


Cardio–Renal and Systemic Effects of SGLT2i Dapagliflozin on Short-Term Anthracycline and HER-2-Blocking Agent Therapy-Induced Cardiotoxicity

 ,
,  ,
,  , ,
, , 
 , ,
, ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Preclinical Model of Short-Term Doxorubicin-Trastuzumab Cardiotoxicity
2.2. Transthoracic Echocardiography and Blood Analysis
2.3. Myocardial NLRP-3 and MyD-88 Expression
2.4. Systemic Troponin-T, BNP, H-FABP and hs-CRP Levels
2.5. Analysis of Myocardial Lipid Peroxidation and Inflammation
2.6. IHC Staining of CTRD and Pro-Inflammatory Biomarkers
2.7. Biomarkers of Damages in Myocardial Tissue
2.8. Statistical Analyses
3. Results
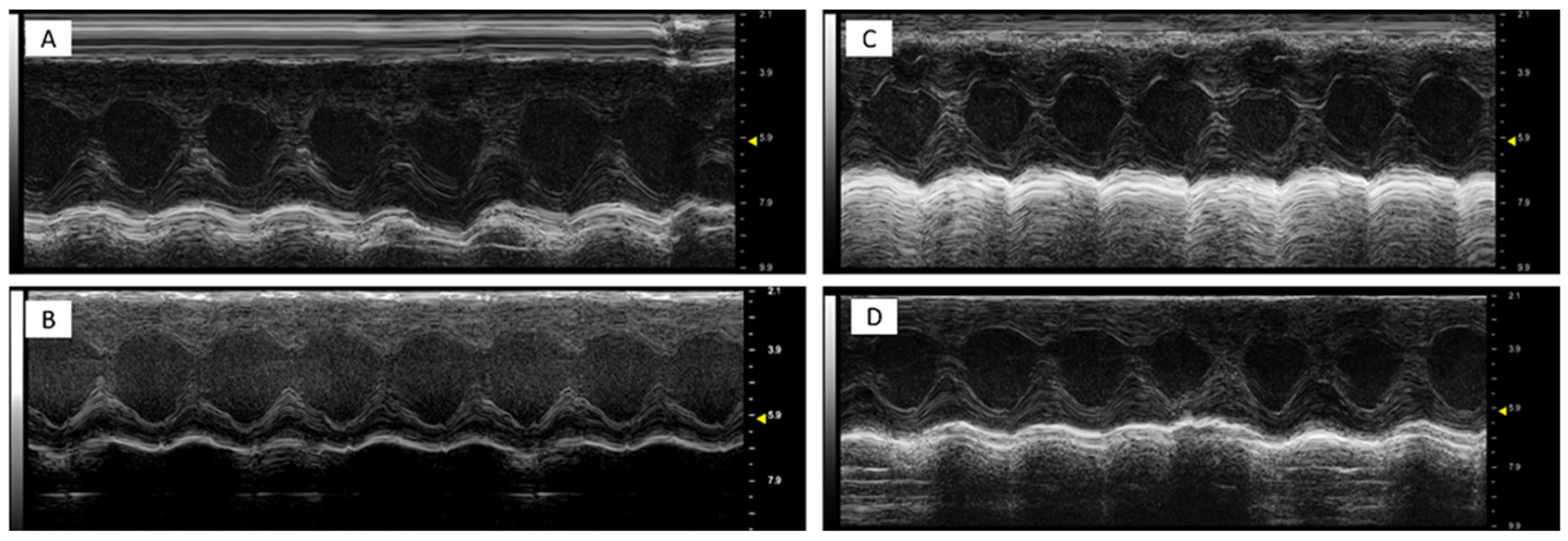
3.1. Dapagliflozin Improves EF and Radial/Longitudinal Strain During Anthracycline and HER-2-Blocking Agent Therapy
3.2. Dapagliflozin Inhibits Myocardial Apoptosis, Lipid Peroxidation and Cellular Injury
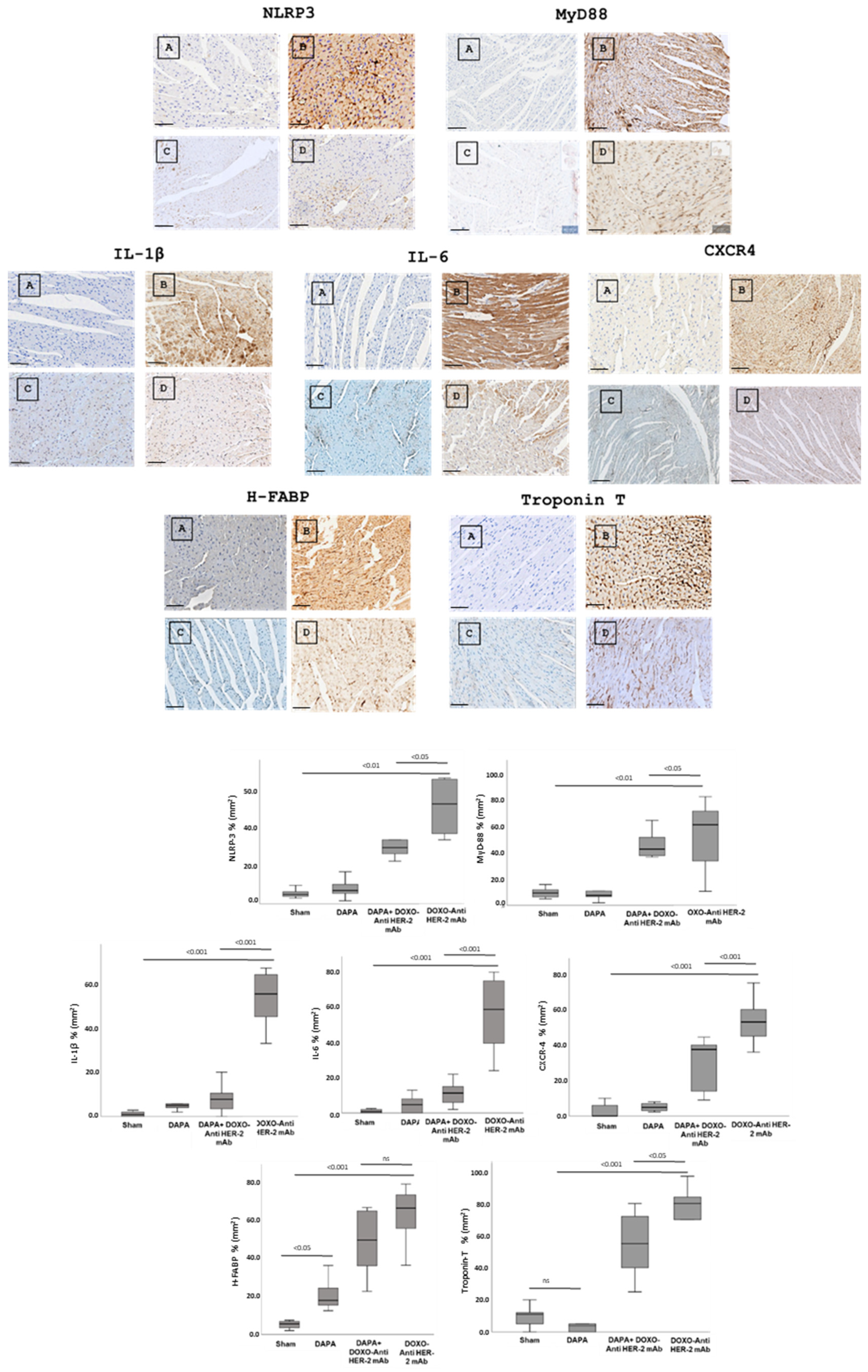
3.3. Dapagliflozin Reduces Myocardial Inflammation Through NLRP3 and MyD88
3.4. Dapagliflozin Reduces IHC Staining of CXCR4, IL-1, IL-6, HFABP, Troponin-T, NLRP3 and Myd-88 in Myocardial Tissue
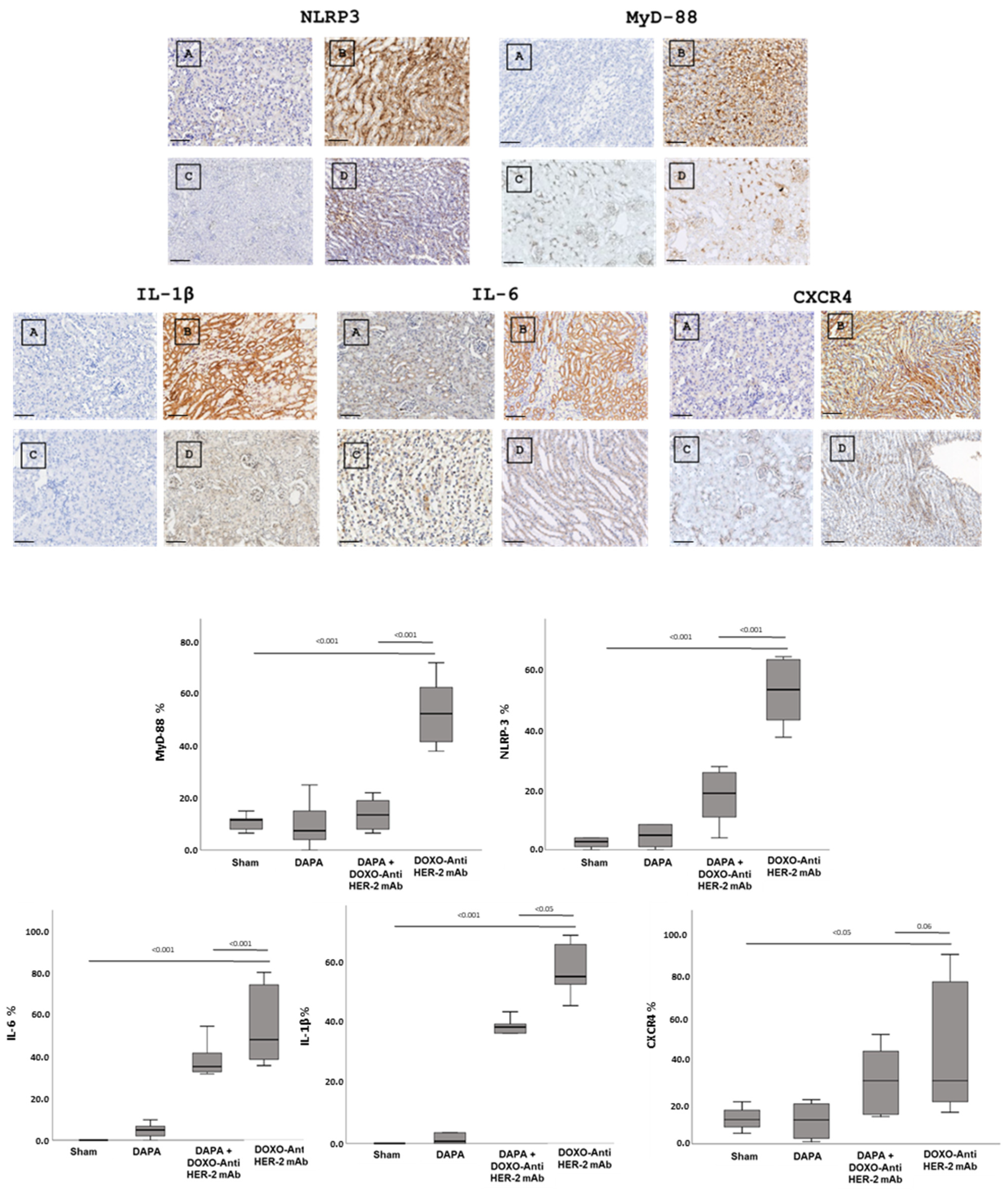
3.5. Dapagliflozin Reduces IHC Staining of IL-1, IL-6, CXCR4, NLRP3 and Myd-88 in Renal Tissue
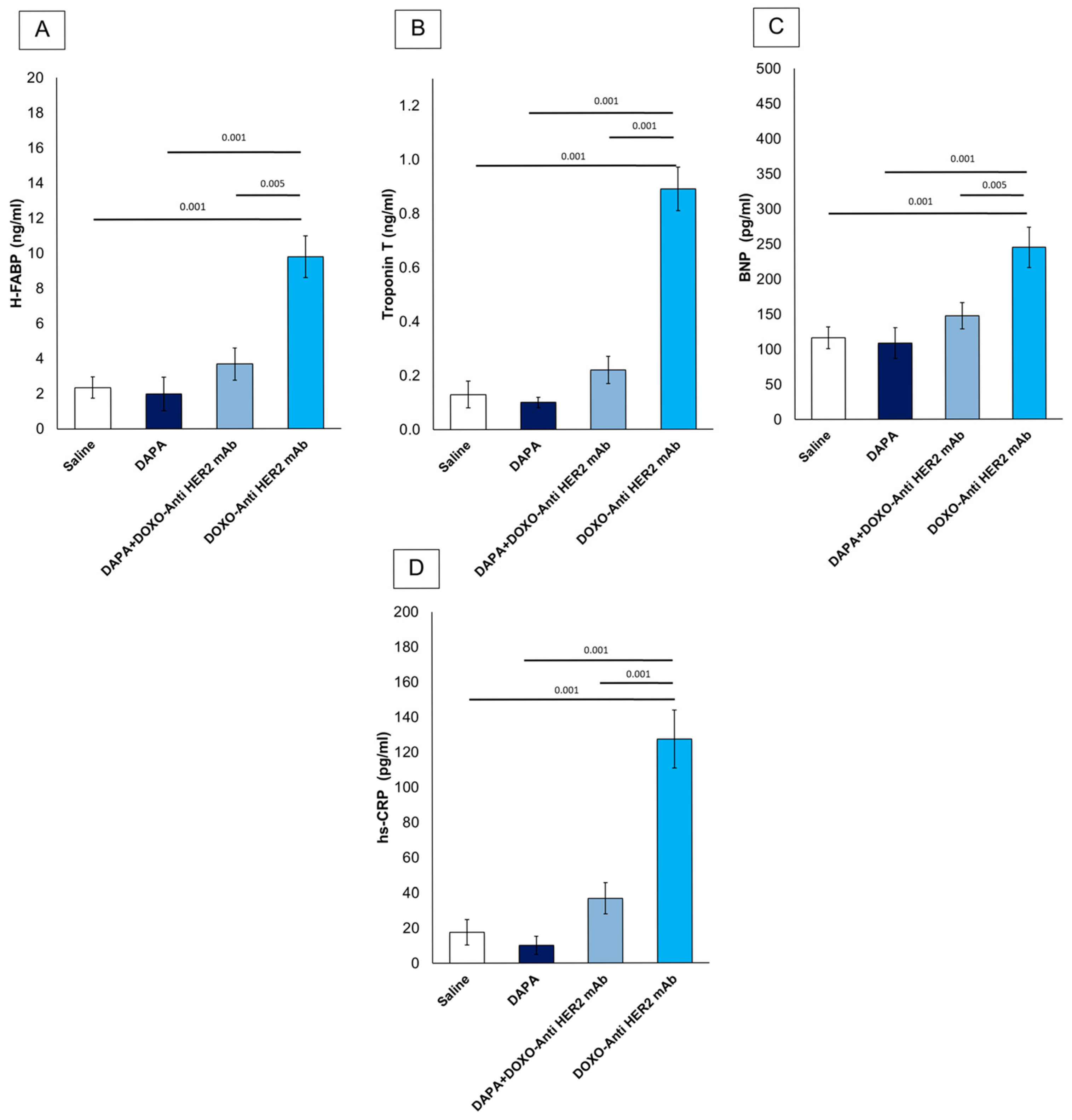
3.6. Dapagliflozin Reduces Systemic Levels of CTRD-Related Biomarkers and Inflammation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DOXO | Doxorubicin |
| HER-2 | Human Epidermal Growth Factor Receptor 2 |
| SGLT2 | Sodium–Glucose Cotransporter 2 |
| T2DM | Type 2 Diabetes Mellitus |
| NF-κB | Nuclear Factor Kappa-Light-Chain-Enhancer of Activated B Cells |
| mAb | Monoclonal Antibody |
| DAPA | Dapagliflozin |
| LV | Left Ventricle |
| ECG | Electrocardiogram |
| FS | Fractional Shortening |
| EF | Ejection Fraction |
| RS | Radial Strain |
| LS | Longitudinal Strain |
| STE | Speckle-Tracking Echocardiography |
| NLRP3 | NOD-, LRR- and Pyrin Domain-Containing Protein 3 |
| MyD88 | Myeloid Differentiation Primary Response 88 |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| BNP | Brain Natriuretic Peptide |
| NT-ProBNP | N-Terminal Pro-Brain Natriuretic Peptide |
| hs-CRP | High-Sensitivity C-Reactive Protein |
| MDA | Malondialdehyde |
| 4-HNE | 4-Hydroxy-2-Nonenal |
| IL | Interleukin |
| IL-1α | Interleukin-1 Alpha |
| IL-1β | Interleukin-1 Beta |
| IL-2 | Interleukin-2 |
| IL-4 | Interleukin-4 |
| IL-6 | Interleukin-6 |
| IL-10 | Interleukin-10 |
| IL-12 | Interleukin-12 |
| IL-17α | Interleukin-17 Alpha |
| IFN-γ | Interferon-Gamma |
| TNF-α | Tumor Necrosis Factor Alpha |
| G-CSF | Granulocyte Colony-Stimulating Factor |
| GM-CSF | Granulocyte-Macrophage Colony-Stimulating Factor |
| CTRD | Chemotherapy-Related Cardiotoxicity |
| CXCR4 | C-X-C Chemokine Receptor Type 4 |
| H-FABP | Heart-Type Fatty Acid-Binding Protein |
| FFPE | Formalin-Fixed, Paraffin-Embedded |
References
