Serum Paraoxonase-1-Related Variables and Lipoprotein Profile in Patients with Lung or Head and Neck Cancer: Effect of Radiotherapy


 , , , , ,
, , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
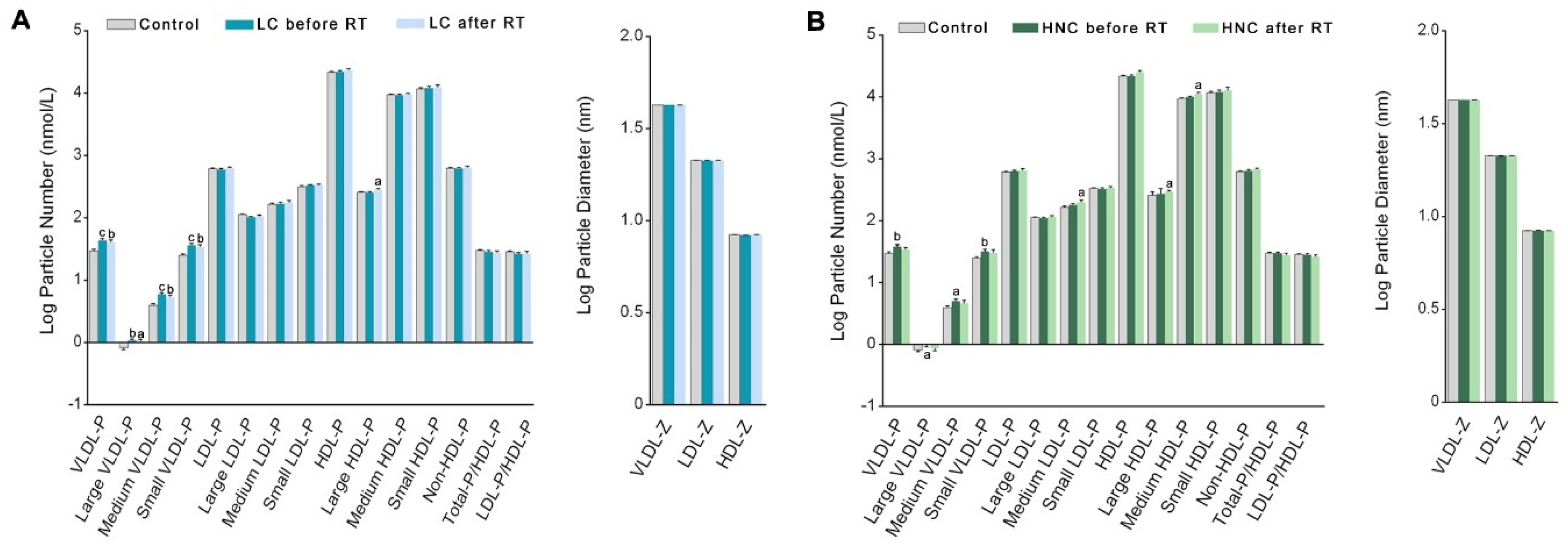
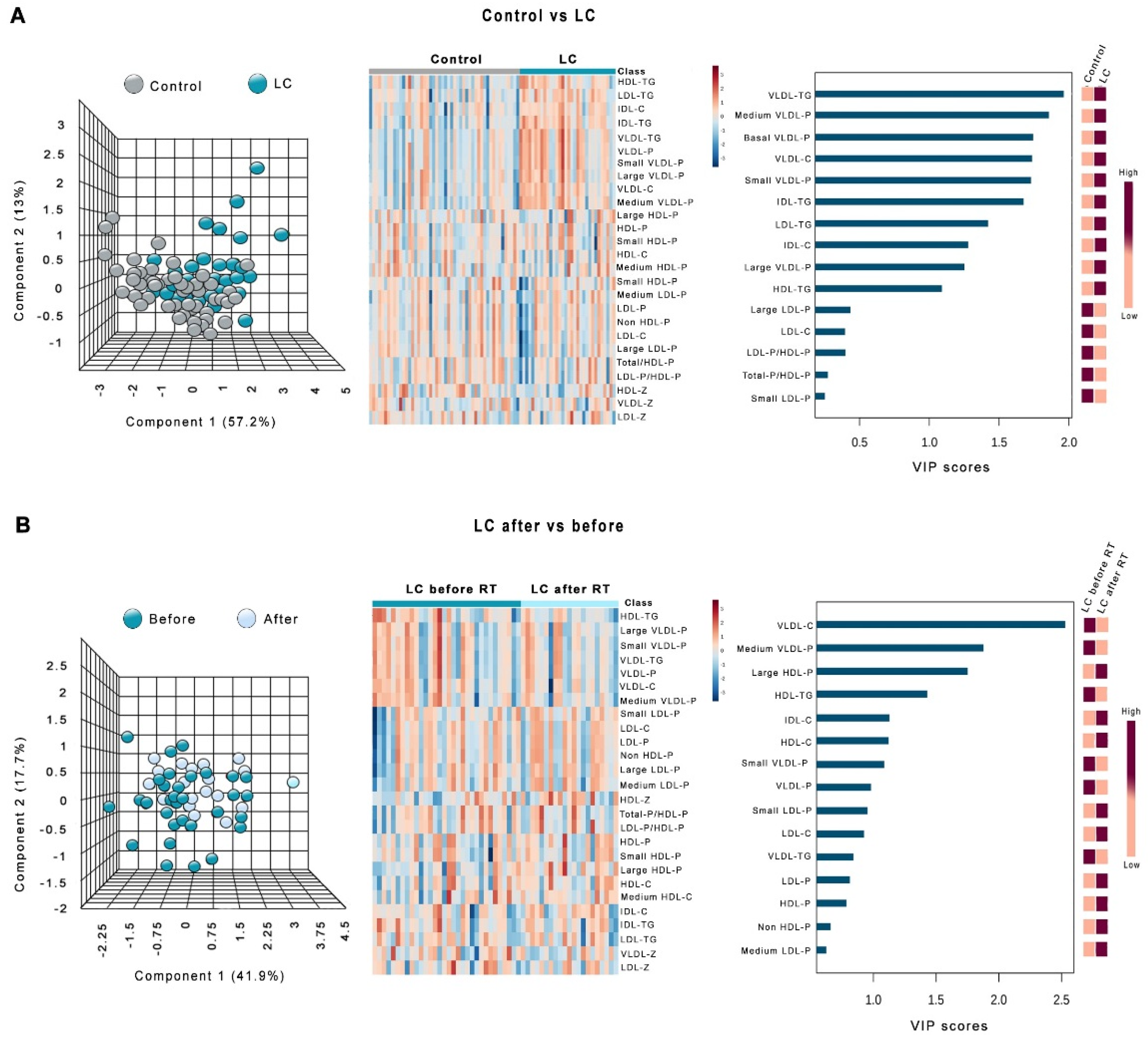
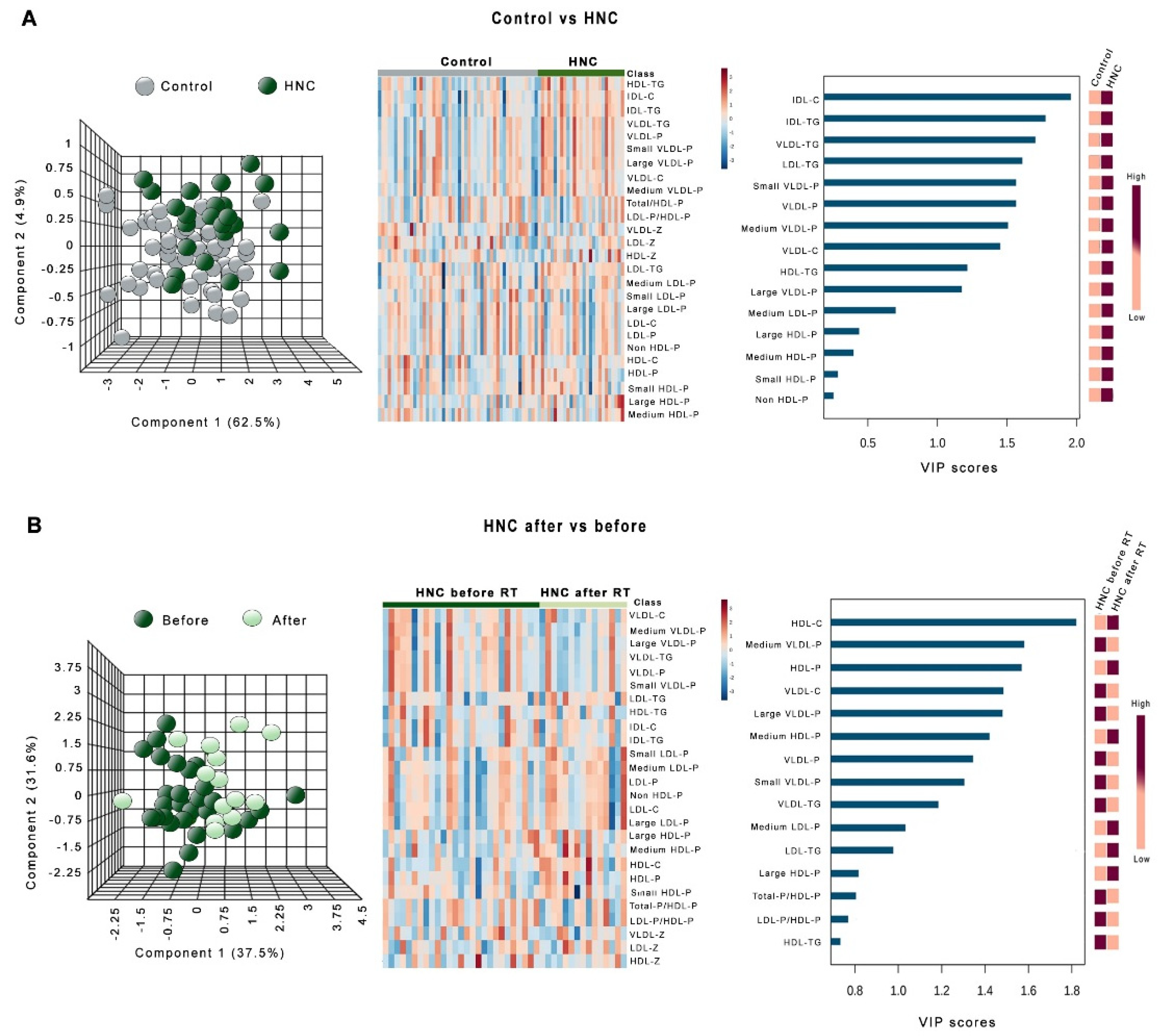
3.1. Changes in PON1-Related Variables and Lipoprotein Profile in Patients with LC or HNC
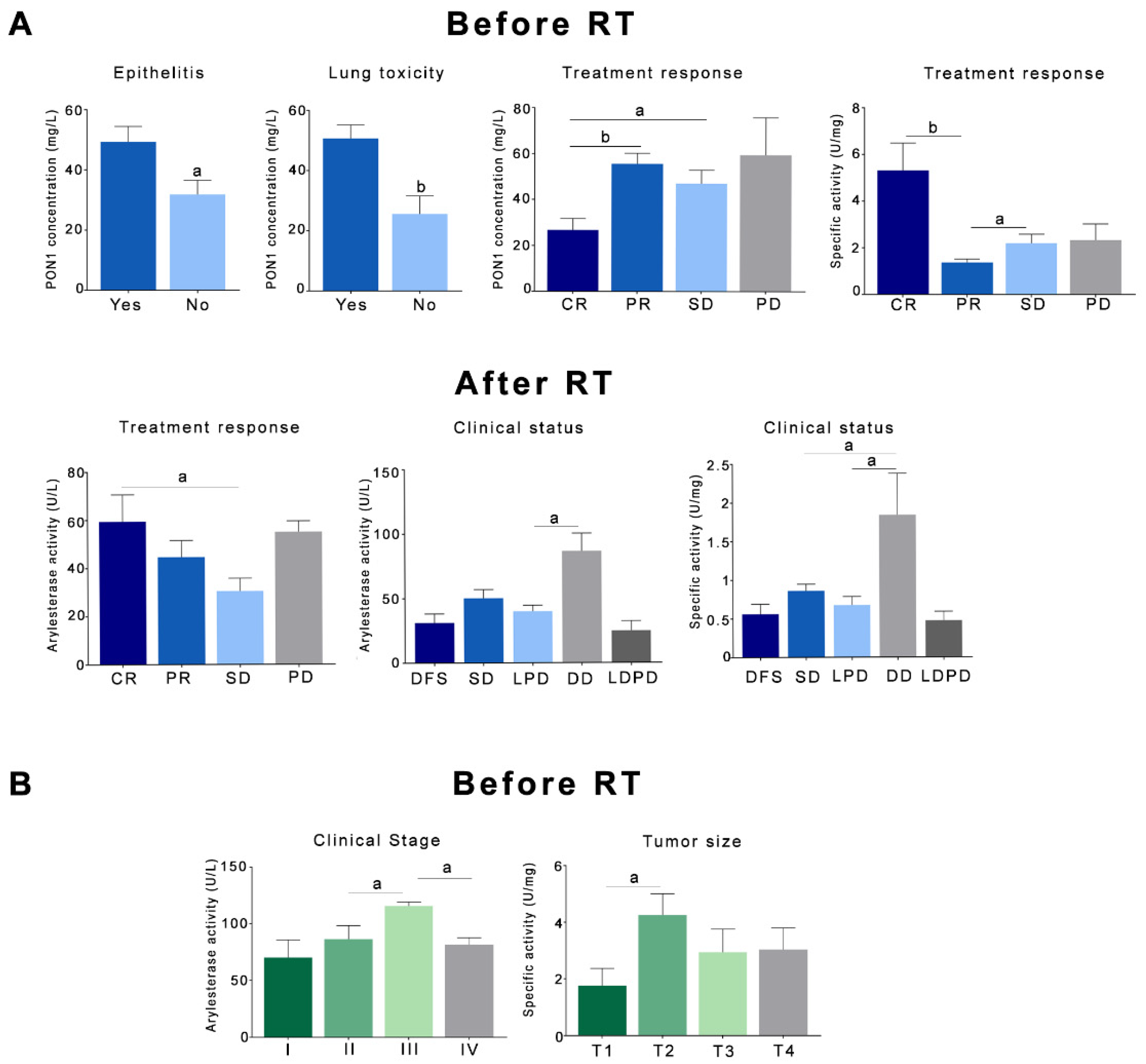
3.2. Relationships Between the Analytical Variables and the Clinical and Pathological Characteristics of the Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dela Cruz, C.S.; Tanoue, L.T.; Matthay, R.A. Lung cancer: Epidemiology, etiology, and prevention. Clin. Chest Med. 2011, 32, 605–644. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.; Fedewa, S.; Chen, A.Y. Epidemiology and demographics of the head and neck cancer population. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 381–395. [Google Scholar] [CrossRef] [PubMed]
- Elkiran, E.T.; Mar, N.; Aygen, B.; Gursu, F.; Karaoglu, A.; Koca, S. Serum paraoxonase and arylesterase activities in patients with lung cancer in a Turkish population. BMC Cancer 2007, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Barrera, G. Oxidative stress and lipid peroxidation products in cancer progression and therapy. ISRN Oncol. 2012, 2012, 137289. [Google Scholar] [CrossRef] [PubMed]
- Aviram, M.; Rosenblat, M. Paraoxonases 1, 2, and 3, oxidative stress, and macrophage cell formation during atherosclerosis development. Free Radic. Biol. Med. 2004, 37, 1304–1316. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Marsillach, J.; Joven, J. The paraoxonases: Role in human diseases and methodological difficulties in measurement. Crit. Rev. Clin. Lab. Sci. 2009, 46, 83–106. [Google Scholar] [CrossRef] [PubMed]
- Khersonsky, O.; Tawfik, D. Structure-reactivity studies of serum paraoxonase PON1 suggest that its native activity is lactonase. Biochemistry 2005, 44, 6371–6382. [Google Scholar] [CrossRef] [PubMed]
