
Profiles of Motor-Cognitive Interference in Parkinson’s Disease—The Trail-Walking-Test to Discriminate between Motor Phenotypes


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.2.1. Sociodemographic Information, Cognitive Performance, and Fall-Associated Self-Efficacy
2.2.2. Rating Scale for Parkinson’s Disease
2.2.3. Trail-Walking Test
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Reliability of Measurement Repetition in the TWT
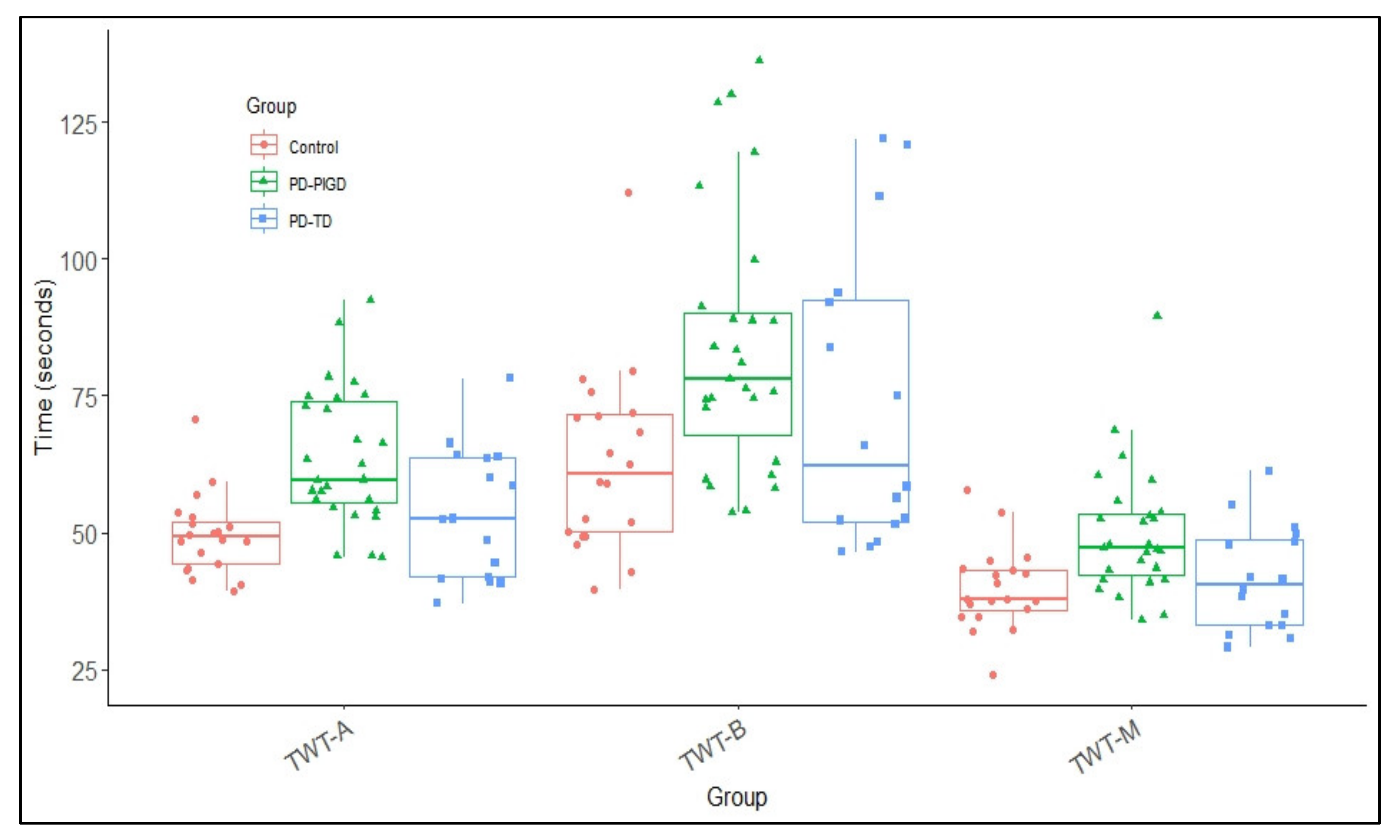
3.3. Times as Performance Measure in the TWT
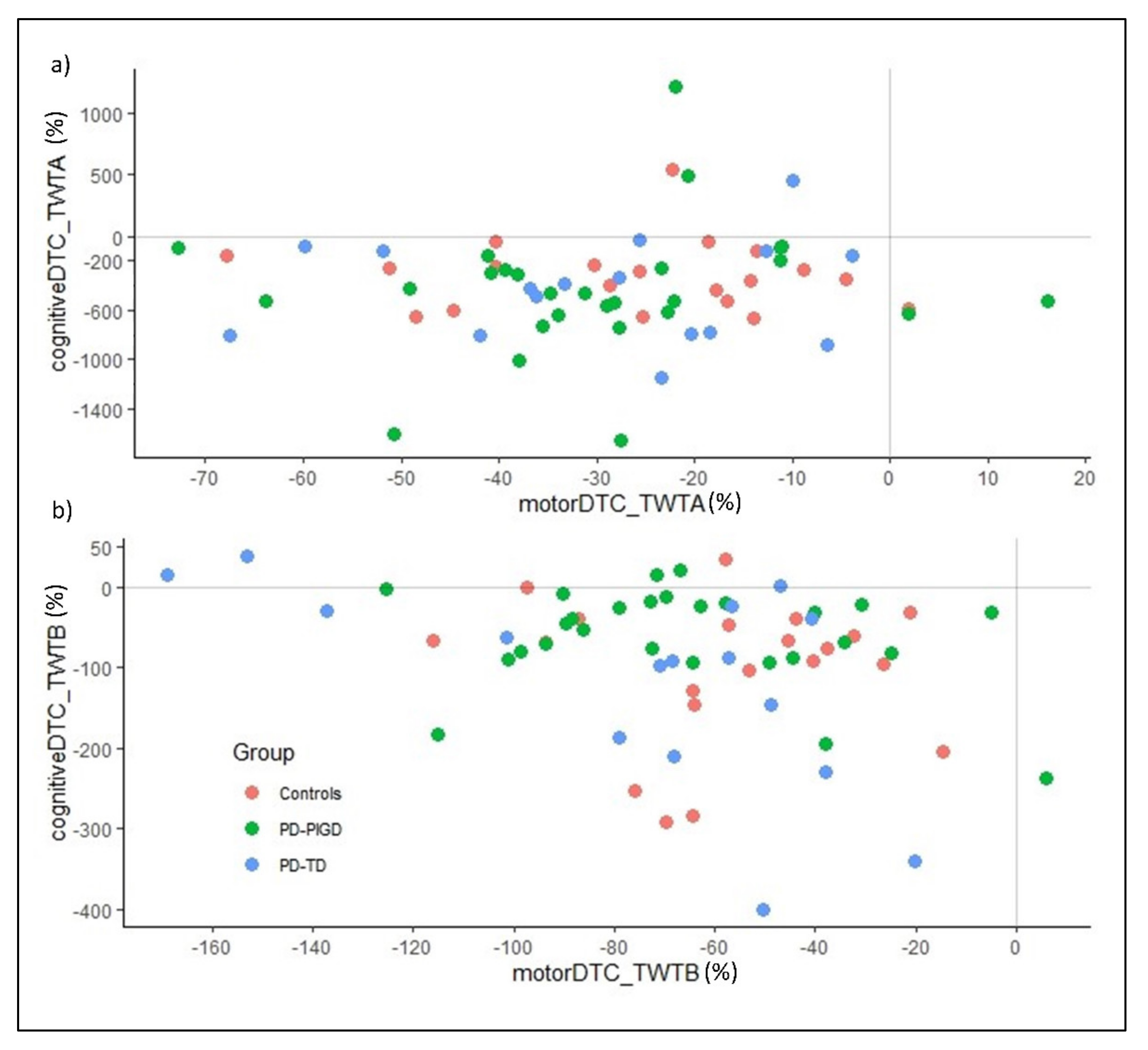
3.4. Motor-Related Cognitive Costs and Cognitive-Related Motor Costs in the TWT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aarsland, D.; Bronnick, K.; Williams-Gray, C.; Weintraub, D.; Marder, K.; Kulisevsky, J.; Burn, D.; Barone, P.; Pagonabarraga, J.; Allcock, L.; et al. Mild cognitive impairment in Parkinson disease: A multicenter pooled analysis. Neurology 2010, 75, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Watson, G.S.; Leverenz, J.B. Profile of cognitive impairment in Parkinson’s disease. Brain Pathol. 2010, 20, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Kehagia, A.A.; Barker, R.A.; Robbins, T.W. Neuropsychological and clinical heterogeneity of cognitive impairment and dementia in patients with Parkinson’s disease. Lancet Neurol. 2010, 9, 1200–1213. [Google Scholar] [CrossRef]
- Aarsland, D.; Andersen, K.; Larsen, J.P.; Lolk, A. Prevalence and characteristics of dementia in Parkinson disease: An 8-year prospective study. Arch. Neurol. 2003, 60, 387–392. [Google Scholar] [CrossRef]
