Effects of a Two-Year Home-Based Exercise Training Program on Oxidized LDL and HDL Lipids in Coronary Artery Disease Patients with and without Type-2 Diabetes

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
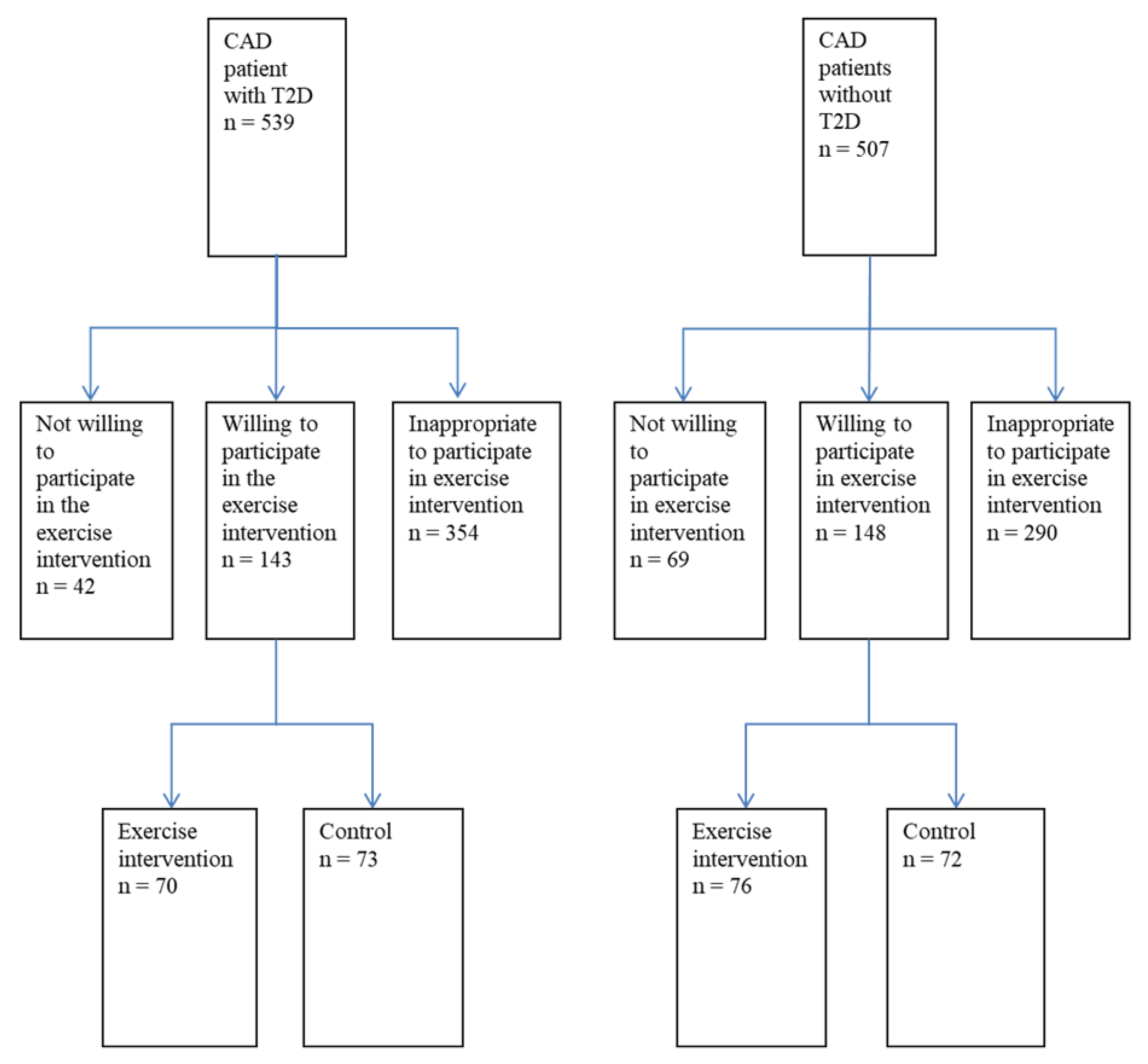
2.1. Subjects and Study Protocol
2.2. Exercise Training Intervention
2.3. Measurement of Leisure-Time Physical Activity (LTPA)
- (1)
- No LTPA (very little physical activity or light housework).
- (2)
- Random LTPA (random light physical activity like walking or cycling).
