
Sleep in Disorders of Consciousness: A Brief Overview on a Still under Investigated Issue
 , ,
, , 
Abstract
1. Introduction
2. General Characteristics of Sleep Pattern
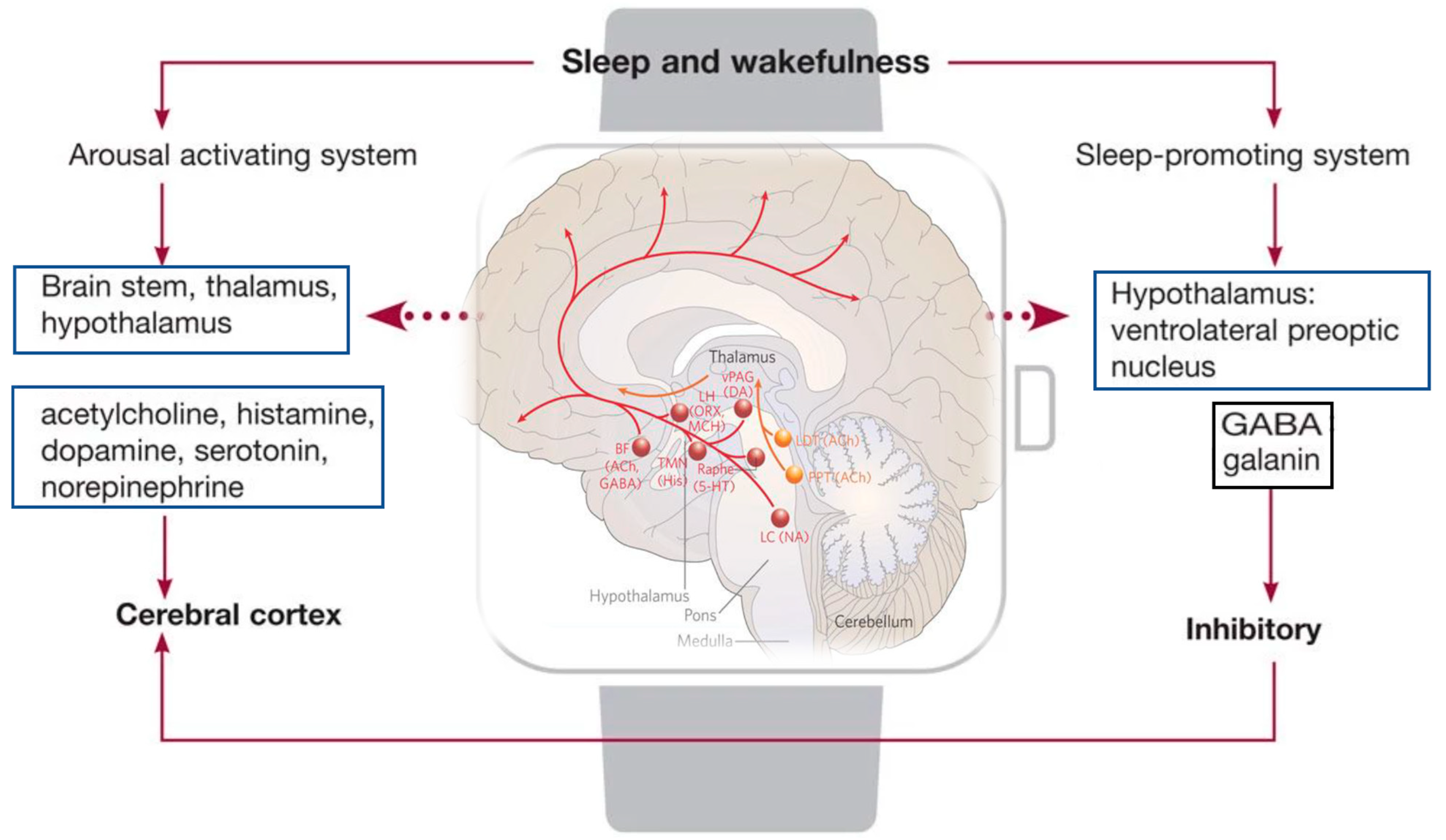
2.1. Anatomy and Physiology of the Sleep–Wake Cycle
2.2. Sleep
3. Characteristics and Assessment of Sleep in UWS/MCS
4. Treatment
Non-Pharmacological Treatment
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schiff, N.D. Central thalamic contributions to arousal regulation and neurological disorders of consciousness. Ann. N. Y. Acad. Sci. 2008, 1129, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, R.S.; Cacciola, A.; Bramanti, P.; Milardi, D. Neural correlates of consciousness: What we know and what we have to learn! Neurol. Sci. 2015, 36, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Laureys, S.; Boly, M.; Moonen, G.; Maquet, P. Two dimensions of consciousness: Arousal and awareness. Encycl. Neurosci. 2009, 2, 1133–1142. [Google Scholar]
- Vanhaudenhuyse, A.; Demertzi, A.; Schabus, M.; Noirhomme, Q.; Bredart, S.; Boly, M.; Phillips, C.; Soddu, A.; Luxen, A.; Moonen, G.; et al. Two distinct neuronal networks mediate the awareness of environment and of self. J. Cogn. Neurosci. 2011, 23, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Fins, J.J.; Laureys, S.; Schiff, N.D. Disorders of consciousness after acquired brain injury: The state of the science. Nat. Rev. Neurol. 2014, 10, 99–114. [Google Scholar] [CrossRef]
- Gosseries, O.; Zasler, N.D.; Laureys, S. Recent advances in disorders of consciousness: Focus on the diagnosis. Brain Inj. 2014, 28, 1141–1150. [Google Scholar] [CrossRef]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. European Task Force on Disorders of Consciousness. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef]
- Thibaut, A.; Bodien, Y.G.; Laureys, S.; Giacino, J.T. Minimally conscious state “plus”: Diagnostic criteria and relation to functional recovery. J. Neurol. 2020, 267, 1245–1254. [Google Scholar] [CrossRef]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef]
- Majerus, S.; Gill-Thwaites, H.; Andrews, K.; Laureys, S. Behavioral evaluation of consciousness in severe brain damage. Prog. Brain Res. 2005, 150, 397–413. [Google Scholar]
- Zhang, B.; Huang, K.; Karri, J.; O’Brien, K.; DiTommaso, C.; Li, S. Many Faces of the Hidden Souls: Medical and Neurological Complications and Comorbidities in Disorders of Consciousness. Brain Sci. 2021, 11, 608. [Google Scholar] [CrossRef] [PubMed]
- Ashwal, S.; Cranford, R.; Bernet, J.L. Multi-Society Task Force on PVS. Medical aspects of the persistent vegetative state. N. Engl. J. Med. 1994, 330, 1499–1508. [Google Scholar]
- Giacino, J.T.; Kalmar, K. Diagnostic and prognostic guidelines for the vegetative and minimally conscious states. Neuropsychol. Rehabil. 2005, 15, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Steppacher, I.; Kaps, M.; Kissler, J. Will time heal? A long-term follow-up of severe disorders of consciousness. Ann. Clin. Transl. Neurol. 2014, 1, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Arico, I.; Naro, A.; Pisani, L.R.; Leo, A.; Muscarà, N.; De Salvo, S.; Silvestri, R.; Bramanti, P.; Calabrò, R.C. Could combined sleep and pain evaluation be useful in the diagnosis of disorders of consciousness (DOC)? Preliminary findings. Brain Inj. 2016, 30, 159–163. [Google Scholar] [CrossRef]
