
The Relationship between Exercise and Salivary Oxidative Stress: A Systematic Review

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Registration Protocol and Study Design
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Selection Process
2.6. Data Collection Process
2.7. Quality Assessment Analysis
2.8. Risk of Bias
2.9. Statistical Synthesis
2.10. Assessment of Quality of Evidence
3. Results
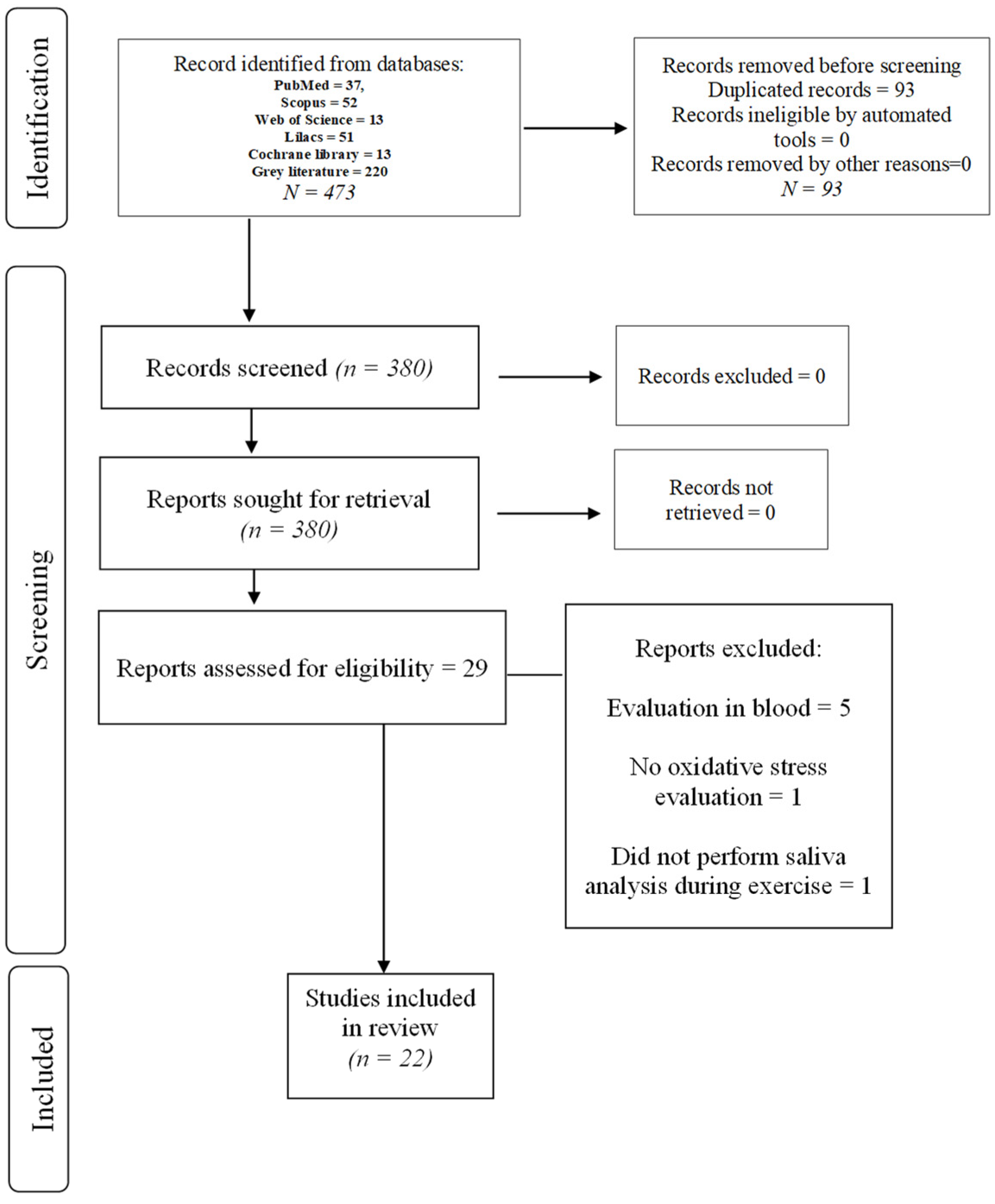
3.1. Study Selection
3.2. Study Characteristics
3.3. Results of Individual Studies and Syntheses
3.4. Risk of Bias
3.5. Certainty of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kanaley, J.A.; Colberg, S.R.; Corcoran, M.H.; Malin, S.K.; Rodriguez, N.R.; Crespo, C.J.; Kirwan, J.P.; Zierath, J.R. Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement from the American College of Sports Medicine. Med. Sci. Sports Exerc. 2022, 54, 353–368. [Google Scholar] [CrossRef]
- Fernandes, R.; Correa, M.; Santos, M.; Almeida, A.; Fagundes, N.; Maia, L.; Lima, R. The Effects of Moderate Physical Exercise on Adult Cognition: A Systematic Review. Front. Physiol. 2018, 9, 667. [Google Scholar] [CrossRef] [PubMed]
- Wackerhage, H.; Schoenfeld, B.J. Personalized, Evidence-Informed Training Plans and Exercise Prescriptions for Performance, Fitness and Health. Sports Med. 2021, 51, 1805–1813. [Google Scholar] [CrossRef]
- Toldy, A.; Stadler, K.; Sasvári, M.; Jakus, J.; Jung, K.J.; Chung, H.Y.; Berkes, I.; Nyakas, C.; Radák, Z. The effect of exercise and nettle supplementation on oxidative stress markers in the rat brain. Brain Res. Bull. 2005, 65, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Boveris, A.; Navarro, A. Brain mitochondrial dysfunction in aging. IUBMB Life 2008, 60, 308–314. [Google Scholar] [CrossRef]
- Leeuwenburgh, C.; Heinecke, J.W. Oxidative stress and antioxidants in exercise. Curr. Med. Chem. 2001, 8, 829–838. [Google Scholar] [CrossRef]
- Powers, S.K.; Deminice, R.; Ozdemir, M.; Yoshihara, T.; Bomkamp, M.P.; Hyatt, H. Exercise-induced oxidative stress: Friend or foe? J. Sport Health Sci. 2020, 9, 415–425. [Google Scholar] [CrossRef]
- Syu, G.-D.; Chen, H.-i.; Jen, C.J. Severe Exercise and Exercise Training Exert Opposite Effects on Human Neutrophil Apoptosis via Altering the Redox Status. PLoS ONE 2011, 6, e24385. [Google Scholar] [CrossRef]
- Sureda, A.; Batle, J.M.; Tur, J.A.; Pons, A. Competitive apnea diving sessions induces an adaptative antioxidant response in mononucleated blood cells. J. Physiol. Biochem. 2015, 71, 373–380. [Google Scholar] [CrossRef]
- Lima, F.D.; Stamm, D.N.; Della-Pace, I.D.; Dobrachinski, F.; de Carvalho, N.R.; Royes, L.F.F.; Soares, F.A.; Rocha, J.B.; González-Gallego, J.; Bresciani, G. Swimming Training Induces Liver Mitochondrial Adaptations to Oxidative Stress in Rats Submitted to Repeated Exhaustive Swimming Bouts. PLoS ONE 2013, 8, e55668. [Google Scholar] [CrossRef]
- Powers, S.K.; Radak, Z.; Ji, L.L. Exercise-induced oxidative stress: Past, present and future. J. Physiol. 2016, 594, 5081–5092. [Google Scholar] [CrossRef]
- Sone, R.; Eda, N.; Kosaki, K.; Endo, M.; Watanabe, K. Influence of acute high-intensity exercise on salivary nitric oxide levels. J. Oral Sci. 2019, 61, 307–312. [Google Scholar] [CrossRef]
- Evans, L.; Zhang, F.; Omaye, S. Vitamin C Supplementation Reduces Exercise-Induced Oxidative Stress and Increases Peak Muscular Force. Food Nutr. Sci. 2017, 8, 812–822. [Google Scholar] [CrossRef]
- Biagini, D.; Lomonaco, T.; Ghimenti, S.; Fusi, J.; Cerri, E.; De Angelis, F.; Bellagambi, F.G.; Oger, C.; Galano, J.M.; Bramanti, E.; et al. Saliva as a non-invasive tool for monitoring oxidative stress in swimmers athletes performing a VO2max cycle ergometer test. Talanta 2020, 216, 120979. [Google Scholar] [CrossRef]
- Deminice, R.; Sicchieri, T.; Payao, P.O.; Jordao, A.A. Blood and salivary oxidative stress biomarkers following an acute session of resistance exercise in humans. Int. J. Sports Med. 2010, 31, 599–603. [Google Scholar] [CrossRef]
- Battino, M.; Ferreiro, M.S.; Gallardo, I.; Newman, H.N.; Bullon, P. The antioxidant capacity of saliva. J. Clin. Periodontol. 2002, 29, 189–194. [Google Scholar] [CrossRef]
- Öngöz Dede, F.; Bozkurt Doğan, Ş.; Balli, U.; Avci, B.; Durmuşlar, M.C.; Baratzade, T. Glutathione levels in plasma, saliva and gingival crevicular fluid after periodontal therapy in obese and normal weight individuals. J. Periodontal Res. 2016, 51, 726–734. [Google Scholar] [CrossRef]
