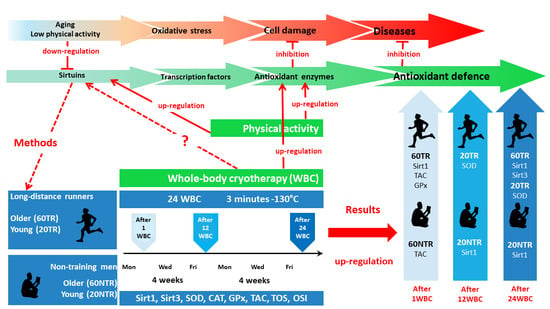
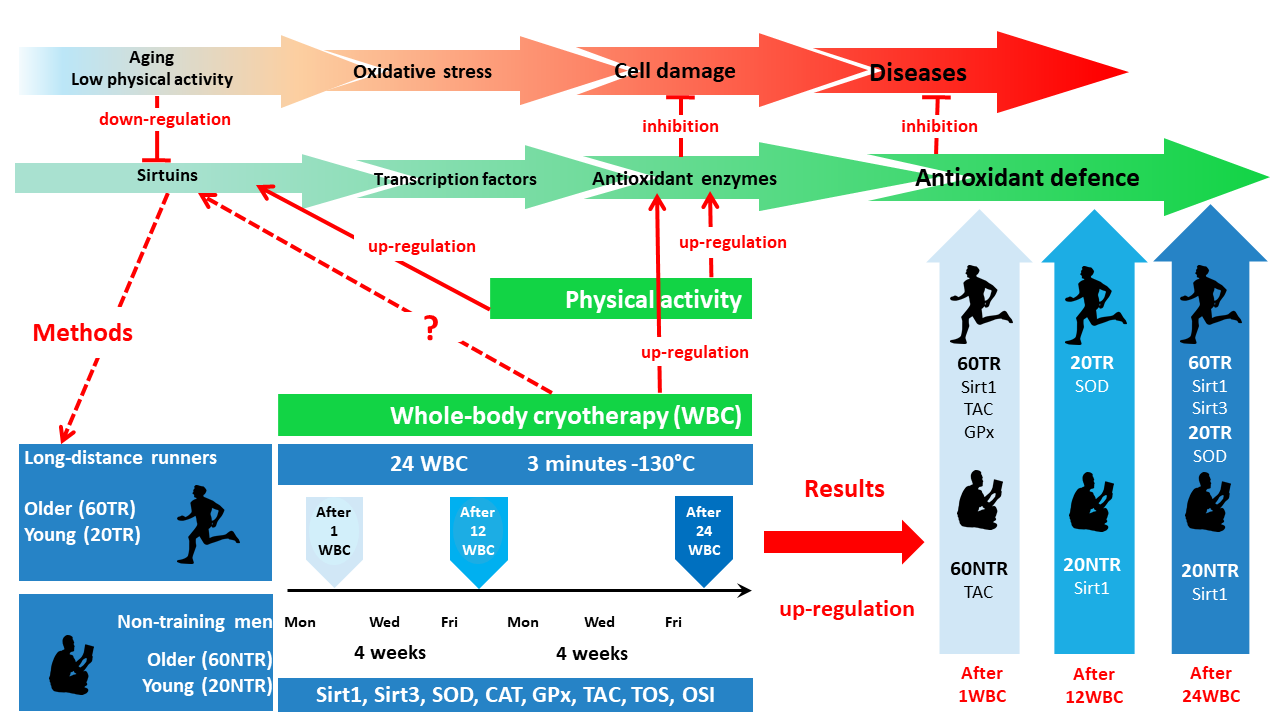
The Effect of Repeated Whole-Body Cryotherapy on Sirt1 and Sirt3 Concentrations and Oxidative Status in Older and Young Men Performing Different Levels of Physical Activity

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
- (1)
- 60 TR, older training men (training experience 6.71 ± 5.79 years),
- (2)
- 60 NTR, older non-training men,
- (3)
- 20 TR, young training men (training experience 3.35 ± 1.83 years),
- (4)
- 20 NTR, young non-training men.
2.3. Whole-Body Cryotherapy
2.4. Somatic Measurements
2.5. Biochemical Analysis
2.6. Assessment of Physical Activity
2.7. Assessment of Nutritional Behaviour
2.8. Statistical Analysis
3. Results
3.1. Influence of WBC on the Level of Sirtuins and Markers of Oxidative Stress in Older Males
3.2. Influence of WBC on the Level of Sirtuins and Markers of Oxidative Stress in Young Males
3.3. Correlations
3.3.1. Correlations between the Concentrations of Sirtuins and Pro-Oxidative-Antioxidant Markers in Training and Non-Training Men
3.3.2. Correlations between Sirtuin Concentration and the Level of Physical Activity in Training and Non-Training Men
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing. Available online: https://www.who.int/health-topics/ageing#tab=tab_1 (accessed on 19 October 2020).
