
Advances in Non-Invasive Neuromodulation Techniques for Improving Cognitive Function: A Review

Abstract
1. Introduction
2. Application of tDCS in the Cognitive Domain
3. Application of tACS in the Cognitive Domain
4. Application of TMS in the Cognitive Domain
5. Application of TAS in the Cognitive Domain
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sandberg, A.; Bostrom, N. Converging cognitive enhancements. Ann. N. Y. Acad. Sci. 2006, 1093, 201–227. [Google Scholar] [CrossRef] [PubMed]
- Wojtalik, J.A.; Brown, W.J.; Mesholam-Gately, R.I.; Kotwani, A.; Keshavan, M.S.; Eack, S.M. Predictors of treatment discontinuation during an 18-month multi-site randomized trial of Cognitive Enhancement Therapy for early course schizophrenia. Psychiatry Res. 2023, 326, 115254. [Google Scholar] [CrossRef] [PubMed]
- Caruso, G.; Torrisi, S.A.; Mogavero, M.P.; Currenti, W.; Castellano, S.; Godos, J.; Ferri, R.; Galvano, F.; Leggio, G.M.; Grosso, G.; et al. Polyphenols and neuroprotection: Therapeutic implications for cognitive decline. Pharmacol. Ther. 2021, 232, 108013. [Google Scholar] [CrossRef] [PubMed]
- Snowball, A.; Tachtsidis, I.; Popescu, T.; Thompson, J.; Delazer, M.; Zamarian, L.; Zhu, T.; Kadosh, R.C. Long-Term Enhancement of Brain Function and Cognition Using Cognitive Training and Brain Stimulation. Curr. Biol. 2013, 23, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Szymoniuk, M.; Chin, J.-H.; Domagalski, Ł.; Biszewski, M.; Jóźwik, K.; Kamieniak, P. Brain stimulation for chronic pain management: A narrative review of analgesic mechanisms and clinical evidence. Neurosurg. Rev. 2023, 46, 127. [Google Scholar] [CrossRef] [PubMed]
- Park, K.S.; Choi, S.H.; Yoon, H. Modulation of sleep using noninvasive stimulations during sleep. Biomed. Eng. Lett. 2023, 13, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; Pascual-Leone, A. Technology Insight: Noninvasive brain stimulation in neurology—Perspectives on the therapeutic potential of rTMS and tDCS. Nat. Clin. Pract. Neurol. 2007, 3, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Kanai, R.; Chaieb, L.; Antal, A.; Walsh, V.; Paulus, W. Frequency-Dependent Electrical Stimulation of the Visual Cortex. Curr. Biol. 2008, 18, 1839–1843. [Google Scholar] [CrossRef] [PubMed]
- George, M.S.; Aston-Jones, G. Noninvasive techniques for probing neurocircuitry and treating illness: Vagus nerve stimulation (VNS), transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS). Neuropsychopharmacology 2010, 35, 301–316. [Google Scholar] [CrossRef]
- Feng, B.; Zhang, Y.; Luo, L.; Wu, J.; Yang, S.; Zhang, N.; Tan, Q.; Wang, H.; Ge, N.; Ning, F.; et al. Transcutaneous electrical acupoint stimulation for post-traumatic stress disorder: Assessor-blinded, randomized controlled study. Psychiatry Clin. Neurosci. 2018, 73, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Knotkova, H.; Nitsche, M.A.; Bikson, M.; Woods, A.J. Practical Guide to Transcranial Direct Current Stimulation Principles; Procedures and Applications: New York, NY, USA, 2019; pp. 133–156. [Google Scholar] [CrossRef]
