
A Mid-Cycle Rise in Positive and Drop in Negative Moods among Healthy Young Women: A Pilot Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Materials
3. Results
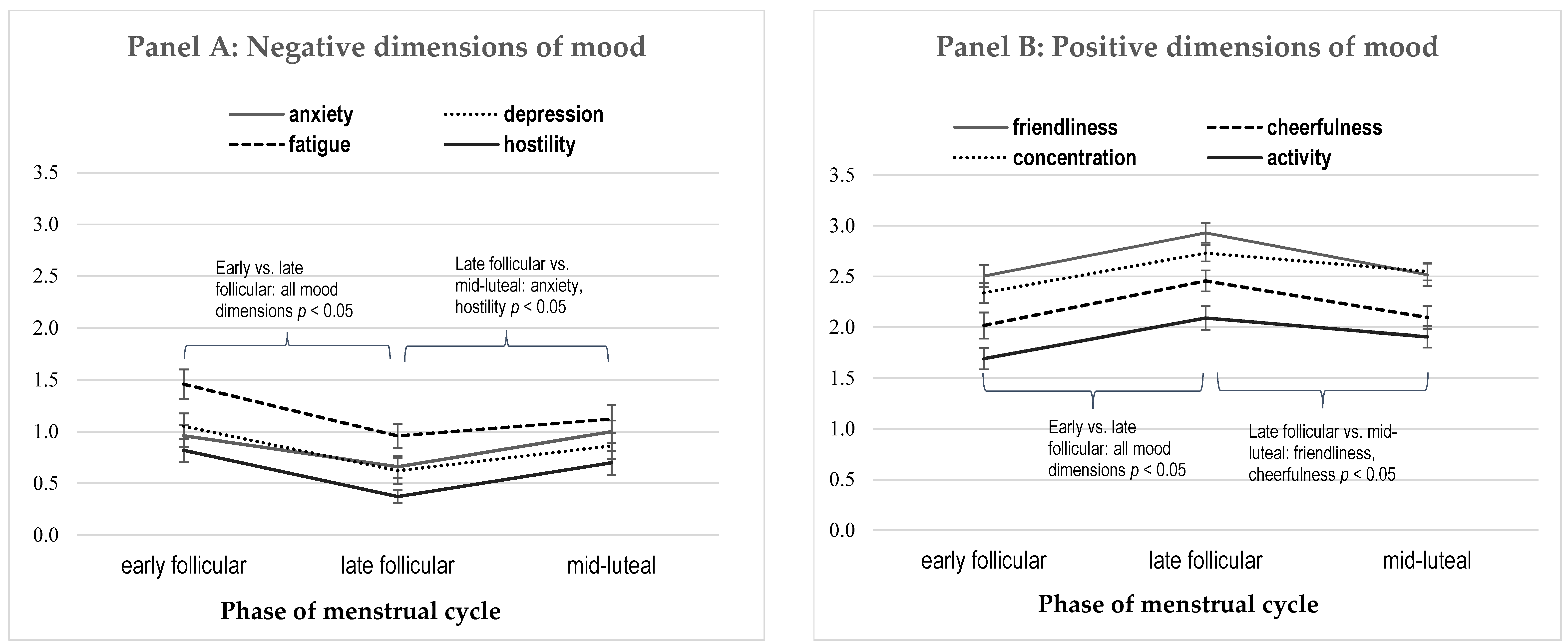
3.1. Mood across Menstrual Cycle
3.2. Co-Variability of Various Mood Dimensions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gehlert, S.; Song, I.H.; Chang, C.H.; Hartlage, S.A. The prevalence of premenstrual dysphoric disorder in a randomly selected group of urban and rural women. Psychol. Med. 2009, 39, 129–136. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, P.M.S.; Bäckström, T.; Brown, C.; Dennerstein, L.; Endicott, J.; Epperson, C.N.; Yonkers, K. Towards a consensus on diagnostic criteria, measurement and trial design of the premenstrual disorders: The ISPMD Montreal consensus. Arch. Women’s Ment. Health 2011, 14, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Sveinsdóttir, H.; Bäckström, T. Prevalence of menstrual cycle symptom cyclicity and premenstrual dysphoric disorder in a random sample of women using and not using oral contraceptives. Acta Obstet. Gynecol. Scand. 2000, 79, 405–413. [Google Scholar] [CrossRef]
- Campagne, D.M.; Campagne, G. The premenstrual syndrome revisited. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 130, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Romans, S.; Clarkson, R.; Einstein, G.; Petrovic, M.; Stewart, D. Mood and the menstrual cycle: A review of prospective data studies. Gend. Med. 2012, 9, 361–384. [Google Scholar] [CrossRef]
- Chocano-Bedoya, P.O.; Bertone-Johnson, E.R. Premenstrual Syndrome. In Women and Health; Academic Press: Cambridge, MA, USA, 2013; pp. 179–191. [Google Scholar]
- McFarlane, J.; Martin, C.L.; Williams, T.M. Mood fluctuations. Psychol. Women Q. 1988, 12, 201–223. [Google Scholar] [CrossRef]
- Lorenz, T.K.; Gesselman, A.N.; Vitzthum, V.J. Variance in mood symptoms across menstrual cycles: Implications for premenstrual dysphoric disorder. Women’s Reprod. Health 2017, 4, 77–88. [Google Scholar] [CrossRef][Green Version]
- Schwartz, D.H.; Romans, S.E.; Meiyappan, S.; De Souza, M.J.; Einstein, G. The role of ovarian steroid hormones in mood. Horm. Behav. 2012, 62, 448–454. [Google Scholar] [CrossRef]
- Gildersleeve, K.; Haselton, M.G.; Fales, M.R. Do Women’s Mate Preferences Change Across the Ovulatory Cycle? A Meta-Analytic Review. Psychol. Bull. 2014, 140, 1205–1259. [Google Scholar] [CrossRef]
- Reiber, C. An evolutionary model of premenstrual syndrome. Med. Hypotheses 2008, 70, 1058–1065. [Google Scholar] [CrossRef]
- Gangestad, S.W.; Thornhill, R. Human oestrus. Proc. R. Soc. Lond. B Biol. Sci. 2008, 275, 991–1000. [Google Scholar] [CrossRef]