- Loo, J.A.; Yan, W.; Ramachandran, P.; Wong, D.T. Comparative Human Salivary and Plasma Proteomes. J. Dent. Res. 2010, 89, 1016–1023. [Google Scholar] [CrossRef]
- Augusto-Oliveira, M.; Arrifano, G.d.P.; Lopes-Araújo, A.; Santos-Sacramento, L.; Lima, R.R.; Lamers, M.L.; Le Blond, J.; Crespo-Lopez, M.E. Salivary biomarkers and neuropsychological outcomes: A non-invasive approach to investigate pollutants-associated neurotoxicity and its effects on cognition in vulnerable populations. Environ. Res. 2021, 200, 111432. [Google Scholar] [CrossRef] [PubMed]
- Buzalaf, M.A.R.; Ortiz, A.d.C.; Carvalho, T.S.; Fideles, S.O.M.; Araújo, T.T.; Moraes, S.M.; Buzalaf, N.R.; Reis, F.N. Saliva as a diagnostic tool for dental caries, periodontal disease and cancer: Is there a need for more biomarkers? Expert Rev. Mol. Diagn. 2020, 20, 543–555. [Google Scholar] [CrossRef]
- Evans, L.W.; Omaye, S.T. Use of Saliva Biomarkers to Monitor Efficacy of Vitamin C in Exercise-Induced Oxidative Stress. Antioxidants 2017, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Sterne, J.A.; Savovic, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10, 29–31. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: New York, NY, USA, 2021. [Google Scholar]
- Lee, Y.-H.; Kim, J.H.; Zhou, H.; Kim, B.W.; Wong, D.T. Salivary transcriptomic biomarkers for detection of ovarian cancer: For serous papillary adenocarcinoma. J. Mol. Med. 2012, 90, 427–434. [Google Scholar] [CrossRef]
- Caramez, F. Respostas Adaptativas ao Treinamento Físico em Parâmetros Bioquimicos Salivares de Atletas de Futebol; Universidade do Estado do Rio de Janeiro: Rio de Janeiro, Brazil, 2016. [Google Scholar]
- Puspaningtyas, D.E.; Afriani, Y.; Mahfida, S.L.; Kushartanti, W.; Farmawati, A. Effect of exercise on lipid peroxidation in student soccer players. J. Med. Sci. 2018, 50, 91–100. [Google Scholar] [CrossRef]
- Škrgat, S.; Marčun, R.; Kern, I.; Šilar, M.; Šelb, J.; Fležar, M.; Korošec, P. Systemic and airway oxidative stress in competitive swimmers. Respir. Med. 2018, 137, 129–133. [Google Scholar] [CrossRef]
- Grushin, A.; Dudnik, E.; Glazachev, O.; Zotkin, S.; Zelenkova, I.; Korneev, P.; Koprov, S.; Almiashev, D. Assessment of the oxidative-antioxidant status and aerobic performance of elite skiers-racers in the dynamics of training cycle at moderate altitude. Sports Med. Res. Prac. 2019, 4, 12. [Google Scholar] [CrossRef]
- Sone, R.; Matsuba, K.; Tahara, R.; Eda, N.; Kosaki, K.; Jesmin, S.; Miyakawa, S.; Watanabe, K. Assessment of Salivary Nitric Oxide Levels in Elite University Athletes in Japan: Findings From a Cross Sectional Study Design. J. Clin. Med. Res. 2019, 11, 114–120. [Google Scholar] [CrossRef]
- West, D.J.; Cunningham, D.J.; Finn, C.V.; Scott, P.M.; Crewther, B.T.; Cook, C.J.; Kilduff, L.P. The metabolic, hormonal, biochemical, and neuromuscular function responses to a backward sled drag training session. J. Strength Cond. Res. 2014, 28, 265–272. [Google Scholar] [CrossRef]
- Damirchi, A.; Zareei, A.S.; Sariri, R. Salivary antioxidants of male athletes after aerobic exercise and garlic supplementation on: A randomized, double blind, placebo-controlled study. J. Oral Biol. Craniofac. Res. 2015, 5, 146–152. [Google Scholar] [CrossRef]
- Sari-Sarraf, V.; Amirsasan, R.; Zolfi, H. The effect of eight weeks aerobic training and exhaustive exercise on salivary and blood antioxidant enzymes in sedentary men. Sport Physiol. Manag. Investig. 2017, 9, 75–85. [Google Scholar]
- Rodrigues de Araujo, V.; Lisboa, P.; Boaventura, G.; Caramez, F.; Pires, L.; Oliveira, E.; Moura, E.; Casimiro-Lopes, G. Acute high-intensity exercise test in soccer athletes affects salivary biochemical markers. Free. Radic. Res. 2018, 52, 850–855. [Google Scholar] [CrossRef]
- Menezes, E.F.; Peixoto, L.G.; Teixeira, R.R.; Justino, A.B.; Puga, G.M.; Espindola, F.S. Potential Benefits of Nitrate Supplementation on Antioxidant Defense System and Blood Pressure Responses after Exercise Performance. Oxidative Med. Cell. Longev. 2019, 2019, 7218936. [Google Scholar] [CrossRef]