- Bielak-Zmijewska, A.; Grabowska, W.; Przybylska, D. Impact of cellular senescence on organismal aging and age-related diseases. Postepy Biochem. 2014, 60, 147–160. [Google Scholar] [PubMed]
- Kumar, R.; Cheterjee, P.; Sharma, P.K.; Singh, A.K.; Gupta, A.; Gill, K.; Tripathi, M.; Dey, A.B.; Dey, S. Sirtuin 1: Promising serum protein marker for early detection of Alzheimer’s disease. PLoS ONE 2013, 8, e61560. [Google Scholar] [CrossRef]
- Villanova, L.; Vernucci, E.; Pucci, B. Influence of age and physical exercise on sirtuin activity in humans. J. Biol. Regul. Homeost. Agents 2013, 27, 497–507. [Google Scholar] [PubMed]
- Wendling, D.; Abbas, W.; Godfrin-Valnet, M.; Kumar, A.; Guillot, X.; Khan, K.A.; Vidon, C.; Coquard, L.; Toussirot, E.; Prati, C.; et al. Dysregulated serum IL-23 and SIRT1 activity in peripheral blood mononuclear cells of patients with rheumatoid arthritis. PLoS ONE 2015, 10, e0119981. [Google Scholar] [CrossRef] [PubMed]
- Piotrowska, A.; Bartnik, E. The role of reactive oxygen species and mitochondria in aging. Postepy Biochem. 2014, 60, 240–247. [Google Scholar] [PubMed]
- Sies, H. Oxidative stress: Oxidants and antioxidants. Exp. Physiol. 1997, 82, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Kasapoglu, M.; Ozben, T. Alterations of antioxidant enzymes and oxidative stress markers in aging. Exp. Gerontol. 2001, 36, 209–220. [Google Scholar] [CrossRef]
- Kumawat, M.; Sharma, T.K.; Singh, I.; Singh, N.; Singh, S.K.; Ghalaut, V.S.; Shankar, V.; Vardey, S.K. Decrease in antioxidant status of plasma and erythrocytes from geriatric population. Dis. Markers 2012, 33, 303–308. [Google Scholar] [CrossRef][Green Version]
- Güney, S.; Cumaoğlu, A.; Öztürk, G.; Akbulut, K.G.; Karasu, Ç. Comparison of melatonin effect on oxidant Status and antioxidant capacity in liver and heart of young and aged rats. Int. J. Gerontol. 2013, 7, 45–49. [Google Scholar] [CrossRef]
- Suresh, D.R.; Kumaran, S.; Annam, V.; Veena, H. Age related changes in malondialdehyde: Total antioxidant capacity ratio—A novel marker of oxidative stress. Int. J. Pharm. Bio Sci. 2010, 1, 1–6. [Google Scholar]
- Jackson, M.J.; McArdle, A. Age-related changes in skeletal muscle reactive oxygen species generation and adaptive responses to reactive oxygen species. J. Physiol. 2011, 589, 2139–2145. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity: Implications for metabolic syndrome, diabetes, hypertension, dyslipidemia, atherosclerosis, and cancer. Obes. Res. Clin. Pract. 2013, 7, e330–e341. [Google Scholar] [CrossRef] [PubMed]
- Panth, N.; Paudel, K.R.; Parajuli, K. Reactive oxygen species: A key hallmark of cardiovascular disease. Adv. Med. 2016, 2016. [Google Scholar] [CrossRef]
- Jiang, T.; Sun, Q.; Chen, S. Oxidative stress: A major pathogenesis and potential therapeutic target of antioxidative agents in Parkinson’s disease and Alzheimer’s disease. Prog. Neurobiol. 2016, 147, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Ohl, K.; Tenbrock, K.; Kipp, M. Oxidative stress in multiple sclerosis: Central and peripheral mode of action. Exp. Neurol. 2016, 277, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.; Mazur, M.; Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef] [PubMed]
- Bjork, L.; Jenkins, N.T.; Witkowski, S.; Hagberg, J.M. Circulating biomarkers of nitro-oxidative stress biomarkers in active and inactive men. Int. J. Sports Med. 2012, 33, 279–284. [Google Scholar]
- Lubkowska, A.; Dolegowska, B.; Szygula, Z. Whole-body cryostimulation—Potential beneficial treatment for improving antioxidant capacity in healthy men—Significance of the number of sessions. PLoS ONE 2012, 7, e46352. [Google Scholar] [CrossRef]
