

A Standard Operating Procedure for Dual-Task Training to Improve Physical and Cognitive Function in Older Adults: A Scoping Review





Abstract
1. Introduction
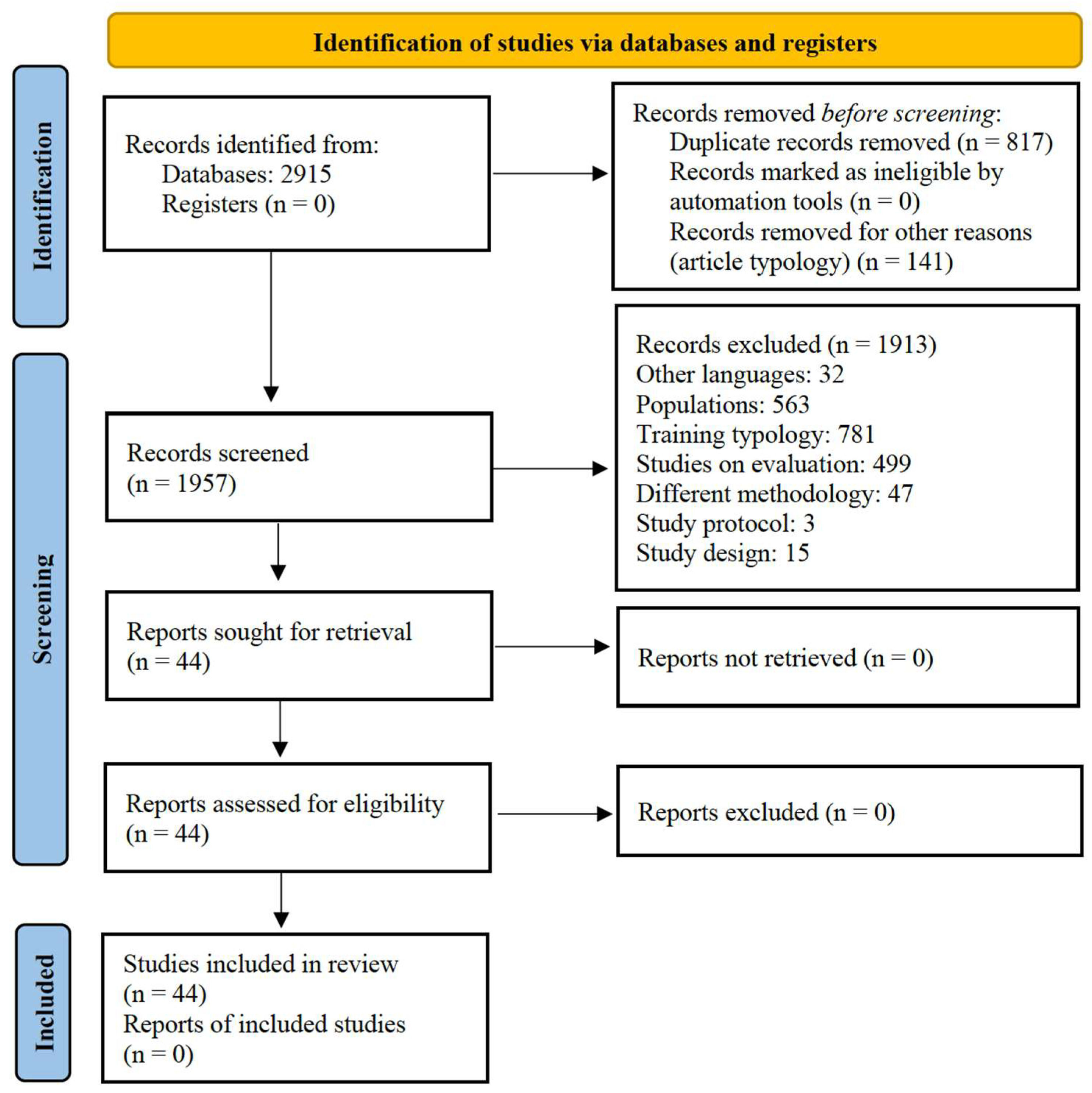
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Collection
- Group 1: dual task, double task;
- Group 2: training, protocol, practice, exercise;
- Group 3: cognitive function, cognition;
- Group 4: older adults, elderly.
2.3. Study Record
3. Results
3.1. Characteristics of the Studies
3.2. Description of the Intervention
3.3. Characteristics of the Dual-Task Training
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| DT | Dual task |
| SOP | Standard operating procedure |
References
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Petrigna, L.; Gentile, A.; Mani, D.; Pajaujiene, S.; Zanotto, T.; Thomas, E.; Paoli, A.; Palma, A.; Bianco, A. Dual-task conditions on static postural control in older adults: A systematic review and meta-analysis. J. Aging Phys. Act. 2020, 29, 162–177. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.J.; Kannan, P.; Wong, T.W.; Fong, K.N.K.; Winser, S.J. A Systematic Review Exploring the Theories Underlying the Improvement of Balance and Reduction in Falls Following Dual-Task Training among Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 16890. [Google Scholar] [CrossRef] [PubMed]
- Huxhold, O.; Li, S.-C.; Schmiedek, F.; Lindenberger, U. Dual-tasking postural control: Aging and the effects of cognitive demand in conjunction with focus of attention. Brain Res. Bull. 2006, 69, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Dubost, V.; Allali, G.; Gonthier, R.; Hermann, F.R.; Kressig, R.W. ‘Faster counting while walking’ as a predictor of falls in older adults. Age Ageing 2007, 36, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Al-Yahya, E.; Dawes, H.; Smith, L.; Dennis, A.; Howells, K.; Cockburn, J. Cognitive motor interference while walking: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2011, 35, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Omana, H.; Madou, E.; Montero-Odasso, M.; Payne, M.W.; Viana, R.; Hunter, S.W. The effect of dual-task testing on the balance and gait of people with lower limb amputations: A systematic review. PM R 2023, 15, 94–128. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, T.B.; Leite, P.B.; Doná, F.; Pompeu, J.E.; Swarowsky, A.; Torriani-Pasin, C. The effects of dual task gait and balance training in Parkinson’s disease: A systematic review. Physiother. Theory Pract. 2020, 36, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Muir-Hunter, S.W.; Wittwer, J.E. Dual-task testing to predict falls in community-dwelling older adults: A systematic review. Physiotherapy 2016, 102, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Abou, L.; Peters, J.; Fritz, N.E.; Sosnoff, J.J.; Kratz, A.L. Motor Cognitive Dual-Task Testing to Predict Future Falls in Multiple Sclerosis: A Systematic Review. Neurorehabil Neural Repair 2022, 36, 757–769. [Google Scholar] [CrossRef] [PubMed]
- Versi, N.; Murphy, K.; Robinson, C.; Franklin, M. Simultaneous Dual-Task Interventions That Improve Cognition in Older Adults: A Scoping Review of Implementation-Relevant Details. J. Aging Res. 2022, 2022, 6686910. [Google Scholar] [CrossRef] [PubMed]
- Petrigna, L.; Pajaujiene, S.; Iacona, G.M.; Thomas, E.; Paoli, A.; Bianco, A.; Palma, A. The execution of the grooved pegboard test in a dual-task situation: A pilot study. Heliyon 2020, 6, e04678. [Google Scholar] [CrossRef] [PubMed]
- Cedervall, Y.; Stenberg, A.M.; Åhman, H.B.; Giedraitis, V.; Tinmark, F.; Berglund, L.; Halvorsen, K.; Ingelsson, M.; Rosendahl, E.; Åberg, A.C. Timed Up-and-Go Dual-Task Testing in the Assessment of Cognitive Function: A Mixed Methods Observational Study for Development of the UDDGait Protocol. Int. J. Environ. Res. Public Health 2020, 17, 1715. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Kocher, M.; Finer, L.; Murata, N.; Stickley, C. Reliability of clinically feasible dual-task tests: Expanded timed get up and go test as a motor task on young healthy individuals. Gait Posture 2018, 60, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Li, X.; He, S.T.; Zhu, H.A.; Lam, F.M.H.; Pang, M.Y.C. The effect of dual-task training on cognitive ability, physical function, and dual-task performance in people with dementia or mild cognitive impairment: A systematic review and meta-analysis. Clin. Rehabil. 2024, 38, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Tian, H.; Thabane, L.; Ma, J.; Wu, H.; Zhong, Q.; Gao, Y.; Sun, C.; Zhu, Y.; Wang, T. The Effects of Dual-Task Training on Cognitive and Physical Functions in Older Adults with Cognitive Impairment; A Systematic Review and Meta-Analysis. J. Prev. Alzheimer’s Dis. 2022, 9, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Collette, F.; Olivier, L.; Van der Linden, M.; Laureys, S.; Delfiore, G.; Luxen, A.; Salmon, E. Involvement of both prefrontal and inferior parietal cortex in dual-task performance. Brain Res. Cogn. Brain Res. 2005, 24, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, M.; Castro, M.A.; Vilas-Boas, J.P. Muscular and Prefrontal Cortex Activity during Dual-Task Performing in Young Adults. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Paik, E. Functions of the prefrontal cortex in the human brain. J. Korean Med. Sci. 1998, 13, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Kirova, A.-M.; Bays, R.B.; Lagalwar, S. Working memory and executive function decline across normal aging, mild cognitive impairment, and Alzheimer’s disease. BioMed Res. Int. 2015, 2015, 748212. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Yin, S.; Lang, M.; He, R.; Li, J. The more the better? A meta-analysis on effects of combined cognitive and physical intervention on cognition in healthy older adults. Ageing Res. Rev. 2016, 31, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Ercan Yildiz, S.; Fidan, O.; Gulsen, C.; Colak, E.; Genc, G.A. Effect of dual-task training on balance in older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2024, 121, 105368. [Google Scholar] [CrossRef] [PubMed]
- Ghai, S.; Ghai, I.; Effenberg, A.O. Effects of dual tasks and dual-task training on postural stability: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 557–577. [Google Scholar] [CrossRef] [PubMed]
- Varela-Vásquez, L.A.; Minobes-Molina, E.; Jerez-Roig, J. Dual-task exercises in older adults: A structured review of current literature. J. Frailty Sarcopenia Falls 2020, 5, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Johansson, H.; Folkerts, A.K.; Hammarström, I.; Kalbe, E.; Leavy, B. Effects of motor-cognitive training on dual-task performance in people with Parkinson’s disease: A systematic review and meta-analysis. J. Neurol. 2023, 270, 2890–2907. [Google Scholar] [CrossRef] [PubMed]