- (3)
- Moderate LTPA (Engages in physical activity at moderate level 2 to 3 times per week).
- (4)
- Moderate or high LTPA (Engages in physical activity at moderate or high level more than 3 times per week).
2.4. Exercise-Capacity Measurement
2.5. Exercise Training Load
2.6. Measurements of CV Risk Factors
2.7. Determination of Oxidized Lipoprotein Lipids
2.8. Statistical Analysis
3. Results
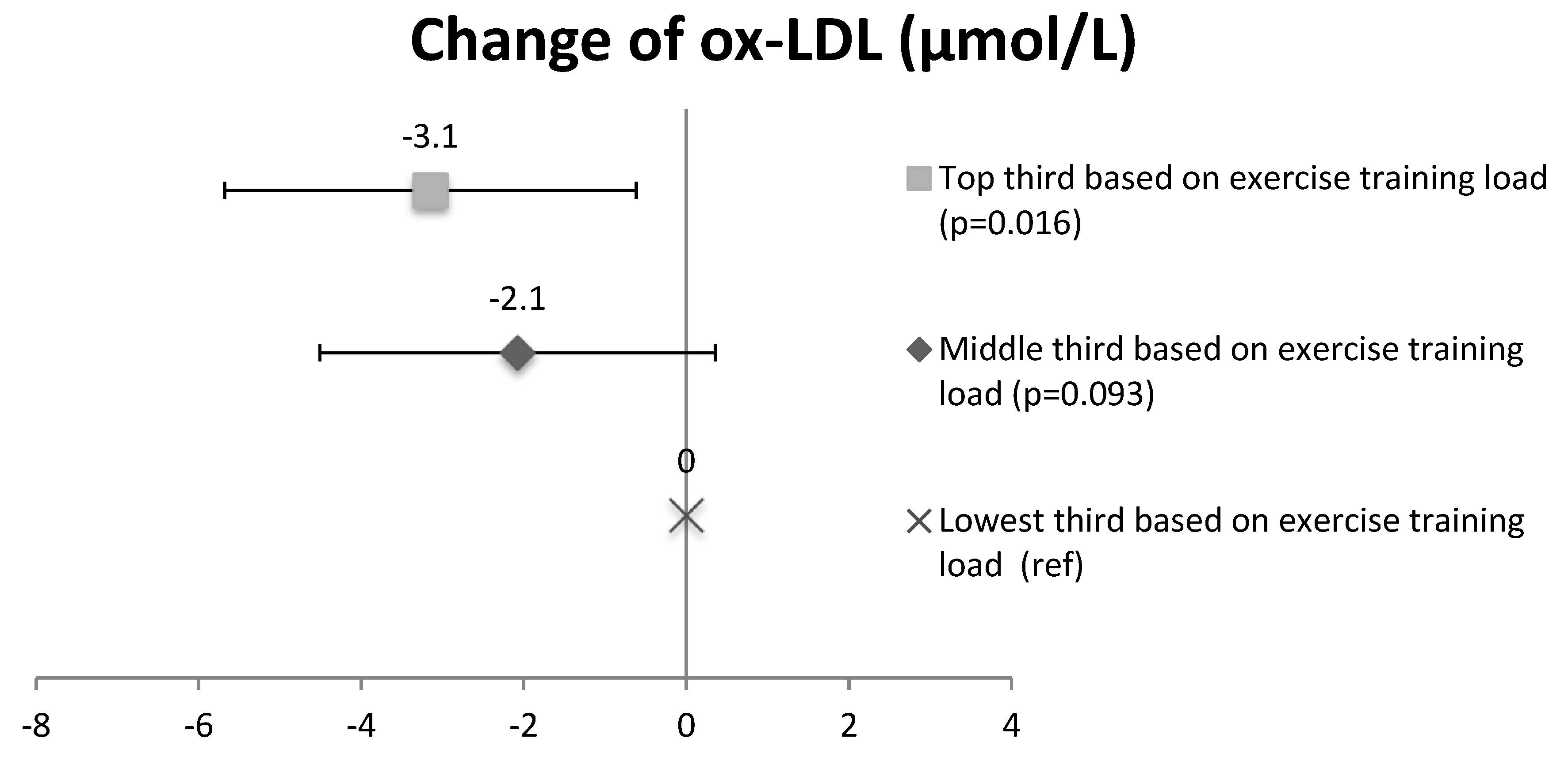
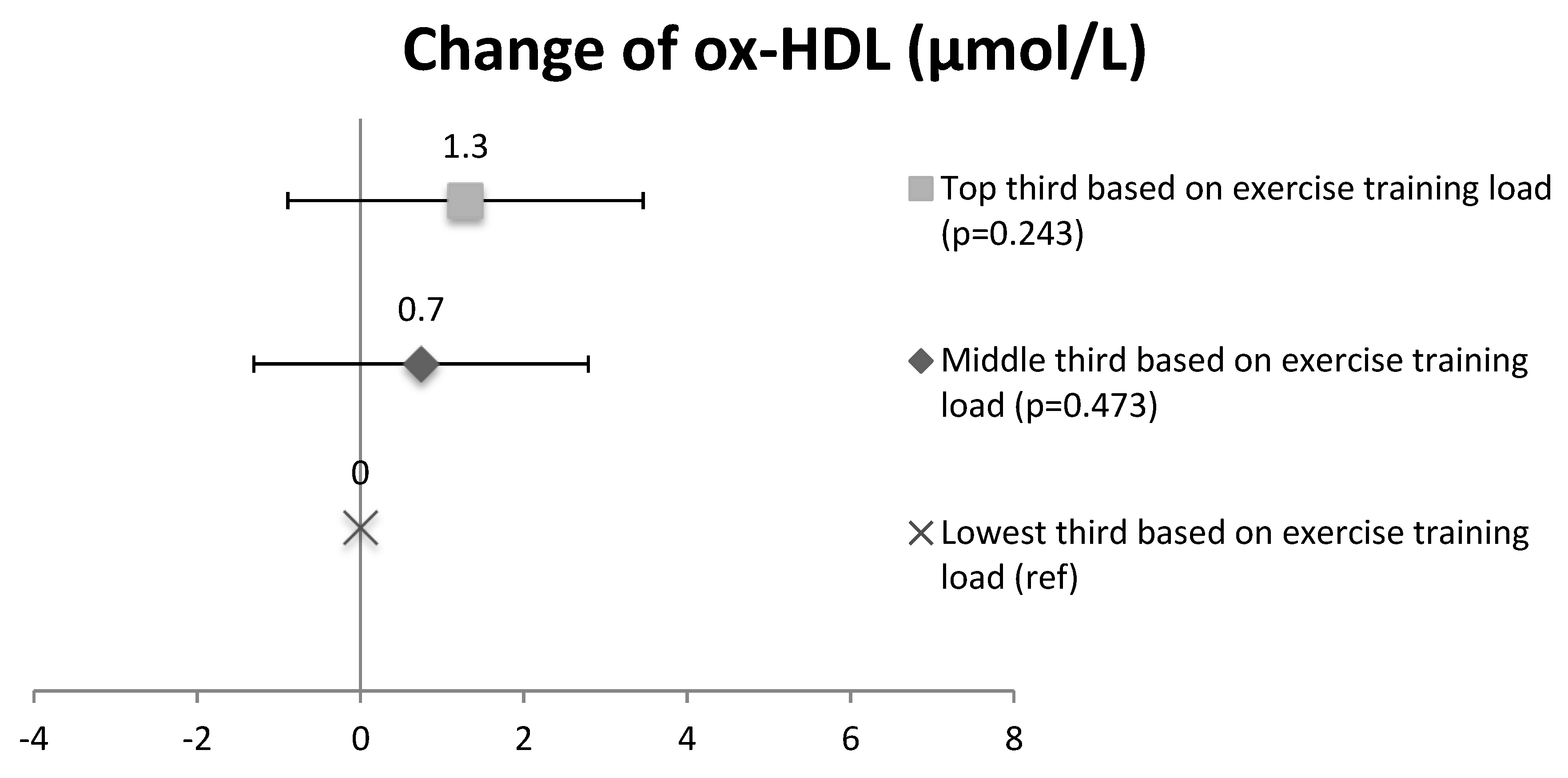
3.1. Ox-LDL and Ox-HDL in Training Load Subgroups
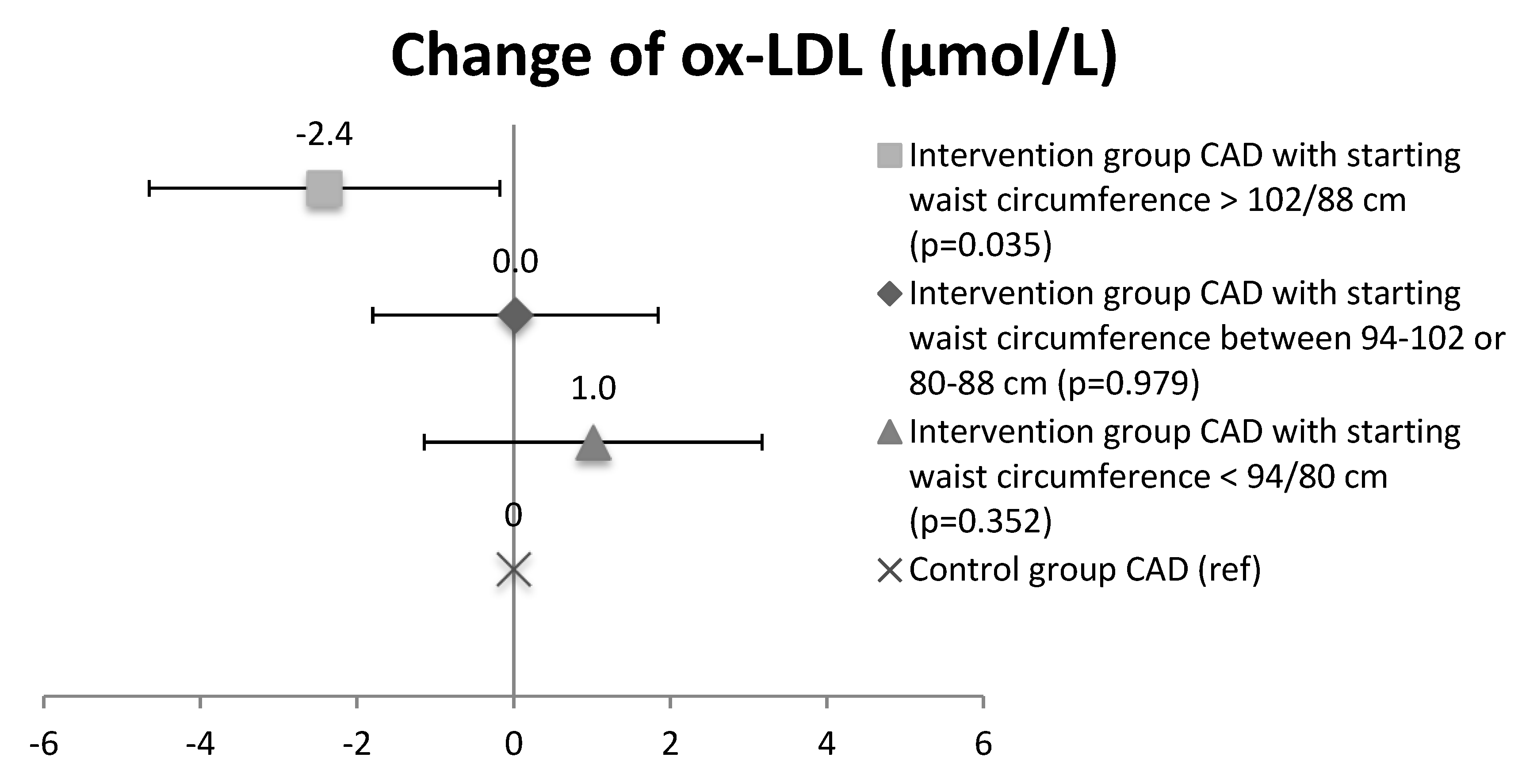
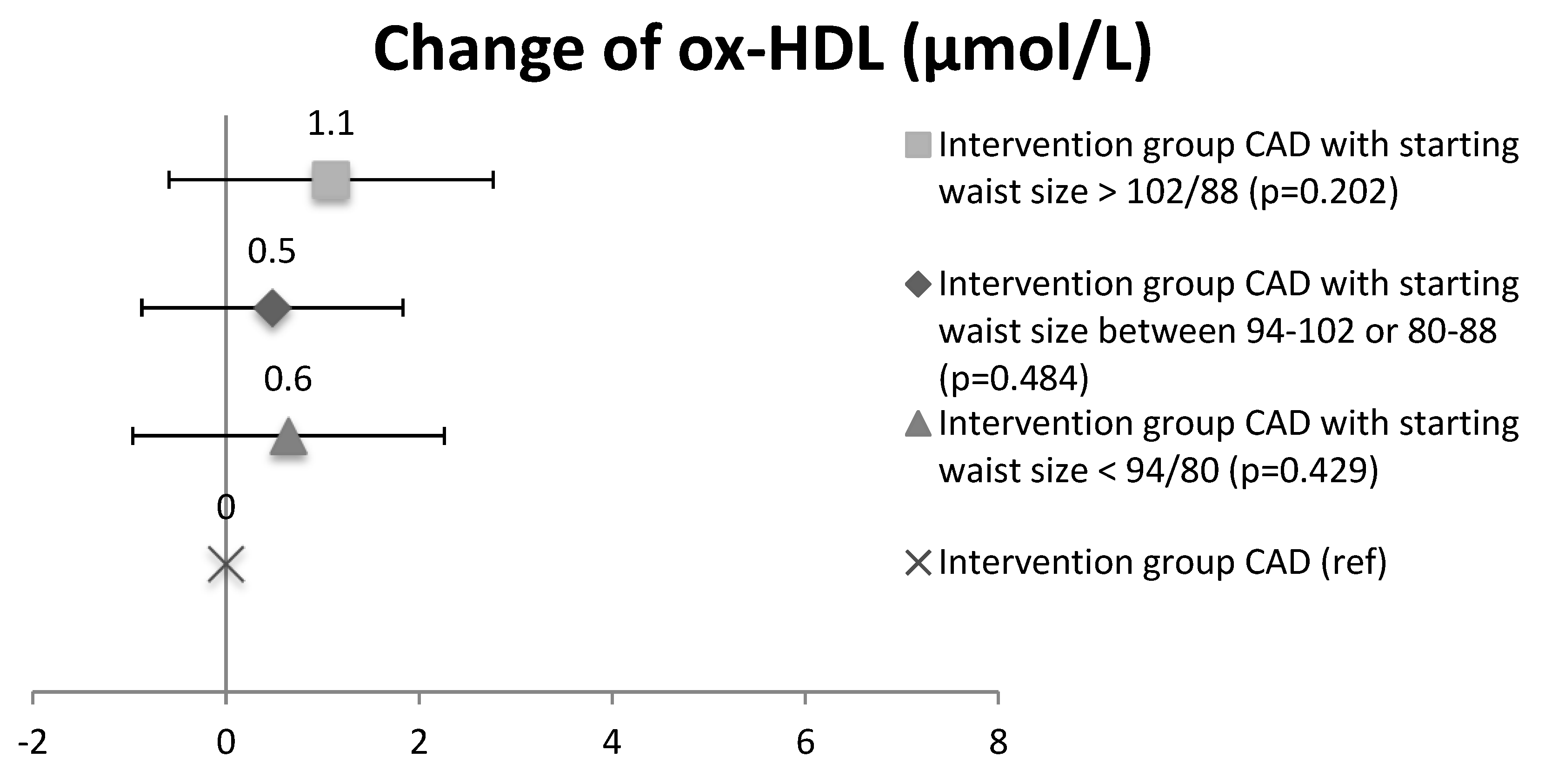
3.2. Ox-LDL and Ox-HDL Lipids in the Intervention Waist Circumference Subgroups
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Diseases Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; Stampfer, M.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [CrossRef] [PubMed]
- Conroy, R.M.; Pyorala, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetiére, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Vasankari, T.; Ahotupa, M.; Toikka, J.; Mikkola, J.; Irjala, K.; Pasanen, P.; Neuvonen, K.; Raitakari, O.; Viikari, J. Oxidized LDL and thickness of carotid intima-media are associated with coronary atherosclerosis in middle-aged men: Lower levels of oxidized LDL with statin therapy. Atherosclerosis 2001, 155, 403–412. [Google Scholar] [CrossRef]
- Raitakari, O.T.; Toikka, J.O.; Laine, H.; Ahotupa, M.; Iida, H.; Viikari, J.; Hartiala, J.; Knuuti, J. Reduced myocardial flow reserve relates to increased carotid intima-media thickness in healthy young men. Atherosclerosis 2001, 156, 469–475. [Google Scholar] [CrossRef]
- Toikka, J.; Niemi, P.; Ahotupa, M.; Niinikoski, H.; Viikari, J.; Rönnemaa, T.; Hartiala, J.; Raitakari, O. Large artery elastic properties in young men: Relationships to serum lipoproteins and oxidized low-density lipoprotein cholesterol. Art. Thromb. Vasc. Biol. 1999, 19, 436–441. [Google Scholar] [CrossRef]