- Wang, N.; Ming, D.; Ke, Y.; Du, J.; Liu, W.; Kong, L.; Zhao, X.; Liu, S.; Xu, M.; An, X. High-Definition Transcranial Direct Current Stimulation (HD-tDCS) enhances working memory training. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 329–332. [Google Scholar]
- McIntire, L.K.; McKinley, R.A.; Nelson, J.M.; Goodyear, C. Transcranial direct current stimulation versus caffeine as a fatigue countermeasure. Brain Stimul. 2017, 10, 1070–1078. [Google Scholar] [CrossRef]
- Fernández, A.; Cid-Fernández, S.; Díaz, F. Transcranial direct current stimulation (tDCS). An effective tool for improving episodic memory in young people? An. De Psicol. 2021, 37, 468–477. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, Q.; Zhao, J.; Leng, X.; Han, J.; Xia, F.; Pang, Y.; Chen, H. Anodal transcranial direct current stimulation (tDCS) over the left dorsolateral prefrontal cortex improves attentional control in chronically stressed adults. Front. Neurosci. 2023, 17, 1182728. [Google Scholar] [CrossRef] [PubMed]
- Krause, B.; Márquez-Ruiz, J.; Kadosh, R.C. The effect of transcranial direct current stimulation: A role for cortical excitation/inhibition balance? Front. Hum. Neurosci. 2013, 7, 602. [Google Scholar] [CrossRef] [PubMed]
- Weller, S.; Nitsche, M.A.; Plewnia, C. Enhancing cognitive control training with transcranial direct current stimulation: A systematic parameter study. Brain Stimul. 2020, 13, 1358–1369. [Google Scholar] [CrossRef] [PubMed]
- Friehs, M.A.; Frings, C. Cathodal tDCS increases stop-signal reaction time. Cogn. Affect. Behav. Neurosci. 2019, 19, 1129–1142. [Google Scholar] [CrossRef] [PubMed]
- Pope, P.A. Modulating Cognition Using Transcranial Direct Current Stimulation of the Cerebellum. J. Vis. Exp. 2015, 96, e52302. [Google Scholar] [CrossRef]
- Albizu, A.; Fang, R.; Indahlastari, A.; O’shea, A.; Stolte, S.E.; See, K.B.; Boutzoukas, E.M.; Kraft, J.N.; Nissim, N.R.; Woods, A.J. Machine learning and individual variability in electric field characteristics predict tDCS treatment response. Brain Stimul. 2020, 13, 1753–1764. [Google Scholar] [CrossRef]
- Albizu, A.; Indahlastari, A.; Huang, Z.; Waner, J.; Stolte, S.E.; Fang, R.; Woods, A.J. Machine-learning defined precision tDCS for improving cognitive function. Brain Stimul. 2023, 16, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Müller, D.; Habel, U.; Brodkin, E.S.; Weidler, C. High-definition transcranial direct current stimulation (HD-tDCS) for the enhancement of working memory–A systematic review and meta-analysis of healthy adults. Brain Stimul. 2022, 15, 1475–1485. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, H.; Jeong, H.; Roh, D.; Kim, D.H. TACS as a promising therapeutic option for improving cognitive function in mild cognitive impairment: A direct comparison between tACS and tDCS. J. Psychiatr. Res. 2021, 141, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Fayzullina, R.; Bullard, B.M.; Levina, V.; Reinhart, R.M.G. A meta-analysis suggests that tACS improves cognition in healthy, aging, and psychiatric populations. Sci. Transl. Med. 2023, 15, eabo2044. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Zhang, Z.; Yao, Z.; Ming, D.; Zhou, P. Modulation of Sustained Attention by Theta-tACS over the Lateral and Medial Frontal Cortices. Neural Plast. 2021, 2021, 5573471. [Google Scholar] [CrossRef] [PubMed]