- Kondziella, D.; Bender, A.; Diserens, K.; van Erp, W.; Estraneo, A.; Formisano, R.; Laureys, S.; Naccache, L.; Ozturk, S.; Rohaut, B.; et al. European Academy of Neurology guideline on the diagnosis of coma and other disorders of consciousness. Eur. J. Neurol. 2020, 27, 741–756. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Bramanti, P.; Naro, A. Towards new methods of diagnosis in disorders of consciousness. Lancet Neurol. 2016, 15, 1114–1115. [Google Scholar] [CrossRef]
- Pan, J.; Wu, J.; Liu, J.; Wu, J.; Wang, F. A Systematic Review of Sleep in Patients with Disorders of Consciousness: From Diagnosis to Prognosis. Brain Sci. 2021, 11, 1072. [Google Scholar] [CrossRef]
- de Biase, S.; Gigli, G.L.; Lorenzut, S.; Bianconi, C.; Sfreddo, P.; Rossato, G.; Basaldella, F.; Fuccaro, M.; Corica, A.; Tonon, D.; et al. The importance of polysomnography in the evaluation of prolonged disorders of consciousness: Sleep recordings more adequately correlate than stimulus-related evoked potentials with patients’ clinical status. Sleep Med. 2014, 15, 393–400. [Google Scholar] [CrossRef]
- Noormandi, A.; Shahrokhi, M.; Khalili, H. Potential benefits of zolpidem in disorders of consciousness. Expert Rev. Clin. Pharmacol. 2017, 10, 983–992. [Google Scholar] [CrossRef]
- Arnaldi, D.; Terzaghi, M.; Cremascoli, R.; De Carli, F.; Maggioni, G.; Pistarini, C.; Nobili, F.; Moglia, A.; Manni, R. The prognostic value of sleep patterns in disorders of consciousness in the sub-acute phase. Clin. Neurophysiol. 2015, 127, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Wislowska, M.; del Giudice, R.; Lechinger, J.; Wielek, T.; Heib, D.P.J.; Pitiot, A.; Pichler, G.; Michitsch, G.; Donis, J.; Schabus, M. Night and day variations of sleep in patients with disorders of consciousness. Sci. Rep. 2017, 7, 266. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Xia, X.; Li, X. A review of resting-state electroencephalography analysis in disorders of consciousness. Front. Neurol. 2017, 8, 471. [Google Scholar]
- Buzsáki, G.; Anastassiou, C.A.; Koch, C. The origin of extracellular fields and currents—EEG, ECoG, LFP and spikes. Nat. Rev. Neurosci. 2012, 13, 407–420. [Google Scholar] [CrossRef]
- Brenner, R.P. The Interpretation of the EEG in Stupor and Coma. Neurol. 2005, 11, 271–284. [Google Scholar] [CrossRef] [PubMed]
- De Salvo, S.; Caminiti, F.; Bonanno, L.; De Cola, M.C.; Corallo, F.; Caizzone, A.; Rifici, C.; Bramanti, P.; Marino, S. Neurophysiological assessment for evaluating residual cognition in vegetative and minimally conscious state patients: A pilot study. Funct. Neurol. 2015, 30, 237–244. [Google Scholar] [CrossRef]
- Pan, J.; Xie, Q.; Qin, P.; Chen, Y.; He, Y.; Huang, H.; Wang, F.; Ni, X.; Cichocki, A.; Yu, R.; et al. Prognosis for patients with cognitive motor dissociation identified by brain-computer interface. Brain 2020, 143, 1177–1189. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Xie, Q.; He, Y.; Wang, F.; Di, H.; Laureys, S.; Yu, R.; Li, Y. Detecting awareness in patients with disorders of consciousness using a hybrid brain–computer interface. J. Neural Eng. 2014, 11, 056007. [Google Scholar] [CrossRef]
- Cacciatore, M.; Magnani, F.G.; Leonardi, M.; Sebastiano, D.R.; Sattin, D. Sleep Treatments in Disorders of Consciousness: A Systematic Review. Diagnostics 2021, 12, 88. [Google Scholar] [CrossRef]
- Rundo, J.V.; Downey, R. Polysomnography. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; Volume 160, pp. 381–392. ISBN 978-0-444-64032-1. [Google Scholar]
- Rechtschaffen, A.; Kales, A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages in Human Subjects; National Institutes of Health Publications, US Government Printing Office: Washington, DC, USA, 1968.
