
Eye-Tracking Assessment in Patients with Disorders of Consciousness: A Systematic Review

 , and
, and 
Highlights
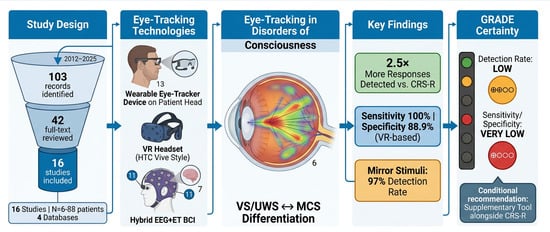
- Eye-tracking detects 2.5× more visual responses than standard clinical observation (46.2% vs. 18.1%), demonstrating its superior sensitivity for identifying covert consciousness signs missed by CRS-R.
- Mirror stimuli achieve the highest detection rates (97% of patients with MCS), followed by person (69%) and object (57%) stimuli, providing immediate practical guidance for optimising clinical assessment protocols.
- Advanced VR-based systems achieve high diagnostic accuracy: sensitivity 100% and specificity 88.9% (RPTL-V biomarker), with preliminary prognostic value—62.5% of overt trackers demonstrated command-following at one year.
- High heterogeneity and small sample size of selected studies supported a conditional recommendation for eye-tracking as a supplementary tool alongside CRS-R, not a replacement.
Abstract
1. Introduction
2. Materials and Methods
2.1. PICO Framework
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategy
2.4. Study Selection and Data Extraction
2.5. Risk of Bias Assessment
2.6. Certainty of Evidence
3. Results
3.1. Study Selection and Characteristics
3.2. Risk of Bias Assessment Findings
3.3. Synthesis of Findings
3.3.1. Detection of Visual Pursuit and Fixation
3.3.2. Stimulus Type Effects
3.3.3. Objective Eye-Tracking vs. Clinical Assessment
3.3.4. Advanced Technologies: VR and Hybrid BCI Systems
3.3.5. Prognostic Value
3.3.6. GRADE Certainty Assessment
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johansson, J.; Möller, M.; Franzon, K.; Stenberg, J.; Godbolt, A.K. Eye tracking to support assessment of patients with prolonged disorder of consciousness—A case series. J. Rehabil. Med. 2025, 57, jrm41324. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Fins, J.J. Rethinking disorders of consciousness: New research and its implications. Hastings Cent. Rep. 2005, 35, 22–24. [Google Scholar]
- Ting, W.K.-C.; Perez Velazquez, J.L.; Cusimano, M.D. Eye Movement Measurement in Diagnostic Assessment of Disorders of Consciousness. Front. Neurol. 2014, 5, 137. [Google Scholar] [CrossRef]
- Giacino, J.T.; Kalmar, K.; Whyte, J. The JFK Coma Recovery Scale-Revised: Measurement characteristics and diagnostic utility. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef]
- Schnakers, C.; Vanhaudenhuyse, A.; Giacino, J.; Ventura, M.; Boly, M.; Majerus, S.; Moonen, G.; Laureys, S. Diagnostic accuracy of the vegetative and minimally conscious state: Clinical consensus versus standardized neurobehavioral assessment. BMC Neurol. 2009, 9, 35. [Google Scholar] [CrossRef]
- Majerus, S.; Gill-Thwaites, H.; Andrews, K.; Laureys, S. Behavioral evaluation of conscious ness in severe brain damage. Prog. Brain Res. 2005, 150, 397–413. [Google Scholar]
- Candelieri, A.; Cortese, M.D.; Dolce, G.; Riganello, F.; Sannita, W.G. Visual pursuit: Within-day variability in the severe disorder of consciousness. J. Neurotrauma 2011, 28, 2013–2017. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.M.; Coleman, M.R.; Boly, M.; Davis, M.H.; Laureys, S.; Pickard, J.D. Detecting awareness in the vegetative state. Science 2006, 313, 1402. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Pan, J.; He, Y.; Xie, Q.; Yu, T.; Huang, H.; Lv, W.; Zhang, J.; Yu, R.; Li, Y. Visual Fixation Assessment in Patients with Disorders of Consciousness Based on Brain-Computer Interface. Neurosci. Bull. 2018, 34, 679–690. [Google Scholar] [CrossRef]
- Estraneo, A.; Moretta, P.; Cardinale, V.; De Tanti, A.; Gatta, G.; Giacino, J.T.; Trojano, L. A multicentre study of intentional behavioural responses measured using the Coma Recovery Scale-Revised in patients with minimally conscious state. Clin. Rehabil. 2015, 29, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Kondziella, D.; Bender, A.; Diserens, K.; van Erp, W.; Estraneo, A.; Formisano, R.; Laureys, S.; Naccache, L.; Ozturk, S.; Rohaut, B.; et al. EAN Panel on Coma, Disorders of Consciousness. European Academy of Neurology guideline on the diagnosis of coma and other disorders of consciousness. Eur. J. Neurol. 2020, 27, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.A.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef]
- Lee, H.H.; Hyun, C.; Kang, C.H.; Moon, W.J.; Lee, J. Evaluating impaired consciousness after acquired brain injury using a virtual-reality-based eye-tracking system. Preprint 2024. [Google Scholar] [CrossRef]
- Zurek, G.; Binder, M.; Kunka, B.; Kosikowski, R.; Rodzeń, M.; Karaś, D.; Mucha, G.; Olejniczak, R.; Gorączko, A.; Kujawa, K.; et al. Can Eye Tracking Help Assess the State of Consciousness in Non-Verbal Brain Injury Patients? J. Clin. Med. 2024, 13, 6227. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Duchowski, A.T. Eye Tracking Methodology: Theory and Practice, 3rd ed.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Magliacano, A.; Rosenfelder, M.; Hieber, N.; Bender, A.; Estraneo, A.; Trojano, L. Spontaneous eye blinking as a diagnostic marker in prolonged disorders of consciousness. Sci. Rep. 2021, 11, 22393. [Google Scholar] [CrossRef]