- Ponce-Ruiz, N.; Murillo-González, F.E.; Rojas-García, A.E.; Mackness, M.; Bernal-Hernández, Y.Y.; Barrón-Vivanco, B.S.; González-Arias, C.A.; Medina-Díaz, I.M. Transcriptional regulation of human paraoxonase 1 by nuclear receptors. Chem. Biol. Interact. 2017, 268, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, M.; Korkmaz, M.H.; Simsek, E.; Terzi, E.; Oz Bedir, B.E.; Uysal, T.K.; Bayir, O.; Saylam, G.; Guler, O.O. Do CO(2) and oxidative stress induce cancer?: A brief study about the evaluation of PON 1, CAT, CA and XO enzyme levels on head and neck cancer patients. J. Enzyme Inhib. Med. Chem. 2019, 34, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.R.; Barone-Adesi, F.; Koutros, S.; Lerro, C.C.; Blair, A.; Lubin, J.; Heltshe, S.L.; Hoppin, J.A.; Alavanja, M.C.; Beane Freeman, L.E. Incidence of solid tumours among pesticide applicators exposed to the organophosphate insecticide diazinon in the Agricultural Health Study: An updated analysis. Occup. Environ. Med. 2015, 72, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Chi, P.D.; Liu, W.; Chen, H.; Zhang, J.P.; Lin, Y.; Zheng, X.; Liu, W.; Dai, S. High-density lipoprotein cholesterol is a favorable prognostic factor and negatively correlated with C-reactive protein level in non-small cell lung carcinoma. PLoS ONE 2014, 9, e91080. [Google Scholar] [CrossRef] [PubMed]
- Mallol, R.; Amigó, N.; Rodríguez, M.A.; Heras, M.; Vinaixa, M.; Plana, N.; Rock, E.; Ribalta, J.; Yanes, O.; Masana, L.; et al. Liposcale: A novel advanced lipoprotein test based on 2D diffusion-ordered 1H NMR spectroscopy. J. Lipid Res. 2015, 56, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Sloan, J.A.; Loprinzi, C.L.; Laurine, J.A.; Novotny, P.J.; Vargas-Chanes, D.; Krook, J.E.; O’Connell, M.J.; Kugler, J.W.; Tirona, M.T.; Kardinal, C.G.; et al. A simple stratification factor prognostic for survival in advanced cancer: The good/bad/uncertain index. J. Clin. Oncol. 2001, 9, 3539–3546. [Google Scholar] [CrossRef] [PubMed]
- Bots, W.T.; van den Bosch, S.; Zwijnenburg, E.M.; Dijkema, T.; van den Broek, G.B.; Weijs, W.L.J.; Verhoef, L.C.G.; Kaanders, J.H. Reirradiation of head and neck cancer: Long-term disease control and toxicity. Head Neck 2017, 39, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Aranda, N.; Viteri, F.E.; Montserrat, C.; Arija, V. Effects of C282Y, H63D, and S65C HFE gene mutations, diet, and life-style factors on iron status in a general Mediterranean population from Tarragona, Spain. Ann. Hematol. 2010, 89, 767–773. [Google Scholar] [CrossRef]