- Linna, M.; Ahotupa, M.; Löppönen, M.; Irjala, K.; Vasankari, T. Circulating oxidized LDL lipids, when proportioned to HDL-c, emerged as a risk factor of all-cause mortality in a population-based survival study. Age Ageing 2013, 42, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Toikka, J.; Laine, H.; Ahotupa, M.; Haapanen, A.; Viikari, J.; Hartiala, J.J.; Raitakari, O. Increased arterial intima-media thickness and in vivo LDL oxidation in young men with borderline hypertension. Hypertension 2000, 36, 929–933. [Google Scholar] [CrossRef] [PubMed]
- Linna, M.; Ahotupa, M.; Irjala, K.; Pöllänen, P.; Huhtaniemi, I.; Mäkinen, J.; Perheentupa, A.; Vasankari, T. Smoking and low serum testosterone associates with high concentration of oxidized LDL. Ann. Med. 2008, 40, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Linna, M.; Borg, P.; Kukkonen-Harjula, K.; Fogelholm, M.; Ahotupa, M.; Vasankari, T. Weight reduction lowers and consecutive weight maintenance preserves reduced risk for atheroclerosis indicated by lower levels of oxidized LDL. Int. J. Obes. 2007, 31, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Kresanov, P.; Ahotupa, M.; Vasankari, T.; Kaikkonen, J.; Kähönen, M.; Lehtimäki, T.; Viikari, J.; Raitakari, O. The associations of oxidized high-density lipoprotein lipids with risk factors for atherosclerosis. The Cardiovascular Risk in Young Finns Study. Free Radic. Biol. Med. 2013, 65, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Balady, G.J.; Williams, M.A.; Ades, P.A.; Bittner, V.; Comoss, P.; Foody, J.M.; Franklin, B.; Sanderson, B.; Southard, D.; American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; et al. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: A Scientific statement from HT American Heart Association Exercise, Cardiac Rehabilitation, And Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation 2007, 115, 2675–2682. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Corra, U.; Benzwr, W.; Bjarnason-Wehrens, B.; Dendale, P.; Gaita, D.; McGee, H.; Mendes, M.; Niebauer, J.; Zwisler, A.D.; et al. Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Secondary prevention through cardiac rehabilitation: From knowledge to implementation. A position paper from Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Buse, J.B.; Ginsberg, H.N.; Bakris, G.L.; Clark, N.G.; Costa, F.; Eckel, R.; Fonseca, V.; Gerstein, H.C.; Grundy, S.; Nesto, R.W.; et al. American Heart Association; American Diabetes Association. Primary prevention of cardiovascular diseases in people with diabetes mellitus: A scientific statement from the American Heart Association and American Diabetes Association. Circulation 2007, 115, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Hill, J.O.; Jacobsen, D.J.; Potteiger, J.; Sullivan, D.K.; Johnson, S.L.; Heelan, K.; Hise, M.; Fennessey, P.V.; Sonko, B.; et al. Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: The Midwest Exercise Trial. Arch. Int. Med. 2003, 163, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Eliakim, A.; Makowski, G.S.; Brasel, J.A.; Cooper, D.M. Adiposity, lipid levels, and brief endurance training in nonobese adolescent males. Int. J. Sports Med. 2000, 21, 327. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Marcus, B.H.; Gallgher, K.I.; Napolitano, M.; Lang, W. Effect of exercise duration and intensity on weight loss in overweight, sedentary women. JAMA 2003, 290, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Kosola, J.; Ahotupa, M.; Kyröläinen, H.; Santtila, M.; Vasankari, T. Both poor cardiorespiratory and weak muscle fitness are