- Pichierri, G.; Wolf, P.; Murer, K.; de Bruin, E.D. Cognitive and cognitive-motor interventions affecting physical functioning: A systematic review. BMC Geriatr. 2011, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Oliva, H.N.P.; Machado, F.S.M.; Rodrigues, V.D.; Leao, L.L.; Monteiro, R.S. The effect of dual-task training on cognition of people with different clinical conditions: An overview of systematic reviews. IBRO Rep. 2020, 9, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Fritz, N.E.; Cheek, F.M.; Nichols-Larsen, D.S. Motor-Cognitive Dual-Task Training in Persons With Neurologic Disorders: A Systematic Review. J. Neurol. Phys. Ther. 2015, 39, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Ozemek, C.; Bonikowske, A.; Christle, J.; Gallo, P. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2025. [Google Scholar]
- Angiuoli, S.V.; Gussman, A.; Klimke, W.; Cochrane, G.; Field, D.; Garrity, G.M.; Kodira, C.D.; Kyrpides, N.; Madupu, R.; Markowitz, V. Toward an online repository of standard operating procedures (SOPs) for (meta) genomic annotation. OMICS J. Integr. Biol. 2008, 12, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Tuck, M.K.; Chan, D.W.; Chia, D.; Godwin, A.K.; Grizzle, W.E.; Krueger, K.E.; Rom, W.; Sanda, M.; Sorbara, L.; Stass, S. Standard operating procedures for serum and plasma collection: Early detection research network consensus statement standard operating procedure integration working group. J. Proteome Res. 2009, 8, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Petrigna, L.; Pajaujiene, S.; Delextrat, A.; Gómez-López, M.; Paoli, A.; Palma, A.; Bianco, A. The importance of standard operating procedures in physical fitness assessment: A brief review. Sport Sci. Health 2022, 18, 21–26. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Araújo, E.M.; Coelho, H.J., Jr.; Sousa, C.V.; Rosa, T.D.; Neto, I.V.S.; Marzetti, E.; Franco, O.L.; Aguiar, S.D. Improving serum redox balance, inflammatory status, physical function, and cognitive ability through dual-task resistance training and detraining in nursing home residents. Exp. Gerontol. 2025, 200, 112662. [Google Scholar] [CrossRef] [PubMed]
- Chuang, I.C.; Chen, I.C.; Wu, Y.R.; Li, K.Y. Prediction and mediation analysis for treatment responses to combined cognitive and physical training for older adults. Sci. Rep. 2024, 14, 10571. [Google Scholar] [CrossRef] [PubMed]
- Jabeen, H.; Mahmood, T.; Mahmood, W.; Ahmad, N. Effects of Physical Cognitive Dual Task Training versus Conventional Single Task Training for Balance and Quality of Life among Older Adults—A Quasi Experimental Study. Int. J. Gerontol. 2024, 18, 258–262. [Google Scholar] [CrossRef]
- Rajalaxmi, V.; Arthi, J.; Kumar, G.M.; Muthukumaran, N.; Balathandayutham, K.; Saraswathi, K.; Kavitha, E. Effects of Dual Task Training Versus PNF Pattern on Balance and Cognition in Geriatric Population. Int. J. Life Sci. Pharma Res. 2022, 12, L1–L7. [Google Scholar] [CrossRef]
- Rezola-Pardo, C.; Arrieta, H.; Gil, S.M.; Zarrazquin, I.; Yanguas, J.J.; López, M.A.; Irazusta, J.; Rodriguez-Larrad, A. Comparison between multicomponent and simultaneous dual-task exercise interventions in long-term nursing home residents: The Ageing-ONDUAL-TASK randomized controlled study. Age Ageing 2019, 48, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Rezola-Pardo, C.; Irazusta, J.; Mugica-Errazquin, I.; Gamio, I.; Sarquis-Adamson, Y.; Gil, S.M.; Ugartemendia, M.; Montero-Odasso, M.; Rodriguez-Larrad, A. Effects of multicomponent and dual-task exercise on falls in nursing homes: The AgeingOn Dual-Task study. Maturitas 2022, 164, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Yuzlu, V.; Oguz, S.; Timurtas, E.; Aykutoglu, E.; Polat, M.G. The Effect of 2 Different Dual-Task Balance Training Methods on Balance and Gait in Older Adults: A Randomized Controlled Trial. Phys. Ther. 2022, 102, pzab298. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, S.; Yamada, M.; Tanigawa, T.; Sekiyama, K.; Kawagoe, T.; Suzuki, M.; Yoshikawa, S.; Abe, N.; Otsuka, Y.; Nakai, R.; et al. A 12-Week Physical and Cognitive Exercise Program Can Improve Cognitive Function and Neural Efficiency in Community-Dwelling Older Adults: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Trombini-Souza, F.; de Moura, V.T.G.; da Silva, L.W.N.; dos Santos Leal, I.; Nascimento, C.A.; Silva, P.S.T.; Perracini, M.R.; Sacco, I.C.N.; de Araújo, R.C.; de Maio Nascimento, M. Effects of two different dual-task training protocols on gait, balance, and cognitive function in community-dwelling older adults: A 24-week randomized controlled trial. PeerJ 2023, 11, e15030. [Google Scholar] [CrossRef] [PubMed]
- Anandh, S.; Varadharajulu, G.; Alate, M.M.; Mane, D.A. Effect of dual task training on balance and gait over regular and diversified land surfaces in independent elderly. Int. J. Curr. Res. Rev. 2021, 13, 165–168. [Google Scholar] [CrossRef]
- Akin, H.; Senel, A.; Taskiran, H.; Kaya Mutlu, E. Do motor-cognitive and motor-motor dual task training effect differently balance performance in older adults? Eur. Geriatr. Med. 2021, 12, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Amini, A.; Vaezmousavi, M.; Shirvani, H. The effectiveness of cognitive-motor training on reconstructing cognitive health components in older male adults, recovered from the COVID-19. Neurol. Sci. 2022, 43, 1395–1403. [Google Scholar] [CrossRef] [PubMed]
- Silsupadol, P.; Shumway-Cook, A.; Lugade, V.; van Donkelaar, P.; Chou, L.S.; Mayr, U.; Woollacott, M.H. Effects of single-task versus dual-task training on balance performance in older adults: A double-blind, randomized controlled trial. Arch. Phys. Med. Rehabil. 2009, 90, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Ansai, J.H.; de Andrade, L.P.; Buto, M.S.D.; Barroso, V.D.; Farche, A.C.S.; Rossi, P.G.; Takahashi, A.C.D. Effects of the Addition of a Dual Task to a Supervised Physical Exercise Program on Older Adults’ Cognitive Performance. J. Aging Phys. Act. 2017, 25, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.F.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- American Geriatrics Society Panel on Exercise and Osteoarthritis (A.G.S.P.). Exercise prescription for older adults with osteoarthritis pain: Consensus practice recommendations. A supplement to the AGS Clinical Practice Guidelines on the management of chronic pain in older adults. J. Am. Geriatr. Soc. 2001, 49, 808–823. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Araújo, E.M.; Uchida, M.C.; Marzetti, E.; Aguiar, S.D.S. Effects of resistance training associated with a verbal fluency task on physical performance and cognitive function in frail nursing home residents. Arch. Gerontol. Geriatr. 2024, 121, 105353. [Google Scholar] [CrossRef] [PubMed]