- Holmqvist, K.; Nyström, M.; Andersson, R.; Dewhurst, R.; Jarodzka, H.; Van de Weijer, J. Eye Tracking: A Comprehensive Guide to Methods and Measures; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Overbeek, B.U.H.; Eilander, H.J.; Lavrijsen, J.C.M.; Koopmans, R.T.C.M. Are visual functions diagnostic signs of the minimally conscious state? an integrative review. J. Neurol. 2018, 265, 1957–1975. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Slater, M.; Sanchez-Vives, M.V. Enhancing our lives with immersive virtual reality. Front. Robot. AI 2016, 3, 74. [Google Scholar] [CrossRef]
- Wolpaw, J.R.; Wolpaw, E.W. (Eds.) Brain-Computer Interfaces: Principles and Practice; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Pfurtscheller, G.; Allison, B.Z.; Brunner, C.; Bauernfeind, G.; Solis-Escalante, T.; Scherer, R.; Zander, T.O.; Mueller-Putz, G.; Neuper, C.; Birbaumer, N. The hybrid BCI. Front. Neurosci. 2010, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Johansson, J.; Franzon, K.; Godbolt, A.K.; Möller, M.C. Methodological aspects of using a wearable eye-tracker to support diagnostic clinical evaluation of prolonged disorders of consciousness. J. Rehabil. Med. 2021, 53, jrm00213. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Aklepi, G.; Manolovitz, B.; Robayo, L.E.; Sarafraz, A.; Blandino, C.F.; Arwari, B.; Sobczak, E.; Bass, D.; Ghamasaee, P.; Bolaños Saavedra, A.; et al. Covert Tracking to Immersive Stimuli in Traumatic Brain Injury Subjects with Disorders of Consciousness. J. Neurotrauma 2024, 41, 646–659. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Trojano, L.; Moretta, P.; Loreto, V.; Cozzolino, A.; Santoro, L.; Estraneo, A. Quantitative assessment of visual behavior in disorders of consciousness. J. Neurol. 2012, 259, 1888–1895. [Google Scholar] [CrossRef]
- Trojano, L.; Moretta, P.; Loreto, V.; Santoro, L.; Estraneo, A. Affective saliency modifies visual tracking behavior in disorders of consciousness. J. Neurol. 2013, 260, 306–308. [Google Scholar] [CrossRef]
- Thonnard, M.; Wannez, S.; Keen, S.; Brédart, S.; Bruno, M.-A.; Gosseries, O.; Demertzi, A.; Thibaut, A.; Chatelle, C.; Charland-Verville, V.; et al. Detection of visual pursuit in patients in minimally conscious state: A matter of stimuli and visual plane? Brain Inj. 2014, 28, 1164–1170. [Google Scholar] [CrossRef] [PubMed]
- Naro, A.; Calabrò, R.S.; Russo, M.; Leo, A.; Pollicino, P.; Quartarone, A.; Bramanti, P. Can transcranial direct current stimulation be useful in differentiating unresponsive wakefulness syndrome from minimally conscious state patients? Restor. Neurol. Neurosci. 2015, 33, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Wannez, S.; Heine, L.; Thonnard, M.; Gosseries, O.; Laureys, S.; Coma Science Group collaborators. The repetition of behavioral assessments in diagnosis of disorders of consciousness. Ann. Neurol. 2017, 81, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Wannez, S.; Gosseries, O.; Azzolini, D.; Martial, C.; Cassol, H.; Aubinet, C.; Annen, J.; Martens, G.; Bodart, O.; Heine, L.; et al. Prevalence of coma-recovery scale-revised signs of consciousness in patients in minimally conscious state. Neuropsychol. Rehabil. 2018, 28, 1350–1359. [Google Scholar] [CrossRef] [PubMed]
- Kujawa, K.; Zurek, G.; Kwiatkowska, A.; Olejniczak, R.; Żurek, A. Assessment of Language Functions in Patients with Disorders of Consciousness Using an Alternative Communication Tool. Front Neurol. 2021, 12, 684362. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sattin, D.; Rossi Sebastiano, D.; Magnani, F.G.; D’Incerti, L.; Marotta, G.; Benti, R.; Tirelli, S.; Bersano, A.; Duran, D.; Visani, E.; et al. Visual fixation in disorders of consciousness: Development of predictive models to support differential diagnosis. Physiol. Behav. 2021, 230, 113310. [Google Scholar] [CrossRef] [PubMed]
- Kujawa, K.; Żurek, A.; Gorączko, A.; Olejniczak, R.; Zurek, G. Monitoring Eye Movements Depending on the Type of Visual Stimulus in Patients with Impaired Consciousness Due to Brain Damage. Int. J. Environ. Res. Public Health 2022, 19, 6280. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yi, Z.; Pan, J.; Chen, Z.; Lu, D.; Cai, H.; Li, J.; Xie, Q. Hybrid brain-computer interface integrating EEG and eye-tracking for consciousness assessment in patients with disorders of consciousness. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 2759–2771. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Zamora, F.J.; Lajoie, K.; Miller, A.B.; Marigold, D.S. Age-related changes in gaze sampling strategies during obstacle navigation. Gait Posture 2020, 76, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Owsley, C. Aging and vision. Vis. Res. 2011, 51, 1610–1622. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author & Year | Sample Size | Age Range (Years) | Study Aim | Sample Characteristics | Study Design | Eye-Tracking Protocol | Main Findings |
|---|---|---|---|---|---|---|---|