- Varastegan, S.; Kazemi, R.; Rostami, R.; Khomami, S.; Zandbagleh, A.; Hadipour, A.L. Remember NIBS? tACS improves memory performance in elders with subjective memory complaints. GeroScience 2022, 45, 851–869. [Google Scholar] [CrossRef] [PubMed]
- Krebs, C.; Peter, J.; Wyss, P.; Brem, A.-K.; Klöppel, S. Transcranial electrical stimulation improves cognitive training effects in healthy elderly adults with low cognitive performance. Clin. Neurophysiol. 2021, 132, 1254–1263. [Google Scholar] [CrossRef] [PubMed]
- Fusco, G.; Fusaro, M.; Aglioti, S.M. Midfrontal-occipital θ-tACS modulates cognitive conflicts related to bodily stimuli. Soc. Cogn. Affect. Neurosci. 2020, 17, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Kasten, F.H.; Herrmann, C.S. Transcranial Alternating Current Stimulation (tACS) Enhances Mental Rotation Performance during and after Stimulation. Front. Hum. Neurosci. 2017, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Kasten, F.H.; Maess, B.; Herrmann, C.S. Facilitated Event-Related Power Modulations during Transcranial Alternating Current Stimulation (tACS) Revealed by Concurrent tACS-MEG. eNeuro 2018, 5, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Wischnewski, M.; Joergensen, M.L.; Compen, B.; Schutter, D.J.L.G. Frontal Beta Transcranial Alternating Current Stimulation Improves Reversal Learning. Cereb. Cortex 2020, 30, 3286–3295. [Google Scholar] [CrossRef] [PubMed]
- Spooner, R.K.; Wilson, T.W. Spectral specificity of gamma-frequency transcranial alternating current stimulation over motor cortex during sequential movements. Cereb. Cortex 2022, 33, 5347–5360. [Google Scholar] [CrossRef] [PubMed]
- Nissim, N.R.; McAfee, D.C.; Edwards, S.; Prato, A.; Lin, J.X.; Lu, Z.; Coslett, H.B.; Hamilton, R.H. Efficacy of Transcranial Alternating Current Stimulation in the Enhancement of Working Memory Performance in Healthy Adults: A Systematic Meta-Analysis. Neuromodulation Technol. Neural Interface 2023, 26, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Nardone, R.; Sebastianelli, L.; Versace, V.; Ferrazzoli, D.; Saltuari, L.; Trinka, E. TMS–EEG Co-Registration in Patients with Mild Cognitive Impairment, Alzheimer’s Disease and Other Dementias: A Systematic Review. Brain Sci. 2021, 11, 303. [Google Scholar] [CrossRef] [PubMed]
- Kozel, F.A.; Motes, M.A.; Didehbani, N.; DeLaRosa, B.; Bass, C.; Schraufnagel, C.D.; Jones, P.; Morgan, C.R.; Spence, J.S.; Kraut, M.A.; et al. Repetitive TMS to augment cognitive processing therapy in combat veterans of recent conflicts with PTSD: A randomized clinical trial. J. Affect. Disord. 2018, 229, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, C.; Ciricugno, A.; Urgesi, C.; Cattaneo, Z. Cerebellar contribution to emotional body language perception: A TMS study. Soc. Cogn. Affect. Neurosci. 2019, 17, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Abrahamyan, A.; Clifford, C.W.; Arabzadeh, E.; Harris, J.A. Low Intensity TMS Enhances Perception of Visual Stimuli. Brain Stimul. 2015, 8, 1175–1182. [Google Scholar] [CrossRef]