- Iber, C.; Ancoli, I.-S.; Andrew, L.; Stuart, F. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Westchester, IL, USA, 2007. [Google Scholar]
- Fiorillo, L.; Fiorillo, L.; Puiatti, A.; Papandrea, M.; Ratti, P.-L.; Favaro, P.; Roth, C.; Bargiotas, P.; Bassetti, C.L.; Faraci, F.D. Automated sleep scoring: A review of the latest approaches. Sleep Med. Rev. 2019, 48, 101204. [Google Scholar]
- Mousavi, S.; Afghah, F.; Acharya, U.R. SleepEEGNet: Automated sleep stage scoring with sequence to sequence deep learning approach. PLoS ONE 2019, 14, e0216456. [Google Scholar] [CrossRef] [PubMed]
- Phan, H.; Andreotti, F.; Cooray, N.; Chéen, O.Y.; De Vos, M. SeqSleepNet: End-to-End Hierarchical Recurrent Neural Network for Sequence-to-Sequence Automatic Sleep Staging. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Zhang, J.; Wang, F.; Liu, W.; Huang, H.; Tang, W.; Liao, H.; Li, M.; Wu, J.; Li, X.; et al. Automatic Sleep Staging Based on EEG-EOG Signals for Depression Detection. Intell. Autom. Soft Comput. 2021, 28, 53–71. [Google Scholar] [CrossRef]
- Chen, T.; Huang, H.; Pan, J.; Li, Y. An EEG-based brain-computer interface for automatic sleep stage classification. In Proceedings of the 2018 13th IEEE Conference on Industrial Electronics and Applications (ICIEA), Wuhan, China, 31 May–2 June 2018; IEEE: New York, NY, USA; pp. 1988–1991. [Google Scholar]
- Roth, T. Characteristics and determinants of normal sleep. J. Clin. Psychiatry 2004, 65, 8–11. [Google Scholar]
- Izac, M.S.M. Basic Anatomy and Physiology of Sleep. Am. J. Electroneurodiagn. Technol. 2006, 46, 18–38. [Google Scholar] [CrossRef]
- Reichert, C.F.; Maire, M.; Schmidt, C.; Cajochen, C. Sleep-Wake Regulation and Its Impact on Working Memory Performance: The Role of Adenosine. Biology 2016, 5, 11. [Google Scholar] [CrossRef]
- Gerashchenko, D.; Murillo-Rodriguez, E.; Lin, L.; Xu, M.; Hallett, L.; Nishino, S.; Mignot, E.; Shiromani, P.J. Relationship between CSF hypocretin levels and hypocretin neuronal loss. Exp. Neurol. 2003, 184, 1010–1016. [Google Scholar] [CrossRef]
- Siegel, J.M. Hypocretin (orexin): Role in normal behavior and neuropathology. Annu. Rev. Psychol. 2004, 55, 125–148. [Google Scholar] [CrossRef]
- Brown, R.E.; Stevens, D.R.; Haas, H.L. The physiology of brain histamine. Prog. Neurobiol. 2001, 63, 637–672. [Google Scholar] [CrossRef]
- Watanabe, T.; Taguchi, Y.; Shiosaka, S.; Tanaka, J.; Kubota, H.; Terano, Y.; Tohyama, M.; Wada, H. Distribution of the his-taminergic neuron system in the central nervous system of rats: A fluorescent immunohistochemical analysis with histidine decarboxylase as a marker. Brain Res. 1984, 1, 13–25. [Google Scholar] [CrossRef]
- Ko, E.M.; Estabrooke, I.V.; McCarthy, M.; Scammell, T.E. Wake-related activity of tuberomammillary neurons in rats. Brain Res. 2003, 992, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Lin, J.-S.; Sakai, K. Neuronal Activity of Histaminergic Tuberomammillary Neurons during Wake-Sleep States in the Mouse. J. Neurosci. 2006, 26, 10292–10298. [Google Scholar] [CrossRef] [PubMed]
- McCarley, R.W. Sleep Neurophysiology: Basic Mechanisms Underlying Control of Wakefulness and Sleep. In Sleep Disorders Medicine. Basic Science, Technical Considerations, and Clinical Aspects; Chokroverty, B.H., Ed.; Elsevier: Amsterdam, The Netherlands, 1999; pp. 51–59. [Google Scholar]
- Jones, B.E. From waking to sleeping: Neuronal and chemical substrates. Trends Pharmacol. Sci. 2005, 26, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Lena, I.; Parrot, S.; Deschaux, O.; Muffat-Joly, S.; Sauvinet, V.; Renaud, B.; Suaud-Chagny, M.F.; Gottesmann, C. Variations in extracellular levels of dopamine, noradrenaline, glutamate, and aspartate across the sleep—wake cycle in the medial prefrontal cortex and nucleus accumbens of freely moving rats. J. Neurosci. Res. 2005, 81, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Aston-Jones, G.; Bloom, F.E. Activity of norepinephrine-containing locus coeruleus neurons in behaving rats anticipates fluctuations in the sleep-waking cycle. J. Neurosci. 1981, 1, 876–886. [Google Scholar] [CrossRef]
- Gervasoni, D.; Darracq, L.; Fort, P.; Soulière, F.; Chouvet, G.; Luppi, P.-H. Electrophysiological evidence that noradrenergic neurons of the rat locus coeruleus are tonically inhibited by GABA during sleep. Eur. J. Neurosci. 1998, 10, 964–970. [Google Scholar] [CrossRef] [PubMed]
- McCarley, R.W.; Hobson, J.A. Neuronal excitability modulation over the sleep cycle: A structural and mathematical model. Science 1975, 189, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Smith, Y.; Kieval, J.Z. Anatomy of the dopamine system in the basal ganglia. Trends Neurosci. 2000, 23, S28–S33. [Google Scholar] [CrossRef]
- Jacobs, B.L.; Fornal, C.A. Activity of brain serotonergic neurons in the behaving animal. Pharmacol. Rev. 1991, 43, 563–578. [Google Scholar]
- Wu, M.-F.; John, J.; Boehmer, L.N.; Yau, D.; Nguyen, G.B.; Siegel, J.M. Activity of dorsal raphe cells across the sleep-waking cycle and during cataplexy in narcoleptic dogs. J. Physiol. 2004, 554, 202–215. [Google Scholar] [CrossRef]