- Hobson, P.; Meara, J. The detection of dementia and cognitive impairment in a community population of elderly people with Parkinson’s disease by use of the CAMCOG neuropsychological test. Age Ageing 1999, 28, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Hely, M.A.; Reid, W.G.; Adena, M.A.; Halliday, G.M.; Morris, J.G. The Sydney multicenter study of Parkinson’s disease: The inevitability of dementia at 20 years. Mov. Disord. 2008, 23, 837–844. [Google Scholar] [CrossRef]
- Amboni, M.; Barone, P.; Ms, L.I.; Lista, I.; Tranfaglia, R.; Fasano, A.; Picillo, M.; Vitale, C.; Santangelo, G.; Agosti, V.; et al. Gait patterns in parkinsonian patients with or without mild cognitive impairment. Mov. Disord. 2012, 27, 1536–1543. [Google Scholar] [CrossRef]
- Marchese, R.; Bove, M.; Abbruzzese, G. Effect of cognitive and motor tasks on postural stability in Parkinson’s disease: A posturographic study. Mov. Disord. 2003, 18, 652–658. [Google Scholar] [CrossRef]
- Kelly, V.E.; Eusterbrock, A.J.; Shumway-Cook, A. A review of dual-task walking deficits in people with Parkinson’s disease: Motor and cognitive contributions, mechanisms, and clinical implications. Parkinson’s Dis. 2012, 2012, 918719. [Google Scholar] [CrossRef]
- Pelicioni, P.H.; Menant, J.C.; Henderson, E.J.; Latt, M.D.; Brodie, M.A.; Lord, S.R. Mild and marked executive dysfunction and falls in people with Parkinson’s disease. Braz. J. Phys. Ther. 2021, 25, 437–443. [Google Scholar] [CrossRef]
- Mak, M.K.; Wong, A.; Pang, M.Y. Impaired executive function can predict recurrent falls in Parkinson’s disease. Arch. Phys. Med. Rehabil. 2014, 95, 2390–2395. [Google Scholar] [CrossRef] [PubMed]
- Foster, E.R.; Hershey, T. Everyday Executive Function is Associated with Activity Participation in Parkinson Disease without Dementia. OTJR Occup. Particip. Health 2011, 31, S16–S22. [Google Scholar] [CrossRef] [PubMed]
- Poldrack, R.A.; Sabb, F.W.; Foerde, K.; Tom, S.M.; Asarnow, R.F.; Bookheimer, S.Y.; Knowlton, B.J. The neural correlates of motor skill automaticity. J. Neurosci. 2005, 25, 5356–5364. [Google Scholar] [CrossRef] [PubMed]