related to a high concentration of oxidized low-density lipoprotein lipids. Scand. J. Med. Sci. Sports 2012, 22, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Kosola, J.; Ahotupa, M.; Kyröläinen, H.; Santtila, M.; Vasankari, T. Good aerobic and muscular fitness protects overweight men from elevated oxidized LDL. Med. Sci. Sports Exerc. 2012, 44, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Ahotupa, M.; Suomela, J.P.; Vuorimaa, T.; Vasankari, T. Lipoprotein-specific transport of circulating lipid peroxides. Ann. Med. 2010, 42, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Tiainen, S.; Luoto, R.; Ahotupa, M.; Raitanen, J.; Vasankari, T. 6-mo aerobic exercise intervention enhances the lipid peroxide transport function of HDL. Free Radic. Res. 2016, 50, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, J.J.; Kiviniemi, A.M.; Hautala, A.J.; Piira, O.-P.; Lepojärvi, E.S.; Perkiömäki, J.S.; Junttila, M.J.; Huikuri, H.V.; Tulppo, M.P. Effects of physical activity and exercise training on cardiovascular risk in coronary artery disease patients with and without type 2 diabetes. Diabetes Care 2015, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Saltin, B.; Grimby, G. Physiological analysis of middle-aged and old former athletes. Comparison with still active athletes of the same ages. Circulation 1968, 38, 1104–1115. [Google Scholar] [CrossRef] [PubMed]
- Aires, N.; Selmer, R.; Thelle, D. The validity of self-reported leisure time physical activity, and its relationship to serum cholesterol, blood pressure and body mass index. A population based study of 332,182 men and women aged 40–42 years. Eur. J. Epidemiol. 2003, 18, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Rödjer, L.; Jonsdottir, I.H.; Rosengren, A.; Björck, L.; Grimby, G.; Thelle, D.S.; Lappas, G.; Börjesson, M. Self-reported leisure time physical activity: A useful assessment tool in everyday health care. BMC Public Health 2012, 12, 693. [Google Scholar] [CrossRef] [PubMed]