- Mila-Kierzenkowska, C.; Jurecka, A.; Wozniak, A.; Szpinda, M.; Augustynska, B.; Wozniak, B. The effect of submaximal exercise preceded by single whole-body cryotherapy on the markers of oxidative stress and inflammation in blood of volleyball players. Oxid. Med. Cell. Longev. 2013, 2013, 409567. [Google Scholar] [CrossRef]
- Miller, E.; Mrowicka, M.; Malinowska, K.; Kedziora, J.; Majsterek, I. The effects of whole-body cryotherapy and melatonin supplementation on total antioxidative status and some antioxidative enzymes in multiple sclerosis patients. Polski Merkuriusz Lekarski Organ Polskiego Towarzystwa Lekarskiego 2011, 31, 150–153. [Google Scholar]
- Miller, E.; Mrowicka, M.; Malinowska, K.; Mrowicki, J.; Saluk-Juszczak, J.; Kedziora, J. Effects of whole-body cryotherapy on a total antioxidative status and activities of antioxidative enzymes in blood of depressive multiple sclerosis patients. World J. Biol. Psychiatry 2011, 12, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, A.; Wozniak, B.; Drewa, G. The influence of whole-body cryostimulation on blood enzymatic antioxidant barrier of kayakers during training. Med. Sport. 2007, 23, 207–214. [Google Scholar]
- Stanek, A.; Sieron, A. Contemporary whole-body cryotherapy in wellness. Ann. Acad. Med. Siles 2012, 66, 64–70. [Google Scholar]
- Lubkowska, A.; Chudecka, M.; Klimek, A.; Szygula, Z.; Fraczek, B. Acute effect of a single whole-body cryostimulation on prooxidant–antioxidant balance in blood of healthy, young men. J. Therm. Biol. 2008, 33, 464–467. [Google Scholar] [CrossRef]
- Stanek, A.; Romuk, E.; Wielkoszynski, T.; Bartus, S.; Cieslar, G.; Cholewka, A. Decreased lipid profile and oxidative stress in healthy subjects who underwent whole-body cryotherapy in closed cryochamber with subsequent kinesiotherapy. Oxid. Med. Cell. Longev. 2019, 2019, 7524878. [Google Scholar] [CrossRef]
- Lawson, M.; Uciechowska, U.; Schemies, J.; Rumpf, T.; Jung, M.; Sippl, W. Inhibitors to understand molecular mechanisms of NAD(+)-dependent deacetylases (sirtuins). Biochim. Biophys. Acta 2010, 1799, 726–739. [Google Scholar] [CrossRef]
- Merksamer, P.I.; Liu, Y.; He, W.; Hirschey, M.D.; Chen, D.; Verdin, E. The sirtuins, oxidative stress and aging: An emerging link. Aging 2013, 5, 144–150. [Google Scholar] [CrossRef]
- Kucinska, M.; Piotrowska, H.; Murias, M. Sirtuins—Modulation of their activity as a novel therapeutic target. Polski Merkuriusz Lekarski Organ Polskiego Towarzystwa Lekarskiego 2010, 28, 231–235. [Google Scholar]
- Pardo, P.S.; Boriek, A.M. The physiological roles of Sirt1 in skeletal muscle. Aging 2011, 3, 430–437. [Google Scholar] [CrossRef]
- Sack, M.N.; Finkel, T. Mitochondrial metabolism, sirtuins, and aging. Cold Spring Harb. Perspect. Biol. 2012. [Google Scholar] [CrossRef]
- Chang, H.C.; Guarente, L. SIRT1 and other sirtuins in metabolism. Trends Endocrinol. Metab. 2014, 25, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Denu, J.M.; Gottesfeld, J.M. Minireview series on sirtuins: From biochemistry to health and disease. J. Biol. Chem. 2012, 287, 42417–42418. [Google Scholar] [CrossRef] [PubMed]
- Parihar, P.; Solanki, I.; Mansuri, M.L.; Parihar, M.S. Mitochondrial sirtuins: Emerging roles in metabolic regulations, energy homeostasis and diseases. Exp. Gerontol. 2015, 61, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Togliatto, G.; Gambino, R.; Ponzo, V.; Lombardo, G.; Rosato, R.; Cassader, M.; Brizzi, M.F. Impact of sirtuin-1 expression on H3K56 acetylation and oxidative stress: A double-blind randomized controlled trial with resveratrol supplementation. Acta Diabetol. 2018, 55, 331–340. [Google Scholar] [CrossRef]