| Trojano et al., 2012 [27] | 18 (9 VS/UWS, 9 MCS) | 19–69 | Quantitative assessment of visual behaviour in DOC | Chronic DOC patients; infrared eye-tracking | Observational cross-sectional | Infrared eye tracker; stimuli: moving red circle, moving parrot image, moving photo of relative; VP defined as series of fixations on target | MCS patients showed significantly higher on-target fixations (67.8%) vs. VS/UWS patients (32.2%); quantitative eye-tracking differentiated diagnostic groups |
| Trojano et al., 2013 [28] | 26 (13 VS/UWS, 13 MCS) | VS patients: 21–65; MCS patients: 7–76 | Investigate affective saliency effects on visual tracking | Chronic DOC patients | Observational cross-sectional | Infrared eye tracker; stimuli: moving circle, moving parrot, moving photo of close relative | MCS patients showed significantly higher tracking of relative’s photo (37.3%) vs. parrot (29.9%) vs. circle (30.6%); affective saliency modulates visual tracking in MCS but not VS/UWS |
| Thonnard et al., 2014 [29] | 88 (47 MCS−, 41 MCS+) | Mean 51 ± 20 | Detection of visual pursuit in MCS; effects of stimuli and visual plane | MCS patients assessed with CRS-R | Observational cross-sectional | CRS-R protocol; stimuli: mirror, person, object; horizontal and vertical planes assessed | 97% tracked mirror, 69% tracked person, 57% tracked object; mirror most sensitive stimulus; more horizontal tracking overall; MCS− showed more horizontal preference than MCS+ |
| Naro et al., 2015 [30] | 25 DOC, 2 EMCS, 1 LIS and 20 healthy controls | Healthy controls: Mean 56.5 ± 6.3; DOC subgroups: Mean 52–57 | Visual fixation in chronic DOC for differential diagnosis | Chronic DOC patients | Observational cross-sectional | Eye-tracking assessment of visual fixation | Visual fixation patterns differentiate diagnostic categories in chronic DOC; supports use of eye-tracking for differential diagnosis |
| Wannez et al., 2017 [31] | 123 DOC | Mean 40 ± 14; Range 18–72 | Assess mirror efficiency in visual pursuit assessment in MCS | MCS patients | Observational cross-sectional | Eye-tracking with mirror stimulus; comparison with other stimuli | Mirror confirmed as most efficient stimulus for detecting visual pursuit in MCS patients; supports preferential use of mirror in assessment protocols |
| Wannez et al., 2018 [32] | 31 DOC and 23 healthy controls | DOC patients: Mean 40.23 ± 13.19; Healthy subjects: Mean 28 ± 7 | Objective assessment of visual pursuit in DOC using wearable eye tracker | MCS patients | Exploratory observational | Wearable eye tracker; assessment of visual pursuit | Wearable eye-tracking detected visual pursuit responses not observed through clinical assessment alone; objective quantification possible |
| Johansson et al., 2021 [23] | 4 DOC | 22–43 | Methodological aspects of wearable eye-tracker for DOC assessment | DOC patients | Methodological study | Wearable eye tracker; evaluation of technical and practical aspects | Wearable eye-trackers are feasible for DOC assessment; technical considerations include calibration challenges and need for standardised protocols |
| Kujawa et al., 2021 [33] | 6 (all VS/UWS) | 18–62 | Assessment of language functions in DOC using eye-tracking AAC | 6 VS/UWS patients (age 18–62; 3 men, 3 women); aetiology: sudden circulatory arrest; 4–6 months post-injury; diagnosed with GCS ≤ 8 | Longitudinal case series (1, 6, 12 months) | C-Eye Pro infrared system; tasks: selecting pictograms, yes/no questions, sentence matching; 60 min sessions with 25 language tasks; calibration before each session | Average 70.45% task completion rate; high performance suggests potential misdiagnosis (patients may be MCS rather than VS/UWS); high intra-individual variability noted |
| Sattin et al., 2021 [34] | 58 DOC | Mean 66.72 ± 25.07 | Visual fixation in DOC: predictive models for differential diagnosis | DOC patients | Observational cross-sectional | Eye-tracking assessment of visual fixation; development of predictive models | Visual fixation patterns can be modelled to predict diagnostic category; supports integration of eye-tracking into diagnostic algorithms |
| Kujawa et al., 2022 [35] | 12 DOC | 26–67 | Monitoring eye movements by visual stimulus type in impaired consciousness | Patients with impaired consciousness | Observational cross-sectional | Eye-tracking with multiple stimulus types; comparison of responses | Stimulus type significantly influences eye movement patterns and detection rates; supports systematic stimulus selection in protocols |
| Aklepi et al., 2024 [25] | 10 DOC and 20 healthy controls | Mean 29 ± 17 | Covert tracking to immersive stimuli in TBI with DOC | TBI patients with DOC | Observational cross-sectional | Immersive stimuli presentation; assessment of covert tracking | Immersive stimuli can elicit covert tracking responses in TBI patients with DOC; may reveal consciousness signs not detected with standard stimuli |