- Souza, A.V.; Giolo, J.S.; Teixeira, R.R.; Vilela, D.D.; Peixoto, L.G.; Justino, A.B.; Caixeta, D.C.; Puga, G.M.; Espindola, F.S. Salivary and Plasmatic Antioxidant Profile following Continuous, Resistance, and High-Intensity Interval Exercise: Preliminary Study. Oxidative Med. Cell. Longev. 2019, 2019, 5425021. [Google Scholar] [CrossRef]
- Nobari, H.; Nejad, H.A.; Kargarfard, M.; Mohseni, S.; Suzuki, K.; Carmelo Adsuar, J.; Pérez-Gómez, J. The Effect of Acute Intense Exercise on Activity of Antioxidant Enzymes in Smokers and Non-Smokers. Biomolecules 2021, 11, 171. [Google Scholar] [CrossRef]
- Cavas, L.; Arpinar, P.; Yurdakoc, K. Possible interactions between antioxidant enzymes and free sialic acids in saliva: A preliminary study on elite judoists. Int. J. Sports Med. 2005, 26, 832–835. [Google Scholar] [CrossRef] [PubMed]
- Filaire, E.; Massart, A.; Portier, H.; Rouveix, M.; Rosado, F.; Bage, A.S.; Gobert, M.; Durand, D. Effect of 6 Weeks of n-3 Fatty-Acid Supplementation on Oxidative Stress in Judo Athletes. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 496–506. [Google Scholar] [CrossRef]
- Massart, A.; Portier, H.; Rosado, F.; Toumi, H.; Filaire, E. Lipid peroxidation in judoists using oral contraceptives. Int. J. Sports Med. 2012, 33, 781–788. [Google Scholar] [CrossRef]
- Kontorshchikova, K.; Tikhomirova, Y.; Ovchinnikov, A.; Kolegova, T.; Churkina, N.; Kuznetsova, S.Y.; Krylov, V.N. Indices of Free Radical Oxidation in the Oral Fluid as Markers of Athletes’ Functional State. Modern Technol. Med. 2017, 9, 82–85. [Google Scholar] [CrossRef][Green Version]
- Ovchinnikov, A.N.; Deryugina, A.V. Saliva as highly informative substrate for non-invasive analysis of lipoperoxide processes and muscle damage in highly skilled athletes. Klin. Lab. Diagn. 2019, 64, 405–408. [Google Scholar] [CrossRef]
- Podrigalo, L.; Iermakov, S.; Galashko, N.; Galashko, M.; Dzhym, V.Y. Assessment of arm wrestlers’ adaptation status on the base of saliva biochemical characteristics in dynamic of competition and training loads. J. Phys. Educ. Sport 2015, 15, 849. [Google Scholar]
- Mahdivand, A.; Tabar, S.F.; Dehghani, S.; Ebrahimi, F.; Moosavi, S.S.; Ghiri, E.H.; Rezaee, M. The effect of one session Concurrent training on salivary Total antioxidant capacity, IgA and hormonal in male student-athletes. Int. J. Sport Stud. 2013, 3, 448–455. [Google Scholar]
- Sariri, R.; Damirchi, A.; Nazari, Y. Salivary antioxidant variations in athletes after intense exercise. Med. Sport. J. Rom. Sports Med. Soc. 2013, 9, 2043. [Google Scholar]
- Gonzalez, D.; Marquina, R.; Rondon, N.; Rodriguez-Malaver, A.J.; Reyes, R. Effects of aerobic exercise on uric acid, total antioxidant activity, oxidative stress, and nitric oxide in human saliva. Res. Sports Med. 2008, 16, 128–137. [Google Scholar] [CrossRef]
- Viana-Gomes, D.; Rosa, F.L.L.; Mello, R.; Paz, G.A.; Miranda, H.; Salerno, V.P. Oxidative stress, muscle and liver cell damage in professional soccer players during a 2-game week schedule. Sci. Sports 2018, 33, e221–e228. [Google Scholar] [CrossRef]
- Sant’Anna, M.d.L.; Casimiro-Lopes, G.; Boaventura, G.; Marques, S.T.F.; Sorenson, M.M.; Simão, R.; Pinto, V.S. Anaerobic exercise affects the saliva antioxidant/oxidant balance in high-performance pentathlon athletes. Hum. Mov. 2016, 17, 50–55. [Google Scholar] [CrossRef]
- Volodchenko, O.A.; Podrigalo, L.V.; Iermakov, S.S.; Żychowska, M.T.; Jagiełło, W. The Usefulness of Performing Biochemical Tests in the Saliva of Kickboxing Athletes in the Dynamic of Training. BioMed Res. Int. 2019, 2019, 2014347. [Google Scholar] [CrossRef]
- Faelli, E.; Bisio, A.; Codella, R.; Ferrando, V.; Perasso, L.; Panascì, M.; Saverino, D.; Ruggeri, P. Acute and Chronic Catabolic Responses to CrossFit® and Resistance Training in Young Males. Int. J. Environ. Res. Public Health 2020, 17, 7172. [Google Scholar] [CrossRef]
- Tóthová, L.U.; Kamodyová, N.; Červenka, T.; Celec, P. Salivary markers of oxidative stress in oral diseases. Front. Cell. Infect. Microbiol. 2015, 5, 73. [Google Scholar] [CrossRef]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M.; Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef]
- Sies, H. Oxidative stress: Oxidants and antioxidants. Exp. Physiol. 1997, 82, 291–295. [Google Scholar] [CrossRef]
- Devasagayam, T.P.; Tilak, J.C.; Boloor, K.K.; Sane, K.S.; Ghaskadbi, S.S.; Lele, R.D. Free radicals and antioxidants in human health: Current status and future prospects. J. Assoc. Physicians India 2004, 52, 794–804. [Google Scholar]