- Wood, W.; Kressel, L.; Joshi, P.D.; Louie, B. Meta-analysis of menstrual cycle effects on women’s mate preferences. Emot. Rev. 2014, 6, 229–249. [Google Scholar] [CrossRef]
- Adams, D.B.; Gold, A.R.; Burt, A.D. Rise in female-initiated sexual activity at ovulation and Its suppression by oral contraceptives. N. Engl. J. Med. 1978, 299, 1145–1150. [Google Scholar] [CrossRef]
- Haselton, M.G.; Gangestad, S.W. Conditional expression of women’s desires and men’s mate guarding across the ovulatory cycle. Horm. Behav. 2006, 49, 509–518. [Google Scholar] [CrossRef]
- Harvey, M.S. Female sexual behavior: Fluctuations during the menstrual cycle. J. Psychosom. Res. 1987, 31, 101–110. [Google Scholar] [CrossRef]
- Roney, J.R.; Simmons, Z.L. Hormonal predictors of sexual motivation in natural menstrual cycles. Horm. Behav. 2013, 63, 636–645. [Google Scholar] [CrossRef]
- Udry, R.J.; Morris, N.M. Distribution of coitus in the menstrual cycle. Nature 1968, 220, 593–596. [Google Scholar] [CrossRef]
- Wilcox, A.J. On the frequency of intercourse around ovulation: Evidence for biological influences. Hum. Reprod. 2004, 19, 1539–1543. [Google Scholar] [CrossRef]
- Blake, K.R.; Bastian, B.; O’Dean, S.M.; Denson, T.F. High estradiol and low progesterone are associated with high assertiveness in women. Psychoneuroendocrinology 2017, 75, 91–99. [Google Scholar] [CrossRef]
- Durante, K.M.; Griskevicius, V.; Hill, S.E.; Perilloux, C.; Li, N.P. Ovulation, female competition, and product choice: Hormonal influences on consumer behavior. J. Consum. Res. 2011, 37, 921–934. [Google Scholar] [CrossRef]
- Gangestad, S.W.; Garver-Apgar, C.E.; Cousins, A.J.; Thornhill, R. Intersexual conflict across women’s ovulatory cycle. Evol. Hum. Behav. 2014, 35, 302–308. [Google Scholar] [CrossRef]
- Hromatko, I.; Tadinac, M.; Vranić, A. Femininity and masculinity across the menstrual cycle: A relation to mate value. Coll. Antropol. 2008, 32, 81–86. [Google Scholar]
- Miller, S.L. Hormones and Social Affiliation: Menstrual Cycle Shifts in Progesterone Underlie Women’s Attention to Signs of Social Support. Ph.D. Thesis, Florida State University, Tallahassee, FL, USA, 2011. [Google Scholar]
- Schleifenbaum, L.; Stern, J.; Driebe, J.C.; Wieczorek, L.L.; Gerlach, T.M.; Arslan, R.C.; Penke, L. Men are not aware of and do not respond to their female partner’s fertility status: Evidence from a dyadic diary study of 384 couples. Horm. Behav. 2022, 143, 105202. [Google Scholar] [CrossRef]
- Duff, S.J.; Hampson, E. A beneficial effect of estrogen on working memory in postmenopausal women taking hormone replacement therapy. Horm. Behav. 2000, 38, 262–276. [Google Scholar] [CrossRef]
- Farage, M.A.; Osborn, T.W.; MacLean, A.B. Cognitive, sensory, and emotional changes associated with the menstrual cycle: A review. Arch. Gynecol. Obstet. 2008, 278, 299–307. [Google Scholar] [CrossRef]