- Apullan, F.J.; Bourassa, M.G.; Tardif, J.C.; Fortier, A.; Gayda, M.; Nigam, A. Usefulness of self-reported leisure-time physical activity to predict long-term survival in patients with coronary heart disease. Am. J. Cardiol. 2008, 102, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, J.; Kiviniemi, A.; Hautala, A.; Niva, J.; Tulppo, M. Effects of exercise prescription on daily physical activity and maximal exercise capacity in coronary artery disease patients with and without type 2 diabetes. Clin. Physiol. Funct. Imaging 2012, 32, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Ahotupa, M.; Marniemi, J.; Lehtimäki, T.; Talvinen, K.; Raitakari, O.T.; Vasankari, T.; Viikari, J.; Luoma, J.; Ylä-Herttuala, S. Baseline diene conjugation in LDL lipids as a direct measure of in vivo LDL oxidation. Clin. Biochem. 1998, 31, 257–261. [Google Scholar] [CrossRef]
- Väisänen, S.; Gävert, J.; Julkunen, A.; Voutilainen, E.; Penttilä, I. Contents of apolipoprotein A-I, A-II and B of the human serum fractions for high-density and low-density lipoproteins prepared by common precipitation methods. Scand. J. Clin. Lab. Investig. 1992, 52, 853–862. [Google Scholar] [CrossRef]
- Vasankari, T.; Kujala, U.; Vasankari, T.; Ahotupa, M. Reduced oxidized LDL levels after a ten-month exercise training program. Med. Sci. Sports Exerc. 1998, 30, 1496–1501. [Google Scholar] [CrossRef] [PubMed]
- Vasankari, T.; Ahotupa, M.; Viikari, J.; Nuotio, I.; Tikkanen, M. Effects of statin therapy on LDL oxidation. Atherosclerosis 2005, 179, 207–209. [Google Scholar] [CrossRef] [PubMed]
- Ahotupa, M.; Ruutu, M.; Mäntylä, E. Simple methods of quantifying oxidation products and antioxidant potential of low density lipoproteins. Clin. Biochem. 1996, 29, 139–144. [Google Scholar] [CrossRef]