- Gaita, L.; Manzi, B.; Sacco, R.; Lintas, C.; Altieri, L.; Lombardi, F.; Pawlowski, T.L.; Redman, M.; Craig, D.W.; Huentelman, M.J.; et al. Decreased serum arylesterase activity in autism spectrum disorders. Psychiatry Res. 2010, 180, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.T.; Wadleigh, D.J.; Grijalva, V.; Ng, C.; Hama, S.; Gangopadhyay, A.; Shih, D.M.; Lusis, A.J.; Navab, M.; Fogelman, A.M. Human paraoxonase-3 is an HDL-associated enzyme with biological activity similar to paraoxonase-1 protein but is not regulated by oxidized lipids. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 542–547. [Google Scholar] [CrossRef]
- Jeyarajah, E.J.; Cromwell, W.C.; Otvos, J.D. Lipoprotein particle analysis by nuclear magnetic resonance spectroscopy. Clin. Lab. Med. 2006, 26, 847–870. [Google Scholar] [CrossRef]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristics (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar]
- Grootveld, M. Introduction to the applications of chemometric techniques in ‘Omics’ research: Common pitfalls, misconceptions and ‘rights and wrongs’. In Metabolic Profiling: Disease and Xenobiotics; Grootveld, M., Ed.; Royal Society of Chemistry: Cambridge, UK, 2014; pp. 1–34. [Google Scholar]
- Krzystek-Korpacka, M.; Boehm, D.; Matusiewicz, M.; Diakowska, D.; Grabowski, K.; Gamian, A. Paraoxonase 1 (PON1) status in gastroesophageal malignancies and associated paraneoplastic syndromes- connection with inflammation. Clin. Biochem. 2008, 41, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Karaman, E.; Uzun, H.; Papila, I.; Balci, H.; Ozdilek, A.; Genc, H.; Yanardag, H.; Papila, C. Serum paraoxonase activity and oxidative DNA damage in patients with laryngeal squamous cell carcinoma. J. Craniofac. Surg. 2010, 21, 1745–1749. [Google Scholar] [CrossRef] [PubMed]
- Balci, H.; Genc, H.; Papila, C.; Can, G.; Papila, B.; Yanardag, H.; Uzun, H. Serum lipid hydroperoxide levels and paraoxonase activity in patients with lung, breast, and colorectal cancer. J. Clin. Lab. Anal. 2012, 26, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.M.; Sung, H.J.; Yoon, Y.H.; Kim, B.G.; Yang, W.S.; Lee, C.; Park, H.M.; Kim, B.J.; Kim, B.G.; Lee, S.Y.; et al. Integrated glycoproteomics demonstrates fucosylated serum paraoxonase 1 alterations in small cell lung cancer. Mol. Cell. Proteom. 2014, 13, 30–48. [Google Scholar] [CrossRef] [PubMed]