- Bashir, S.; Al-Hussain, F.; Hamza, A.; Shareefi, G.F.; Abualait, T.; Yoo, W.-K. Role of Single Low Pulse Intensity of Transcranial Magnetic Stimulation over the Frontal Cortex for Cognitive Function. Front. Hum. Neurosci. 2020, 14, 205. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Li, Y.; Cao, D.; Qian, Z.; Tang, Y.; Wang, J. TMS-EEG signatures of facilitated cognitive reappraisal in emotion regulation by left ventrolateral prefrontal cortex stimulation. Neuropsychologia 2023, 184, 108560. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Sanz, S.; Ghotme, K.A.; Hedmont, D.; Arévalo-Jaimes, M.Y.; Kadosh, R.C.; Serra-Grabulosa, J.M.; Redolar-Ripoll, D. Use of transcranial magnetic stimulation for studying the neural basis of numerical cognition: A systematic review. J. Neurosci. Methods 2022, 369, 109485. [Google Scholar] [CrossRef] [PubMed]
- Parkin, B.L.; Ekhtiari, H.; Walsh, V.F. Non-invasive Human Brain Stimulation in Cognitive Neuroscience: A Primer. Neuron 2015, 87, 932–945. [Google Scholar] [CrossRef] [PubMed]
- Anaesthesia Professional Committee of Chinese Association of Integrative Medicine, Gansu Society of Integrative Medicine. Clinical practice guideline for acupoint stimulation-assisted treatment of postoperative pain. Chin. J. Anaesthesiol. 2021, 41, 1159–1165. [Google Scholar] [CrossRef]
- Vickers, A.J.; Vertosick, E.A.; Lewith, G.; MacPherson, H.; Foster, N.E.; Sherman, K.J.; Irnich, D.; Witt, C.M.; Linde, K. Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis. J. Pain 2017, 19, 455–474. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.-Q.; Lu, W.-J.; Tan, W.-Q.; Liu, X.; Wang, Y.-T.; Wang, N.-B.; Zhuang, L.-X. Effectiveness of Acupuncture for Anxiety Among Patients with Parkinson Disease a Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2232133. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.; Cao, Y.; Chang, S.; Huang, Q.; Zhang, Z.; Wei, W.; Yao, J.; Pei, H.; Li, H. A network meta-analysis on the improvement of cognition in patients with vascular dementia by different acupuncture therapies. Front. Neurosci. 2022, 16, 1053283. [Google Scholar] [CrossRef] [PubMed]
- Yan, F.; Song, D.; Dong, Z.; Zhang, Y.; Wang, H.; Huang, L.; Wang, Y.; Wang, Q. Alternation of EEG Characteristics during Transcutaneous Acupoint Electrical Stimulation–Induced Sedation. Clin. EEG Neurosci. 2020, 53, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Chen, Y.M.; Yu, P.; Luo, F.M.; Gao, Y.; Chen, J.; Wang, P.M.; Wang, Y.M.; Zhao, Y.M.; Lei, Y. Effect of magnetic stimulation of Shenmen point on cognitive function of chronic insomnia: A randomized controlled clinical trial. Medicine 2020, 99, e23807. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-F.; Liang, W.-D.; Wang, B.-Y.; Guo, M.-L.; Zhou, J.-S.; Chen, L.; Zhong, M.-L.; Ye, J.-M. Transcutaneous electrical acupoint stimulation for reducing cognitive dysfunction in lumbar spine surgery: A randomized, controlled trail. Front. Aging Neurosci. 2022, 14, 1034998. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Yin, C.; Li, Y.; Gao, F.; Yu, L.; Wang, Z.; Wang, Q. Effects of Transcutaneous Electrical Acupoint Stimulation on Postoperative Cognitive Decline in Elderly Patients: A Pilot Study. Clin. Interv. Aging 2021, 16, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Yin, N.; Wang, A.; Xu, G. Cerebral cortex Functional Networks of Transdermal Electrical Stimulation at Daling (PC7) Acupoint. Clin. EEG Neurosci. 