- Hampson, E. Variations in sex-related cognitive abilities across the menstrual cycle. Brain Cogn. 1990, 14, 26–43. [Google Scholar] [CrossRef]
- Kimura, D. Sex and Cognition; MIT Press: Cambridge, MA, USA, 2000. [Google Scholar]
- Wharton, W.; Gleason, C.E.; Olson, S.R.; Carlsson, C.M.; Asthana, S. Neurobiological Underpinnings of the Estrogen—Mood Relationship. Curr. Psychiatry Rev. 2012, 8, 247–256. [Google Scholar] [CrossRef]
- Sharkey, K.M.; Crawford, S.L.; Kim, S.; Joffe, H. Objective sleep interruption and reproductive hormone dynamics in the menstrual cycle. Sleep Med. 2014, 15, 688–693. [Google Scholar] [CrossRef]
- Dubol, M.; Wikström, J.; Lanzenberger, R.; Epperson, C.N.; Sundström-Poromaa, I.; Comasco, E. Grey matter correlates of affective and somatic symptoms of premenstrual dysphoric disorder. Sci. Rep. 2022, 12, 5996. [Google Scholar] [CrossRef]
- Hausmann, M.; Güntürkün, O. Steroid fluctuations modify functional cerebral asymmetries: The hypothesis of progesterone-mediated interhemispheric decoupling. Neuropsychologia 2000, 38, 1362–1374. [Google Scholar] [CrossRef]
- Strahler, J.; Hermann, A.; Schmidt, N.M.; Stark, R.; Hennig, J.; Munk, A.J. Food cue-elicited brain potentials change throughout menstrual cycle: Modulation by eating styles, negative affect, and premenstrual complaints. Horm. Behav. 2020, 124, 104811. [Google Scholar] [CrossRef]
- Kiesner, J.; Mendle, J.; Eisenlohr-Moul, T.A.; Pastore, M. Cyclical symptom change across the menstrual cycle: Attributional, affective, and physical symptoms. Clin. Psychol. Sci. 2016, 4, 882–894. [Google Scholar] [CrossRef]
- Kiesner, J.; Eisenlohr-Moul, T.; Mendle, J. Evolution, the Menstrual Cycle, and Theoretical Overreach. Perspect. Psychol. Sci. 2020, 15, 1113–1130. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Blake, K.R.; Dixson, B.J.W.; O’Dean, S.M.; Denson, T.F. Standardized protocols for characterizing women’s fertility: A data-driven approach. Horm. Behav. 2016, 81, 74–83. [Google Scholar] [CrossRef]
- Gangestad, S.W.; Haselton, M.G.; Welling, L.L.; Gildersleeve, K.; Pillsworth, E.G.; Burriss, R.P.; Larson, C.M.; Puts, D.A. How valid are assessments of conception probability in ovulatory cycle research? Evaluations, recommendations, and theoretical implications. Evol. Hum. Behav. 2016, 37, 85–96. [Google Scholar] [CrossRef]
- Taub, J.M.; Berger, R.J. Acute shifts in the sleep-wakefulness cycle: Effects on performance and mood. Psychosom. Med. 1974, 36, 164–173. [Google Scholar] [CrossRef]
- Prizmic, Z. Correlation among the CTQ Results and the Parameters of Circadian Variations of Oral Temperature, Pulse, and Mood Dimensions. Master’s Thesis, Department of Psychology, University of Zagreb, Zagreb, Croatia, 1988. [Google Scholar]