- Gianni, L.; Eiermann, W.; Semiglazov, V.; Manikhas, A.; Lluch, A.; Tjulandin, S.; Zambetti, M.; Vazquez, F.; Byakhow, M.; Lichinitser, M.; et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): A randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet 2010, 375, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Lee, S.; Sim, S.H.; Park, I.H.; Lee, K.S.; Kwak, M.H.; Kim, H.J. Cumulative incidence of chemotherapy-induced cardiotoxicity during a 2-year follow-up period in breast cancer patients. Breast Cancer Res Treat. 2020, 182, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Mohsin, S.; Hasan, M.; Sheikh, Z.M.; Mustafa, F.; Tegeltija, V.; Kumar, S.; Kumar, J. Efficacy of SGLT2 inhibitors for anthracycline-induced cardiotoxicity: A meta-analysis in cancer patients. Future Cardiol. 2024, 20, 395–407. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kommu, S. The Role of SGLT2 Inhibitors on Heart Failure Outcomes in Nondiabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Cardiovasc. Pharmacol. 2024, 83, 158–166, Erratum in J. Cardiovasc. Pharmacol. 2024, 83, 359. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quagliariello, V.; Canale, M.L.; Bisceglia, I.; Iovine, M.; Paccone, A.; Maurea, C.; Scherillo, M.; Merola, A.; Giordano, V.; Palma, G.; et al. Sodium-glucose cotransporter 2 inhibitor dapagliflozin prevents ejection fraction reduction, reduces myocardial and renal NF-κB expression and systemic pro-inflammatory biomarkers in models of short-term doxorubicin cardiotoxicity. Front. Cardiovasc. Med. 2024, 11, 1289663. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kasichayanula, S.; Liu, X.; Lacreta, F.; Griffen, S.C.; Boulton, D.W. Clinical pharmacokinetics and pharmacodynamics of dapagliflozin, a selective inhibitor of sodium-glucose co-transporter type 2. Clin. Pharmacokinet. 2014, 53, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Dutka, M.; Bobiński, R.; Francuz, T.; Garczorz, W.; Zimmer, K.; Ilczak, T.; Ćwiertnia, M.; Hajduga, M.B. SGLT-2 Inhibitors in Cancer Treatment-Mechanisms of Action and Emerging New Perspectives. Cancers 2022, 14, 5811. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Park, L.K.; Lim, K.H.; Volkman, J.; Abdiannia, M.; Johnston, H.; Nigogosyan, Z.; Siegel, M.J.; McGill, J.B.; McKee, A.M.; Salam, M.; et al. Safety, tolerability, and effectiveness of the sodium-glucose cotransporter 2 inhibitor (SGLT2i) dapagliflozin in combination with standard chemotherapy for patients with advanced, inoperable pancreatic adenocarcinoma: A phase 1b observational study. Cancer Metab. 2023, 11, 6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Lorenzo, C.; Paciello, R.; Riccio, G.; Rea, D.; Barbieri, A.; Coppola, C.; Maurea, N. Cardiotoxic effects of the novel approved anti-ErbB2 agents and reverse cardioprotective effects of ranolazine. Onco Targets Ther. 2018, 11, 2241–2250. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tocchetti, C.G.; Carpi, A.; Coppola, C.; Quintavalle, C.; Rea, D.; Campesan, M.; Arcari, A.; Piscopo, G.; Cipresso, C.; Monti, M.G.; et al. Ranolazine protects from doxorubicin-induced oxidative stress and cardiac dysfunction. Eur. J. Heart Fail. 2014, 16, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Cappetta, D.; Esposito, G.; Coppini, R.; Piegari, E.; Russo, R.; Ciuffreda, L.P.; Rivellino, A.; Santini, L.; Rafaniello, C.; Scavone, C.; et al. Effects of ranolazine in a model of doxorubicin-induced left ventricle diastolic dysfunction. Br. J. Pharmacol. 2017, 174, 3696–3712. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Desai, V.G.; Vijay, V.; Han, T.; Moland, C.L.; Phanavanh, B.; Lee, T.; Davis, K.J.; Muskhelishvili, L.; Stine, K.C.; Fuscoe, J.C. Doxorubicin-induced delayed-onset subclinical cardiotoxicity in mice. J. Appl. Toxicol. 2022, 42, 778–792. [Google Scholar] [CrossRef] [PubMed]
- Olorundare, O.E.; Adeneye, A.A.; Akinsola, A.O.; Ajayi, A.M.; Agede, O.A.; Soyemi, S.S.; Mgbehoma, A.I.; Okoye, I.I.; Albrecht, R.M.; Ntambi, J.M.; et al. Therapeutic Potentials of Selected Antihypertensive Agents and Their Fixed-Dose Combinations Against Trastuzumab-Mediated Cardiotoxicity. Front. Pharmacol. 2021, 11, 610331. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dabour, M.S.; George, M.Y.; Daniel, M.R.; Blaes, A.H.; Zordoky, B.N. The Cardioprotective and Anticancer Effects of SGLT2 Inhibitors: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2024, 6, 159–182. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, C.; Zhang, J.; Xue, M.; Li, X.; Han, F.; Liu, X.; Xu, L.; Lu, Y.; Cheng, Y.; Li, T.; et al. SGLT2 inhibition with empagliflozin attenuates myocardial oxidative stress and fibrosis in diabetic mice heart. Cardiovasc. Diabetol. 2019, 18, 15. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Riccio, G.; Antonucci, S.; Coppola, C.; D’Avino, C.; Piscopo, G.; Fiore, D.; Maurea, C.; Russo, M.; Rea, D.; Arra, C.; et al. Ranolazine Attenuates Trastuzumab-Induced Heart Dysfunction by Modulating ROS Production. Front. Physiol. 2018, 9, 38. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quagliariello, V.; De Laurentiis, M.; Rea, D.; Barbieri, A.; Monti, M.G.; Carbone, A.; Paccone, A.; Altucci, L.; Conte, M.; Canale, M.L.; et al. The SGLT-2 inhibitor empagliflozin improves myocardial strain, reduces cardiac fibrosis and pro-inflammatory cytokines in non-diabetic mice treated with doxorubicin. Cardiovasc. Diabetol. 2021, 20, 150. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quagliariello, V.; Passariello, M.; Di Mauro, A.; Cipullo, C.; Paccone, A.; Barbieri, A.; Palma, G.; Luciano, A.; Buccolo, S.; Bisceglia, I.; et al. Immune checkpoint inhibitor therapy increases systemic SDF-1, cardiac DAMPs Fibronectin-EDA, S100/Calgranulin, galectine-3, and NLRP3-MyD88-chemokine pathways. Front. Cardiovasc. Med. 2022, 9, 930797, Erratum in Front. Cardiovasc. Med. 2023, 10, 1129873. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhao, R.; Shu, F.; Zhang, C.; Song, F.; Xu, Y.; Guo, Y.; Xue, K.; Lin, J.; Shu, X.; Hsi, D.H.; et al. Early Detection and Prediction of Anthracycline-Induced Right Ventricular Cardiotoxicity by 3-Dimensional Echocardiography. JACC CardioOncol. 2020, 2, 13–22. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quagliariello, V.; Passariello, M.; Rea, D.; Barbieri, A.; Iovine, M.; Bonelli, A.; Caronna, A.; Botti, G.; De Lorenzo, C.; Maurea, N. Evidences of CTLA-4 and PD-1 Blocking Agents-Induced Cardiotoxicity in Cellular and Preclinical Models. J. Pers. Med. 2020, 10, 179. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Todd, E.A.; Williams, M.; Kamiar, A.; Rasmussen, M.A.; Shehadeh, L.A. Echocardiography protocol: A tool for infrequently used parameters in mice. Front. Cardiovasc. Med. 2022, 9, 1038385. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Linsky, P.L.; Choi, Y.; Ouseph, R.; Slaughter, M.S.; Keller, B.B.; Jones, C.M. High-Resolution Imaging Using the VisualSonics Vevo 2100 on Isolated, Perfused Porcine Kidneys on Mechanical Circulatory Support. ASAIO J. 2014, 60, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Kohut, A.; Patel, N.; Singh, H. Comprehensive Echocardiographic Assessment of the Right Ventricle in Murine Models. J. Cardiovasc. Ultrasound 2016, 24, 229–238. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gowri Sankar, S.; Alwin Prem Anand, A. Cytokine IP-10 and GM-CSF are prognostic biomarkers for severity in secondary dengue infection. Hum. Immunol. 2021, 82, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Quagliariello, V.; Basilicata, M.G.; Pepe, G.; De Anseris, R.; Di Mauro, A.; Scognamiglio, G.; Palma, G.; Vestuto, V.; Buccolo, S.; Luciano, A.; et al. Combination of Spirulina platensis, Ganoderma lucidum and Moringa oleifera Improves Cardiac Functions and Reduces Pro-Inflammatory Biomarkers in Preclinical Models of Short-Term Doxorubicin-Mediated Cardiotoxicity: New Frontiers in Cardioncology? J. Cardiovasc. Dev. Dis. 2022, 9, 423. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cortellino, S.; Quagliariello, V.; Delfanti, G.; Blaževitš, O.; Chiodoni, C.; Maurea, N.; Di Mauro, A.; Tatangelo, F.; Pisati, F.; Shmahala, A.; et al. Fasting mimicking diet in mice delays cancer growth and reduces immunotherapy-associated cardiovascular and systemic side effects. Nat. Commun. 2023, 14, 5529. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Clark, L.N.; Elwood, H.R.; Uhlenhake, E.E.; Smoller, B.R.; Shalin, S.C.; Gardner, J.M. Nuclear factor XIIIa staining (clone AC-1A1 mouse monoclonal) is a highly sensitive marker of sebaceous differentiation in normal and neoplastic sebocytes. J. Cutan. Pathol. 2016, 43, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, D.B.; Peng, X.; Chen, B.; Pentassuglia, L.; Lim, C.C. Mechanisms of anthracycline cardiac injury: Can we identify strategies for cardioprotection? Prog. Cardiovasc. Dis. 2010, 53, 105–113. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Van Linthout, S. Shared Mechanisms in Cancer and Cardiovascular Disease: S100A8/9 and the NLRP3 Inflammasome: JACC: CardioOncology State-of-the-Art Review. J. Am. Coll. Cardiol. CardioOncol. 2024, in press. [CrossRef]