- Baumert, P.; Lake, M.J.; Stewart, C.E.; Drust, B.; Erskine, R.M. Genetic variation and exercise-induced muscle damage: Implications for athletic performance, injury and ageing. Eur. J. Appl. Physiol. 2016, 116, 1595–1625. [Google Scholar] [CrossRef]
- Silva, J.R.; Rumpf, M.C.; Hertzog, M.; Castagna, C.; Farooq, A.; Girard, O.; Hader, K. Acute and Residual Soccer Match-Related Fatigue: A Systematic Review and Meta-analysis. Sports Med. 2018, 48, 539–583. [Google Scholar] [CrossRef]
- Needleman, I.; Ashley, P.; Fine, P.; Haddad, F.; Loosemore, M.; de Medici, A.; Donos, N.; Newton, T.; van Someren, K.; Moazzez, R.; et al. Consensus statement: Oral health and elite sport performance. Br. Dent. J. 2014, 217, 587–590. [Google Scholar] [CrossRef]
- Hecksteden, A.; Faude, O.; Meyer, T.; Donath, L. How to Construct, Conduct and Analyze an Exercise Training Study? Front. Physiol. 2018, 9, 1007. [Google Scholar] [CrossRef]
- Hopkins, W.G. Sample Size for Individual Responses. J. Appl. Physiol. 2015, 118, 1444–1446. [Google Scholar] [CrossRef] [PubMed]
- McKay, C.D.; Verhagen, E. ‘Compliance’versus ‘adherence’in sport injury prevention: Why definition matters. Br. J. Sports Med. 2016, 50, 382–383. [Google Scholar] [CrossRef]
- Sella, F.; Raz, G.; Cohen Kadosh, R. When randomisation is not good enough: Matching groups in intervention studies. Psychon. Bull. Rev. 2021, 28, 2085–2093. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rating the quality of evidence--study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]


{kind=link}
| Author/Year/Country | Participants | Age (Mean) | Salivary Oxidative Stress Evaluation | Type of Exercise | Results | Main Conclusions |
|---|---|---|---|---|---|---|
| Biagini 2020 Italy | n = 10 swimming athletes | 23 ± 5 years | Carbonyls, isoprostanes e prostanoids [5 min before the test (t0), at the maximal exercise peak (t1), 2.5 (t2), 5 min (t3) and 10 (t4) minutes after the VO2max] Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Incremental cycle ergometer test Workload of 25 W for the first 5 min followed by an increase of 25 W every minute until fatigue 70 rpm | 15-F2t-IsoP (pg/mL): t0: 14 ± 6; t1: 17 ± 7; t2: 12 ± 1; t3: 11 ± 2; t4: 14 ± 2; | The results showed a significant increase in the oxidative stress biomarkers (isoprostanes) during physical exercise with a marked decrease to baseline levels, 10 min after the maximum peak observed in exercise. |
| Cavas, 2005 Turkey | n = 12 males judoists | 18 ± 3.2 years | FSA, SOD, CAT, GSH-Px Two intervals 2 h Pre-test 2 h Post-training Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | 2 h Judo training session | SOD (IU/mg protein)Pre-training: 1.29 ± 0.56; Post-training: 1.83 ± 0.49. CAT (IU/mg protein) Pre-training: 9.12 ± 1.14 Post-training: 16.27 ± 2.56; GSH-Px (IU/mg protein) Pre-training: 1.55 ± 0.05; Post-training: 1.80 ± 0.08. FSA (mg protein/mL) Pre-training: 0.182 ± 0.010; Post-training: 1.80 ± 0.020 | There was an increase of all antioxidant parameters evaluated as well as an increase of FSA levels in saliva. |
| Damirchi, 2015 Iran | n = 16 | 24.7 ± 2.4 years | CAT, SOD, POD Pre- and post-evaluation One hour later With/without loading Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Treadmill run: Warm-up of 3 min (8.05 km/h) and gradient increase of 2.5% every 2 min until exhaustion | Increase of SOD, CAT, POD post-exercise (p < 0.05) with and without loading # | After exhaustive aerobic exercise, the results demonstrate a significant increase in salivary antioxidant enzymes SOD and POD, and CAT activity in response to the rise in free radicals caused by aerobic exercise. |
| Deminice, 2010 Brazil | n = 11 healthy and well-trained males | 25.9 ± 2.8 years | Thiobarbituric acid reactive substances (TBARS), lipid hydroperoxides, advanced oxidation protein products (AOPP), uric acid (UA), Glutathione reduced (GSH), Pre-test/Post-test (10 min) Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Resistance hypertrophy training 3 sets of 10 reps. of bench press, cable pull down, overhead press, leg extension, leg flexion and leg press −75% 1 RM | TBARS (µmol/L): Pre: 2.0 ± 1.2; Post: 2.5 ± 1.2; Lipid hydroperoxides (µ mol H2O2 equivalents/L): Pre: 10.2 ± 2.6; Post: 11.4 ± 4.5; AOPP (µmol chloramine -T equivalents/L): Pre: 30.8 ± 14.8; Post: 37.4 ± 17.5; Uric acid (mg/dL): Pre: 2.1 ± 1.1; Post 3.1 ± 1.1 *; GSH (mml/L): Pre: 0.16 ± 0.03; Post: 0.18 ± 0.01 | After the resistance hypertrophy training, UA levels were significantly higher. However, the other parameters did not present a statistical difference. |
