and Cardiovascular Disease. Antioxidants 2020, 9, 907. https://doi.org/10.3390/antiox9100907
Liu M, Dudley SC Jr. Magnesium, Oxidative Stress, Inflammation, and Cardiovascular Disease. Antioxidants. 2020; 9(10):907. https://doi.org/10.3390/antiox9100907
Chicago/Turabian StyleLiu, Man, and Samuel C. Dudley, Jr. 2020. "Magnesium, Oxidative Stress, Inflammation, and Cardiovascular Disease" Antioxidants 9, no. 10: 907. https://doi.org/10.3390/antiox9100907
APA StyleLiu, M., & Dudley, S. C., Jr. (2020). Magnesium, Oxidative Stress, Inflammation, and Cardiovascular Disease. Antioxidants, 9(10), 907. https://doi.org/10.3390/antiox9100907