- Chertow, G.M.; Correa-Rotter, R.; Vart, P.; Jongs, N.; McMurray, J.J.V.; Rossing, P.; Langkilde, A.M.; Sjöström, C.D.; Toto, R.D.; Wheeler, D.C.; et al. Effects of Dapagliflozin in Chronic Kidney Disease, with and Without Other Cardiovascular Medications: DAPA-CKD Trial. J. Am. Heart Assoc. 2023, 12, e028739. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Salvatore, T.; Galiero, R.; Caturano, A.; Rinaldi, L.; Di Martino, A.; Albanese, G.; Di Salvo, J.; Epifani, R.; Marfella, R.; Docimo, G.; et al. An Overview of the Cardiorenal Protective Mechanisms of SGLT2 Inhibitors. Int. J. Mol. Sci. 2022, 23, 3651. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eaton, H.; Timm, K.N. Mechanisms of trastuzumab induced cardiotoxicity—Is exercise a potential treatment? Cardiooncology 2023, 9, 22. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moliterni, A.; Ménard, S.; Valagussa, P.; Biganzoli, E.; Boracchi, P.; Balsari, A.; Casalini, P.; Tomasic, G.; Marubini, E.; Pilotti, S.; et al. HER2 overexpression and doxorubicin in adjuvant chemotherapy for resectable breast cancer. J. Clin. Oncol. 2003, 21, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.; Zhang, X.; Li, J. Personalized Trastuzumab-Induced Cardiac Dysfunction Risk Stratification and Surveillance. JACC CardioOncol. 2025, 7, 216–218. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Belger, C.; Abrahams, C.; Imamdin, A.; Lecour, S. Doxorubicin-induced cardiotoxicity and risk factors. Int. J. Cardiol. Heart Vasc. 2023, 50, 101332. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hou, H.; Xu, Y.; Xie, M.; Chen, R. Exploring the potential molecular mechanism of trastuzumab-induced cardiotoxicity based on RNA sequencing and bioinformatics analysis. Biochem. Pharmacol. 2023, 208, 115388. [Google Scholar] [CrossRef] [PubMed]
- Anjos, M.; Fontes-Oliveira, M.; Costa, V.M.; Santos, M.; Ferreira, R. An update of the molecular mechanisms underlying doxorubicin plus trastuzumab induced cardiotoxicity. Life Sci. 2021, 280, 119760. [Google Scholar] [CrossRef] [PubMed]
- An, J.; Sheikh, M.S. Toxicology of Trastuzumab: An Insight into Mechanisms of Cardiotoxicity. Curr. Cancer Drug Targets 2019, 19, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, N.; Rosenthal, A.; Dabas, N.; Kropotova, Y.; Lippman, M.; Bishopric, N.H. Trastuzumab-induced cardiotoxicity: A review of clinical risk factors, pharmacologic prevention, and cardiotoxicity of other HER2-directed therapies. Breast Cancer Res. Treat. 2021, 188, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Rochette, L.; Guenancia, C.; Gudjoncik, A.; Hachet, O.; Zeller, M.; Cottin, Y.; Vergely, C. Anthracyclines/trastuzumab: New aspects of cardiotoxicity and molecular mechanisms. Trends Pharmacol. Sci. 2015, 36, 326–348. [Google Scholar] [CrossRef] [PubMed]