- Jones, B.E. Activity, modulation and role of basal forebrain cholinergic neurons innervating the cerebral cortex. Brain Res. 2004, 145, 157–169. [Google Scholar] [CrossRef]
- Mileykovskiy, B.Y.; Kiyashchenko, L.I.; Siegel, J.M. Behavioral Correlates of Activity in Identified Hypocretin/Orexin Neurons. Neuron 2005, 46, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Kiyashchenko, L.I.; Mileykovskiy, B.Y.; Maidment, N.; Lam, H.A.; Wu, M.-F.; John, J.; Peever, J.; Siegel, J.M. Release of Hypocretin (Orexin) during Waking and Sleep States. J. Neurosci. 2002, 22, 5282–5286. [Google Scholar] [CrossRef] [PubMed]
- Murillo-Rodríguez, E.; Arias-Carrión, O.; Sanguino-Rodríguez, K.; González-Arias, M.; Har, R. Mechanisms of Sleep-Wake Cycle Modulation. CNS Neurol. Disord. Drug Targets 2009, 8, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Dijk, D.-J.; Czeisler, C.A. Paradoxical timing of the circadian rhythm of sleep propensity serves to consolidate sleep and wakefulness in humans. Neurosci. Lett. 1994, 166, 63–68. [Google Scholar] [CrossRef]
- Dijk, D.J.; Cajochen, C. Melatonin and the circadian regulation of sleep initiation, consolidation, structure, and the sleep EEG. J. Biol. Rhythm. 1997, 6, 627–635. [Google Scholar] [CrossRef]
- Easton, A.; Meerlo, P.; Bergmann, B.; Turek, F.W. The Suprachiasmatic Nucleus Regulates Sleep Timing and Amount in Mice. Sleep 2004, 27, 1307–1318. [Google Scholar] [CrossRef]
- Sherin, J.E.; Shiromani, P.J.; McCarley, R.W.; Saper, C.B. Activation of Ventrolateral Preoptic Neurons during Sleep. Science 1996, 271, 216–219. [Google Scholar] [CrossRef]
- Szymusiak, R.; Alam, N.; Steininger, T.L.; McGinty, D. Sleep–waking discharge patterns of ventrolateral preoptic/anterior hypothalamic neurons in rats. Brain Res. 1998, 803, 178–188. [Google Scholar] [CrossRef]
- Lu, J.; Greco, M.A.; Shiromani, P.; Saper, C.B. Effect of Lesions of the Ventrolateral Preoptic Nucleus on NREM and REM Sleep. J. Neurosci. 2000, 20, 3830–3842. [Google Scholar] [CrossRef]
- Lu, J.; Bjorkum, A.A.; Xu, M.; Gaus, S.E.; Shiromani, P.J.; Saper, C.B. Selective Activation of the Extended Ventrolateral Preoptic Nucleus during Rapid Eye Movement Sleep. J. Neurosci. 2002, 22, 4568–4576. [Google Scholar] [CrossRef] [PubMed]
- Sterman, M.B.; Clemente, C.D. Forebrain inhibitory mechanisms:cortical synchronization induced by basal forebrain stimu-lation. Exp. Neurol. 1962, 6, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Sterman, M.B.; Clemente, C.D. Forebrain inhibitory mechanisms: Sleep patterns induced by basal forebrain stimulation in the behaving cat. Exp. Neurol. 1962, 6, 103–117. [Google Scholar] [CrossRef]
- Siegel, J.M. Brainstem Mechanisms Generating REM Sleep. In Principles and Practice of Sleep Medicine; Kryger, M.H., Roth, T., Dement, W.C., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2000; pp. 112–133. [Google Scholar]
- Hallanger, A.E.; Levey, A.I.; Lee, H.J.; Rye, D.B.; Wainer, B.H. The origins of cholinergic and other subcortical afferents to the thalamus in the rat. J. Comp. Neurol. 1987, 262, 105–124. [Google Scholar] [CrossRef] [PubMed]
- Kayama, Y.; Ohta, M.; Jodo, E. Firing of ‘possibly’ cholinergic neurons in the rat laterodorsal tegmental nucleus during sleep and wakefulness. Brain Res. 1992, 569, 210–220. [Google Scholar] [CrossRef]
- Bekinschtein, T.A.; Golombek, D.A.; Simonetta, S.H.; Coleman, M.R.; Manes, F.F. Circadian rhythms in the vegetative state. Brain Inj. 2009, 23, 915–919. [Google Scholar] [CrossRef]
- Blume, C.; Lechinger, J.; Santhi, N.; del Giudice, R.; Gnjezda, M.-T.; Pichler, G.; Scarpatetti, M.; Donis, J.; Michitsch, G.; Schabus, M. Significance of circadian rhythms in severely brain-injured patients: A clue to consciousness? Neurology 2017, 88, 1933–1941. [Google Scholar] [CrossRef]
- Cruse, D.; Thibaut, A.; Demertzi, A.; Nantes, J.C.; Bruno, M.-A.; Gosseries, O.; Vanhaudenhuyse, A.; Bekinschein, T.A.; Owen, A.M.; Laureys, S. Actigraphy assessments of circadian sleep-wake cycles in the vegetative and minimally conscious states. BMC Med. 2013, 11, 18. [Google Scholar] [CrossRef]
- Isono, M.; Wakabayashi, Y.; Fujiki, M.M.; Kamida, T.; Kobayashi, H. Sleep cycle in patients in a state of permanent unconsciousness. Brain Inj. 2002, 16, 705–712. [Google Scholar] [CrossRef]
- Mertel, I.; Pavlov, Y.G.; Barner, C.; Müller, F.; Diekelmann, S.; Kotchoubey, B. Sleep in disorders of consciousness: Behavioral and polysomnographic recording. BMC Med. 2020, 18, 350. [Google Scholar] [CrossRef]
- Mura, E.; Pistoia, F.; Sara, M.; Sacco, S.; Carolei, A.; Govoni, S. Pharmacological modulation of the state of awareness in patients with disorders of consciousness: An overview. Curr. Pharm. Des. 2014, 20, 4121–4139. [Google Scholar] [CrossRef]
- Yeo, B.T.T.; Tandi, J.; Chee, M.W.L. Functional connectivity during rested wakefulness predicts vulnerability to sleep deprivation. Neuroimage 2015, 111, 147–158. [Google Scholar] [CrossRef]