- Arenas, M.; Rodríguez, E.; Sahebkar, A.; Sabater, S.; Rizo, D.; Pallisé, O.; Hernández, M.; Riu, F.; Camps, J.; Joven, J. Paraoxonase-1 activity in patients with cancer: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2018, 127, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Marsillach, J.; Mackness, B.; Mackness, M.; Riu, F.; Beltrán, R.; Joven, J.; Camps, J. Immunohistochemical analysis of paraoxonases-1, 2, and 3 expression in normal mouse tissues. Free Radic. Biol. Med. 2008, 45, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, L.; Hernandez, A.F.; Lopez-Caballero, J.J.; Gil, F.; Pla, A. Immunohistochemical evidence for the expression and induction of paraoxonase in rat liver, kidney, lung and brain tissue. Implications for its physiological role. Chem. Biol. Interact. 2001, 137, 123–137. [Google Scholar] [CrossRef]
- Eom, S.Y.; Yim, D.H.; Lee, C.H.; Choe, K.H.; An, J.Y.; Lee, K.Y.; Kim, Y.D.; Kim, H. Interactions between paraoxonase 1 genetic polymorphisms and smoking and their effects on oxidative stress and lung cancer risk in a Korean population. PLoS ONE 2015, 10, e0119100. [Google Scholar] [CrossRef]
- Aviram, M.; Rosenblat, M.; Billecke, S.; Erogul, J.; Sorenson, R.; Bisgaier, C.L.; Newton, R.S.; La Du, B. Human serum paraoxonase (PON 1) is inactivated by oxidized low density lipoprotein and preserved by antioxidants. Free Radic. Biol. Med. 1999, 26, 892–904. [Google Scholar] [CrossRef]
- Arenas, M.; García-Heredia, A.; Cabré, N.; Luciano-Mateo, F.; Hernández-Aguilera, A.; Sabater, S.; Bonet, M.; Gascón, M.; Fernández-Arroyo, S.; Fort-Gallifa, I.; et al. Effect of radiotherapy on activity and concentration of serum paraoxonase-1 in breast cancer patients. PLoS ONE 2017, 27, e0188633. [Google Scholar] [CrossRef]
- Camps, J.; García-Heredia, A.; Hernández-Aguilera, A.; Joven, J. Paraoxonases, mitochondrial dysfunction and non-communicable diseases. Chem. Biol. Interact. 2016, 259, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Marsillach, J.; Camps, J.; Ferré, N.; Beltran, R.; Rull, A.; Mackness, B.; Mackness, M.; Joven, J. Paraoxonase-1 is related to inflammation, fibrosis and PPAR delta in experimental liver disease. BMC Gastroenterol. 2009, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.M.; Carmella, S.G.; Wang, R.; Tan, Y.T.; Adams-Haduch, J.; Gao, Y.T.; Hecht, S.S. Relationship of the oxidative damage biomarker 8-epi-prostaglandin F2α to risk of lung cancer development in the Shanghai Cohort Study. Carcinogenesis 2018, 39, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Şahin, F.; Aslan, A.F. Relationship between inflammatory and biological markers and lung cancer. J. Clin. Med. 2018, 7, 160. [Google Scholar] [CrossRef] [PubMed]