- Radosevic-Vidacek, B.; Vidacek, S.; Kaliterna, L. The Circadian Rhythm Parameters in Mood Variables. In Chronobiology & Chronomedicine: Basic Research and Applications. Proceedings of the 4th Annual meeting of the European Society for Chronobiology; Morgan, E., Ed.; Peter Lang: Frankfurt am Main, Germany, 1990; pp. 286–294. [Google Scholar]
- Blake, K.R.; McCartney, M.; Arslan, R.C. Menstrual cycle and hormonal contraception effects on self-efficacy, assertiveness, regulatory focus, optimism, impulsiveness, and risk-taking. J. Exp. Soc. Psychol. 2022, 10, 104382. [Google Scholar] [CrossRef]
- Schleifenbaum, L.; Driebe, J.; Gerlach, T.; Penke, L.; Arslan, R. Women feel more attractive before ovulation: Evidence from a large-scale online diary study. Evol. Hum. Sci. 2021, 3, E47. [Google Scholar] [CrossRef]
- Romans, S.E.; Clarkson, R.F.; Einstein, G.; Kreindler, D.; Aredo, S. Crying, oral contraceptive use and the menstrual cycle. J. Affect. Disord. 2017, 208, 272–277. [Google Scholar] [CrossRef]
- Havlíček, J.; Cobey, K.D.; Barrett, L.; Klapilová, K. The spandrels of Santa Barbara? A new perspective on the peri-ovulation paradigm. Behav. Ecol. 2015, 26, 1249–1260. [Google Scholar] [CrossRef]
- Barth, C.; Villringer, A.; Sacher, J. Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods. Front. Neurosci. 2015, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.G. Women’s Well-Being and the Menstrual Cycle. In Encyclopedia of Quality of Life and Well-Being Research; Springer: Berlin/Heidelberg, Germany, 2014; pp. 7173–7178. [Google Scholar]
- McAra, N. A Mixed Methods Examination of Attitudes and Perceived Mood Change and Well-Being across the Menstrual Cycle. Master’s Thesis, Abertay University, Dundee, UK, 2017. [Google Scholar]
- Sacher, J.; Okon-Singer, H.; Villringer, A. Evidence from neuroimaging for the role of the menstrual cycle in the interplay of emotion and cognition. Front. Hum. Neurosci. 2013, 7, 374. [Google Scholar] [CrossRef]
- Van Wingen, G.A.; Ossewaarde, L.; Bäckström, T.; Hermans, E.J.; Fernández, G. Gonadal hormone regulation of the emotion circuitry in humans. Neuroscience 2011, 191, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Halbreich, U.; Kahn, L.S. Role of estrogen in the aetiology and treatment of mood disorders. CNS Drugs 2001, 15, 797–817. [Google Scholar] [CrossRef] [PubMed]
- Shors, T.J.; Leuner, B. Estrogen-mediated effects on depression and memory formation in females. J. Affect. Disord. 2003, 74, 85–96. [Google Scholar] [CrossRef]