- Castaño, L.A.A.; Castillo de Lima, V.; Barbieri, J.F.; de Lucena, E.G.P.; Gáspari, A.F.; Arai, H.; Teixeira, C.V.L.; Coelho-Júnior, H.J.; Uchida, M.C. Resistance Training Combined With Cognitive Training Increases Brain Derived Neurotrophic Factor and Improves Cognitive Function in Healthy Older Adults. Front. Psychol. 2022, 13, 870561. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, H.; Khanmohammadi, R.; Olyaei, G.; Talebian, S.; Hadian, M.R.; Najafi, M. Video game and motor-cognitive dual-task training could be suitable treatments to improve dual-task interference in older adults. Neurosci. Lett. 2021, 760, 136099. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, L.L.; Cordes, T.; Meixner, C.; Schoene, D.; Voelcker-Rehage, C.; Wollesen, B. Can cognitive-motor training improve physical functioning and psychosocial wellbeing in nursing home residents? A randomized controlled feasibility study as part of the PROCARE project. Aging Clin. Exp. Res. 2021, 33, 943–956. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- de Souto Barreto, P.; Morley, J.E.; Chodzko-Zajko, W.; Pitkala, K.H.; Weening-Djiksterhuis, E.; Rodriguez-Mañas, L.; Barbagallo, M.; Rosendahl, E.; Sinclair, A.; Landi, F. Recommendations on physical activity and exercise for older adults living in long-term care facilities: A taskforce report. J. Am. Med. Dir. Assoc. 2016, 17, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Wollesen, B.; Mattes, K.; Schulz, S.; Bischoff, L.L.; Seydell, L.; Bell, J.W.; von Duvillard, S.P. Effects of Dual-Task Management and Resistance Training on Gait Performance in Older Individuals: A Randomized Controlled Trial. Front. Aging Neurosci. 2017, 9, 415. [Google Scholar] [CrossRef] [PubMed]
- Wollesen, B.; Voelcker-Rehage, C. Training effects on motor-cognitive dual-task performance in older adults: A systematic review. Eur. Rev. Aging Phys. Act. 2014, 11, 5–24. [Google Scholar] [CrossRef]
- Sherrington, C.; Whitney, J.C.; Lord, S.R.; Herbert, R.D.; Cumming, R.G.; Close, J.C. Effective exercise for the prevention of falls: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2008, 56, 2234–2243. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J.; Latham, N.K. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst. Rev. 2009, 2009, Cd002759. [Google Scholar] [CrossRef] [PubMed]
- Fiatarone, M.A.; Marks, E.C.; Ryan, N.D.; Meredith, C.N.; Lipsitz, L.A.; Evans, W.J. High-intensity strength training in nonagenarians: Effects on skeletal muscle. Jama 1990, 263, 3029–3034. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Mackintosh, S.; Halbert, J. Does the ‘Otago exercise programme’reduce mortality and falls in older adults?: A systematic review and meta-analysis. Age Ageing 2010, 39, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Wollesen, B.; Schulz, S.; Seydell, L.; Delbaere, K. Does dual task training improve walking performance of older adults with concern of falling? BMC Geriatr. 2017, 17, 213. [Google Scholar] [CrossRef] [PubMed]
- Wollesen, B.; Voelcker-Rehage, C.; Willer, J.; Zech, A.; Mattes, K. Feasibility study of dual-task-managing training to improve gait performance of older adults. Aging Clin. Exp. Res. 2015, 27, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Littbrand, H.; Carlsson, M.; Lundin-Olsson, L.; Lindelöf, N.; Håglin, L.; Gustafson, Y.; Rosendahl, E. Effect of a high-intensity functional exercise program on functional balance: Preplanned subgroup analyses of a randomized controlled trial in residential care facilities. J. Am. Geriatr. Soc. 2011, 59, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Blasco-Lafarga, C.; Cordellat, A.; Forte, A.; Roldán, A.; Monteagudo, P. Short and Long-Term Trainability in Older Adults: Training and Detraining Following Two Years of Multicomponent Cognitive-Physical Exercise Training. Int. J. Environ. Res. Public Health 2020, 17, 5984. [Google Scholar] [CrossRef] [PubMed]
- Blasco-Lafarga, C.; Martinez-Navarro, I.; Cordellat, A.; Roldán, A.; Monteagudo, P.; Sanchis-Soler, G.; Sanchis-Sanchis, R. Método de Entrenamiento Funcional Cognitivo Neuromotor. España Pat. 2016, 156, 24. [Google Scholar]
- Chen, Y.L.; Tseng, C.H.; Lin, H.T.; Wu, P.Y.; Chao, H.C. Dual-task multicomponent exercise-cognitive intervention improved cognitive function and functional fitness in older adults. Aging Clin. Exp. Res. 2023, 35, 1855–1863. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J. ACSM’s Exercise for Older Adults; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Conradsson, D.; Halvarsson, A. The effects of dual-task balance training on gait in older women with osteoporosis: A randomized controlled trial. Gait Posture 2019, 68, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Halvarsson, A.; Dohrn, I.-M.; Ståhle, A. Taking balance training for older adults one step further: The rationale for and a description of a proven balance training programme. Clin. Rehabil. 2015, 29, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.M.; Maduro, P.A.; Rios, P.M.B.; Nascimento, L.D.S.; Silva, C.N.; Kliegel, M.; Ihle, A. The Effects of 12-Week Dual-Task Physical-Cognitive Training on Gait, Balance, Lower Extremity Muscle Strength, and Cognition in Older Adult Women: A Randomized Study. Int. J. Environ. Res. Public Health 2023, 20, 5498. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.D.; Maduro, P.A.; Rios, P.M.B.; Nascimento, L.D.; Silva, C.N.; Kliegel, M.; Ihle, A. Effects of 12 Weeks of Physical-Cognitive Dual-Task Training on Executive Functions, Depression, Sleep Quality, and Quality of Life in Older Adult Women: A Randomized Pilot Study. Sustainability 2023, 15, 97. [Google Scholar] [CrossRef]
- Falbo, S.; Condello, G.; Capranica, L.; Forte, R.; Pesce, C. Effects of Physical-Cognitive Dual Task Training on Executive Function and Gait Performance in Older Adults: A Randomized Controlled Trial. BioMed Res. Int. 2016, 2016, 5812092. [Google Scholar] [CrossRef] [PubMed]
- Voelcker-Rehage, C.; Niemann, C. Structural and functional brain changes related to different types of physical activity across the life span. Neurosci. Biobehav. Rev. 2013, 37, 2268–2295. [Google Scholar] [CrossRef] [PubMed]
- Granacher, U.; Muehlbauer, T.; Göstemeyer, G.; Gruber, S.; Gruber, M. The performance of balance exercises during daily tooth brushing is not sufficient to improve balance and muscle strength in healthy older adults. BMC Geriatr. 2021, 21, 257. [Google Scholar] [CrossRef] [PubMed]