| Faelli, 2020 Italy | n = 20 | CrossFit: 24.6 ± 3.4 years RT: 26.3 ± 3.6 years | Uric acid Cotton swabs and saliva collection tubes ELISA immunosorbent assay | Cross-fit and resistance training (RT) Cross-fit session: 2 min of rest between exercises 4 min of running, jumping rope; pull-ups and squats, front squats and kettlebell swings at 50–60% 1RM RT: 60 min, 3 sets of 15 reps. (i.e., bicep curls, lateral pulldowns, triceps pulldowns, bench presses, military presses, leg extensions, reverse leg curls, and seated leg presses). | Uric acid (mg/dL): CrossFitPre_1: 8.68 ± 0.55; Post_1 11.62 ± 0.36 *; Pre_ 24: 9.18 ± 0.53; Post_24: 12.51± 0.31 * RT Pre_1: 5.42 ± 0.41; Post_1 7.18 ± 0.51 *; Pre_ 24: 6.22 ± 0.38; Post_24: 7.79 ± 0.70 * | Uric acid levels increased in both groups acutely. |
| Filaire 2010 France | n = 20 judo competitors | 22.3 ± 1.4 years | GSH-Px (T1 = before the training session; T2 = after the training session; T3 = after six weeks just before the training session; T4 = after six weeks after the training session) Non-stimulated collection of saliva in tubes Fluorometric high-performance liquid chromatography–HPLC | 2 h—Judo-training session Judospecific skills and drills and randori (fighting practice) with varying intensity of 85–90% of VO2max | GSH-Px (U/g): T1: 48.6 ± 2.5; T2: 54.2 ± 23.5 *; T3: 45.6 ± 3.0; T4: 53.0 ± 2.9 | A significant increase of GSH-Px was detected after the training session (p < 0.05). |
| Gonzalez, 2008 Venezuela | n = 24 | 27.21 ± 9.64 years | UA, TAC, Lipid hydroperoxides, nitrite determination (NO2) Stimulated collection of saliva in tubes (gum chewing) Spectrophotometric evaluation | 10 km race | UA (p = 0.003), TAC increased (p < 0.0001); lipid hydroperoxides decreased (p < 0.0001); NO2 no effect (p > 0.05) # | Aerobic exercise-induced increased both TAC and UA. |
| Kontorshchikova, 2017 Russian Federation | n = 23 track and field athletes, swimming athletes | 18.7 ± 0.6 years | DC, TC, SB Unstimulated collection of saliva in tubes Spectrophotometric evaluation | Anaerobic interval physical exercise 3×100 m distances by a flat race with an active 45 s rest between them for the track and field athletes, 4 × 50 m by the main swimming style with an active rest between the distances also for 45 s for the swimmers. | DC (relative units): Before exercise: 0.29 ± 0.01; After exercise: 0.31 ± 0.02. TC (relative units): Before exercise: 0.35 ± 0.03; After exercise: 0.49 ± 0.04. SB (relative units): Before exercise: 99.94 ± 9.41; After exercise: 189.12 ± 7.69. SB/(DC + TC) (relative units): Before exercise 158.65 ± 9.22; After exercise 237.88 ± 8.84. | There was an increase of lipid peroxidation levels (DC, TC, SB) after physical exercise. |
| Mahdivand, 2013 Iran | n = 20 athlete students | 23 ± 2 years | TAC Non-stimulated collection of saliva in tubes ELISA | Session training concurrent (aerobic and resistance) for 100 min. 10 min warm-up (moderate running and stretching) 20 min of running with 85–80% of maximum heart rate (MHR); 10 min of active recovery; followed by 50 min (opening leg, chest press, back thigh, underarm stretch, triceps and biceps) in three sets of 6–8 repetitions at 85–90% of 1RM; cooling step to 10 min (walking and stretching) | Total antioxidant capacity (µL. mL−1): Before: 1.96 ± 0.199; 1 h After: 1.74 ± 0.222; 24 h After: 1.78 ± 0.217. | Training concurrent (aerobic—resistance) can significantly reduce salivary total antioxidant levels. |
| Massart, 2012 France | n = 28 female judoists | 23.4 ± 1.8 years | MDA, Lipid peroxides (POOL), GPx T1 Pre-test/T2 Post-test 20 min/10 min Non-stimulated collection of saliva in tubes Fluorometric high-performance liquid chromatography—HPLC | Judo training session | Cdmax (UA): NCU: T1: 93.4 ± 9.5; T2: 125.4 ± 11.3; Rmax (UA): NCU: T1: 1.33 ± 0.2; T2: 1.22 ± 0.1; MDA (µg.Ml−1): NCU: T1: 0.04 ± 0.01; T2: 0.07 ± 0.01; POOL: NCU: T1: 278.9 ± 24.6; T2: 378.0 ± 13.9; GPx (U.g−1) NCU: T1: 62.5 ± 4.3; T2: 73.1 ± 2.3. | Training was able to increase the levels of some antioxidants in athletes. |