- Shao, Y.; Wang, L.; Ye, E.; Jin, X.; Ni, W.; Yang, Y.; Wen, B.; Hu, D.; Yang, Z. Decreased thalamocortical functional connectivity after 36 hours of total sleep deprivation: Evidence from resting state FMRI. PLoS ONE 2013, 8, e78830. [Google Scholar] [CrossRef]
- Miraglia, F.; Tomino, C.; Vecchio, F.; Gorgoni, M.; De Gennaro, L.; Rossini, P.M. The brain network organization during sleep onset after deprivation. Clin. Neurophysiol. 2021, 132, 36–44. [Google Scholar] [CrossRef]
- De Weer, A.-S.; Da Ros, M.; Berré, J.; Mélot, C.; Goldman, S.; Peigneux, P. Environmental influences on activity patterns in altered states of consciousness: Activity patterns in disorders of consciousness. Eur. J. Neurol. 2011, 18, 1432–1434. [Google Scholar] [CrossRef]
- Schabus, M.; Wislowska, M.; Angerer, M.; Blume, C. Sleep and circadian rhythms in severely brain-injured patients—A comment. Clin. Neurophysiol. 2018, 129, 1780–1784. [Google Scholar] [CrossRef]
- Blume, C.; Angerer, M.; Raml, M.; del Giudice, R.; Santhi, N.; Pichler, G.; Kunz, A.B.; Scarpatetti, E.; Trinka, E.; Schabus, M. Healthier rhythm, healthier brain? Integrity of circadian melatonin and temperature rhythms relates to the clinical state of brain-injured patients. Eur. J. Neurol. 2019, 26, 1051–1059. [Google Scholar] [CrossRef]
- Cologan, V.; Drouot, X.; Parapatics, S.; Delorme, A.; Gruber, G.; Moonen, G.; Laureys, S. Sleep in the unresponsive wake-fulness syndrome and minimally conscious state. J. Neurotrauma 2013, 30, 339–346. [Google Scholar] [CrossRef]
- Forgacs, P.B.; Conte, M.M.; Fridman, E.A.; Voss, H.U.; Victor, J.D.; Schiff, N.D. Preservation of electroencephalographic organization in patients with impaired consciousness and imaging-based evidence of command-following. Ann. Neurol. 2014, 76, 869–879. [Google Scholar] [CrossRef]
- Kotchoubey, B.; Pavlov, Y. Sleep patterns open the window into disorders of consciousness. Clin. Neurophysiol. 2018, 129, 668–669. [Google Scholar] [CrossRef]
- Sebastiano, D.R.; Visani, E.; Panzica, F.; Sattin, D.; Bersano, A.; Nigri, A.; Ferraro, S.; Parati, E.; Leonardi, M.; Franceschetti, S. Sleep patterns associated with the severity of impairment in a large cohort of patients with chronic disorders of consciousness. Clin. Neurophysiol. 2018, 129, 687–693. [Google Scholar] [CrossRef]
- Brown, R.; Basheer, R.; McKenna, J.; Strecker, R.E.; McCarley, R. Control of Sleep and Wakefulness. Physiol. Rev. 2012, 92, 1087–1187. [Google Scholar] [CrossRef]
- Landgraf, D.; Shostak, A.; Oster, H. Clock genes and sleep. Pflügers Arch. Eur. J. Physiol. 2012, 463, 3–14. [Google Scholar] [CrossRef]
- Sakurai, T. The neural circuit of orexin (hypocretin): Maintaining sleep and wakefulness. Nat. Rev. Neurosci. 2007, 8, 171–181. [Google Scholar] [CrossRef]
- Claustrat, B.; Brun, J.; Chazot, G. The basic physiology and pathophysiology of melatonin. Sleep Med. Rev. 2005, 9, 11–24. [Google Scholar] [CrossRef]
- Reiter, R.J. Pineal Melatonin: Cell Biology of Its Synthesis and of Its Physiological Interactions. Endocr. Rev. 1991, 12, 151–180. [Google Scholar] [CrossRef]
- Nambu, T.; Sakurai, T.; Mizukami, K.; Hosoya, Y.; Yanagisawa, M.; Goto, K. Distribution of orexin neurons in the adult rat brain. Brain Res. 1999, 827, 243–260. [Google Scholar] [CrossRef]
- Yang, X.-A.; Song, C.-G.; Yuan, F.; Zhao, J.-J.; Jiang, Y.-L.; Yang, F.; Kang, X.-G.; Jiang, W. Prognostic roles of sleep electroencephalography pattern and circadian rhythm biomarkers in the recovery of consciousness in patients with coma: A prospective cohort study. Sleep Med. 2020, 69, 204–212. [Google Scholar] [CrossRef]
- Lucca, L.F.; Lofaro, D.; Pignolo, L.; Leto, E.; Ursino, M.; Cortese, M.D.; Conforti, D.; Tonin, P.; Cerasa, A. Outcome prediction in disorders of consciousness: The role of coma recovery scale revised. BMC Neurol. 2019, 19, 68. [Google Scholar] [CrossRef]
- Gottshall, J.L.; Rossi Sebastiano, D. Sleep in disorders of consciousness: Diagnostic, prognostic, and therapeutic considerations. Curr. Opin. Neurol. 2020, 33, 684–690. [Google Scholar] [CrossRef]
- Nekrasova, J.; Kanarskii, M.; Yankevich, D.; Shpichko, A.; Borisov, I.; Pradhan, P.; Miroshnichenko, M. Retrospective analysis of sleep patterns in patients with chronic disorders of consciousness. Sleep Med. X 2020, 2, 100024. [Google Scholar] [CrossRef]
- Silverman, D. Retrospective study of EEG in coma. Electroencephalogr. Clin. Neurophysiol. 1963, 15, 486–503. [Google Scholar] [CrossRef]
- Kang, X.-G.; Yang, F.; Li, W.; Ma, C.; Li, L.; Jiang, W. Predictive value of EEG-awakening for behavioral awakening from coma. Ann. Intensive Care 2015, 5, 52. [Google Scholar] [CrossRef]
- Hulihan, J.F., Jr.; Syna, D.R. Electroencephalographic sleep patterns in post-anoxic stupor and coma. Neurology 1994, 44, 758–760. [Google Scholar] [CrossRef]
- Oksenberg, A.; Gordon, C.; Arons, E.; Sazbon, L. Phasic Activities of Rapid Eye Movement Sleep in Vegetative State Patients. Sleep 2001, 24, 703–706. [Google Scholar] [CrossRef]