- Muehlbauer, T.; Roth, R.; Bopp, M.; Granacher, U. An exercise sequence for progression in balance training. J. Strength Cond. Res. 2012, 26, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Gregory, M.A.; Gill, D.P.; Zou, G.; Liu-Ambrose, T.; Shigematsu, R.; Fitzgerald, C.; Hachinski, V.; Shoemaker, K.; Petrella, R.J. Group-based exercise combined with dual-task training improves gait but not vascular health in active older adults without dementia. Arch. Gerontol. Geriatr. 2016, 63, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Gill, D.P.; Gregory, M.A.; Zou, G.; Liu-Ambrose, T.; Shigematsu, R.; Hachinski, V.; Fitzgerald, C.; Petrella, R.J. The Healthy Mind, Healthy Mobility Trial: A Novel Exercise Program for Older Adults. Med. Sci. Sports Exerc. 2016, 48, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Halvarsson, A.; Franzén, E.; Ståhle, A. Balance training with multi-task exercises improves fall-related self-efficacy, gait, balance performance and physical function in older adults with osteoporosis: A randomized controlled trial. Clin. Rehabil. 2015, 29, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Halvarsson, A.; Oddsson, L.; Franzén, E.; Ståhle, A. Long-term effects of a progressive and specific balance-training programme with multi-task exercises for older adults with osteoporosis: A randomized controlled study. Clin. Rehabil. 2016, 30, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Ho, V.; Chan, Y.H.; Merchant, R.A. Patterns of improvement in functional ability and predictors of responders to dual-task exercise: A latent class analysis. Front. Public Health 2022, 10, 1069970. [Google Scholar] [CrossRef] [PubMed]
- Merchant, R.A.; Tsoi, C.; Tan, W.; Lau, W.; Sandrasageran, S.; Arai, H. Community-based peer-led intervention for healthy ageing and evaluation of the ‘HAPPY’program. J. Nutr. Health Aging 2021, 25, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Tasvuran Horata, E.; Cetin, S.Y.; Erel, S. Effects of individual progressive single- and dual-task training on gait and cognition among older healthy adults: A randomized-controlled comparison study. Eur. Geriatr. Med. 2021, 12, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Brustio, P.R.; Rabaglietti, E.; Formica, S.; Liubicich, M.E. Dual-task training in older adults: The effect of additional motor tasks on mobility performance. Arch. Gerontol. Geriatr. 2018, 75, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Jardim, N.Y.V.; Bento-Torres, N.V.O.; Costa, V.O.; Carvalho, J.P.R.; Pontes, H.T.S.; Tomás, A.M.; Sosthenes, M.C.K.; Erickson, K.I.; Bento-Torres, J.; Diniz, C.W.P. Dual-Task Exercise to Improve Cognition and Functional Capacity of Healthy Older Adults. Front. Aging Neurosci. 2021, 13, 589299. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Yoo, G.E. Rhythm-Motor Dual Task Intervention for Fall Prevention in Healthy Older Adults. Front. Psychol. 2019, 10, 3027. [Google Scholar] [CrossRef] [PubMed]
- Kitazawa, K.; Showa, S.; Hiraoka, A.; Fushiki, Y.; Sakauchi, H.; Mori, M. Effect of a dual-task net-step exercise on cognitive and gait function in older adults. J. Geriatr. Phys. Ther. 2015, 38, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Konak, H.E.; Kibar, S.; Ergin, E.S. The effect of single-task and dual-task balance exercise programs on balance performance in adults with osteoporosis: A randomized controlled preliminary trial. Osteoporos. Int. 2016, 27, 3271–3278. [Google Scholar] [CrossRef] [PubMed]
- Mundada, P.H.; Dadgal, R.M. Comparison of Dual Task Training Versus Aerobics Training in Improving Cognition in Healthy Elderly Population. Cureus 2022, 14, e29027. [Google Scholar] [CrossRef] [PubMed]
- Nieto-Guisado, A.; Solana-Tramunt, M.; Cabrejas, C.; Morales, J. The Effects of an 8-Week Cognitive-Motor Training Program on Proprioception and Postural Control Under Single and Dual Task in Older Adults: A Randomized Clinical Trial. Healthcare 2024, 12, 2297. [Google Scholar] [CrossRef] [PubMed]
- Me, N. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar]
- Norouzi, E.; Vaezmosavi, M.; Gerber, M.; Pühse, U.; Brand, S. Dual-task training on cognition and resistance training improved both balance and working memory in older people. Phys. Sportsmed. 2019, 47, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Pantoja-Cardoso, A.; Aragao-Santos, J.C.; Santos, P.D.; Dos-Santos, A.C.; Silva, S.R.; Lima, N.B.C.; Vasconcelos, A.B.S.; Fortes, L.D.; Da Silva-Grigoletto, M.E. Functional Training and Dual-Task Training Improve the Executive Function of Older Women. Geriatrics 2023, 8, 83. [Google Scholar] [CrossRef] [PubMed]
- Párraga-Montilla, J.A.; Aibar-Almazán, A.; Cabrera-Linares, J.C.; Lozano-Aguilera, E.; Huete, V.S.; Arrieta, M.D.E.; Latorre-Román, P.A. A Randomized Controlled Trial Protocol to Test the Efficacy of a Dual-Task Multicomponent Exercise Program vs. a Simple Program on Cognitive and Fitness Performance in Elderly People. Int. J. Environ. Res. Public Health 2021, 18, 6507. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, H.; Rezola-Pardo, C.; Zarrazquin, I.; Echeverria, I.; Yanguas, J.J.; Iturburu, M.; Gil, S.M.; Rodriguez-Larrad, A.; Irazusta, J. A multicomponent exercise program improves physical function in long-term nursing home residents: A randomized controlled trial. Exp. Gerontol. 2018, 103, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Larrad, A.; Arrieta, H.; Rezola, C.; Kortajarena, M.; Yanguas, J.J.; Iturburu, M.; Susana, M.G.; Irazusta, J. Effectiveness of a multicomponent exercise program in the attenuation of frailty in long-term nursing home residents: Study protocol for a randomized clinical controlled trial. BMC Geriatr. 2017, 17, 60. [Google Scholar] [CrossRef] [PubMed]
- Rosado, H.; Bravo, J.; Raimundo, A.; Carvalho, J.; Marmeleira, J.; Pereira, C. Effects of two 24-week multimodal exercise programs on reaction time, mobility, and dual-task performance in community-dwelling older adults at risk of falling: A randomized controlled trial. BMC Public Health 2021, 21, 408. [Google Scholar] [CrossRef] [PubMed]
- Santos, P.C.; Machado, D.R.L.; Abdalla, P.P.; Santos, C.V.; Lopes, S.; Martins, A.C.; Mota, J.; Mesquita, C. Otago Exercise Program Plus Cognitive Dual-task can Reduce Fall Risk, Improve Cognition and Functioning in Older Adults. Curr. Aging Sci. 2023, 16, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.C.; Santos, C.; Silva, C.; Baltazar, D.; Moreira, J.; Tavares, N. Does modified Otago Exercise Program improves balance in older people? A systematic review. Prev. Med. Rep. 2018, 11, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Sedaghati, P.; Goudarzian, M.; Ahmadabadi, S.; Tabatabai-Asl, S.M. The impact of a multicomponent-functional training with postural correction on functional balance in the elderly with a history of falling. J. Exp. Orthop. 2022, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Agmon, M.; Belza, B.; Nguyen, H.Q.; Logsdon, R.G.; Kelly, V.E. A systematic review of interventions conducted in clinical or community settings to improve dual-task postural control in older adults. Clin. Interv. Aging 2014, 9, 477–492. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.; Rosado, H.; Cruz-Ferreira, A.; Marmeleira, J. Effects of a 10-week multimodal exercise program on physical and cognitive function of nursing home residents: A psychomotor intervention pilot study. Aging Clin. Exp. Res. 2018, 30, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Rezola-Pardo, C.; Arrieta, H.; Gil, S.M.; Yanguas, J.J.; Iturburu, M.; Irazusta, J.; Sanz, B.; Rodriguez-Larrad, A. A randomized controlled trial protocol to test the efficacy of a dual-task multicomponent exercise program in the attenuation of frailty in long-term nursing home residents: Aging-ON(DUAL-TASK) study. BMC Geriatr. 2019, 19, 6. [Google Scholar] [CrossRef] [PubMed]