| Menezes, 2019 Brazil | n = 14 | 22 ± 1 years | NO2–, Alpha-Amylase, Lactate, UA, TAC, TBARS, SOD. Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | acute intense exercise Cycle ergometer 35-watt increments every 2 min and a fixed rotation of 70 rpm until exhaustion At least 30 min of test | NO decrease (p < 0.05) UA increased (p < 0.05) TBARS decrease (p < 0.05) # | There was an increased salivary level of NO, uric acid and total antioxidant capacity (TAC), reduced superoxide dismutase (SOD) activity and TBARS levels. |
| Nobari, 2021 Iran | n = 40 young men | 22.93 ± 1.76 years | POX, SOD, CAT Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Pre- and post-acute intense exercise, and after one hour Treadmill run 8.05 km/h for three minutes. After 3 min the incline was set to 2.5% for every 2 min | POX—F (1, 263.49). p < 001 CAT—F (2135.79). p < 0.001 SOD—F(1.33,108.02) p < 0.001 # | The results demonstrate that intense and acute exercise increases the antioxidant capacity even after one hour after training. |
| Ovchinnikov, 2019 Russia | n = 70; cyclical sports (swimming and athletics) | 16–20 Years | DC, TC, GSH Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Running and swimming training 3 × 100 m distances by a flat race with an active 45 s rest between them for the track and field athletes, 4 × 50 m by the main swimming style with an active rest between the distances also for 45 s for the swimmers. | Swimmers (n = 40) DC Before: 0.28 ± 0.001 After: 0.28 ± 0.002 TC Before: 0.35 ± 0.004 After: 0.37 ± 0.004 * GSH Before: 127.23 ± 3.42 After: 147.24 ± 4.81 * General athletes (n = 30) DC Before: 0.28 ± 0.003 After: 0.29 ± 0.004 * TC Before: 0.33 ± 0.009 After: 0.34 ± 0.008* GSH Before: 89.27 ± 3.59 After: 141.83 ± 7.50 * | Physical activities with maximum power with rest intervals stimulate the generation of MDA and increased levels of GSH for track and field and swim athletes. |
| Podrigalo, 2015 Ukraine | n = 26 weightlifting athletes | 22.13 ± 3.24 years | DC, TC, (TBARS) CAT, SH, GSH Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Group 1- wrestling’s competition 1a: experienced sportsmen; 1b: beginners’ sportsmen group 2- training Competition and dynamic training loads | Malonic dialdehyde (µmol/l): 1a group: Before: 6.86 ± 1.96; After: 4.77 ± 1.03. 1b group: Before: 3.08 ± 0.69, After: 6.85 ± 1.14 *. 2 group: Before: 3.12 ± 0.35; After: 8.18 ± 1.60 * Diene conjugates (µmol/L): 1a group: Before: 41.26 ± 4.78; After: 29.55 ± 3.21 *. 1b group: Before: 27.88 ± 2.87, After: 38.54 ± 3.50 *. 2 group: Before: 28.38 ± 1.11; After: 83.33 ± 9.69 *. CAT (µcat/L) 1a group: Before: 4.28 ± 0.57; After: 4.19 ± 0.39. 1b group: Before: 2.63 ± 0.35, After: 4.98 ± 0.47 *. 2 group: Before: 1.78 ± 0.21; After: 3.91 ± 0.51 GSH (mmol/L): 1a group: Before: 3.18 ± 0.66; After: 3.64 ± 0.57. 1b group: Before: 2.82 ± 0.51, After: 3.45 ± 0.45. 2 group: Before: 1.39 ± 0.20; After: 3.10 ± 0.35 * SH-groups (mmol/L) 1a group: Before: 2.26 ± 0.59; After: 1.68 ± 0.47. 1b group: Before: 1.31 ± 0.34, After: 1.93 ± 0.23. 2nd group: Before: 1.05 ± 0.14; After: 2.36 ± 0.39 * | Bio-chemical criteria of different skillfulness sportsmen illustrate different degree of stability and capacity of adaptation potentials. |
| Rodrigues de Araujo, 2018 Brazil | n = 32 | 21.2 ± 4.2 years | SOD, CAT, GSH, GSSG, TBARS, MDA, Uric Acid Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | high-intensity interval exercise (HIIE) Successive 40 m sprints with direction changes Bangsbo sprint test | TBARs (nmol/mL): Pre: 9.20 ± 3.13; Post: 8.50 ± 2.43; MDA (µM): Pre: 5.40 ± 2.15; Post: 5.37 ± 1.52; GSSG (µM): Pre: 2.04 ± 1.18; Post: 2.10 ± 1.13; Uric acid (mg/dL): Pre: 2.66 ± 1.33; Post: 1.66 ± 0.92 *; SOD (U/g.dL−1): Pre: 32.59 ± 43.88; Post: 37.41 ± 42.05; CAT (U/g.dL−1): Pre: 1.65 ± 1.53; Post: 1.66 ± 2.90. | In terms of redox homeostasis, the authors saw varying findings for TBARs, MDA, GSH, GSSG, CAT, and SOD, while uric acid decreased significantly. |
| Sant’Anna, 2016 Brazil | n = 7 military athletes | 27.1 ± 5.4 years | TBARS, TAC, GSH, UA Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Exercise test (RAST) warm up-5 min + 6 × 35 m sprint. | TBARS (µM): Pre: 0.9 ± 0.2; Post: 1.9 ± 0.2. TAC: It increased by 46.6% after exercise compared to before. GSH: There was no significant change # Uric acid (µM): Pre 178.9 ± 21.4; Post: 293.5 ± 9.4 | RAST triggers free radical production, as evaluated by lipid peroxidation in saliva, and at the same time reveals an increased antioxidant activity as a adaption. |