- Chawda, J.G.; Jain, S.S.; Patel, H.R.; Chaduvula, N.; Patel, K. The relationship between serum lipid levels and the risk of oral cancer. Indian J. Med. Paediatr. Oncol. 2011, 32, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Rai, P.; Hallikeri, K.; Anehosur, V.; Kale, J. Serum lipid profile in oral squamous cell carcinoma: Alterations and association with some clinicopathological parameters and tobacco use. Int. J. Oral Maxillofac. Surg. 2016, 45, 713–720. [Google Scholar] [CrossRef]
- Lin, X.; Lu, L.; Liu, L.; Wei, S.; He, Y.; Chang, J.; Lian, X. Blood lipids profile and lung cancer risk in a meta-analysis of prospective cohort studies. J. Clin. Lipidol. 2017, 11, 1073–1081. [Google Scholar] [CrossRef]
- Carreras-Torres, R.; Johansson, M.; Haycock, P.C.; Wade, K.H.; Relton, C.L.; Martin, R.M.; Davey Smith, G.; Albanes, D.; Aldrich, M.C.; Andrew, A.; et al. Obesity, metabolic factors and risk of different histological types of lung cancer: A Mendelian randomization study. PLoS ONE 2017, 12, e0177875. [Google Scholar] [CrossRef]
- Hao, B.; Yu, M.; Sang, C.; Bi, B.; Chen, J. Dyslipidemia and non-small cell lung cancer risk in Chinese population: A case-control study. Lipids Health Dis. 2018, 17, 278. [Google Scholar] [CrossRef]
- Lyu, Z.; Li, N.; Wang, G.; Feng, X.; Chen, S.; Su, K.; Li, F.; Wei, L.; Li, X.; Xie, S.; et al. Independent and joint associations of blood lipids and lipoproteins with lung cancer risk in Chinese males: A prospective cohort study. Int. J. Cancer 2019, 144, 2972–2984. [Google Scholar] [CrossRef]
- Sproull, M.; Kramp, T.; Tandle, A.; Shankavaram, U.; Camphausen, K. Serum amyloid A as a biomarker for radiation exposure. Radiat. Res. 2015, 184, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Sproull, M.; Kramp, T.; Tandle, A.; Shankavaram, U.; Camphausen, K. Multivariate analysis of radiation responsive proteins to predict radiation exposure in total-body irradiation and partial-body irradiation models. Radiat. Res. 2017, 187, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.S.; Chang, H.J.; Chang, Y.C.; Huang, S.C.; Ko, H.L.; Chang, C.C.; Yeh, Y.W.; Jiang, J.S.; Lee, C.Y.; Chi, M.S.; et al. Serum amyloid a as a predictive marker for radiation pneumonitis in lung cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Feurgard, C.; Bayle, D.; Guézingar, F.; Sérougne, C.; Mazur, A.; Lutton, C.; Aigueperse, J.; Gourmelon, P.; Mathé, D. Effects of ionizing radiation (neutrons/gamma rays) on plasma lipids and lipoproteins in rats. Radiat. Res. 1998, 150, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Ossetrova, N.I.; Stanton, P.; Krasnopolsky, K.; Ismail, M.; Doreswamy, A.; Hieber, K.P. Biomarkers for radiation biodosimetry and injury assessment after mixed-field (neutron and gamma) radiation in the mouse total-body irradiation model. Health Phys. 2018, 115, 727–742. [Google Scholar] [CrossRef]
- Sehitogulları, A.; Aslan, M.; Sayır, F.; Kahraman, A.; Demir, H. Serum paraoxonase-1 enzyme activities and oxidative stress levels in patients with esophageal squamous cell carcinoma. Redox Rep. 2014, 19, 199–205. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical and Demographic Characteristics | Control Group n = 50 | Lung Cancer n = 33 | Head and Neck Cancer n = 28 | p-Value * |
|---|---|---|---|---|
| Age, years | 42 (35–47) | 72 (65–79) | 65 (56–73) | <0.001 |
| Male sex, n (%) | 25 (50.0) | 26 (78.8) | 25 (89.3) | <0.001 |
| Alcohol habit (>20 g/day), n (%) | 15 (30.0) | 8 (24.2) | 11 (39.3) | 0.042 |
| Smoking, n (%) Current smoker Former smoker | 17 (34.0) 0 (0.0) | 14 (42.4) 17 (51.5) | 16 (57.1) 6 (21.4) | <0.001 |
| Hypertension, n (%) | 4 (8.0) | 19 (57.6) | 17 (60.7) | <0.001 |
| Type 2 diabetes mellitus, n (%) | 5 (10.0) | 10 (30.3) | 6 (21.4) | 0.085 |
| Cancer stage, n (%) | ||||
| Stage I | − | 14 (42.4) | 5 (17.9) | − |
| Stage II | − | 4 (12.1) | 5 (17.9) | − |
| Stage III | − | 15 (45.5) | 5 (17.9) | − |
| Stage IV | − | 0 (0.0) | 13 (46.3) | − |
| Histology, n (%) | ||||
| Squamous carcinoma | − | 18 (54.5) | 26 (92.9) | − |
| Adenocarcinoma | − | 13 (39.4) | 1 (3.6) | − |
| Others | − | 2 (6.0) | 1 (3.6) | − |
| Chemotherapy treatment, n (%) | − | 18 (54.5) | 17 (60.7) | − |
| Secondary effects of radiotherapy, n (%) | ||||
| Epithelitis | − | 24 (72.7) | 25 (89.3) | − |
| Lung toxicity | − | 25 (75.8) | − | − |
| Xerostomia | − | − | 22.0 (78.6) | − |
| Mucositis | − | − | 20.0 (71.4) | − |
| Esophagitis | − | − | 6.0 (21.5) | − |
| Model | B | Standard Error | p-Value | Exp (B) | 95% IC for Exp (B) |
|---|---|---|---|---|---|
| Paraoxonase-1 concentration | −0.107 | 0.040 | 0.007 | 0.899 | 0.832–0.971 |