- Johnson, M.L.; Irving, B.A.; Lanza, I.R.; Vendelbo, M.H.; Konopka, A.R.; Robinson, M.M.; Henderson, G.C.; Klaus, K.A.; Morse, D.M.; Heppelmann, C.; et al. Differential effect of endurance training on mitochondrial protein damage, degradation, and acetylation in the context of aging. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1386–1393. [Google Scholar] [CrossRef]
- Bordone, L.; Guarente, L. Calorie restriction SIRT1 and metabolism: Understanding longevity. Nat. Rev. Mol. Cell Biol. 2005, 6, 298–305. [Google Scholar] [CrossRef]
- Vargas-Ortiz, K.; Pérez-Vázquez, V.; Macías-Cervantes, M.H. Exercise and sirtuins: A way to mitochondrial health in skeletal muscle. Int. J. Mol. Sci. 2019, 20, 2717. [Google Scholar] [CrossRef]
- Perovic, A.; Unic, A.; Dumic, J. Recreational scuba diving: Negative or positive effects of oxidative and cardiovascular stress? Biochem. Med. 2014, 24, 235–247. [Google Scholar] [CrossRef]
- Shi, T.; Wang, F.; Stieren, E.; Tong, Q. SIRT3, a mitochondrial sirtuin deacetylase, regulates mitochondrial function and thermogenesis in brown adipocytes. J. Biol. Chem. 2005, 280, 13560–13567. [Google Scholar] [CrossRef]
- Lubkowska, A.; Szygula, Z.; Klimek, A.; Torii, M. Do sessions of cryostimulation have influence on white blood cell count, level of IL6 and total oxidative and antioxidative status in healthy men? Eur. J. Appl. Physiol. 2010, 109, 67–72. [Google Scholar] [CrossRef]
- Sutkowy, P.; Augustynska, B.; Wozniak, A.; Rakowski, A. Physical exercise combined with whole-body cryotherapy in evaluating the level of lipid peroxidation products and other oxidant stress indicators in kayakers. Oxid. Med. Cell. Longev. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Szpotowicz-Czech, B.; Wiecek, M.; Szymura, J.; Maciejczyk, M.; Szygula, Z. Changes in chosen immune system indicators and the level of HSP-70 after single whole-body cryostimulation in healthy men. Cent. Eur. J. Immunol. 2018, 43, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Szymura, J.; Wiecek, M.; Maciejczyk, M.; Gradek, J.; Kantorowicz, M.; Szygula, Z. Unchanged erythrocyte profile after exposure to cryogenic temperatures in elder marathon runners. Front. Physiol. 2018, 9, 659. [Google Scholar] [CrossRef] [PubMed]
- Wiecek, M.; Szymura, J.; Sproull, J.; Szygula, Z. Decreased blood asprosin in hyperglycemic menopausal women as a result of whole-body cryotherapy regardless of metabolic syndrome. J. Clin. Med. 2019, 8, 1428. [Google Scholar] [CrossRef] [PubMed]
- Wiecek, M.; Szymura, J.; Sproull, J.; Szygula, Z. Whole-body cryotherapy is an effective method of reducing abdominal obesity in menopausal women with metabolic syndrome. J. Clin. Med. 2020, 9, 2797. [Google Scholar] [CrossRef] [PubMed]
- Stanek, A.; Sieron-Stoltny, K.; Romuk, E.; Cholewka, A.; Wielkoszynski, T.; Cieslar, G.; Kwiatek, S.; Sieron, A.; Kawczyk-Krupka, A. Whole-body cryostimulation as an effective method of reducing oxidative stress in healthy men. Adv. Clin. Exp. Med. 2016, 25, 1281–1291. [Google Scholar] [CrossRef]
- Mansur, A.P.; Roggerio, A.; Goes, M.F.S.; Avakian, S.D.; Leal, D.P.; Maranhão, R.C.; Strunz, C.M.C. Serum concentrations and gene expression of sirtuin 1 in healthy and slightly overweight subjects after caloric restriction or resveratrol supplementation: A randomized trial. Int. J. Cardiol. 2017, 227, 788–794. [Google Scholar] [CrossRef]
- Gliemann, L.; Schmidt, J.F.; Olesen, J.; Biensø, R.S.; Peronard, S.L.; Grandjean, S.U.; Mortensen, S.P.; Nyberg, M.; Bangsbo, J.; Pilegaard, H.; et al. Resveratrol blunts the positive effects of exercise training on cardiovascular health in aged men. J. Physiol. 2013, 591, 5047–5059. [Google Scholar] [CrossRef]