| Sariri, 2013 Iran | n = 28 male athlete university students | 22.9 ± 1.5 years | UA, CAT, POX, SOD Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Treadmill Run Astrand test at 8.01 km/h | Both enzymatic and non-enzymatic antioxidants increased immediately significantly after exercise. # | Aerobic exercise until exhaustion increases the activity of SOD, catalase, peroxidase in saliva of athlete men. |
| Sari-Sarraf, 2016 Iran | n = 27 | 18–21 years | MDA, TAC Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | a progressive exercise to exhaustion on treadmill | TAC (µmol/mL): Pratice: Pre: 0.79 ± 0.20; Post: 0.88 ± 0.17; Exautive: 0.87 ± 0.21; Control: Pre: 0.77 ± 0.18; Post: 0.79 ± 0.23; Exautive: 0.77 ± 0.23; MDA (nmol/mL): Pratice: Pre: 0.48 ± 0.14; Post: 0.51 ± 0.17; Exautive: 0.54 ± 0.16; Control: Pre: 0.52 ± 0.17; Post: 0.49 ± 0.23; Exautive: 0.46 ± 0.10 | Physical activity promoted an increase in lipid peroxidation and reduced antioxidant capacity, additionally it was observed that the increase in lipid peroxidation was lower in the trained group, demonstrating that physical conditioning can induce a protective effect against lipid peroxidation |
| Sone, 2019 Japan | n = 9 healthy men | 23.8 ± 1.4 years | NO levels Cotton swabs and saliva collection tubes ELISA immunosorbent assay | Cycling After a 10-min warm-up, subjects cycled for 50 min at 80% VO2peak | Nitrite (µmol/L): Pre-exercise: Pre: 447 ± 65; Post 0 h: 353 ± 57; Post 1 h: 367 ± 56; Post 2 h: 355 ± 49; Post 3 h: 303 ± 44. Exercise: Pre: 388 ± 82; Post 0 h: 380 ± 76; Post 1 h: 389 ± 66; Post 2 h: 401 ± 63; Post 3 h: 365 ± 53. | The results demonstrate that salivary NO levels are increased because of exercise-related stress. |
| Souza, 2019 Brazil | n = 13 healthy men | 27.62 ± 1.28 years | NO, TAC, SOD, CAT, GSH, UA Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Resistance exercise (RE): 3 sets of 12-repetition maximum (12- RM) in squat (smith machine), leg press 45°, lying leg curl, and stiff exercises, in that order, with a 2 min recovery interval between sets and exercises. High-Intensity Interval Exercise (HIIE): 1 min cycling bouts at 100% of wVO2max, interspersed with 1 min of passive recovery periods at 40% of VO2max until voluntary exhaustion. The continuous exercise (CE) protocol: continuous cycling for 60 min at 50–60% of wVO2max. | NO decrease (p < 0.05) -RT, HIIE, and CT TAC, SOD, CAT, GSH, UA increased (p < 0.05) for HIIE and CE # | The results demonstrate an increase in the activity levels of amylase, total protein, and salivary nitric oxide. Additionally, in RE showed a small increase in antioxidants, while in HIIE and CE this response was more accentuated. |
| Viana-gomes, 2018 Brazil | n = 8 soccer players | 27.2 ± 5.5 years | TAC, TBARS, UA. Cotton swabs and saliva collection tubes Spectrophotometric evaluation | 48 h post-game-one (day 4): 1-h training session designed to simulate a game 72 h Post-game one (day 5): Resistance training consisted of 3 sets of leg press, leg extensions, leg curls, power cleans and calf raises each with self-suggested recovery intervals between sets and exercises. 24 h post-game two (day 7): low-intensity jogging for15 min (~60% heart rate peak) and low-intensity (i.e., 2 sets per exercise) resistance training over 30 min. | UA (IU/dL) Basal: 2.5 ± 0.3; P-G1: 2.2 ± 0.4; 48 P-G1: 2.5 ± 2.1; P-G2: 2.4 ± 0.8; 24 P-G2: 2.6 ± 2.5; 48 P-G2: 1.5 ± 0.2. TBARS (µmol/L) Basal: 2.1 ± 0.3; P-G1: 3.1 ± 0.4; 48 P-G1: 2.0 ± 0.2; P-G2: 3.4 ± 0.4; 24 P-G2: 2.2 ± 0.3; 48 P-G2: 2.3 ± 0.2. | The results showed an increase in TBARS after both games compared to uric acid reduction after 48 h. The antioxidant capacity did not differ. |