| Lee et al., 2024 [14] | 21 (15 DOC, 6 healthy controls) | DOC patients: Median 67 (IQR: 64.5–72.5); Healthy controls: Median 55 (IQR: 52.3–58.3) | VR-based eye-tracking system for impaired consciousness; validation of RPTL biomarker | DOC group: median age 67 (IQR 64.5–72.5), 60% women; etiologies: SAH, SDH, ICH, HBI, TBI; chronicity 32–560 days; CRS-R assessment | Observational cross-sectional with 1-year follow-up | HTC Vive HMD with infrared pupil tracking (60 Hz); 9 visuoauditory VR stimuli; RPTL-V and RPTL-A calculated (pupil trajectory during stimuli vs. blank); validated against VEP/BAEP | RPTL-V cut-off 14.737 (sensitivity 100%, specificity 88.9%); RPTL-A cut-off 30.019 (sensitivity 88.9%, specificity 83.3%); overt tracking predicted command-following at 1 year in 62.5%; one patient showed RPTL response not detected by CRS-R |
| Yi et al., 2024 [36] | 9 DOC, 1 LIS, 10 healthy controls | Patients: Mean 38.8 ± 22.2; Healthy volunteers: Mean 24.0 ± 1.2 | Hybrid BCI integrating EEG and eye-tracking for DOC | DOC patients | Observational cross-sectional | Hybrid BCI system combining EEG and eye-tracking; multimodal assessment | Integration of EEG and eye-tracking provides complementary information for consciousness assessment; hybrid approach may improve diagnostic accuracy |
| Zurek et al., 2024 [15] | 46 DOC | ≥18 (specific range not provided) | Can eye-tracking help assess consciousness in non-verbal brain injury patients; MCSD test vs. CRS-R | Non-verbal brain injury patients; multi-centre trial, Poland 2022–2023 | Multi-centre clinical trial | MCSD (Multimodal Consciousness State Detection) test incorporating eye-tracking; comparison with CRS-R | Eye-tracking-based MCSD test provides additional diagnostic information beyond CRS-R; supports integration into clinical assessment protocols |
| Johansson et al., 2025 [1] | 12 (outpatients with prolonged DOC) | Median 43; Range 18–64 | Eye-tracking to support assessment of prolonged DOC | 12 outpatients with prolonged DOC | Observational cross-sectional | Wearable eye tracker; comparison with clinical assessment | Eye-tracking detected responses in 46.2% of trials vs. 18.1% by clinical assessment alone; demonstrates superior sensitivity of objective eye-tracking |
| Study | Study Design | Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other Bias | Overall Risk |
|---|---|---|---|---|---|---|---|---|
| Lee et al., 2024 [14] | Observational prospective cohort (single-centre, n = 15) | Unclear (inclusion/exclusion criteria specified but sampling method not clearly described) | Unclear (VR protocol described but uncalibrated pupil trajectories acknowledged; standardisation not fully detailed) | Low (VEP/BAEP assessed by two domain experts via visual inspection; objective electrophysiological measures; ROC-determined cut-offs) | High (1/3 covert tracking patients died before follow-up; follow-up methods varied face-to-face vs. video calls; missing data not fully quantified) | Unclear (no pre-registration mentioned; sample size limitation acknowledged; one discordance case noted) | Low (no competing interests declared; age discrepancy between DOC and controls noted but deemed negligible) | High |
| Naro et al., 2015 [30] | Interventional prospective sham-controlled crossover (single-centre, n = 25) | Low (inclusion/exclusion criteria clearly defined; consecutive enrollment from neurorehabilitation unit) | Low (standardised TMS/tDCS protocols; sham-controlled; randomised order; healthy controls and examiners blinded) | Low (blinded examiners analysing EEG data; objective neurophysiological measures; standardised analysis procedures) | Unclear (no explicit dropout or missing data reported; all 25 patients appear to have completed protocol) | Low (methods and outcomes clearly described; limitations acknowledged; no pre-registration but systematic protocol) | Low (no conflicts of interest declared; funded by Italian Ministry of Health) | Low |
| Sattin et al., 2021 [34] | Observational prospective cohort (single-centre, n = 58) | Low (consecutive enrollment; clear inclusion/exclusion criteria; representative sample from neurorehabilitation unit) | Low (standardised CRS-R and VEP protocols; trained examiners; objective electrophysiological measures) | Low (objective VEP measurements; blinded analysis not stated but objective measures reduce bias; ROC analysis for cut-offs) | Low (all 58 patients completed assessments; no missing data reported) | Low (comprehensive reporting of methods and outcomes; limitations discussed; statistical methods appropriate) | Low (no conflicts of interest declared; funded by Italian Ministry of Health) | Low |
| Thonnard et al., 2014 [29] | Observational prospective cohort (single-centre, n = 88 MCS) | Low (consecutive enrollment; clear diagnostic criteria; representative MCS sample) | Low (standardised CRS-R protocol; trained examiners; systematic assessment of pursuit across multiple stimuli) | Unclear (clinical observation without objective measurement; no blinding mentioned; subjective judgement of pursuit) | Low (all 88 patients completed assessments; comprehensive data reported) | Low (detailed reporting of pursuit patterns; limitations discussed; no pre-registration but systematic protocol) | Low (no conflicts of interest apparent; academic study) | Unclear |