- Vo, J.B.; Ramin, C.; Veiga, L.H.S.; Brandt, C.; Curtis, R.E.; Bodelon, C.; Barac, A.; Roger, V.L.; Feigelson, H.S.; Buist, D.S.M.; et al. Long-term cardiovascular disease risk after anthracycline and trastuzumab treatments in US breast cancer survivors. J. Natl. Cancer Inst. 2024, 116, 1384–1394. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nowsheen, S.; Viscuse, P.V.; O’Sullivan, C.C.; Sandhu, N.P.; Haddad, T.C.; Blaes, A.; Klemp, J.; Nhola, L.; Herrmann, J.; Ruddy, K.J. Incidence, Diagnosis, and Treatment of Cardiac Toxicity from Trastuzumab in Patients with Breast Cancer. Curr. Breast Cancer Rep. 2017, 9, 173–182. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mauro, A.G.; Mezzaroma, E.; Toldo, S.; Melendez, G.C.; Franco, R.L.; Lesnefsky, E.J.; Abbate, A.; Hundley, W.G.; Salloum, F.N. NLRP3-mediated inflammation in cardio-oncology: Sterile yet harmful. Transl Res. 2023, 252, 9–20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alexandraki, A.; Papageorgiou, E.; Zacharia, M.; Keramida, K.; Papakonstantinou, A.; Cipolla, C.M.; Tsekoura, D.; Naka, K.; Mazzocco, K.; Mauri, D.; et al. New Insights in the Era of Clinical Biomarkers as Potential Predictors of Systemic Therapy-Induced Cardiotoxicity in Women with Breast Cancer: A Systematic Review. Cancers 2023, 15, 3290. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vuong, J.T.; Stein-Merlob, A.F.; Cheng, R.K.; Yang, E.H. Novel Therapeutics for Anthracycline Induced Cardiotoxicity. Front. Cardiovasc. Med. 2022, 9, 863314. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mezzaroma, E.; Abbate, A.; Toldo, S. NLRP3 Inflammasome Inhibitors in Cardiovascular Diseases. Molecules 2021, 26, 976. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Toldo, S.; Abbate, A. The role of the NLRP3 inflammasome and pyroptosis in cardiovascular diseases. Nat. Rev. Cardiol. 2024, 21, 219–237. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Blyszczuk, P.; Kania, G.; Dieterle, T.; Marty, R.R.; Valaperti, A.; Berthonneche, C.; Pedrazzini, T.; Berger, C.T.; Dirnhofer, S.; Matter, C.M.; et al. Myeloid differentiation factor-88/interleukin-1 signaling controls cardiac fibrosis and heart failure progression in inflammatory dilated cardiomyopathy. Circ. Res. 2009, 105, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Fang, Z.M.; Yi, X.; Wei, X.; Jiang, D.S. The interaction between ferroptosis and inflammatory signaling pathways. Cell Death Dis. 2023, 14, 205. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Baik, A.H.; Oluwole, O.O.; Johnson, D.B.; Shah, N.; Salem, J.E.; Tsai, K.K.; Moslehi, J.J. Mechanisms of Cardiovascular Toxicities Associated With Immunotherapies. Circ. Res. 2021, 128, 1780–1801. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Katkenov, N.; Mukhatayev, Z.; Kozhakhmetov, S.; Sailybayeva, A.; Bekbossynova, M.; Kushugulova, A. Systematic Review on the Role of IL-6 and IL-1β in Cardiovascular Diseases. J. Cardiovasc. Dev. Dis. 2024, 11, 206. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Döring, Y.; Pawig, L.; Weber, C.; Noels, H. The CXCL12/CXCR4 chemokine ligand/receptor axis in cardiovascular disease. Front. Physiol. 2014, 5, 212. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Beji, S.; Milano, G.; Scopece, A.; Cicchillitti, L.; Cencioni, C.; Picozza, M.; D’Alessandra, Y.; Pizzolato, S.; Bertolotti, M.; Spaltro, G.; et al. Doxorubicin upregulates CXCR4 via miR-200c/ZEB1-dependent mechanism in human cardiac mesenchymal progenitor cells. Cell Death Dis. 2017, 8, e3020. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhu, J.; Zhang, J.; Zhang, L.; Du, R.; Xiang, D.; Wu, M.; Zhang, R.; Han, W. Interleukin-1 signaling mediates acute doxorubicin-induced cardiotoxicity. Biomed. Pharmacother. 2011, 65, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Sarkar, A.; Chen, Y.; Xu, B.; Zhu, X.; Yuan, Y.; Guan, T. Overexpression of heart-type fatty acid binding protein enhances fatty acid-induced podocyte injury. Exp. Ther. Med. 2018, 15, 2054–2061. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kato, E.T.; Silverman, M.G.; Mosenzon, O.; Zelniker, T.A.; Cahn, A.; Furtado, R.H.M.; Kuder, J.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A.; et al. Effect of Dapagliflozin on Heart Failure and Mortality in Type 2 Diabetes Mellitus. Circulation 2019, 139, 2528–2536. [Google Scholar] [CrossRef] [PubMed]
- Kurata, Y.; Nangaku, M. Dapagliflozin for the treatment of chronic kidney disease. Expert. Rev. Endocrinol. Metab. 2022, 17, 275–291. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Groups (n = 6) | Treatments |
|---|---|
| Saline (control) | 100 μL saline solution |
| Doxorubicin-HER-2-blocking agent (Doxo-HER-2 mAb) | Doxorubicin at 2.17 mg/kg/day via intraperitoneal administration (i.p) for 5 days, followed by HER-2 mAb administration at 2.25 mg/kg i.p for an additional 5 days |
| Dapagliflozin (Dapa) | Dapagliflozin 10 mg/kg/day via oral gavage |
| Doxorubicin-HER-2-blocking agent + dapagliflozin (Doxo-HER-2 mAb + Dapa) | Doxo-HER-2 mAb + dapagliflozin combination at the same concentrations as each drug administered alone |
| Antibody | Clone | Host | Dilution µg/mL | Code (Company) |
|---|---|---|---|---|
| NLRP-3 | MA5-23919 | Rat/IgG2a | 1:100 | Invitrogen (Waltham, MA, USA) |
| MYD-88 | (E-11): sc-74532 | Mouse/IgG2b | 1:150 | S.Cruz (Santa Cruz, CA, USA) |
| IL-1 | (B-7): sc-9983 | Mouse/IgG2b | 1:100 | S.Cruz (Santa Cruz, CA, USA) |
| IL-6 | (E-4): sc-28343 | Mouse/IgG2a | 1:200 | S.Cruz (Santa Cruz, CA, USA) |
| CXCR4 | 60042-1-Ig | Mouse/IgM | 1:150 | ProteinTech (Rosemont, IL, USA) |
| Troponin-T | T-C (CT3): sc-20025 | Mouse/IgG2a | 1:100 | S.Cruz (Santa Cruz, CA, USA) |
| H-FABP | 328607 | Mouse/IgG2a | 1:100 | Biotechne (Minneapolis, MN, USA) |
| Heart-Related Indices | Sham (Saline) | DOXO-HER-2 mAb | DAPA | DAPA + DOXO-HER-2 mAb |
|---|---|---|---|---|
| IVS; d-D (mm) | 0.54 ± 0.09 | 0.61 ± 0.09 ns | 0.47 ± 0.13 | 0.56 ± 0.12 ns |
| LVID; d-D (mm) | 1.92 ± 0.21 | 3.1± 0.18 c | 1.87 ± 0.11 | 2.37 ± 0.28 C |