| Age | 0.205 | 0.097 | 0.035 | 1.227 | 1.015–1.484 |
| Sex | −1.362 | 2.238 | 0.543 | 0.256 | 0.003–20.600 |
| Smoking | 4.107 | 1.963 | 0.036 | 60.794 | 1.296–2851.701 |
| Arterial hypertension | 0.321 | 2.753 | 0.907 | 1.378 | 0.006–303.664 |
| Diabetes mellitus | −0.448 | 3.732 | 0.905 | 0.639 | 0.000–960.204 |
| Constant | −5.486 | 6.553 | 0.402 | 0.004 | − |
| Model * | B | Standard Error | p-Value | Exp (B) | 95% IC for Exp (B) |
|---|---|---|---|---|---|
| Arylesterase Activity | −0.037 | 0.013 | 0.005 | 0.964 | 0.939–0.989 |
| Age | 0.144 | 0.071 | 0.042 | 1.154 | 1.005–1.326 |
| Sex | −2.033 | 2.060 | 0.324 | 0.131 | 0.002–7.428 |
| Smoking | 2.845 | 1.600 | 0.075 | 17.199 | 0.747–395.05 |
| Arterial hypertension | 1.605 | 2.841 | 0.572 | 4.977 | 0.019–1304.649 |
| Diabetes mellitus | −1.385 | 2.437 | 0.570 | 0.250 | 0.002–29.732 |
| Constant | −1.365 | 4.227 | 0.747 | 0.255 | − |
| Variable * | Control Group | Lung Cancer Before Radiotherapy | Lung Cancer After Radiotherapy |
|---|---|---|---|
| Hemoglobin (g/dL) | 14.9 (13.9–15.2) | 13.5 (11.0–13.9) c | 12.0 (11.3–13.1) c |
| Platelets (×109/L) | 277.0 (230.5–301.5) | 293.5 (241.0–357.0) | 175.0 (138.5–202.0) c,d |
| Total-cholesterol (mg/dL) | 155.9 (140.2–172.8) | 154.4 (135.6–177.0) | 161.8 (139.9–178.9) |
| VLDL-cholesterol (mg/dL) | 12.1 (8.6–16.7) | 18.0 (13.6–21.7) b | 15.9 (10.3–20.3) |
| IDL-cholesterol (mg/dL) | 7.3 (4.9–9.9) | 8.9 (7.3–10.0) a | 10.0 (7.3–11.2) b |
| LDL-cholesterol (mg/dL) | 89.3 (80.3–100.5) | 88.1 (68.9–99.4) | 92.6 (69.3–106.6) |
| HDL-cholesterol (mg/dL) | 43.4 (38.1–51.8) | 43.6 (34.3–52.1) | 47.1 (38.5–49.3) |
| Total-triglycerides (mg/dL) | 69.3 (49.5–82.2) | 97.3 (77.2–122.9) c | 94.0 (69.7–104.5) c |
| VLDL-triglycerides (mg/dL) | 38.1 (29.4–49.3) | 64.0 (41.1–78.1) c | 60.3 (44.2–69.6) c |
| IDL-triglycerides (mg/dL) | 6.8 (4.9–8.3) | 9.4 (7.7–10.2) c | 9.8 (7.4–11.0) c |
| LDL-triglycerides (mg/dL) | 8.8 (6.5–11.2) | 11.6 (8.6–14.7) b | 11.0 (8.7–14.9) b |
| HDL-triglycerides (mg/dL) | 11.3 (8.7–15.3) | 14.3 (11.8–17.9) b | 13.7 (11.9–14.9) |
| Variable * | Control Group | Head and Neck Cancer Before Radiotherapy | Head and Neck Cancer After Radiotherapy |
|---|---|---|---|
| Hemoglobin (g/dL) | 14.9 (13.9–15.2) | 13.9 (11.8–14.8) | 11.2 (10.3–12.4) c,d |
| Platelets (×109/L) | 277.0 (230.5–301.5) | 208.0 (154.5–327.0) | 195.0 (161.0–277.0) a |