| Trojano et al., 2012 [27] | Observational case–control (single-centre, n = 18 DOC: 9 MCS, 9 UWS) | Unclear (convenience sample; small sample size; no details on consecutive enrollment or sampling method) | Low (standardised infrared eye-tracking protocol using MyTobii T60; objective measurements; fixed stimulus presentation) | Low (objective eye-tracking measurements; automated data recording; chi-square analysis for statistical comparison) | Low (all 18 patients completed protocol; no missing data reported) | Unclear (no pre-registration; small sample acknowledged; unclear if all planned analyses reported) | Low (no conflicts of interest apparent; academic study) | Unclear |
| Trojano et al., 2013 [28] | Observational case series (single-centre, sample size unclear) | High (sample size not clearly reported; convenience sample; unclear enrollment procedures) | Low (standardised infrared eye-tracking protocol using MyTobii T60; objective measurements; controlled stimulus presentation) | Low (objective eye-tracking measurements; automated data recording; chi-square analysis) | Unclear (sample size unclear; no attrition data reported) | High (sample size not clearly stated; limited methodological details; unclear if all outcomes reported) | Low (no conflicts of interest apparent; academic study) | High |
| Wannez et al., 2018 [32] | Observational prospective cohort (single-centre, n = 31 patients, 23 controls) | Low (clear inclusion/exclusion criteria; consecutive enrollment; representative sample) | Low (standardised automated device protocol; C-score and M-score algorithms; objective measurements) | Low (automated scoring algorithms; objective measurements; blinded validation against CRS-R; 100% subject-level agreement κ = 1.0) | Low (all 54 participants completed protocol; comprehensive data reported) | Low (detailed reporting of methods and validation; limitations discussed; systematic protocol) | Low (no conflicts of interest declared; funded by Belgian National Funds for Scientific Research) | Low |
| Wannez et al., 2017 [31] | Observational prospective cohort (single-centre, n = 123 DOC) | Low (consecutive enrollment; clear diagnostic criteria; large representative sample) | Low (standardised CRS-R protocol; trained examiners; repeated assessments up to 5 times) | Low (standardised CRS-R with established reliability; multiple assessments reduce bias; systematic protocol) | Low (all 123 patients completed multiple assessments; comprehensive data reported) | Low (detailed reporting of misdiagnosis rates; limitations discussed; systematic protocol) | Low (no conflicts of interest declared; funded by Belgian National Funds for Scientific Research) | Low |
| Yi et al., 2024 [36] | Observational case–control (single-centre, n = 10 patients, 10 controls) | Unclear (convenience sample; small sample size; no details on consecutive enrollment) | Low (standardised hybrid BCI protocol combining EEG and eye-tracking; objective measurements; controlled stimulus presentation) | Low (objective EEG and eye-tracking measurements; automated data recording; statistical analysis of communication accuracy) | Low (all 20 participants completed protocol; no missing data reported) | Unclear (no pre-registration; small sample acknowledged; unclear if all planned analyses reported) | Low (funded by National Natural Science Foundation of China; no conflicts of interest declared) | Unclear |
| Zurek et al., 2024 [15] | Observational prospective cohort (single-centre, n = 46 analysed from 66 recruited) | Unclear (30% excluded; inclusion/exclusion criteria specified but sampling method not fully described) | Low (standardised C-EYE X eye-tracker protocol; MCSD algorithm; objective measurements; controlled testing environment) | Low (objective eye-tracking measurements; automated MCSD scoring; blinded comparison with CRS-R) | High (30% excluded: 20 patients excluded for various reasons; missing data not fully quantified; no analysis of excluded vs. included) | Unclear (no pre-registration mentioned; sample size limitation acknowledged; need for larger studies noted) | Low (funded by government grant and company; authors declare scientific rigour; no competing interests) | High |
| Aklepi et al., 2024 [25] | Observational prospective pilot (single-centre, n = 10 TBI) | Low (single-centre convenience sample but clear inclusion/exclusion criteria; recruited 20 healthy volunteers and 10 TBI subjects) | Low (standardised VET protocol using Tobii Pro Glasses 2; predefined tracking criteria; screen position confirmed; calibration attempted) | Low (multiple levels of blinding implemented; objective eye-tracking measurements 50 Hz; two independent examiners Cohen’s κ = 0.8 CI 0.7–0.96) | Low (84 tested trials; one subject and one trial did not generate sufficient ML data resulting in 72 tested trials; follow-up: all accounted at 6 months, 1 lost/1 deceased/1 regressed at 12 months) | Low (pre-registered ClinicalTrials.gov NCT04712591; analysis plan pre-determined; acknowledged as pilot not powered for differences) | Low (multiple NIH and institutional funding; one author minority shareholder at iCE Neurosystems; no industry sponsorship of this study) | Low |