2022, 54, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Qiao, Y.; Wang, L.; Hao, P. Magnetic stimulation at acupoints relieves mental fatigue: An Event Related Potential (P300) study. Technol. Health Care 2017, 25, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Ren, M.; Xu, J.; Zhao, J.; Zhang, S.; Wang, W.; Xu, S.; Zhou, Z.; Chen, X.; Chen, S.; Li, Y.; et al. The Modulation of Working-Memory Performance Using Gamma-Electroacupuncture and Theta-Electroacupuncture in Healthy Adults. Evid. Based Complement. Altern. Med. 2021, 2021, 2062718. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Chen, D.; Zhang, X. A transcutaneous acupoint electrical simulation glove for relieving the mental fatigue of crane drivers in real building environment. Comput. Methods Biomech. Biomed. Eng. 2024, 1–14. [Google Scholar] [CrossRef]
- Chen, H.; Jann, K.; Li, Y.; Huang, J.; Chen, Y.; Kang, Y.; Gong, Z.; Huang, Y.; Wang, H.; Zhan, S.; et al. A true response of the brain network during electroacupuncture stimulation at scalp acupoints: An fMRI with simultaneous EAS study. Brain Behav. 2022, 13, e2829. [Google Scholar] [CrossRef] [PubMed]
- Yin, N.; Wang, A.-X.; Wang, H.-L. Electroencephalogram Analysis of Magnetic Stimulation at Different Acupoints. Front. Neurosci. 2022, 16, 848308. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Yu, H.; Ding, W.; Guo, L.; Xu, G.; Yin, N. Changes in Brain Functional Networks of Insomniacs Induced by Magnetic Stimulation at Acupoints. IEEE Trans. Appl. Supercond. 2018, 29, 0500104. [Google Scholar] [CrossRef]
- Dai, Y.-Y.; Yin, N.; Yu, H.; Xu, G.-Z. Cerebral cortex functional networks of magnetic stimulation at acupoints along the pericardium meridian. J. Integr. Neurosci. 2019, 18, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin. Neurophysiol. 2020, 132, 269–306. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Author (Year) | Stimulation Method/Study Design | Subjects | Target Brain Regions | Target Symptom/Measure | Results |
|---|---|---|---|---|---|
| Ningci et al. [13] (2019) | Anodal/sham stimulation 2 mA 20 min Single blind | n = 20 age: 18–25 | Anodal: F3 (Cathodal: FZ, FP1, FT7, C3) | 4-Back, 6-Back, adaptive N-Back | correct rate ↑ Maximum working memory capacity ↑ |
| McIntire et al. [14] (2017) | Anodal/coffee/sham stimulation 2 mA 30 min Single blind | n = 50 age: 22–32 | Left DLPFC (Right upper part of the biceps) | Fatigue, alertness/vigilance task, delayed match-sample working memory task, PVT | Alertness ↑ Mood ↑ |
| Fernández et al. [15] (2021) | Anodal/placebo control 2 mA 18 min Double-blind | n = 30 age: 18–28 | Left DLPFC (Fp2) | Episodic memory tasks, immediate/delayed recognition/recall tasks | Reaction time ↓ Episodic Memory ↑ |
| Liu et al. [16] (2023) | Anodal tDCS/sham stimulation 2 mA 20 min Double-blind | n = 40 age: 18–26 | Left DLPFC (F4) | Attention/Attention network test | Control of attention ↑ |
| Weller et al. [18] (2022) | Anodal/cathodal/sham stimulation 1 mA/2 mA 19 min Single blind | n = 162 age: 18–39 | Left DLPFC/Right DLPFC | Cognitive/PASAT rhythm auditory serial addition task, flanker task | Effect of cognitive training ↑ |