- Scarpino, M.; Lolli, F.; Hakiki, B.; Lanzo, G.; Sterpu, R.; Atzori, T.; Portaccio, E.; Draghi, F.; Amantini, A.; Grippo, A. EEG and Coma Recovery Scale-Revised prediction of neurological outcome in Disorder of Consciousness patients. Acta Neurol. Scand. 2020, 142, 221–228. [Google Scholar] [CrossRef]
- Wielek, T.; Lechinger, J.; Wislowska, M.; Blume, C.; Ott, P.; Wegenkittl, S.; del Giudice, R.; Heib, D.P.J.; Mayer, H.A.; Laureys, S.; et al. Sleep in patients with disorders of consciousness characterized by means of machine learning. PLoS ONE 2018, 13, e0190458. [Google Scholar] [CrossRef]
- Locatelli, F.; Formica, F.; Galbiati, S.; Avantaggiato, P.; Beretta, E.; Carnovale, C.; Pozzi, M.; Clementi, E.; Strazzer, S. Poly-somnographic analysis of a pediatric case of baclofen-induced central sleep apnea. J. Clin. Sleep Med. 2019, 15, 351–354. [Google Scholar] [CrossRef]
- Silva, M.A.; Schwartz, D.J.; Nakase-Richardson, R. Functional improvement after severe brain injury with disorder of con-sciousness paralleling treatment for comorbid obstructive sleep apnoea: A case report. Int. J. Rehabil. Res. 2019, 42, 285–288. [Google Scholar] [CrossRef]
- Adams, Z.M.; Forgacs, P.B.; Conte, M.M.; Nauvel, T.J.; Drover, J.D.; Schiff, N.D. Late and progressive alterations of sleep dynamics following central thalamic deep brain stimulation (CT-DBS) in chronic minimally conscious state. Clin. Neurophysiol. 2016, 127, 3086–3092. [Google Scholar] [CrossRef]
- Formica, F.; Pozzi, M.; Avantaggiato, P.; Molteni, E.; Arrigoni, F.; Giordano, F.; Clementi, E.; Strazzer, S. Disordered con-sciousness or disordered wakefulness? The importance of prolonged polysomnography for the diagnosis, drug therapy, and rehabilitation of an unresponsive patient with brain injury. J. Clin. Sleep Med. 2017, 13, 1477–1481. [Google Scholar] [CrossRef]
- Gottshall, J.L.; Adams, Z.M.; Forgacs, P.B.; Schiff, N.D. Daytime Central Thalamic Deep Brain Stimulation Modulates Sleep Dynamics in the Severely Injured Brain: Mechanistic Insights and a Novel Framework for Alpha-Delta Sleep Generation. Front. Neurol. 2019, 10, 20. [Google Scholar] [CrossRef]
- Dhamapurkar, S.K.; Wilson, B.A.; Rose, A.; Watson, P.; Shiel, A. Does Modafinil improve the level of consciousness for people with a prolonged disorder of consciousness? A retrospective pilot study. Disabil. Rehabil. 2017, 39, 2633–2639. [Google Scholar] [CrossRef]
- Lees, J.; Michalopoulou, P.G.; Lewis, S.W.; Preston, S.; Bamford, C.; Collier, T.; Kalpakidou, A.; Wykes, T.; Emsley, R.; Pandina, G. Modafinil and cognitive enhancement in schizophrenia and healthy volunteers: The effects of test battery in a randomized controlled trial. Psychol. Med. 2017, 47, 2358–2368. [Google Scholar] [CrossRef]
- Rasmussen, N.-A.; Schrøder, P.; Olsen, L.R.; Brødsgaard, M.; Undén, M.; Bech, P. Modafinil augmentation in depressed patients with partial response to antidepressants: A pilot study on self-reported symptoms covered by the Major Depression Inventory (MDI) and the Symptom Checklist (SCL-92). Nord. J. Psychiatr. 2005, 59, 173–178. [Google Scholar] [CrossRef]
- Turner, D.C.; Robbins, T.W.; Clark, L.; Aron, A.R.; Dowson, J.; Sahakian, B.J. Cognitive enhancing effects of modafinil in healthy volunteers. Psychopharmacology 2003, 165, 260–269. [Google Scholar] [CrossRef]
- Mahoney, J.J. Cognitive dysfunction in individuals with cocaine use disorder: Potential moderating factors and pharmaco-logical treatments. Exp. Clin. Psychopharmacol. 2019, 27, 203–214. [Google Scholar] [CrossRef]
- Kalechstein, A.D.; Mahoney, J.J., III; Yoon, J.H.; Bennett, R.; De La Garza II, R. Modafinil, but not escitalopram, improves working memory and sustained attention in long-term, high-dose cocaine users. Neuropharmacology 2013, 64, 472–478. [Google Scholar] [CrossRef]
- Pack, A.I.; Black, J.E.; Schwartz, J.R.L.; Matheson, J.K. Modafinil as Adjunct Therapy for Daytime Sleepiness in Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2001, 164, 1675–1681. [Google Scholar] [CrossRef]
- Moldofsky, H.; Broughton, R.J.; Hill, J.D. A randomized trial of the long-term, continued efficacy and safety of modafinil in narcolepsy. Sleep Med. 2000, 1, 109–116. [Google Scholar] [CrossRef]
- Czeisler, C.A.; Walsh, J.K.; Roth, T.; Hughes, R.J.; Wright, K.P.; Kingsbury, L.; Arora, S.; Schwartz, J.R.L.; Niebler, G.E.; Dinges, D.F. Modafinil for excessive sleepiness associated with shift-work sleep disorder. N. Engl. J. Med. 2005, 353, 476–486. [Google Scholar] [CrossRef]
- Dehaene, S.; Changeux, J.-P. Experimental and theoretical approaches to conscious processing. Neuron 2011, 70, 200–227. [Google Scholar] [CrossRef]
- Dehaene, S.; Changeux, J.-P.; Naccache, L.; Sackur, J.; Sergent, C. Conscious, preconscious, and subliminal processing: A testable taxonomy. Trends Cogn. Sci. 2006, 10, 204–211. [Google Scholar] [CrossRef]
- Tononi, G. An information integration theory of consciousness. BMC Neurosci. 2004, 5, 42. [Google Scholar] [CrossRef] [PubMed]