| Johansson et al., 2021 [23] | Observational methodological case series (single-centre, n = 4) | High (four patients from single rehabilitation clinic; convenience sample; no randomisation; very small sample) | Unclear (CRS-R administered per standard protocol; Tobii Pro Glasses 2 used 50 Hz; arousal optimisation attempted; standardisation not fully detailed) | Low (blinded scoring of clinical vs. eye-tracking protocols; objective eye-tracking measurements; stepwise analysis) | High (Patient 3 had complete data for only 21% of trials due to gaze deviation; data retrieved 96–100% for 3/4 patients but only 21% for one; no discussion of missing data impact) | Unclear (no pre-registration; feasibility study with exploratory aims; unclear if all planned outcomes reported) | Low (funded by SLL Innovation and Promobilia; no conflicts of interest apparent; no industry sponsorship) | High |
| Johansson et al., 2025 [1] | Observational case series (single-centre, n = 12) | High (convenience sample recruited consecutively from single rehabilitation unit; small sample; only prolonged PDOC patients; limits generalisability) | Unclear to High (standardised CRS-R protocol; equipment comfort issues noted: 4 patients showed poor responses wearing eye-tracker but improved without it; calibration problems and difficulties linking eye movements to stimuli) | Low (blinded scoring by different assessors; objective eye-tracking measurements; however recorded eye movements often subtle, strained, frequently interrupted) | Unclear (response data obtained from 238/288 trials 82.6%; no data for 50 trials due to closed eyes or extreme angles; eye-tracking data obtained median 89.6% range 37.5–100%; unclear if patient-level attrition) | Unclear (no pre-registration; unclear if all planned outcomes reported) | Low (funded by Innovationsfonden Region Stockholm and Promobilia; no conflicts of interest declared) | High |
| Kujawa et al., 2021 [33] | Observational longitudinal (1, 6, 12 months; single-centre, n = 6) | High (six patients aged 18–62; convenience sample; all UWS from sudden circulatory arrest; small sample; no randomisation) | High (calibration procedure described; 25 tasks per session randomly selected; session frequency varied due to patient health and willingness; lack of standardisation in session frequency) | Unclear (no blinding reported; objective eye-tracking measurements; monitored eye opening and gaze direction; unclear who scored outcomes and whether blinded) | Unclear (variable cooperation noted in Patients 3, 5, 6: sometimes considerable decrease in efficiency or no cooperation; no explicit dropout rates or missing data handling; frequency varied due to changing health) | Unclear (no pre-registration; unclear if all outcomes reported; limited statistical analysis) | Low (no conflicts of interest declared; no industry sponsorship apparent) | High |
| Kujawa et al., 2022 [35] | Observational examining eyeball movement patterns (single-centre, n = 12 final from 20 initial) | High (recruited from single Palliative Care Centre; started N = 20, final N = 12 after exclusions and deaths; convenience sample; small sample acknowledged as limitation) | Low to Unclear (standardised protocol using C-Eye device 30 Hz, 0.4° accuracy, 40 cm/s velocity threshold; one-point calibration; fixed distance 50 cm; monitor position adjusted; no head stabilisation) | Low (automated data recording and analysis; assessment independent of human investigator; objective measurement of fixations and saccades; built-in software detected all eye movements automatically) | Very Serious (3 failed calibrations excluded; 5 persons died during project; started N = 20, final N = 12: 40% attrition; no analysis of differences between completers and non-completers) | Unclear (no pre-registration; unclear if all planned outcomes reported) | Low (no conflicts of interest declared) | High |
| Study | No. of Participants | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Certainty |
|---|---|---|---|---|---|---|---|
| Lee et al., 2024 [14] | 15 DOC patients | Serious (high attrition bias; unclear selection and performance bias; varied follow-up methods) | Not Serious (single study; internal consistency not assessable) | Not Serious (direct comparison of eye-tracking RPTL vs. CRS-R; relevant patient population; 1-year functional outcome) | Very Serious (very small sample n = 15; only 1 patient showed covert tracking without CRS-R response; wide variation in follow-up assessment methods) | Undetected (single study; no competing interests declared) | Very Low |
| Naro et al., 2015 [30] | 25 DOC patients (15 UWS, 10 MCS) | Not Serious (low risk across all domains; blinded sham-controlled crossover design; standardised protocols) | Not Serious (single study; consistent findings across cortical connectivity measures) | Not Serious (directly addresses cortical connectivity in DOC; relevant population; appropriate intervention and comparator) | Serious (moderate sample n = 25; no confidence intervals reported for some measures; single-centre study) | Undetected (single study; no conflicts of interest; funded by Italian Ministry of Health) | Moderate |