- Pacifici, F.; Di Cola, D.; Pastore, D.; Abete, P.; Guadagni, F.; Donadel, G.; Bellia, A.; Esposito, E.; Salimei, C.; Sinibaldi Salimei, P.; et al. Proposed tandem effect of physical activity and sirtuin 1 and 3 activation in regulating glucose homeostasis. Int. J. Mol. Sci. 2019, 20, 4748. [Google Scholar] [CrossRef]
- Lanza, I.R.; Short, D.K.; Short, K.R.; Raghavakaimal, S.; Basu, R.; Joyner, M.J.; McConnell, J.P.; Nair, K.S. Endurance exercise as a countermeasure for aging. Diabetes 2008, 57, 2933–2942. [Google Scholar] [CrossRef]
- Sarkin, J.; Campbell, J.; Gross, L.; Roby, J.; Bazzo, S.; Sallis, J.; Calfas, K. Project GRAD seven-day physical activity recall interviewer’s manual. Med. Sci. Sports Exerc. 1997, 29, S91–S102. [Google Scholar]
- Szponar, L.; Wolnicka, K.; Rychli, E. Album of Photographs of Food Products and Dishes; Institute of Food and Nutrition: Warsaw, Poland, 2000; pp. 1–82. [Google Scholar]
- Fritz, C.O.; Morris, P.E. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W. Sadly, the earth is still round (p < 0.05). J. Sport Health Sci. 2012, 1, 9–11. [Google Scholar] [CrossRef]
- Sutkowy, P.; Wozniak, A.; Rajewski, P. Single whole-body cryostimulation procedure versus single dry sauna bath: Comparison of oxidative impact on healthy male volunteers. BioMed Res. Int. 2015, 2015, 406353. [Google Scholar] [CrossRef] [PubMed]
- Lubkowska, A.; Dolegowska, B.; Szygula, Z.; Klimek, A. Activity of selected enzymes in erythrocytes and level of plasma antioxidants in response to single whole-body cryostimulation in humans. Scand. J. Clin. Lab. Investig. 2009, 69, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Sutkowy, P.; Wozniak, A.; Mila-Kierzenkowska, C.; Jurecka, A. The concentration of thiobarbituric acid reactive substances (TBARS) and vitamins A and E in blood of amateur athletes after single whole-body cryostimulation. Med. Sport. 2011, 1, 43–54. [Google Scholar]
- Dugué, B.; Smolander, J.; Westerlund, T.; Oksa, J.; Nieminen, R.; Moilanen, E.; Mikkelsson, M. Acute and long-term effects of winter swimming and whole-body cryotherapy on plasma antioxidative capacity in healthy women. Scand. J. Clin. Lab. Investig. 2005, 65, 395–402. [Google Scholar] [CrossRef]
- Hirvonen, H.; Kautiainen, H.; Moilanen, E.; Mikkelsson, M.; Leirisalo-Repo, M. The effect of cryotherapy on total antioxidative capacity in patients with active seropositive rheumatoid arthritis. Rheumatol. Int. 2017, 37, 1481–1487. [Google Scholar] [CrossRef]
- Kilic, U.; Gok, O.; Erenberk, U.; Dundaroz, M.R.; Torun, E.; Kucukardali, Y.; Elibol-Can, B.; Uysal, O.; Dundar, T. A remarkable age-related increase in SIRT1 protein expression against oxidative stress in elderly: SIRT1 gene variants and longevity in human. PLoS ONE 2015, 10, e0117954. [Google Scholar] [CrossRef]
- Koltai, E.; Bori, Z.; Osvath, P.; Ihasz, F.; Peter, S.; Toth, G.; Degens, H.; Rittweger, J.; Boldogh, I.; Radak, Z. Master athletes have higher miR-7, SIRT3 and SOD2 expression in skeletal muscle than age-matched sedentary controls. Redox Biol. 2018, 19, 46–51. [Google Scholar] [CrossRef]
- Gurd, B.J.; Perry, C.G.; Heigenhauser, G.J.; Spriet, L.L.; Bonen, A. High-intensity interval training increases SIRT1 activity in human skeletal muscle. Appl. Physiol. Nutr. Metab. 2010, 35, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Radak, Z.; Bori, Z.; Koltai, E.; Fatouros, I.G.; Jamurtas, A.Z.; Douroudos, I.I.; Terzis, G.; Nikolaidis, M.G.; Chatzinikolaou, A.; Sovatzidis, A.; et al. Age-dependent changes in 8-oxoguanine-DNA glycosylase activity are modulated by adaptive responses to physical exercise in human skeletal muscle. Free Radic Biol. Med. 2011, 51, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, A.; Wozniak, B.; Drewa, G.; Mila-Kierzenkowska, C.; Rakowski, A.; Porzych, M. Lipid peroxidation in blood of kayakers after whole-body cryostimulation and training. Med. Sport. 2007, 1, 15–22. [Google Scholar]