- Ciurleo, R.; Bramanti, P.; Calabrò, R.S. Pharmacotherapy for disorders of consciousness: Are ‘awakening’ drugs really a possibility? Drugs 2013, 73, 1849–1862. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulos, M.; Katsakiori, P.; Kefalopoulou, Z.; Ellul, J.; Chroni, E.; Constantoyannis, C. Vegetative state and minimally conscious state: A review of the therapeutic interventions. Stereotact. Funct. Neurosurg. 2010, 88, 199–207. [Google Scholar] [CrossRef]
- Giacino, J.T.; Whyte, J.; Bagiella, E.; Kalmar, K.; Childs, N.; Khademi, A.; Eifert, B.; Long, D.; Katz, D.I.; Cho, S. Place-bo-controlled trial of amantadine for severe traumatic brain injury. N. Engl. J. Med. 2012, 366, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Thibaut, A.; Schiff, N.; Giacino, J.; Laureys, S.; Gosseries, O. Therapeutic interventions in patients with prolonged disorders of consciousness. Lancet Neurol. 2019, 18, 600–614. [Google Scholar] [CrossRef] [PubMed]
- Margetis, K.; Korfias, S.I.; Gatzonis, S.; Boutos, N.; Stranjalis, G.; Boviatsis, E.; Sakas, D.E. Intrathecal baclofen associated with improvement of consciousness disorders in spasticity patients. Neuromodul. Technol. Neural Interface 2014, 17, 699–704. [Google Scholar] [CrossRef]
- Pistoia, F.; Sacco, S.; Sara, M.; Franceschini, M.; Carolei, A. Intrathecal Baclofen: Effects on Spasticity, Pain, and Consciousness in Disorders of Consciousness and Locked-in Syndrome. Curr. Pain Headache Rep. 2015, 19, 466. [Google Scholar] [CrossRef]
- Castronovo, V.; Scifo, P.; Castellano, A.; Aloia, M.S.; Iadanza, A.; Marelli, S.; Cappa, S.F.; Strambi, L.F.; Falini, A. White Matter Integrity in Obstructive Sleep Apnea before and after Treatment. Sleep 2014, 37, 1465–1475. [Google Scholar] [CrossRef]
- Arendt, J.; Broadway, J. Light and melatonin as zeitgebers in man. Chronobiol. Int. 1987, 4, 273–282. [Google Scholar] [CrossRef]
- Yelden, K.; James, L.M.; Duport, S.; Kempny, A.; Farmer, S.F.; Leff, A.P.; Playford, E.D. A simple intervention for disorders of consciousness- is there a light at the end of the tunnel? Front. Neurol. 2022, 13, 824880. [Google Scholar] [CrossRef]
- Wang, J.; Di, H. Natural light exposure and circadian rhythm: A potential therapeutic approach for disorders of consciousness. Sleep 2022, 45, zac094. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Gehrman, P.; Martin, J.L.; Shochat, T.; Marler, M.; Corey-Bloom, J.; Levi, L. Increased light exposure consolidates sleep and strengthens circadian rhythms in severe Alzheimer’s disease patients. Behav. Sleep Med. 2003, 1, 22–36. [Google Scholar] [CrossRef]
- Videnovic, A.; Klerman, E.B.; Wang, W.; Marconi, A.; Kuhta, T.; Zee, P.C. Timed light therapy for sleep and daytime sleepiness associated with Parkinson disease: A randomized clinical trial. JAMA Neurol. 2017, 74, 411–418. [Google Scholar] [CrossRef]
- Beaven, C.M.; Ekström, J. A comparison of blue light and caffeine effects on cognitive function and alertness in humans. PLoS ONE 2013, 8, e76707. [Google Scholar] [CrossRef]
- Cajochen, C. Alerting effects of light. Sleep Med. Rev. 2007, 11, 453–464. [Google Scholar] [CrossRef]
- Angerer, M.; Pichler, G.; Angerer, B.; Scarpatetti, M.; Schabus, M.; Blume, C. From dawn to dusk—Mimicking natural daylight exposure improves circadian rhythm entrainment in patients with severe brain injury. Sleep 2022, 45, zac065. [Google Scholar] [CrossRef]
- Jagannath, A.; Varga, N.; Dallmann, R.; Rando, G.; Gosselin, P.; Ebrahimjee, F.; Taylor, L.; Mosneagu, D.; Stefaniak, J.; Walsh, S.; et al. Adenosine integrates light and sleep signalling for the regulation of circadian timing in mice. Nat. Commun. 2021, 12, 2113. [Google Scholar] [CrossRef]
- Blume, C.; Del Giudice, R.; Wislowska, M.; Lechinger, J.; Schabus, M. Across the consciousness continuum—From unresponsive wakefulness to sleep. Front. Hum. Neurosci. 2015, 9, 105. [Google Scholar] [CrossRef]
- Duclos, C.; Dumont, M.; Blais, H.; Paquet, J.; Potvin, M.-J.; Menon, D.K.; Bernard, F.; Gosselin, N. Severe sleep-wake dis-turbances in acute and post-acute traumatic brain injury: A case report. Brain Inj. 2014, 28, 657. [Google Scholar]
- Tononi, G.; Cirelli, C. Sleep and the Price of Plasticity: From Synaptic and Cellular Homeostasis to Memory Consolidation and Integration. Neuron 2014, 81, 12–34. [Google Scholar] [CrossRef]
- Gobert, F.; Luauté, J.; Raverot, V.; Cotton, F.; Dailler, F.; Claustrat, B.; Perrin, F.; Gronfier, C. Is circadian rhythmicity a prerequisite to coma recovery? Circadian recovery concomitant to cognitive improvement in two comatose patients. J. Pineal Res. 2019, 66, e12555. [Google Scholar] [CrossRef]
- D’Aleo, G.; Bramanti, P.; Silvestri, R.; Saltuari, L.; Gerstenbrand, F.; Di Perri, R. Sleep spindles in the initial stages of the vegetative state. Neurol. Sci. 1994, 15, 347–351. [Google Scholar] [CrossRef]
- D’Aleo, G.; Saltuari, L.; Gerstenbrand, F.; Bramanti, P. Sleep in the last remission stages of vegetative state of traumatic nature. Funct. Neurol. 1994, 9, 189–692. [Google Scholar]