- Vuorimaa, T.; Ahotupa, M.; Irjala, K.; Vasankari, T. Acute prolonged exercise reduces moderately oxidized LDL in healthy men. Int. J. Sports Med. 2005, 26, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Välimäki, I.; Vuorimaa, T.; Ahotupa, M.; Kekkonen, R.A.; Korpela, R.; Vasankari, T. Decreased training volume and increased carbohydrate intake increases oxidized LDL levels. Int. J. Sports Med. 2012, 33, 291–296. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measures | CAD and CAD + T2D Control Baseline (n = 126–132) | CAD and CAD + T2D Control 2 Years (n = 128–132) | CAD and CAD + T2D Exercise Intervention Baseline (n = 84–93) | CAD and CAD + T2D Exercise Intervention 2 Years (n = 85–93) |
|---|---|---|---|---|
| Age (years) | 61.2 (6.1) | 63.2 (6.1) | 62.0 (5.2) | 64.0 (5.2) |
| Gender, male (%) | 98 (74%) | 98 (74%) | 72 (77%) | 72 (77%) |
| Diabetics, n (%) | 64 (50%) | 64 (50%) | 43 (46%) | 43 (46%) |
| Smoking, n (%) | 14 (10%) | 18 (13%) | 6 (7%) | 8 (9%) |
| Height (cm) | 172 (8) | 172 (8) | 171 (9) | 171 (9) |
| Weight (kg) | 83.6 (15.2) | 84.0 (15.4) | 82.1 (13.6) | 81.4 (14.0) |
| BMI (kg/m2) | 28.3 (3.9) | 28.4 (4.1) | 28.1 (3.7) | 27.8 (3.7) |
| Waist (cm) | 98.8 (12.9) | 100.5 (13.6) | 97.5 (11.2) | 96.6 (11.1) |
| Systolic RR (mmHg) | 145 (23) | 145 (26) | 145 (23) | 144 (21) |
| Diastolic RR (mmHg) | 82 (11) | 80 (13) | 83 (12) | 80 (10) |
| HbA1c, % | 6.5 (1.2) | 6.2 (0.9) | 6.2 (0.7) | 6.0 (0.7) |
| Plasma glucose (mmol/L) | 6.5 (1.7) | 6.5 (1.6) | 6.0 (1.1) | 6.2 (1.2) |
| Total cholesterol (mmol/L) | 4.0 (0.9) | 4.0 (0.8) | 4.0 (0.8) | 4.1 (0.8) |
| Triglycerides (mmol/L) | 1.4 (0.9) | 1.5 (0.8) | 1.5 (0.8) | 1.5 (0.7) |
| Ox-HDL (µmol/L) | 29.9 (4.6) | 32.3 (4.9) | 30.2 (5.1) | 32.9 (6.2) |