- Zhang, B.; Cui, S.; Bai, X.; Zhuo, L.; Sun, X.; Hong, Q.; Fu, B.; Wang, J.; Chen, X.; Cai, G. SIRT3 overexpression antagonizes high glucose accelerated cellular senescence in human diploid fibroblasts via the SIRT3-FOXO1 signaling pathway. Age 2013, 35, 2237–2253. [Google Scholar] [CrossRef]
- Bayod, S.; Del Valle, J.; Lalanza, J.F.; Sanchez-Roige, S.; de Luxán-Delgado, B.; Coto-Montes, A.; Canudas, A.M.; Camins, A.; Escorihuela, R.M.; Pallàs, M. Long-term physical exercise induces changes in sirtuin 1 pathway and oxidative parameters in adult rat tissues. Exp. Gerontol. 2012, 47, 925–935. [Google Scholar] [CrossRef]
- Little, J.P.; Safdar, A.; Wilkin, G.P.; Tarnopolsky, M.A.; Gibala, M.J. A practical model of low-volume high-intensity interval training induces mitochondrial biogenesis in human skeletal muscle: Potential mechanisms. J. Physiol. 2010, 588, 1011–1022. [Google Scholar] [CrossRef]

{kind=link}
| Variable | 60 TR | 60 NTR | 20 TR | 20 NTR |
|---|---|---|---|---|
| RBC (106/µL) | 4.75 ± 0.55 | 4.93 ± 0.41 | 4.96 ± 0.33 | 5.21 ± 0.28 |
| HGB (g/dL) | 14.52 ± 1.17 | 15.18 ± 1.19 | 14.68 ± 0.93 | 15.97 ± 0.70 * |
| HCT (%) | 42.47 ± 3.02 | 44.25 ± 3.30 | 43.23 ± 2.57 | 46.27 ± 2.14 * |
| PLT (103/µL) | 229.5 (213–258) | 199.5 (183–299) | 241.5 (226–286) | 212.0 (200–226) * |
| LEUC (103/µL) | 6.2 (4.9–7.7) | 6.4 (5.4–7.9) | 5.46 (4.9–7.13) | 7.09 (5.23–8) |
| NEUT (%) | 53.86 ± 8.46 | 56.26 ± 11.55 | 49.56 ± 13.11 | 49.70 ± 14.03 |
| LYMPH (%) | 33.00 ± 8.97 | 32.20 ± 10.74 | 35.89 ± 10.61 | 36.91 ± 13.18 |
| MONO (%) | 9.40 ± 2.20 | 9.31 ± 2.09 | 9.85 ± 2.66 | 9.47 ± 1.53 |
| EOS (%) | 1.85 (1.6–4.3) | 1.7 (1.2–2.4) # | 3.3 (2.2–5.1) | 3.2 (2.2-4.0) |
| BASO (%) | 0.73 ± 0.19 | 0.54 ± 0.30 | 0.73 ± 0.47 | 0.72 ± 0.31 |
| Glucose (mmol/L) | 5.27 (5.03–5.46) | 5.34 (5.19–5.7) # | 5.02 (4.73–5.16) | 4.82 (4.67–4.94) |
| HbA1C (%) | 5.5 (5.3–5.5) # | 5.3 (4.8–5.4) | 5.2 (5–5.4) | 5.25 (5.2–5.4) |
| CHOL (mmol/L) | 5.33 ± 1.00 # | 4.97 ± 1.04 | 4.24 ± 1.03 | 4.19 ± 1.04 |
| HDL (mmol/L) | 1.83 ± 0.29 | 1.43 ± 0.46 * | 1.61 ± 0.28 | 1.47 ± 0.45 |
| LDL (mmol/L) | 3.08 (2.47–3.66) # | 3.36 (2.56–3.89) | 1.82 (1.66–2.71) | 2.34 (1.94–2.57) |
| TG (mmol/L) | 0.91 ± 0.32 | 1.01 ± 0.35 | 0.78 ± 0.24 | 0.87 ± 0.25 |
| SBP (mmHg) | 128.00 ± 12.29 | 130.56 ± 18.45 | 120.50 ± 16.24 | 120.50 ± 13.83 |
| DBP (mmHg) | 79.50 ± 6.85 | 82.22 ± 11.21 # | 74.50 ± 9.56 | 70.50 ± 7.98 |
| Variable | 60 TR | 60 NTR | 20 TR | 20 NTR |
|---|---|---|---|---|
| Age (years) | 55.5 (51–59) # | 61.5 (58–68) *, # | 23 (21–24) | 21.5 (21–22) |
| BM (kg) | 76.33 ± 6.32 | 77.59 ± 8.21 | 77.28 ± 11.11 | 77.67 ± 6.96 |
| BMI (kg/m2) | 24.87 ± 1.28 | 27.28 ± 2.32 *, # | 23.65 ± 2.51 | 23.74 ± 2.20 |
| PBF (%) | 21.33 ± 4.36 # | 26.40 ± 5.20 # | 16.58 ± 5.78 | 16.09 ± 5.17 |
| LBM (kg) | 60.11 ± 6.62 | 56.52 ± 8.28 *, # | 64.39 ± 10.06 | 65.16 ± 6.69 |
| Variable | Group | Pre 1 WBC | After 1 WBC | After 12 WBC | After 24 WBC | WBC Influence p (Effect Size η2) | ||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 2-1 | 3-1 | 4-1 | ||
| Sirt1 | 60 TR | 1.93 (1.56, 2.40) | 2.67 (1.97, 3.24) | 2.39 (1.42, 3.96) | 2.98 (1.82, 3.68) | 0.03 (0.48) | 0.17 (0.19) | 0.01 (0.73) |
| (ng/mL) | 60 NTR | 2.93 (1.70, 3.94) | 3.45 (1.35, 5.52) | 4.16 (2.06, 5.65) | 3.39 (2.23, 5.03) | 0.29 (0.11) | 0.39 (0.08) | 0.58 (0.03) |
| Sirt3 | 60 TR | 1.11 (1.05, 1.64) | 1.18 (1.04, 1.65) | 1.18 (0.92, 1.52) | 1.69 (1.11, 1.91) | 0.72 (0.01) | 0.44 (0.06) | 0.01 (0.79) |