| Sattin et al., 2021 [34] | 58 DOC patients | Not Serious (low risk across all domains; consecutive enrollment; standardised protocols; objective measures) | Not Serious (single study; consistent VEP findings across patient groups) | Not Serious (directly addresses VEP as predictor of consciousness recovery; relevant population; appropriate outcome measures) | Not Serious (adequate sample n = 58; confidence intervals reported for ROC analysis; AUC 0.832 CI 0.724–0.940) | Undetected (single study; no conflicts of interest; funded by Italian Ministry of Health) | High |
| Thonnard et al., 2014 [29] | 88 MCS patients | Not Serious to Serious (low risk overall but unclear detection bias due to subjective clinical observation without objective measurement) | Not Serious (single study; consistent pursuit patterns across stimuli types) | Not Serious (directly addresses visual pursuit patterns in MCS; relevant population; clinically relevant stimuli) | Not Serious (adequate sample n = 88; comprehensive data on pursuit patterns across multiple stimuli) | Undetected (single study; no conflicts of interest apparent) | Moderate |
| Trojano et al., 2012 [27] | 18 DOC (9 MCS, 9 UWS) | Serious (unclear selection bias; small sample; convenience sampling; unclear reporting bias) | Not Serious (single study; consistent findings: MCS 78% above chance, UWS 0% above chance) | Not Serious (directly addresses eye-tracking detection in DOC; relevant population; objective measurements) | Serious (small sample n = 18; no confidence intervals reported; chi-square p < 0.001 but limited statistical detail) | Undetected (single study; no conflicts of interest apparent) | Low |
| Trojano et al., 2013 [28] | Sample size unclear | Very Serious (high selection bias: sample size not clearly reported; high reporting bias: limited methodological details; unclear attrition) | Not Serious (single study; consistent finding: face vs. circle χ2 = 43.40 p < 0.001) | Not Serious (directly addresses emotional stimulus processing via eye-tracking; relevant population) | Very Serious (sample size unclear; no confidence intervals; limited statistical reporting) | Undetected (single study; no conflicts of interest apparent) | Very Low |
| Wannez et al., 2018 [32] | 31 patients, 23 controls (total 54) | Not Serious (low risk across all domains; automated scoring; blinded validation; 100% subject-level agreement κ = 1.0) | Not Serious (single study; consistent validation results across subgroups; M-score sensitivity/specificity 80–100%) | Not Serious (directly addresses automated eye-tracking device validation; relevant population; appropriate comparator CRS-R) | Not Serious (adequate sample n = 54; confidence intervals not reported but perfect agreement κ = 1.0; sensitivity/specificity 80–100% across subgroups) | Undetected (single study; no conflicts of interest; funded by Belgian National Funds) | High |
| Wannez et al., 2017 [31] | 123 DOC patients | Not Serious (low risk across all domains; consecutive enrollment; large sample; standardised repeated CRS-R assessments) | Not Serious (single study; consistent finding: 5 assessments needed to reduce misdiagnosis to 5%) | Not Serious (directly addresses misdiagnosis rates in DOC; relevant population; clinically important outcome) | Not Serious (large sample n = 123; precise estimates of misdiagnosis rates; visual pursuit in 2/6 missed MCS-, fixation in 1/6) | Undetected (single study; no conflicts of interest; funded by Belgian National Funds) | High |
| Yi et al., 2024 [36] | 10 patients, 10 controls (total 20) | Serious (unclear selection and reporting bias; small sample; convenience sampling) | Not Serious (single study; consistent finding: 5/10 patients 50% achieved significant communication mean 76.1 ± 7.9%) | Not Serious (directly addresses hybrid BCI communication in DOC; relevant population; P5 and P10 communicated but CRS-R communication = 0) | Serious (small sample n = 20; no confidence intervals reported; limited statistical detail) | Undetected (single study; no conflicts of interest; funded by National Natural Science Foundation of China) | Low |
| Zurek et al., 2024 [15] | 46 analysed (from 66 recruited) | Serious (high attrition bias: 30% excluded; unclear selection and reporting bias; missing data not fully quantified) | Not Serious (single study; consistent correlations across all time points T1–T5; consistent with adaptation effect: T1–T2 familiarisation, T3+ reliable) | Not Serious (directly addresses eye-tracking technology validation C-EYE X MCSD; relevant patient population DOC requiring neurorehabilitation; appropriate comparator CRS-R) | Serious (moderate sample n = 46 analysed from 66 recruited; wide confidence intervals for some regression coefficients, e.g., T1 β0: −14.58 to 19.48; acknowledged need for larger studies) | Undetected (single study; funded by government grant and company; authors declare scientific rigour) | Low |