| Friehs et al. [19] (2019) | cathodal stimulation 0.5 mA 20 min | n = 45 age: 19–29 | Right DLPFC | Attention/stop signal task (SST) | Stop signal response time ↑ |
| Pope [20] (2015) | Cathodal/anodal/sham stimulation 2 mA 20 min Double-blind | Three independent groups of participants | Right cerebellum | Rhythmic auditory serial addition task, verb generation task | Cathodal stimulation enables attentional performance ↑ |
| Albizu et al. [21] (2020) | cathodal stimulation 2 mA 20 min Three blind | n = 14 age: 66–81 | Right DLPFC (F3) | Working memory/N-back working memory task | Working memory ↑ |
| Author (Year) | Stimulation Method/Study Design | Subjects | Target Brain Regions | Evaluation Method | Results |
|---|---|---|---|---|---|
| Kim et al. [24] (2021) | tACS: 40 Hz 2 mA 30 min tDCS: 2 mA 30 min double-blind | n = 20 age: 71–81 | DLPFC | Cognitive test | Cognitive test scores ↑ tACS > tDCS |
| Jinwen et al. [26] (2021) | tACS/sham stimulus 6 Hz 1.5 mA 15 min Single blind | n = 12 age: 20–26 | DLPFC | PVT | Reaction time ↓ Sustained Attention ↑ |
| Varastegan et al. [27] (2023) | Active θ-tACS/sham stimulation 6 Hz 2 mA 20 min double-blind | n = 16 age: 56–66 | Medial prefrontal cortex | RAVLT | Episodic memory ↑ |
| Krebs et al. [28] (2021) | tACS: 5 Hz 2 mA 20 min tDCS: 2 mA 20 min double-blind | n = 59 age: 61–85 | DLPFC | Cognitive assessment continuous pattern recognition | Cognitive comprehensive score ↑, effectiveness ↑ |
| Fusco et al. [29] (2022) | sham/θ-tACS/γ-tACS stimulus 6 Hz/40 Hz 12 min | n = 32 age: 22–27 | Medial frontal cortex | Erickson Flanker Task | θ-tACS Reaction time ↑ |
| Kasten & Herrmann [30] (2017) | α-tACS/sham stimulus IAF (8–12 Hz) 20 min | n = 23 age: 20–27 | Cz/Oz | Mental rotation judgment task | Reaction time ↓ Mental rotation performance ↑ |
| Kasten et al. [31] (2018) | tACS/sham IAF(α) 20 min | n = 20 age: 23–29 | Oz/Cz | Mental rotation Task | Performance ↑ |
| Wischnewski et al. [32] (2020) | tACS/sham 20 Hz 15 min Single blind | n = 108 age: 18–34 | DLPFC | Reversal Learning Task | Reversal learning ability ↑ Reaction time ↓ |
| Spooner et al. [33] (2023) | high/low β-tACS:peak of β frequencies ± 10 Hz 2 mA 20 min double-blind | n = 25 age: 21–32 | Left primary motor cortex | Finger Tapping Paradigm | Motor learning function ↑ |
| Author (Year) | Stimulus Intensity | Subjects | Target Brain Regions | Evaluation Method | Results |
|---|---|---|---|---|---|
| Kozel et al. [36] (2018) | Repetitive TMS 110% MT | n = 151 age: 20–50 | Right DLPFC | Cognitive processing therapy | Cognitive ↑ |
| Ferrari et al. [37] (2022) | Three pulses TMS 100% rMT | n = 20 age: 21–25 | Parietal lobe Left cerebellum Early visual cortex | Emotional body posture evaluation task | Cognition ↑ Emotion ↑ |
| Abrahamyan et al. [38] (2015) | Monopulse TMS 60%/70%/80%/90%/100% rMT | n = 11 age: 24–44 | Occipital lobe | Visual Identification Task | Identification of visual stimuli ↑ |
| Bashir et al. [39] (2020) | Monopulse TMS 50%/60%rMT | n = 42 age: 24–27 | Right DLPFC | Stop Signal Test | Level of cognitive function ↑ |