- Sok, S.; Shin, E.; Kim, S.; Kim, M. Effects of Cognitive/Exercise Dual-Task Program on the Cognitive Function, Health Status, Depression, and Life Satisfaction of the Elderly Living in the Community. Int. J. Environ. Res. Public Health 2021, 18, 7848. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Joung, J.; Shin, S.H. Effects of Fumanet exercise on Korean older adults with mild dementia. Jpn. J. Nurs. Sci. 2020, 17, e12286. [Google Scholar] [CrossRef] [PubMed]
- Tait, J.L.; Duckham, R.L.; Rantalainen, T.; Milte, C.M.; Main, L.C.; Nowson, C.A.; Sanders, K.M.; Taaffe, D.R.; Hill, K.D.; Abbott, G.; et al. Effects of a 6-month dual-task, power-based exercise program on cognitive function, neurological and inflammatory markers in older adults: Secondary analysis of a cluster randomised controlled trial. Geroscience 2025, 47, 1251–1268. [Google Scholar] [CrossRef] [PubMed]
- Trombini-Souza, F.; de Maio Nascimento, M.; da Silva, T.F.A.; de Araújo, R.C.; Perracini, M.R.; Sacco, I.C.N. Dual-task training with progression from variable- to fixed-priority instructions versus dual-task training with variable-priority on gait speed in community-dwelling older adults: A protocol for a randomized controlled trial: Variable- and fixed-priority dual-task for older adults. BMC Geriatr. 2020, 20, 76. [Google Scholar] [CrossRef]
- Yokoyama, H.; Okazaki, K.; Imai, D.; Yamashina, Y.; Takeda, R.; Naghavi, N.; Ota, A.; Hirasawa, Y.; Miyagawa, T. The effect of cognitive-motor dual-task training on cognitive function and plasma amyloid β peptide 42/40 ratio in healthy elderly persons: A randomized controlled trial. BMC Geriatr. 2015, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Sergeant, J.A.; Geurts, H.; Oosterlaan, J. How specific is a deficit of executive functioning for attention-deficit/hyperactivity disorder? Behav. Brain Res. 2002, 130, 3–28. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E.; Sherman, E.; Spreen, O. Trail making test. In A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary, 3rd ed.; Oxford University Press: Oxford, UK, 2006; pp. 655–677. [Google Scholar]
- Shigematsu, R.; Okura, T. A novel exercise for improving lower-extremity functional fitness in the elderly. Aging Clin. Exp. Res. 2006, 18, 242–248. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, T.C.G.; Soares, F.C.; De Macedo, L.D.E.D.; Diniz, D.L.W.P.; Bento-Torres, N.V.O.; Picanço-Diniz, C.W. Beneficial effects of multisensory and cognitive stimulation on age-related cognitive decline in long-term-care institutions. Clin. Interv. Aging 2014, 9, 309–321. [Google Scholar] [PubMed]
- Kim, S.J.; Cho, S.-R.; Yoo, G.E. Age-related changes in bimanual instrument playing with rhythmic cueing. Front. Psychol. 2017, 8, 1569. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Cho, S.R.; Yoo, G.E. The Applicability of Rhythm-Motor Tasks to a New Dual Task Paradigm for Older Adults. Front. Neurol. 2017, 8, 671. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Aoyama, T.; Tanaka, B.; Nagai, K.; Ichihashi, N. Seated stepping exercise in a dual-task condition improves ambulatory function with a secondary task: A randomized controlled trial. Aging Clin. Exp. Res. 2011, 23, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Tanaka, B.; Nagai, K.; Aoyama, T.; Ichihashi, N. Rhythmic stepping exercise under cognitive conditions improves fall risk factors in community-dwelling older adults: Preliminary results of a cluster-randomized controlled trial. Aging Ment. Health 2011, 15, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Dorfman, M.; Herman, T.; Brozgol, M.; Shema, S.; Weiss, A.; Hausdorff, J.M.; Mirelman, A. Dual-task training on a treadmill to improve gait and cognitive function in elderly idiopathic fallers. J. Neurol. Phys. Ther. 2014, 38, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Halvarsson, A.; Olsson, E.; Farén, E.; Pettersson, A.; Ståhle, A. Effects of new, individually adjusted, progressive balance group training for elderly people with fear of falling and tend to fall: A randomized controlled trial. Clin. Rehabil. 2011, 25, 1021–1031. [Google Scholar] [CrossRef] [PubMed]
- Silsupadol, P.; Siu, K.-C.; Shumway-Cook, A.; Woollacott, M.H. Training of balance under single-and dual-task conditions in older adults with balance impairment. Phys. Ther. 2006, 86, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.-H.; Kim, M.-J.; Woo, H.-J.; Kim, Y.-S.; Kim, M.-H.; Song, S.-R.; Kang, S.-M.; Choi, Y.-W.; Kim, J.-H. Effect of CLX training combined with PNF pattern on balance ability. J. Korean Phys. Ther. Sci. 2019, 26, 1–8. [Google Scholar] [CrossRef]
- Weeks, D.L.; Forget, R.; Mouchnino, L.; Gravel, D.; Bourbonnais, D. Interaction between attention demanding motor and cognitive tasks and static postural stability. Gerontology 2003, 49, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Hollman, J.H.; Kovash, F.M.; Kubik, J.J.; Linbo, R.A. Age-related differences in spatiotemporal markers of gait stability during dual task walking. Gait Posture 2007, 26, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Wollesen, B.; Wildbredt, A.; van Schooten, K.S.; Lim, M.L.; Delbaere, K. The effects of cognitive-motor training interventions on executive functions in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Paillard, T. The optimal method for improving postural balance in healthy young and older people: Specific training for postural tasks encountered in personal physical practice. Front. Physiol. 2023, 14, 1188496. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, S.; Kumpulainen, S.; Pesola, A.J. Strength-Cognitive Training: A Systemic Review in Adults and Older Adults, and Guidelines to Promote “Strength Exergaming” Innovations. Front. Psychol. 2022, 13, 855703. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.; Domingos, C.; Monteiro, D.; Morouco, P. A Review on Aging, Sarcopenia, Falls, and Resistance Training in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 874. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Lupión, D.; Chirosa-Ríos, L.; Martínez-García, D.; Rodríguez-Pérez, M.; Jerez-Mayorga, D. Effects of Power Training on Functional Capacity Related to Fall Risk in Older Adults: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2023, 104, 1514–1525. [Google Scholar] [CrossRef] [PubMed]
- Syed-Abdul, M.M. Benefits of Resistance Training in Older Adults. Curr. Aging Sci. 2021, 14, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.; Fidalgo, A.; Farinatti, P.; Monteiro, W. Effects of high-intensity interval and continuous moderate aerobic training on fitness and health markers of older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2024, 124, 105451. [Google Scholar] [CrossRef] [PubMed]