| LVPW; d-D (mm) | 0.57 ± 0.12 | 0.6 ± 0.08 ns | 0.52 ± 0.07 | 0.58 ± 0.12 ns |
| LV Mass (mg) | 48.8 ± 2.8 | 58.8 ± 1.9 c | 44.1 ± 1.8 | 49.7 ± 1.66 B |
| LVID; s-D (mm) | 1.37 ± 0.4 | 1.82 ± 0.33 b | 1.31 ± 0.08 | 1.48 ± 0.17 A |
| EF (%) | 94.28 ± 1.8 | 60.2 ± 2.6 c | 95.71 ± 1.3 | 90.8 ± 2.32 C |
| FS (%) | 66.35 ± 2.9 | 38.1 ± 2.12 c | 67.1 ± 2.41 | 61.2 ± 2.63 C |
| Radial Strain (Pk%) | 38.7 ± 2.2 | 9.7 ± 1.7 c | 39.6 ± 1.8 | 30.8 ± 2.88 C |
| Longitudinal Strain (Pk%) | −21.8 ± 1.32 | −10.2 ± 1.9 c | −22.4 ± 3.8 | −19.3 ± 3.2 B |
| Heart weight (g) | 0.14 ± 0.07 | 0.27 ± 1.3 ns | 0.13 ± 0.04 | 0.16 ± 0.08 ns |
| Lipid Peroxidation Products | Sham (Saline) | DOXO-HER-2 mAb | DAPA | DAPA + DOXO-HER-2 mAb |
|---|---|---|---|---|
| MDA (nmol/g protein) | 0.032 ± 0.008 | 0.241 ± 0.03 c | 0.021 ± 0.003 | 0.059 ± 0.09 B |
| 4-HNA (nmol/g protein) | 0.052 ± 0.003 | 0.32 ± 0.07 c | 0.041 ± 0.006 | 0.067 ± 0.07 C |
| Novel Biomarkers of Cardiovascular Injury | Sham (Saline) | DOXO-HER-2 mAb | DAPA | DAPA + DOXO-HER-2 mAb |
|---|---|---|---|---|
| Cardiac myosin light chain (cMLC1) 1 (ng/mL) | 2.23 ± 0.04 | 5.44 ± 0.09 c | 2.18 ± 0.06 | 3.14 ± 0.03 C |
| Growth differentiation factor type 15 (GDF-15) (ng/mL) | 1.25 ± 0.06 | 4.33 ± 0.13 c | 1.13 ± 0.11 | 1.85 ± 0.15 C |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quagliariello, V.; Di Mauro, A.; Ferrara, G.; Bruzzese, F.; Palma, G.; Luciano, A.; Canale, M.L.; Bisceglia, I.; Iovine, M.; Cadeddu Dessalvi, C.; et al. Cardio–Renal and Systemic Effects of SGLT2i Dapagliflozin on Short-Term Anthracycline and HER-2-Blocking Agent Therapy-Induced Cardiotoxicity. Antioxidants 2025, 14, 612. https://doi.org/10.3390/antiox14050612
Quagliariello V, Di Mauro A, Ferrara G, Bruzzese F, Palma G, Luciano A, Canale ML, Bisceglia I, Iovine M, Cadeddu Dessalvi C, et al. Cardio–Renal and Systemic Effects of SGLT2i Dapagliflozin on Short-Term Anthracycline and HER-2-Blocking Agent Therapy-Induced Cardiotoxicity. Antioxidants. 2025; 14(5):612. https://doi.org/10.3390/antiox14050612
Chicago/Turabian StyleQuagliariello, Vincenzo, Annabella Di Mauro, Gerardo Ferrara, Francesca Bruzzese, Giuseppe Palma, Antonio Luciano, Maria Laura Canale, Irma Bisceglia, Martina Iovine, Christian Cadeddu Dessalvi, and et al. 2025. "Cardio–Renal and Systemic Effects of SGLT2i Dapagliflozin on Short-Term Anthracycline and HER-2-Blocking Agent Therapy-Induced Cardiotoxicity" Antioxidants 14, no. 5: 612. https://doi.org/10.3390/antiox14050612
APA StyleQuagliariello, V., Di Mauro, A., Ferrara, G., Bruzzese, F., Palma, G., Luciano, A., Canale, M. L., Bisceglia, I., Iovine, M., Cadeddu Dessalvi, C., Maurea, C., Barbato, M., Inno, A., Berretta, M., Paccone, A., Mauriello, A., Fonderico, C., Maratea, A. C., & Maurea, N. (2025). Cardio–Renal and Systemic Effects of SGLT2i Dapagliflozin on Short-Term Anthracycline and HER-2-Blocking Agent Therapy-Induced Cardiotoxicity. Antioxidants, 14(5), 612. https://doi.org/10.3390/antiox14050612