| Li et al. [40] (2023) | Monopulse TMS 90% rMT | n = 15 age: 20–28 | Left VLPFC parietal lobe | Emotion cognitive reappraisal task | Cognitive ↑ Attention ↑ |
| Author (Year) | Mode of Stimulation | Subjects | Site of Stimulation | Evaluation Method | Results |
|---|---|---|---|---|---|
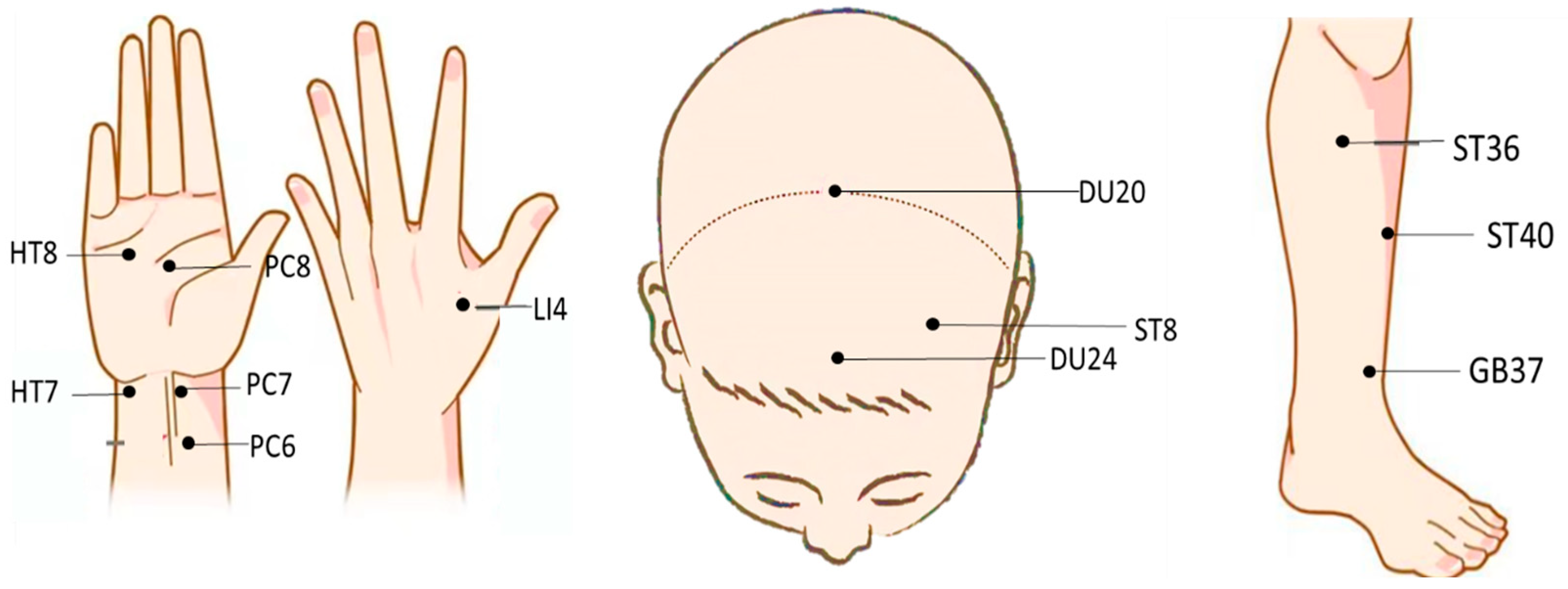
| Liu et al. [50] (2021) | Communication 2–100 Hz Maximum tolerated current | n = 100 age: 65–76 | PC6, LI4, ST36 | MMSE | Postoperative Cognitive function ↑ |
| Wang et al. [54] (2023) | Communication 4~6 mA 1 Hz | n = 10 age: 23–27 | PC8, PC6, LI4 | Simulated driving platform Cognitive task | Vigilance ↑ |
| Chen et al. [55] (2022) | Direct current 1–2 mA | n = 60 age: 20–40 | DU24, ST8 | Visual analogue scale | Functions of left and right executive control networks, sensorimotor networks, and attentional networks ↑ |
| Ren et al. [53] (2021) | Communication 6 Hz 40 Hz | n = 30 age: 18–24 | DU20, DU24 | n-Back | Accuracy ↑ Working Memory ↑ |
| Wang et al. [51] (2023) | Magnetic 1.76 T 1 Hz | n = 21 age: 21–25 | PC7 | Brain functional network analysis | Cognition, spirit, emotion ↑ |
| Yang et al. [52] (2017) | Magnetic 1.76 T 1 Hz | n = 14 age: 20–23 | HT7, LI4, PC8 | Cognitive tasks | P300 ↑ Attention ↑ |
| Yi et al. [56] (2022) | Magnetic 1.76 T 0.5 Hz | n = 20 age: 21–25 | ST36, ST40, GB37 | Brain functional network analysis | There are significant differences in brain functional connectivity in the central region |
| Dai et al. [58] (2019) | Magnetic 1.76 T 1 Hz | n = 14 age: 21–15 | PC7, PC6 | Brain functional network analysis | Functional connectivity of nodes in brain regions related to higher cognitive functions such as emotion, memory, and language ↑ |
| Method of Stimulation | Effect of Stimulation | Cost of Equipment |
|---|---|---|
| tDCS | Memory, Alertness, Mood, Attention, and cognitive ability ↑ | Lower |
| tACS | Cognitive, Sustained Attention, Memory, Effectiveness, Motor learning function ↑ | tACS > tDCS |
| TMS | Emotion, Visual response, Level of cognitive function, Attention ↑ | Higher TMS > tACS > tDCS |
| TAS | Vigilance, Attentional, Working Memory, Cognition, Spirit, Attention ↑ | Depending on the stimulus pattern |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, R.; Huang, L.; Wang, R.; Fei, J.; Wang, H.; Wang, J. Advances in Non-Invasive Neuromodulation Techniques for Improving Cognitive Function: A Review. Brain Sci. 2024, 14, 354. https://doi.org/10.3390/brainsci14040354
Chen R, Huang L, Wang R, Fei J, Wang H, Wang J. Advances in Non-Invasive Neuromodulation Techniques for Improving Cognitive Function: A Review. Brain Sciences. 2024; 14(4):354. https://doi.org/10.3390/brainsci14040354
Chicago/Turabian StyleChen, Ruijuan, Lengjie Huang, Rui Wang, Jieying Fei, Huiquan Wang, and Jinhai Wang. 2024. "Advances in Non-Invasive Neuromodulation Techniques for Improving Cognitive Function: A Review" Brain Sciences 14, no. 4: 354. https://doi.org/10.3390/brainsci14040354
APA StyleChen, R., Huang, L., Wang, R., Fei, J., Wang, H., & Wang, J. (2024). Advances in Non-Invasive Neuromodulation Techniques for Improving Cognitive Function: A Review. Brain Sciences, 14(4), 354. https://doi.org/10.3390/brainsci14040354