| (ng/mL) | 60 NTR | 1.09 (0.87, 1.17) | 0.97 (0.79, 1.16) * | 0.92 (0.81, 1.14) | 1.06 (0.87, 1.13) * | 0.96 (0.00) | 0.20 (0.16) | 0.88 (0.00) |
| SOD | 60 TR | 88.29 (79.07, 91.41) | 90.81 (72.45, 98.58) | 93.12 (86.49, 100.5) | 89.11 (83.41, 94.89) | 0.07 (0.32) | 0.45 (0.06) | 0.88 (0.00) |
| (U/mL) | 60 NTR | 88.91 (81.93, 94.89) | 95.12 (93.12, 100.5) | 96.71(90.09,104.48) | 90.56 (83.66, 100.5) | 0.39 (0.08) | 0.51 (0.04) | 0.72 (0.01) |
| GPx | 60 TR | 1.08 (0.94, 1.42) | 1.19 (1.02, 1.36) | 1.15 (0.88, 1.36) | 1.18 (0.91, 1.31) | 0.05 (0.40) | 0.28 (0.11) | 0.30 (0.09) |
| (µmol/min/mL) | 60 NTR | 1.15 (1.04, 1.39) | 1.11 (1.04, 1.42) | 1.22 (0.96, 1.47) | 1.16 (0.10, 1.44) | 0.88 (0.00) | 0.61 (0.03) | 0.88 (0.00) |
| CAT | 60 TR | 126.57 (103.4, 129.2) | 133.1 (114.6, 140.5) | 123.14 (101.7, 138.9) | 108.56 (88.8, 122.2) | 0.20 (0.16) | 0.88 (0.00) | 0.44 (0.06) |
| (nmol/min/mL) | 60 NTR | 123.54 (105.4, 139.2) | 131.62 (121.0, 139.4) | 125.02 (97.1, 146.2) | 119.37 (105.1, 28.4) | 0.33 (0.09) | 0.51 (0.04) | 0.80 (0.01) |
| TAC | 60 TR | 340.46 (307.75, 356.17) | 383.81 (369.26, 393.83) | 319.30 (291.12, 352.38) | 355.01 (339.30, 361.18) | 0.01 (0.79) | 0.80 (0.01) | 0.11 (0.25) |
| (μmol/L) | 60 NTR | 360.63 (320.71, 378.67) | 386.19 (365.22, 396.65) | 357.03 (288.92, 37892) | 353.36 (306.40, 386.50) | 0.04 (0.44) | 0.51 (0.04) | 0.80 (0.01) |
| TOS | 60 TR | 381.42 (298.43, 427.28) | 342.27 (273.37, 469.79) | 364.42 (328.85, 459.05) | 362.85 (291.71, 461.73) | 0.88 (0.00) | 0.39 (0.08) | 0.88 (0.00) |
| (μmol/L) | 60 NTR | 351.22 (293.06, 433.99) | 389.48 (300.66, 429.07) | 366.88 (319.01, 476.94) | 400.66 (320.80, 508.48) | 0.33 (0.09) | 0.88 (0.00) | 0.39 (0.08) |
| OSI | 60 TR | 1.14 (1.04, 1.25) | 0.96 (0.73, 1.24) | 1.08 (0.94, 1.57) | 0.98 (0.85, 1.46) | 0.06 (0.36) | 0.33 (0.09) | 0.65 (0.00) |
| 60 NTR | 1.13 (0.82, 1.22) | 1.03 (0.76, 1.13) | 1.16 (0.95, 1.52) | 1.29 (1.01, 1.45) | 0.24 (0.14) | 0.58 (0.03) | 0.28 (0.11) | |
| Variable | Group | Pre 1 WBC | After 1 WBC | After 12 WBC | After 24 WBC | WBC Influence p (Effect Size η2) | ||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 2-1 | 3-1 | 4-1 | ||
| Sirt1 | 20 TR | 1.94 (1.44, 3.26) | 1.79 (1.25, 3.32) | 2.81 (1.46, 3.51) | 2.93 (1.57, 3.73) | 0.96 (0.04) | 0.58 (0.11) | 0.45 (0.01) |
| (ng/mL) | 20 NTR | 1.71 (1.31, 3.47) | 2.89 (1.44, 3.64) | 3.16 (2.08, 4.22) | 3.48 (2.85, 5.44) | 0.43 (0.06) | 0.01 (0.62) | 0.05 (0.40) |
| Sirt3 | 20 TR | 1.07 (0.89, 1.23) | 0.97 (0.77, 1.01) | 0.94 (0.83, 1.04) | 1.02 (0.79, 1.08) | 0.15 (0.20) | 0.20 (0.16) | 0.44 (0.06) |
| (ng/mL) | 20 NTR | 1.02 (0.89, 1.16) | 0.98 (0.85, 1.38) | 1.07 (0.96, 1.27) | 1.00 (0.86, 1.16) | 0.96 (0.00) | 0.36 (0.08) | 0.58 (0.03) |
| SOD | 20 TR | 85.29 (76.41, 91.79) | 89.26 (85.23, 95.31) | 92.78 (90.09, 99.01) | 93.53 (87.63, 113.34) | 0.14 (0.22) | 0.01 (0.79) | 0.01 (0.79) |
| (U/mL) | 20 NTR | 81.61 (71.90, 91.79) | 85.38 (75.04, 91.79) | 82.95 (73.70, 90.09) * | 86.81 (82.15, 90.09) * | 0.20 (0.16) | 0.65 (0.02) | 0.11 (0.25) |
| GPx | 20 TR | 1.16 (1.04, 1.34) | 1.22 (1.02, 1.44) | 1.15 (1.07, 1.52) | 1.18 (0.94, 1.47) | 0.33 (0.09) | 0.72 (0.02) | 0.65 (0.04) |
| (µmol/min/mL) | 20 NTR | 1.03 (0.94, 1.36) | 1.04 (0.96, 1.39) | 1.12 (1.04, 1.39) | 1.07 (0.99, 1.12) | 0.58 (0.01) | 0.51 (0.03) | 0.72 (0.01) |
| CAT | 20 TR | 109.90 (95.9, 127.1) | 115.57 (109.0, 126.3) | 110.34 (95.7, 128.5) | 116.19 (106.4, 123.6) | 0.65 (0.02) | 0.58 (0.03) | 0.65 (0.02) |
| (nmol/min/mL) | 20 NTR | 98.74 (87.3, 153.0) | 127.99 (108.8, 144.5) | 126.03 (83.8, 138.4) | 92.51 (86.2, 117.2) | 0.05 (0.40) | 0.44 (0.06) | 0.72 (0.01) |