- Sert, H.; Gulbahar Eren, M.; Gurcay, B.; Koc, F. The effectiveness of a high-intensity interval exercise on cardiometabolic health and quality of life in older adults: A systematic review and meta-analysis. BMC Sports Sci. Med. Rehabil. 2025, 17, 128. [Google Scholar] [CrossRef] [PubMed]
- Treacy, D.; Hassett, L.; Schurr, K.; Fairhall, N.J.; Cameron, I.D.; Sherrington, C. Mobility training for increasing mobility and functioning in older people with frailty. Cochrane Database Syst. Rev. 2022, 6, Cd010494. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, L.V.; Hassan, S.A.; Kasawara, K.T.; Reid, W.D. The effect of mental tracking task on spatiotemporal gait parameters in healthy younger and middle-and older aged participants during dual tasking. Exp. Brain Res. 2019, 237, 3123–3132. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Huang, C.J.; Chen, K.F.; Hung, T.M. Physical activity and working memory in healthy older adults: An ERP study. Psychophysiol. 2013, 50, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Buschkuehl, M.; Jaeggi, S.M.; Hutchison, S.; Perrig-Chiello, P.; Däpp, C.; Müller, M.; Breil, F.; Hoppeler, H.; Perrig, W.J. Impact of working memory training on memory performance in old-old adults. Psychol. Aging 2008, 23, 743. [Google Scholar] [CrossRef] [PubMed]
- Heinzel, S.; Schulte, S.; Onken, J.; Duong, Q.-L.; Riemer, T.G.; Heinz, A.; Kathmann, N.; Rapp, M.A. Working memory training improvements and gains in non-trained cognitive tasks in young and older adults. Aging Neuropsychol. Cogn. 2014, 21, 146–173. [Google Scholar] [CrossRef] [PubMed]
- Camicioli, R.; Howieson, D.; Lehman, S.; Kaye, J. Talking while walking: The effect of a dual task in aging and Alzheimer’s disease. Neurology 1997, 48, 955–958. [Google Scholar] [CrossRef] [PubMed]
- Fournet, M.; Pernon, M.; Catalano Chiuvé, S.; Lopez, U.; Laganaro, M. Attention in post-lexical processes of utterance production: Dual-task cost in younger and older adults. Q. J. Exp. Psychol. 2021, 74, 1852–1872. [Google Scholar] [CrossRef] [PubMed]
- Rafiee Manesh, V.; Inanlu, M.; Yekaninejad, M.S.; Khanmohammadi, R. The effect of different types of cognitive tasks on postural sway fluctuations in older and younger adults: A nonlinear study. J. Bodyw. Mov. Ther. 2024, 37, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Friedman, A.; Polson, M.C.; Dafoe, C.G.; Gaskill, S.J. Dividing attention within and between hemispheres: Testing a multiple resources approach to limited-capacity information processing. J. Exp. Psychol. Hum. Percept. Perform. 1982, 8, 625. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.O.d.; Carvalho de Abreu, D.C.; Moraes, R. Performance of faller and nonfaller older adults on a motor–motor interference task. J. Mot. Behav. 2018, 50, 293–306. [Google Scholar] [CrossRef] [PubMed]
- Navon, D.; Miller, J. Role of outcome conflict in dual-task interference. J. Exp. Psychol. Hum. Percept. Perform. 1987, 13, 435. [Google Scholar] [CrossRef] [PubMed]
- Pashler, H. Dual-task interference in simple tasks: Data and theory. Psychol. Bull. 1994, 116, 220. [Google Scholar] [CrossRef] [PubMed]
- Malik, J.; Stemplewski, R.; Maciaszek, J. The Effect of Juggling as Dual-Task Activity on Human Neuroplasticity: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 7102. [Google Scholar] [CrossRef] [PubMed]
- Bherer, L. Cognitive plasticity in older adults: Effects of cognitive training and physical exercise. Ann. N. Y. Acad. Sci. 2015, 1337, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Lin, L.L.; Hwang, I.S. Age-Related Differences in Reorganization of Functional Connectivity for a Dual Task with Increasing Postural Destabilization. Front. Aging Neurosci. 2017, 9, 96. [Google Scholar] [CrossRef] [PubMed]
- Hwang, I.S.; Huang, C.Y. Neural Correlates of Task Cost for Stance Control with an Additional Motor Task: Phase-Locked Electroencephalogram Responses. PLoS ONE 2016, 11, e0151906. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Woollacott, M. Attentional demands and postural control: The effect of sensory context. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M10–M16. [Google Scholar] [CrossRef] [PubMed]
- Rankin, J.K.; Woollacott, M.H.; Shumway-Cook, A.; Brown, L.A. Cognitive influence on postural stability: A neuromuscular analysis in young and older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M112–M119. [Google Scholar] [CrossRef] [PubMed]
- Law, L.L.; Barnett, F.; Yau, M.K.; Gray, M.A. Effects of combined cognitive and exercise interventions on cognition in older adults with and without cognitive impairment: A systematic review. Ageing Res. Rev. 2014, 15, 61–75. [Google Scholar] [CrossRef] [PubMed]
- Papegaaij, S.; Taube, W.; Baudry, S.; Otten, E.; Hortobágyi, T. Aging causes a reorganization of cortical and spinal control of posture. Front. Aging Neurosci. 2014, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Gallou-Guyot, M.; Mandigout, S.; Bherer, L.; Perrochon, A. Effects of exergames and cognitive-motor dual-task training on cognitive, physical and dual-task functions in cognitively healthy older adults: An overview. Ageing Res. Rev. 2020, 63, 101135. [Google Scholar] [CrossRef] [PubMed]
- Papale, O.; Di Rocco, F.; Festino, E.; Gammino, V.; Cortis, C.; Fusco, A. Do Hand Exercises Influence Physiological Hand Tremor? An Observational Cohort Study on Healthy Young Adults. Appl. Sci. 2024, 14, 4467. [Google Scholar] [CrossRef]
- Hong, X.L.; Cheng, L.J.; Feng, R.C.; Goh, J.; Gyanwali, B.; Itoh, S.; Tam, W.S.W.; Wu, X.V. Effect of physio-cognitive dual-task training on cognition in pre-ageing and older adults with neurocognitive disorders: A meta-analysis and meta-regression of randomized controlled trial. Arch. Gerontol. Geriatr. 2024, 116, 105161. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| 1st Author and Year | N and Sample Age | Duration, Frequency, Time | Intensity/Type/Protocol | Adverse Events/Adherence and Dropout |
|---|---|---|---|---|
| Akin 2021 [44] | 50, 68 yr | 8-weeks, 40-min, G | 10 min WU, 20 min C, 10 min CD | No dropout |
| Amini 2022 [45] | 42, 70 yr | 4-weeks, 2/week, 45-min | I: progressive. ACSM, protocol [46] | No dropout |
| Anandh 2018 [43] | 96, 65–75 yr | 3 ses of training | 10 min WU, walking: 5 min | NI |
| Ansai 2017 [47] | 80, 68 yr | 12-weeks, 3/week, 50-min, G | 10 min WU, 30 min C, 10 min S. ACSM [48], AGSPEO [49] | Training adherence: >70% |
| Machado Araújo 2025 [34] | 11, 83 yr | 12-weeks, 2/week, small G | I: progressive, %1 RM, protocol [50,51] | Dropout rates: <25% |
| Arcila Castaño 2022 [51] | 30, 70 yr | 16-weeks, 2/week, G | I: progressive, %1 RM | Dropout rates: <20% |
| Bagheri 2021 [52] | 70, 65 yr | 16 ses, 3/week, 60-min | I: progressive-adapted | Dropout rates: <12% |