| Volodchenko, 2019 Ukraine | n = 18 kickboxers | 17.29 ± 0.31 years | MDA TBARS, CAT, SOD, Sh-group concentration Non-stimulated collection of saliva in tubes Spectrophotometric evaluation | Training session of 110–130 min warm-up, general development exercises for all muscle groups and exercises stretching (30–35 min); main session block, kicking and striking techniques (40–45 min) and sparring (30–35 min); cool down, breathing and relaxation exercises (10–15 min). | MDA (µmol/L): Before: 4.57 ± 0.25; After: 9.81 ± 0.25 *; Diene conjugates (µmol/L): Before: 24.46 ± 0.31; After: 37.79 ± 0.53 *; CAT (µKat/L): Before: 41.71 ± 0.35; After: 47.85 ± 0.79 *; SH-groups (µmol/L): Before: 2.08 ± 0.16; After: 0.85 ± 0.13 *; SOD Before: 2.07 ± 0.17; After:3.48 ± 0.24 *; | Increased levels of MDA, DC, SH were found after training session. Antioxidant parameters were also reported with elevated levels. |
| Risk of bias | Biagini, 2020 | Damirchi, 2015 | Faelli, 2020 | Filaire. 2010 | Massart, 2012 | Menezes, 2019 | Nobari, 2021 | Ovchinnikov, 2019 | Sari-Sarraf, 2016 | Sone, 2019 | Souza, 2019 | Viana-Gomes, 2018 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Quality Rating | POOR | GOOD | GOOD | GOOD | GOOD | GOOD | GOOD | GOOD | POOR | POOR | GOOD | GOOD |
| Risk of bias | Cavas, 2005 | Gonzalez, 2008 | Deminice, 2010 | Mahdivand, 2013 | Sariri, 2013 | Podrigalo, 2015 | Sant’anna, 2016 | Kontorschikova, 2017 | De Araújo, 2018 | Volodchenko, 2019 | ||
| Quality Rating | FAIR | POOR | GOOD | FAIR | FAIR | FAIR | FAIR | FAIR | GOOD | FAIR | ||
| Certainty Assessment | Impact | Certainty | Importance | ||||||
|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | |||
| Lipid peroxidation after exercise | |||||||||
| 8 | observational studies | not serious | serious a | not serious | serious b | all plausible residual confounding would reduce the demonstrated effect | Lipid peroxidation was evaluated by different methods (TBARS, Diene and triene conjugates, isoprostanes). Six studies showed increased levels of lipid peroxidation after sessions of exercise while two studies did not. Limitations regarding sample size may affected results with no differences. | ⨁◯◯◯Very low | IMPORTANT |
| Nitrite levels after exercise | |||||||||
| 2 | observational studies | not serious | serious c | not serious | serious d | all plausible residual confounding would reduce the demonstrated effect | Higher nitrite levels in saliva were found in studies. However, absence of other evaluations compromised global analysis of oxidative balance. Exercise effects related to nitrite levels may suffer alterations by cofounding factors | ⨁◯◯◯Very low | IMPORTANT |
| Antioxidant parameters after exercise | |||||||||
| 14 | observational studies | not serious | serious e | not serious | serious f | all plausible residual confounding would reduce the demonstrated effect | Evaluation of antioxidant parameters was the predominant analysis. Different methods were employed (GSH, TAC, CAT, SOD) leading to high heterogeneity. Some authors did not performed global analysis of oxidant parameters and difficult to assess real effects of exercise. Reduced sample sizes and absence of cofounding factors also compromised oxidative stress evaluation in salivary content | ⨁◯◯◯Very low | IMPORTANT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves, R.C.C.; Ferreira, R.O.; Frazão, D.R.; de Souza Né, Y.G.; Mendes, P.F.S.; Marañón-Vásquez, G.; Royes, L.F.F.; Fagundes, N.C.F.; Maia, L.C.; Lima, R.R. The Relationship between Exercise and Salivary Oxidative Stress: A Systematic Review. Antioxidants 2022, 11, 1489. https://doi.org/10.3390/antiox11081489
Alves RCC, Ferreira RO, Frazão DR, de Souza Né YG, Mendes PFS, Marañón-Vásquez G, Royes LFF, Fagundes NCF, Maia LC, Lima RR. The Relationship between Exercise and Salivary Oxidative Stress: A Systematic Review. Antioxidants. 2022; 11(8):1489. https://doi.org/10.3390/antiox11081489
Chicago/Turabian StyleAlves, Raphael Charchar Campos, Railson Oliveira Ferreira, Deborah Ribeiro Frazão, Yago Gecy de Souza Né, Paulo Fernando Santos Mendes, Guido Marañón-Vásquez, Luiz Fernando Freire Royes, Nathalia Carolina Fernandes Fagundes, Lucianne Cople Maia, and Rafael Rodrigues Lima. 2022. "The Relationship between Exercise and Salivary Oxidative Stress: A Systematic Review" Antioxidants 11, no. 8: 1489. https://doi.org/10.3390/antiox11081489
APA StyleAlves, R. C. C., Ferreira, R. O., Frazão, D. R., de Souza Né, Y. G., Mendes, P. F. S., Marañón-Vásquez, G., Royes, L. F. F., Fagundes, N. C. F., Maia, L. C., & Lima, R. R. (2022). The Relationship between Exercise and Salivary Oxidative Stress: A Systematic Review. Antioxidants, 11(8), 1489. https://doi.org/10.3390/antiox11081489