- Bull, J.R.; Rowland, S.P.; Scherwitzl, E.B.; Scherwitzl, R.; Danielsson, K.G.; Harper, J. Real-world menstrual cycle characteristics of more than 600,000 menstrual cycles. NPJ Digit. Med. 2019, 2, 83. [Google Scholar] [CrossRef]
- Arslan, R.C.; Blake, K.; Botzet, L.J.; Bürkner, P.C.; DeBruine, L.; Fiers, T.; Grebe, N.; Hahn, A.; Jones, B.C.; Marcinkowska, U.M.; et al. Not within spitting distance: Salivary immunoassays of estradiol have subpar validity for predicting cycle phase. Psychoneuroendocrinology 2022, 149, 105994. [Google Scholar] [CrossRef]


{kind=link}
| Mood Dimension | F | p | Partial Eta Squared |
|---|---|---|---|
| Anxiety | 3.436 | 0.037 | 0.072 |
| Depression | 3.929 | 0.023 | 0.082 |
| Fatigue | 4.438 | 0.015 | 0.092 |
| Hostility | 6.986 | 0.002 | 0.137 |
| Friendliness | 9.290 | 0.001 | 0.174 |
| Cheerfulness | 6.092 | 0.003 | 0.122 |
| Concentration | 6.772 | 0.002 | 0.133 |
| Energy | 3.727 | 0.028 | 0.078 |
| Compared Phases of Cycle | Mood Dimensions | |||||||
|---|---|---|---|---|---|---|---|---|
| Anxiety | Depression | Fatigue | Hostility | Friendliness | Cheerfulness | Concentration | Activity | |
| F-O | 0.035 | 0.006 | 0.004 | <0.001 | <0.001 | 0.001 | 0.001 | 0.008 |
| F-L | 0.811 | 0.252 | 0.090 | 0.393 | 0.856 | 0.515 | 0.061 | 0.159 |
| O-L | 0.013 | 0.112 | 0.285 | 0.009 | <0.001 | 0.010 | 0.083 | 0.102 |
| Anxiety | Depression | Fatigue | Hostility | Friendliness | Cheerfulness | Concentration | Activity | |
|---|---|---|---|---|---|---|---|---|
| Anxiety | 1 | 0.690 ** | 0.275 | 0.722 ** | 0.309 * | 0.406 ** | 0.341 * | 0.168 |
| Depression | 1 | 0.469 ** | 0.753 ** | 0.238 | 0.471 ** | 0.582 ** | 0.373 * | |
| Fatigue | 1 | 0.494 ** | 0.375 * | 0.391 ** | 0.415 ** | 0.720 ** | ||
| Hostility | 1 | 0.428 ** | 0.512 ** | 0.511 ** | 0.383 ** | |||
| Friendliness | 1 | 0.645 ** | 0.288 * | 0.549 ** | ||||
| Cheerfulness | 1 | 0.394 ** | 0.650 ** | |||||
| Concentration | 1 | 0.406 ** | ||||||
| Activity | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hromatko, I.; Mikac, U. A Mid-Cycle Rise in Positive and Drop in Negative Moods among Healthy Young Women: A Pilot Study. Brain Sci. 2023, 13, 105. https://doi.org/10.3390/brainsci13010105
Hromatko I, Mikac U. A Mid-Cycle Rise in Positive and Drop in Negative Moods among Healthy Young Women: A Pilot Study. Brain Sciences. 2023; 13(1):105. https://doi.org/10.3390/brainsci13010105
Chicago/Turabian StyleHromatko, Ivana, and Una Mikac. 2023. "A Mid-Cycle Rise in Positive and Drop in Negative Moods among Healthy Young Women: A Pilot Study" Brain Sciences 13, no. 1: 105. https://doi.org/10.3390/brainsci13010105
APA StyleHromatko, I., & Mikac, U. (2023). A Mid-Cycle Rise in Positive and Drop in Negative Moods among Healthy Young Women: A Pilot Study. Brain Sciences, 13(1), 105. https://doi.org/10.3390/brainsci13010105