| Bischoff 2021 [53] | 24, 83 yr | 16-weeks, 2/week, 45–60-min | 5–10 min WU-mobilization, 40 min C, 5–10 min CD. I: progressive. ACSM [54], protocol [55,56,57,58,59,60,61,62,63,64] | Dropout rates: <4%; Training adherence: >75% |
| Blasco-Lafarga 2020 [65] | 25, 70 yr | Protocol [66], G | 5–10 min CD (amusing, social tasks). I: adapted. Protocol [66] | Dropout rates: <26% |
| Chen 2023 [67] | 50, 68 yr | 12-weeks, 2/week, 90-min, G | 10–15 min WU, 60 min C, 15–20 min S. I: progressive. ACSM [68] | NI |
| Chuang 2024 [35] | 158, 74 yr | 12 ses, 1/week, 120-min | NI | Dropout rates: <12% |
| Conradsson 2019 [69] | 95, 76 yr | 12-weeks, 3/week, 45-min, G | 5 min WU (walk), 30 min C, 5 min CD (walk, S). I: progressive-adapted. Protocol [70] | NI |
| de Maio Nascimento 2023 [71] | 50, 66 yr | 12-weeks, 2/week, 60-min | 10 min WU, 40 min C, 10 min relax. I: progressive. Protocol [72] | Training adherence: >75% |
| Falbo 2016 [73] | 36, 72 yr | 12-weeks, 2/week, 60-min, G | 10 min WU, 30 min C, 20 min S, relax. I: adapted. Protocol [74] | Dropout rates: <36% |
| Granacher 2021 [75] | 51, 66 yr | 8-weeks, daily, 2 per day | I: progressive. Protocol [76] | Training adherence: >92% |
| Gregory 2016 [77] | 44, 73 yr | 26-weeks, 2–3/week, 60–75-min, G–I | I: target heart rate (70–85% max HR). Protocol [78] | Training adherence: >78% |
| Halvarsson 2015 [79] | 69, 76 yr | 12-weeks, 3/week, 45-min, G | I: 3 levels (basic, moderate, advanced), progressive | Training adherence: >89% |
| Halvarsson 2016 [80] | 96, 76 yr | 12-weeks, 3/week, 45-min, G | I: progressive. Protocol [70] | Dropout rates: <12% |
| Ho 2023 [81] | 136, 75 yr | 12-weeks, 2/week, 60-min | Protocol [82] | NI |
| Horata 2021 [83] | 32, 65 yr | 6-weeks, 2/week, 60-min, I | 10 min WU, 10 min CD (breathing, S). I: progressive-adapted. Protocol [84] | Dropout rates: <16% |
| Jabeen 2024 [36] | 30, 62 yr | 6-weeks, 3/week, 40-min | NI | No dropout |
| Jardim 2021 [85] | 72, 67 yr | 24 ses, 2/week, 75-min, G | 10 min WU, 60 min C, 5 min S. I: moderate (60–70% of max HR). Protocol [54] | Dropout rates: <22% |
| Kim 2019 [86] | 20, 79 yr | 8-weeks, 2/week, 30-min, I | I: adapted | NI |
| Kitazawa 2015 [87] | 60, 76 yr | 8-week, 1/week, 60-min | I: increased | No dropout |
| Konak 2016 [88] | 42, 68 yr | 4 weeks, 3/week, 45-min, I | NI | Dropout rates: <11% |
| Mundada 2022 [89] | 40, 64 yr | 6-weeks, 3/week, 45-min | NI | No dropout |
| Nieto-Guisado 2024 [90] | 20, 73 yr | 30-min | 5 min WU, 20 min C, 5 min CD. Mobility, dance | NI |
| Nishiguchi 2015 [41] | 48 | 12-weeks, 1/week, 90-min, G | 15 min S, moderate-intensity, 15 min strength, 60 min DT. I: increased. ACSM [91] | Training adherence: >91% |
| Norouzi 2019 [92] | 60, 68 yr | 60–80-min | Resistance training | No dropout |
| Pantoja-Cardoso 2023 [93] | 62, 67 yr | 16-weeks, 3/week | WU (joint mobility, basic movements), C, CD (breathing, S). I: adapted based on RPE | Dropout rates: <12% |
| Párraga-Montilla 2021 [94] | 43, 81 yr | 8-weeks, 5/week, 60-min | 10 min WU, 40 min C, 10 min CD. I: increased | No dropout |
| Rajalaxmi 2022 [37] | 50, 65–85 yr | 12-weeks, 5/week | NI | NI |
| Rezola-Pardo 2019 [38] | 85, 85 yr | 12-weeks, 2/week, 60-min | I: moderate, adapted. Protocol [95,96] | Dropout rates: <17% |
| Rezola-Pardo 2022 [39] | 85, 85 yr | 12-weeks, 2/week, I | 5 min WU, 5 min breath-relax. I: individualized. Protocol [38] | Dropout rates: <17% |
| Rosado 2021 [97] | 51, 75 yr | 24-weeks, 3/week, 75-min | 10 min WU, 50 min C, 5 min CD (S or breath), 5 min begin-finish ritual. I: moderate intensity (~13 point, RPE) | Dropout rates: <14%; Training adherence: >82% |
| Santos 2023 [98] | 36, 83 yr | 12-weeks, 2/week, 50-min | 6 WU. Protocol [99] | Dropout rates: <25% |
| Sedaghati 2022 [100] | 28, 70 yr | 8-weeks, 3/week, 60-min | Protocol [95,96,101,102,103] | No dropout |
| Sok 2021 [104] | 65, 74 yr | 10-weeks, 2/week, 50-min, G | 5 min WU, 60 min C, 5 min CD, 10 min communication time. I: adapted-increased. Protocol [105] | NI |
| Tait 2025 [106] | 96, 77 yr | 24-weeks, 2/week, 45–60-min, G | WU, 2–3 C, CD. I: moderate-hard on RPE. Progressive | Training adherence: >58% |
| Trombini-Souza 2023 [42] | 60 | 24-weeks, 2/week, 60-min G | 10 min WU (walk, S, joint mobilization), 40 C; 10 min relax (breathing, S. Protocol) [107] | Dropout rates: <50% |
| Wollesen 2017 [62] | 95, 71 yr | 12-weeks, 1/week, 60-min, G | NI | Dropout rates: <11% |
| Wollesen 2017 [56] | 90, 72 yr | NI | I: increased. Protocol [63] | Dropout rates: <4% |
| Yokoyama 2015 [108] | 27, 74 yr | 12-weeks, 3/week, 60-min | 15 min of mental gymnastics (finger motions), 35 C, 10 min of flexibility exercise. I: increased | Dropout rates: <7%; Training adherence: >90% |
| Yuzlu 2022 [40] | 58, 85 yr | 8-weeks, 2/week, I | 10 min WU, 40 min C, 10 min CD | Dropout rates: <14% |
| Protocol Duration (Weeks) | No. of Studies | Session a Week (n) | No. of Studies | Duration (Minutes) | No. of Studies | Intensity | No. of Studies |
|---|---|---|---|---|---|---|---|
| 12 | 16 | 2 | 18 | 60 | 12 | Progressive | 15 |
| 8 | 7 | 3 | 12 | 45 | 6 | Adapted | 4 |
| 24 | 3 | 1 | 4 | 50 | 3 | PA | 4 |
| 16 | 3 | 5 | 2 | 30 | 2 | ||
| 6 | 3 | 7 | 1 | 40 | 2 | ||
| 4 | 2 | 2–3 | 1 | 75 | 2 | ||
| 10 | 1 | 90 | 2 | ||||
| 26 | 1 | 120 | 1 |
| Aspects Evaluated | No. | Aspects Evaluated | No. | Aspects Evaluated | No. | Aspects Evaluated | No. |
|---|---|---|---|---|---|---|---|
| Cognitive function | 20 | Quality of life | 2 | Psycho-affective status | 1 | oxidative stress | 1 |
| Postural balance | 15 | Functional ability | 1 | Depression | 1 | Inflammation | 1 |
| Walking or gait analysis | 11 | Brain activation efficiency | 1 | Life satisfaction | 1 | Vascular health | 1 |
| Physical fitness | 10 | Executive functions | 1 | Frailty | 1 | Brain-derived neurotrophic factor | 1 |
| Falls and risk of falls | 6 | Dual-task interference | 1 | Activity of Daily Living | 1 | Circulating neurological | 1 |
| Muscle strength | 3 | Dual-tasking | 1 | Psychosocial wellbeing | 1 | Inflammatory markers | 1 |
| Cognition | 3 | Health status | 1 | Renal function | 1 | Plasma amyloid β peptide | 1 |
| Mobility | 2 | Cognitive health | 1 | Lipid profile | 1 | Adherence to programs | 1 |
| 1st Author and Year | Primary Task | Secondary Task | Primary Variables Evaluated | Primary Effect |
|---|---|---|---|---|
| Akin 2021 [44] | MT, D | Mental tracking, MT | PB, fear of fall, walk, strength | ++ |
| Amini 2022 [45] | MT, D | Working memory, reaction, discrimination-decision making, mental tracking, verbal fluency [46] | Cognitive health components | ++ |
| Anandh 2018 [43] | MT, walk | Verbal fluency, reaction, other (talking) | PB, gait | ++ |
| Ansai 2017 [47] | MT, RT, PB | Mental tracking, verbal fluency, other | CF, PF | ND |
| Machado Araújo 2025 [34] | MT, RT | Verbal fluency [50,51] | PF, CF, lipid profile, renal function, oxidative stress, inflammation | ++ |