| TAC | 20 TR | 361.85 (343.54, 382.36 | 363.57 (330.87, 378.10) | 356.48 (351.11, 376.17) | 364.05 (354.00, 370.39) | 0.65 (0.02) | 0.88 (0.00) | 0.92 (0.00) |
| (μmol/L) | 20 NTR | 359.44 (342.99, 385.94) | 370.32 (348.22, 381.67) | 347.67 (333.35, 370.52) | 361.4 (358.55, 373.41) | 0.44 (0.06) | 0.24 (0.14) | 0.51 (0.04) |
| TOS | 20 TR | 274.95 (195.15, 377.30) | 280.15 (181.28, 300.97) | 220.31 (147.45, 287.96) | 222.91 (124.03, 294.03) | 0.88 (0.00) | 0.17 (0.19) | 0.33 (0.09) |
| (μmol/L) | 20 NTR | 87.17 (44.23, 111.02) * | 104.01 (66.79, 124.90) * | 111.89 (91.07, 160.46)* | 117.53 (76.33, 163.93) | 0.28 (0.11) | 0.44 (0.06) | 0.28 (0.11) |
| OSI | 20 TR | 0.82 (0.51, 1.04) | 0.77 (0.47, 0.91) | 0.63 (0.42, 0.81) | 0.63 (0.34, 0.89) | 0.96 (0.00) | 0.24 (0.14) | 0.33 (0.09) |
| 20 NTR | 0.23 (0.13, 0.32) * | 0.28 (0.18, 0.33) * | 0.33 (0.24, 0.47)* | 0.33 (0.20, 0.49) | 0.24 (0.14) | 0.28 (0.11) | 0.39 (0.11) | |
| Group | Variable | Sirt1 | Sirt3 | TAC | TOS | OSI | CAT | SOD | GPx | Group |
|---|---|---|---|---|---|---|---|---|---|---|
| Sirt1 | 0.40 | 0.41 | 0.40 | 0.07 | 0.12 | −0.14 | −0.16 | 60 TR | ||
| 60 NTR | Sirt3 | 0.41 | −0.05 | 0.60 | 0.58 | −0.26 | −0.43 | −0.35 | 60 TR | |
| 60 NTR | TAC | 0.76 | 0.62 | 0.26 | −0.37 | 0.75 | 0.38 | 0.57 | 60 TR | |
| 60 NTR | TOS | −0.10 | −0.05 | 0.31 | 0.76 | 0.16 | 0.07 | 0.16 | 60 TR | |
| 60 NTR | OSI | −0.49 | −0.25 | −0.10 | 0.88 | −0.27 | −0.26 | −0.23 | 60 TR | |
| 60 NTR | CAT | −0.72 | −0.20 | −0.36 | 0.33 | 0.49 | 0.44 | 0.34 | 60 TR | |
| 60 NTR | SOD | 0.52 | 0.09 | 0.72 | 0.47 | 0.18 | −0.09 | 0.71 | 60 TR | |
| 60 NTR | GPx | 0.12 | 0.33 | 0.01 | −0.66 | −0.64 | 0.15 | −0.02 |
| Group | Variable | Sirt1 | Sirt3 | TAC | TOS | OSI | CAT | SOD | GPx | Group |
|---|---|---|---|---|---|---|---|---|---|---|
| Sirt1 | 0.19 | 0.34 | −0.26 | −0.35 | 0.20 | 0.02 | 0.26 | 20 TR | ||
| 20 NTR | Sirt3 | 0.79 | −0.13 | −0.28 | −0.39 | 0.05 | 0.77 | −0.40 | 20 TR | |
| 20 NTR | TAC | 0.24 | −0.12 | −0.03 | −0.07 | 0.76 | −0.30 | 0.02 | 20 TR | |
| 20 NTR | TOS | 0.10 | −0.02 | −0.24 | 0.99 | −0.43 | −0.15 | 0.57 | 20 TR | |
| 20 NTR | OSI | −0.12 | −0.12 | −0.33 | 0.95 | −0.47 | −0.22 | 0.55 | 20 TR | |
| 20 NTR | CAT | −0.08 | −0.26 | 0.45 | 0.24 | 0.28 | −0.26 | −0.27 | 20 TR | |
| 20 NTR | SOD | −0.01 | −0.05 | 0.01 | −0.23 | −0.14 | −0.07 | −0.36 | 20 TR | |
| 20 NTR | GPx | −0.21 | −0.36 | −0.05 | −0.23 | −0.21 | 0.23 | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wojciak, G.; Szymura, J.; Szygula, Z.; Gradek, J.; Wiecek, M. The Effect of Repeated Whole-Body Cryotherapy on Sirt1 and Sirt3 Concentrations and Oxidative Status in Older and Young Men Performing Different Levels of Physical Activity. Antioxidants 2021, 10, 37. https://doi.org/10.3390/antiox10010037
Wojciak G, Szymura J, Szygula Z, Gradek J, Wiecek M. The Effect of Repeated Whole-Body Cryotherapy on Sirt1 and Sirt3 Concentrations and Oxidative Status in Older and Young Men Performing Different Levels of Physical Activity. Antioxidants. 2021; 10(1):37. https://doi.org/10.3390/antiox10010037
Chicago/Turabian StyleWojciak, Gabriela, Jadwiga Szymura, Zbigniew Szygula, Joanna Gradek, and Magdalena Wiecek. 2021. "The Effect of Repeated Whole-Body Cryotherapy on Sirt1 and Sirt3 Concentrations and Oxidative Status in Older and Young Men Performing Different Levels of Physical Activity" Antioxidants 10, no. 1: 37. https://doi.org/10.3390/antiox10010037
APA StyleWojciak, G., Szymura, J., Szygula, Z., Gradek, J., & Wiecek, M. (2021). The Effect of Repeated Whole-Body Cryotherapy on Sirt1 and Sirt3 Concentrations and Oxidative Status in Older and Young Men Performing Different Levels of Physical Activity. Antioxidants, 10(1), 37. https://doi.org/10.3390/antiox10010037