| HDL cholesterol (mmol/L) | 1.3 (0.3) | 1.3 (0.3) | 1.2 (0.3) | 1.3 (0.3) |
| Ox-HDL/HDL-cholesterol | 24.6 (6.5) | 26.3 (7.1) | 25.7 (7.3) | 27.2 (8.9) |
| Ox-LDL (µmol/L) | 41.8 (9.3) | 41.2 (9.2) | 43.1 (8.2) | 42.1 (8.4) |
| LDL cholesterol (mmol/L)) | 2.3 (0.8) | 2.3 (0.7) | 2.3 (0.7) | 2.4 (0.8) |
| Ox-LDL/LDL-cholesterol | 19.9 (7.7) | 19.9 (7.6) | 20.0 (7.4) | 19.4 (7.2) |
| Lipid-lowering medication, n (%) | 119 (90%) | 118 (90%) | 84 (90%) | 86 (93%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiainen, S.; Kiviniemi, A.; Hautala, A.; Huikuri, H.; Ukkola, O.; Tokola, K.; Tulppo, M.; Vasankari, T. Effects of a Two-Year Home-Based Exercise Training Program on Oxidized LDL and HDL Lipids in Coronary Artery Disease Patients with and without Type-2 Diabetes. Antioxidants 2018, 7, 144. https://doi.org/10.3390/antiox7100144
Tiainen S, Kiviniemi A, Hautala A, Huikuri H, Ukkola O, Tokola K, Tulppo M, Vasankari T. Effects of a Two-Year Home-Based Exercise Training Program on Oxidized LDL and HDL Lipids in Coronary Artery Disease Patients with and without Type-2 Diabetes. Antioxidants. 2018; 7(10):144. https://doi.org/10.3390/antiox7100144
Chicago/Turabian StyleTiainen, Sanna, Antti Kiviniemi, Arto Hautala, Heikki Huikuri, Olavi Ukkola, Kari Tokola, Mikko Tulppo, and Tommi Vasankari. 2018. "Effects of a Two-Year Home-Based Exercise Training Program on Oxidized LDL and HDL Lipids in Coronary Artery Disease Patients with and without Type-2 Diabetes" Antioxidants 7, no. 10: 144. https://doi.org/10.3390/antiox7100144
APA StyleTiainen, S., Kiviniemi, A., Hautala, A., Huikuri, H., Ukkola, O., Tokola, K., Tulppo, M., & Vasankari, T. (2018). Effects of a Two-Year Home-Based Exercise Training Program on Oxidized LDL and HDL Lipids in Coronary Artery Disease Patients with and without Type-2 Diabetes. Antioxidants, 7(10), 144. https://doi.org/10.3390/antiox7100144