| Arcila Castaño 2022 [51] | MT, RT | Verbal fluency | Body composition, PF, CF, plasma brain-derived neurotrophic factor | ++ |
| Bagheri 2021 [52] | MT, S-D PB | Verbal fluency, mental tracking | dual-task interference | ++ |
| Bischoff 2021 [53] | D PB, AT, RT | Verbal fluency, working memory, discrimination-decision making, mental tracking; MT | PF, psychosocial well-being | ++ |
| Blasco-Lafarga 2020 [65] | DLA | Protocol (Spanish) [66] | PF, CF | ++ |
| Chen 2023 [67] | AT | Working memory, discrimination-decision making, reaction, verbal fluency, mental tracking [109]; MT | CF, functional fitness | ++ |
| Chuang 2024 [35] | Stretching, RT, AT, PB | Sequential and simultaneous cognitive and physical training. Working memory, mental tracking, verbal fluency, other | Instrumental activities of daily living | ++ |
| Conradsson 2019 [69] | S-D PB | Mental tracking, working memory; MT | Gait, PB | ++ |
| De Maio Nascimento 2023 [71] | Gait, PB [72] | Mental tracking, verbal fluency, working memory, other | PB, gait, lower limb strength, CF | ++ |
| Falbo 2016 [73] | DLA, mobility | Discrimination-decision making, working memory [110] | Executive CF, gait | ++ |
| Granacher 2021 [75] | PB | Other (tooth brushing) | PB, strength | ND |
| Gregory 2016 [77] | Stepping [111] | Verbal fluency, mental tracking | Gait, vascular health | ++ |
| Halvarsson 2015 [79] | S-D PB | Cognitive, MT [70] | Fall-related self-efficacy, fear of falling, gait, PB, PF | ++ |
| Halvarsson 2016 [80] | S-D PB | Cognitive, MT [70] | Fall | ++ |
| Ho 2023 [81] | Protocol [82] | No details | functional ability | ++ |
| Horata 2021 [83] | Gait, PB | Working memory [84] | Gait, cognition | ++ |
| Jabeen 2024 [36] | MT | Verbal fluency, working memory, mental tracking | PB, quality of life | ++ |
| Jardim 2021 [85] | AT, RT, PB, coordination | MT; verbal fluency, working memory, mental tracking, discrimination-decision-making, other [112] | CF, PF | ++ |
| Kim 2019 [86] | MT (walk) | MT [113,114] | CF, gait | ++ |
| Kitazawa 2015 [87] | Stepping | Other (rhythmic tasks) | CF, gait, adherence to programs | ++ |
| Konak 2016 [88] | PB | Mental tracking, verbal fluency | PB, activity-specific PB confidence | ++ |
| Mundada 2022 [89] | S-D MT | Verbal fluency, mental tracking | CF | ++ |
| Nieto-Guisado 2024 [90] | PB | Other | PB, knee proprioception | ND |
| Nishiguchi 2015 [41] | Stepping | Verbal fluency, decision making, reaction [115,116] | CF, brain activation efficiency | ++ |
| Norouzi 2019 [92] | RT | MT; working memory, mental tracking [117,118] | CF, PB | ++ |
| Pantoja-Cardoso 2023 [93] | S-D PB, coordination, mobility, MT | Working memory, mental tracking, reaction | CF | + |
| Párraga-Montilla 2021 [94] | MT | Mental tracking, working memory, verbal fluency | CF, PF | ++ |
| Rajalaxmi 2022 [37] | S-D PB | Reaction, working memory; MT [119,120] | PB, CF | ++ |
| Rezola-Pardo 2019 [38] | RT, PB | Working memory, discrimination-decision making [103] | DT, PF, CF, psycho-affective status, quality of life, frailty | ND |
| Rezola-Pardo 2022 [39] | RT, S-D PB | Protocol [103] | Number of falls, number of fallers, parameters associated with fall risk | - |
| Rosado 2021 [97] | Agility, body awareness, mobility, RT | Working memory, discrimination-decision making | CF, mobility, DT | ++ |
| Santos 2023 [98] | Protocol [99] | Verbal fluency, working memory, mental tracking | Risk of falling | ++ |
| Sedaghati 2022 [100] | RT, PB [95,96,101,102,103] | Working memory, verbal fluency, mental tracking | PB | ++ |
| Sok 2021 [104] | Stepping [105] | Other (songs and rhythms) | CF, health status, depression, life satisfaction | ++ |
| Tait 2025 [106] | PB/mobility, RT | Mental tracking, working memory; MT | Cognition, circulating neurological, inflammatory markers | + |
| Trombini-Souza 2023 [42] | Walk, PB | Mental tracking, working memory, verbal fluency [107] | Mobility, CF, PB | ++ |
| Wollesen 2017 [62] | DLA, walk [22] | Reaction; MT | Walk | ++ |
| Wollesen 2017 [56] | DLA, walk [63] | Working memory | Gait | ++ |
| Yokoyama 2015 [108] | RT, AT | Mental tracking, other (Shiritori) | Executive functions, plasma amyloid β peptide (Aβ) 42/40 ratio | ++ |
| Yuzlu 2022 [40] | Motor skills, PB | Working memory, mental tracking, reaction [6,121] | PB, fear of falling, gait | ND |
| Motor Tasks | No. of Studies | Cognitive Tasks | No. of Studies |
|---|---|---|---|
| Postural balance | 21 | Mental tracking | 23 |
| Resistance training exercises | 13 | Working memory tasks | 22 |
| Gait and walking exercises | 6 | Verbal fluency tasks | 20 |
| Aerobic training | 6 | Motor task | 12 |
| Stepping | 4 | Reaction time tasks | 8 |
| Mobility exercise | 4 | Discrimination-decision making | 7 |
| Daily life activities | 4 | ||
| Coordination exercises | 2 | ||
| stretching | 1 | ||
| Agility/body awareness | 1 | ||
| motor skills | 1 |
| Frequency: | 2 sessions a week for 12-weeks | |
| Intensity: | Progressive-adapted (rate of perceived effort) | |
| Time: | 60 min | |
| Type: Dual task | ||
| Primary task | Postural balance | Static and dynamic exercises |
| Resistance training | Machine-based and power training | |
| Aerobic training | High-intensity interval or continuous moderate-intensity | |
| Mobility | Static training | |
| Daily life activities | ||
| Secondary task | Mental tracking | Counting backward, math calculations, solving anagrams |
| Working memory (long- and short-term) | Remembering words, items, shapes, colors, or numbers, complementing proverbs or traditional songs | |
| Verbal fluency | Reading and talking, reverse spelling, and singing songs | |
| Motor | Holding glasses, carrying and/or manipulating objects, tapping, throwing or holding objects, balancing a cup on the palm | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrigna, L.; Amato, A.; Castorina, A.; Musumeci, G. A Standard Operating Procedure for Dual-Task Training to Improve Physical and Cognitive Function in Older Adults: A Scoping Review. Brain Sci. 2025, 15, 785. https://doi.org/10.3390/brainsci15080785
Petrigna L, Amato A, Castorina A, Musumeci G. A Standard Operating Procedure for Dual-Task Training to Improve Physical and Cognitive Function in Older Adults: A Scoping Review. Brain Sciences. 2025; 15(8):785. https://doi.org/10.3390/brainsci15080785
Chicago/Turabian StylePetrigna, Luca, Alessandra Amato, Alessandro Castorina, and Giuseppe Musumeci. 2025. "A Standard Operating Procedure for Dual-Task Training to Improve Physical and Cognitive Function in Older Adults: A Scoping Review" Brain Sciences 15, no. 8: 785. https://doi.org/10.3390/brainsci15080785
APA StylePetrigna, L., Amato, A., Castorina, A., & Musumeci, G. (2025). A Standard Operating Procedure for Dual-Task Training to Improve Physical and Cognitive Function in Older Adults: A Scoping Review. Brain Sciences, 15(8), 785. https://doi.org/10.3390/brainsci15080785