| Total-cholesterol (mg/dL) | 155.9 (140.2–172.8) | 157.8 (140.3–176.0) | 164.9 (151.4–206.5) |
| VLDL-cholesterol (mg/dL) | 12.1 (8.6–16.7) | 14.9 (10.8–19.7) | 12.2 (8.2–17.5) |
| IDL-cholesterol (mg/dL) | 7.3 (4.9–9.9) | 8.5 (6.7–11.8) a | 9.7 (6.6–10.3) |
| LDL-cholesterol (mg/dL) | 89.3 (80.3–100.5) | 93.0 (76.8–100.5) | 99.8 (78.0–110.2) |
| HDL-cholesterol (mg/dL) | 43.4 (38.1–51.8) | 42.6 (38.9–46.6) | 52.1 (44.8–57.2) a |
| Total-triglycerides (mg/dL) | 69.3 (49.5–82.2) | 89.5 (67.8–96.8) b | 78.1 (64.8–88.4) a |
| VLDL-triglycerides (mg/dL) | 38.1 (29.4–49.3) | 54.5 (42.5–62.7) b | 46.3 (33.9–52.0) |
| IDL-triglycerides (mg/dL) | 6.8 (4.9–8.3) | 8.4 (7.5–10.7) b | 8.9 (7.5–9.6) b |
| LDL-triglycerides (mg/dL) | 8.8 (6.5–11.2) | 11.2 (9.3–11.7) a | 12.7 (10.5–14.2) |
| HDL-triglycerides (mg/dL) | 11.3 (8.7–15.3) | 13.1 (11.1–17.6) a | 12.0 (10.6–17.0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Tomàs, E.; Murcia, M.; Arenas, M.; Arguís, M.; Gil, M.; Amigó, N.; Correig, X.; Torres, L.; Sabater, S.; Baiges-Gayà, G.; et al. Serum Paraoxonase-1-Related Variables and Lipoprotein Profile in Patients with Lung or Head and Neck Cancer: Effect of Radiotherapy. Antioxidants 2019, 8, 213. https://doi.org/10.3390/antiox8070213
Rodríguez-Tomàs E, Murcia M, Arenas M, Arguís M, Gil M, Amigó N, Correig X, Torres L, Sabater S, Baiges-Gayà G, et al. Serum Paraoxonase-1-Related Variables and Lipoprotein Profile in Patients with Lung or Head and Neck Cancer: Effect of Radiotherapy. Antioxidants. 2019; 8(7):213. https://doi.org/10.3390/antiox8070213
Chicago/Turabian StyleRodríguez-Tomàs, Elisabet, Mauricio Murcia, Meritxell Arenas, Mònica Arguís, Miriam Gil, Núria Amigó, Xavier Correig, Laura Torres, Sebastià Sabater, Gerard Baiges-Gayà, and et al. 2019. "Serum Paraoxonase-1-Related Variables and Lipoprotein Profile in Patients with Lung or Head and Neck Cancer: Effect of Radiotherapy" Antioxidants 8, no. 7: 213. https://doi.org/10.3390/antiox8070213
APA StyleRodríguez-Tomàs, E., Murcia, M., Arenas, M., Arguís, M., Gil, M., Amigó, N., Correig, X., Torres, L., Sabater, S., Baiges-Gayà, G., Cabré, N., Luciano-Mateo, F., Hernández-Aguilera, A., Fort-Gallifa, I., Camps, J., & Joven, J. (2019). Serum Paraoxonase-1-Related Variables and Lipoprotein Profile in Patients with Lung or Head and Neck Cancer: Effect of Radiotherapy. Antioxidants, 8(7), 213. https://doi.org/10.3390/antiox8070213