| Aklepi et al., 2024 [25] | 10 TBI patients, 20 healthy volunteers | Not Serious (multiple levels of blinding; pre-registered; standardised protocols; low risk across all domains) | Serious (single-centre study with no replication; pilot study not powered for efficacy; machine learning algorithm showed only moderate agreement with human examiners Cohen’s κ = 0.5 CI 0.3–0.7) | Not Serious (direct measurement of target outcome tracking ability; relevant population unresponsive TBI patients; immersive video stimuli directly relevant to clinical assessment) | Serious (small sample n = 10 TBI subjects; wide confidence intervals on some measures, e.g., Cohen’s κ for ML: 0.3–0.7; pilot study acknowledged as not powered for differences; follow-up limited by attrition: 1 lost, 1 deceased, 1 regressed at 12 months) | Undetected (pre-registered study; no evidence of selective reporting) | Low |
| Johansson et al., 2021 [23] | 4 patients | Very Serious (very small sample n = 4; high attrition for one patient 79% data loss; no randomisation; convenience sampling; unclear reporting of outcomes) | Very Serious (high variability in agreement between patients 54–80%; one patient with extreme data loss; variable performance within subjects and test items) | Not Serious (direct assessment of target outcome eye movements during CRS-R; relevant population PDOC patients) | Very Serious (extremely small sample n = 4; no confidence intervals reported; wide variation in results between patients; 75% data loss in one patient) | Undetected (feasibility study with negative/mixed results published; no evidence of selective reporting) | Very Low |
| Johansson et al., 2025 [1] | 12 patients | Serious (small convenience sample n = 12; equipment comfort issues affected 4 patients; methodological challenges with subtle eye movements and calibration) | Serious (poor inter-method agreement Cohen’s κ = 0.073 CI −0.031 to 0.177; wide range in data retrieval rates 37.5–100%; variable results across test items: some significant, some not) | Serious (only prolonged PDOC patients included; equipment design limitations may have affected results; generalisability limited) | Serious (small sample n = 12; wide confidence interval on Cohen’s κ: −0.031 to 0.177; 50/288 trials 17.4% had no data) | Undetected (no evidence of selective reporting; limitations openly discussed) | Very Low |
| Kujawa et al., 2021 [33] | 6 UWS patients | Very Serious (very small sample n = 6; no blinding reported; variable session frequency and patient cooperation; convenience sample) | Serious (high variability in individual patient performance SD range 9.1 to 33.4; three patients showed considerable variability and sometimes no cooperation; non-significant results but trends observed) | Serious (study claims patients diagnosed as UWS but performed tasks suggesting MCS; diagnostic accuracy questioned by authors themselves; unclear clinical relevance of task completion percentages) | Very Serious (extremely small sample n = 6; no confidence intervals reported; wide standard deviations; non-significant statistical tests: p < 0.713 and p < 0.401) | Undetected (no evidence of selective reporting; negative results non-significance reported) | Very Low |
| Kujawa et al., 2022 [35] | 12 final (from 20 initial) | Very Serious (small final sample n = 12; very high attrition rate 40%: 3 failed calibrations, 5 died; convenience sample from single centre; no analysis of attrition impact) | Not Serious (consistent finding across all patients: dynamic > static; all statistical comparisons significant in same direction: p = 0.028, p = 0.002, p = 0.030) | Unclear (relevant population DOC patients; direct measurement of eye movements; however clinical relevance of static vs. dynamic distinction unclear; study limitation acknowledged: small sample and high mortality) | Very Serious (very small final sample n = 12; started n = 20, lost 40%; no confidence intervals reported; limited generalisability acknowledged by authors) | Undetected (no evidence of selective reporting; limitations openly discussed) | Very Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Estraneo, A.; Marcello, L.; Mancino, F.; De Feo, A.; Soricelli, A.; Franzese, M.; Cavaliere, C. Eye-Tracking Assessment in Patients with Disorders of Consciousness: A Systematic Review. Brain Sci. 2026, 16, 590. https://doi.org/10.3390/brainsci16060590
Estraneo A, Marcello L, Mancino F, De Feo A, Soricelli A, Franzese M, Cavaliere C. Eye-Tracking Assessment in Patients with Disorders of Consciousness: A Systematic Review. Brain Sciences. 2026; 16(6):590. https://doi.org/10.3390/brainsci16060590
Chicago/Turabian StyleEstraneo, Anna, Lorenza Marcello, Francesca Mancino, Alessia De Feo, Andrea Soricelli, Monica Franzese, and Carlo Cavaliere. 2026. "Eye-Tracking Assessment in Patients with Disorders of Consciousness: A Systematic Review" Brain Sciences 16, no. 6: 590. https://doi.org/10.3390/brainsci16060590
APA StyleEstraneo, A., Marcello, L., Mancino, F., De Feo, A., Soricelli, A., Franzese, M., & Cavaliere, C. (2026). Eye-Tracking Assessment in Patients with Disorders of Consciousness: A Systematic Review. Brain Sciences, 16(6), 590. https://doi.org/10.3390/brainsci16060590