- Pavlov, Y.G.; Gais, S.; Müller, F.; Schönauer, M.; Schäpers, B.; Born, J.; Kotchoubey, B. Night sleep in patients with vegetative state. J. Sleep Res. 2017, 26, 629–640. [Google Scholar] [CrossRef]
- Oksenberg, A.; Arons, E.; Sazbon, L.; Mizrahi, A.; Radwan, H. Sleep-Related Erections in Vegetative State Patients. Sleep 2000, 23, 1–5. [Google Scholar] [CrossRef]
- Giubilei, F.; Formisano, R.; Fiorini, M.; Vitale, A.; Faroni, J.; Toni, D.; Santilli, V. Sleep abnormalities in traumatic apallic syndrome. J. Neurol. Neurosurg. Psychiatry 1995, 58, 484–486. [Google Scholar] [CrossRef]
- Cologan, V.; Schabus, M.; Ledoux, D.; Moonen, G.; Maquet, P.; Laureys, S. Sleep in disorders of consciousness. Sleep Med. Rev. 2010, 14, 97–105. [Google Scholar] [CrossRef]
- Landsness, E.; Bruno, M.-A.; Noirhomme, Q.; Riedner, B.; Gosseries, O.; Schnakers, C.; Massimini, M.; Laureys, S.; Tononi, G.; Boly, M. Electrophysiological correlates of behavioural changes in vigilance in vegetative state and minimally conscious state. Brain 2011, 134, 2222–2232. [Google Scholar] [CrossRef]
- Bedin, G.; Bersano, A.; Ross, D.S.; Sattin, D.; Ciaraffa, F.; Tosetti, V.; Brenna, G.; Franceschetti, S.; Ciusani, E.; Leonardi, M.; et al. Is period 3 genotype associated with sleep and recovery in patients with disorders of consciousness? Neurorehabil. Neural Repair 2015, 30, 361–469. [Google Scholar]
- Rossi Sebastiano, D.; Panzica, F.; Visani, E.; Rotondi, F.; Scaioli, V.; Leonardi, M.; Sattin, D.; D’Incerti, L.; Parati, E.; Strambi, L.F.; et al. Significance of multiple neurophysiological measures in patients with chronic disorders of consciousness. Clin. Neurophysiol. 2015, 126, 558–564. [Google Scholar] [CrossRef]
- Saper, C.B.; Scammell, T.E.; Lu, J. Hypothalamic regulation of sleep and circadian rhythms. Nature 2005, 437, 1257–1263. [Google Scholar] [CrossRef]
- Valente, M.; Placidi, F.; Oliveira, A.; Bigagli, A.; Morghen, I.; Proietti, R.; Gigli, G. Sleep organization pattern as a prognostic marker at the subacute stage of post-traumatic coma. Clin. Neurophysiol. 2002, 113, 1798–1805. [Google Scholar] [CrossRef]
- Nakase-Ricahrdson, R.; Holcomb, E.M.; Towns, S.; Kamper, J.E.; Barnett, S.D.; Sherer, M.; Evans, C. The relationship between sleep-wake cycle disturbance and trajectory of cognitive recovery during acute traumatic brain injury. J. Head Trauma Rehabil. 2016, 31, 108–116. [Google Scholar]
- Gibson, R.M.; Ray, L.B.; LaForge, G.; Owen, A.M.; Fogel, S.M. 24-h polysomnographic recordings and electrophysiological spectral analyses from a cohort of patients with chronic disorders of consciousness. J. Neurol. 2020, 267, 3650–3663. [Google Scholar] [CrossRef]
- Frohlich, J.; Toker, D.; Monti, M.M. Consciousness among delta waves: A paradox. Brain 2021, 144, 2257–2277. [Google Scholar] [CrossRef]
- Scheinin, A.; Kantonen, O.; Alkire, M.; Långsjö, J.; Kallionpää, R.E.; Kaisti, K.; Radek, L.; Johansson, J.; Sandman, N.; Nyman, M. Foundations of human consciousness: Imaging the twilight zone. J. Neurosci. 2021, 41, 1769–1778. [Google Scholar] [CrossRef]
- Rao, V.; Neubauer, D.; Vaishnavi, S. Sleep Disturbances after Traumatic Brain Injury. Psychiatr. Times 2015, 32, 9. [Google Scholar]



{kind=link}
{kind=link}
| Treatment | Sleep Disorder | Effect |
|---|---|---|
| Modafanil | excessive sleepiness and circadian sleep–wake disorders | significant increase and stabilization of sleep–wake periods. |
| BLS | circadian sleep–wake disorders | circadian restoration of sleep–wake periods |
| CT-DBS | circadian sleep–wake disorders | modification in the cortical activity restoration of good sleep architecture and of most physiological NREM-2 and SWS stages of sleep, |
| PAP | sleep-related breathing disorders | reduction of sleep-apnoea |
| ITB | sleep-related breathing disorders | tapering ITB daily dose improved central sleep apnoea |
| Melatonin, light and caffeine | circadian sleep–wake disorders | circadian rebuilding of sleep–wake cycle |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raciti, L.; Raciti, G.; Militi, D.; Tonin, P.; Quartarone, A.; Calabrò, R.S. Sleep in Disorders of Consciousness: A Brief Overview on a Still under Investigated Issue. Brain Sci. 2023, 13, 275. https://doi.org/10.3390/brainsci13020275
Raciti L, Raciti G, Militi D, Tonin P, Quartarone A, Calabrò RS. Sleep in Disorders of Consciousness: A Brief Overview on a Still under Investigated Issue. Brain Sciences. 2023; 13(2):275. https://doi.org/10.3390/brainsci13020275
Chicago/Turabian StyleRaciti, Loredana, Gianfranco Raciti, David Militi, Paolo Tonin, Angelo Quartarone, and Rocco Salvatore Calabrò. 2023. "Sleep in Disorders of Consciousness: A Brief Overview on a Still under Investigated Issue" Brain Sciences 13, no. 2: 275. https://doi.org/10.3390/brainsci13020275
APA StyleRaciti, L., Raciti, G., Militi, D., Tonin, P., Quartarone, A., & Calabrò, R. S. (2023). Sleep in Disorders of Consciousness: A Brief Overview on a Still under Investigated Issue. Brain Sciences, 13(2), 275. https://doi.org/10.3390/brainsci13020275