- Yogev, G.; Giladi, N.; Peretz, C.; Springer, S.; Simon, E.S.; Hausdorff, J.M. Dual tasking, gait rhythmicity, and Parkinson’s disease: Which aspects of gait are attention-demanding? Eur. J. Neurosci. 2005, 22, 1248–1256. [Google Scholar] [CrossRef]
- Raffegeau, T.E.; Krehbiel, L.M.; Kang, N.; Thijs, F.J.; Altmann, L.J.; Cauraugh, J.H.; Hass, C.J. A meta-analysis: Parkinson’s disease and dual-task walking. Parkinsonism Relat. Disord. 2019, 62, 28–35. [Google Scholar] [CrossRef]
- Aleksovski, D.; Miljkovic, D.; Bravi, D.; Antonini, A. Disease progression in Parkinson subtypes: The PPMI dataset. Neurol. Sci. 2018, 39, 1971–1976. [Google Scholar] [CrossRef]
- Eggers, C.; Pedrosa, D.; Kahraman, D.; Maier, F.; Lewis, C.J.; Fink, G.R.; Schmidt, M.; Timmermann, L. Parkinson Subtypes Progress Differently in Clinical Course and Imaging Pattern. PLoS ONE 2012, 7, e46813. [Google Scholar] [CrossRef]
- Ba, F.; Obaid, M.; Wieler, M.; Camicioli, R.; Martin, W.W. Parkinson Disease: The Relationship between Non-motor Symptoms and Motor Phenotype. Can. J. Neurol. Sci./J. Can. Des Sci. Neurol. 2016, 43, 261–267. [Google Scholar] [CrossRef]
- Huang, X.; Ng, S.E.; Chia, N.Y.; Setiawan, F.; Tay, K.Y.; Au, W.L.; Tan, E.K.; Tan, L.S. Non-motor symptoms in early Parkinson’s disease with different motor subtypes and their associations with quality of life. Eur. J. Neurol. 2019, 26, 400–406. [Google Scholar] [CrossRef]
- Ren, J.; Hua, P.; Pan, C.; Li, Y.; Zhang, L.; Zhang, W.; Xu, P.; Zhang, M.; Liu, W. Non-Motor Symptoms of the Postural Instability and Gait Difficulty Subtype in De Novo Parkinson’s Disease Patients: A Cross-Sectional Study in a Single Center. Neuropsychiatr. Dis. Treat. 2020, 16, 2605–2612. [Google Scholar] [CrossRef]
- Cullen, S.; Montero-Odasso, M.; Bherer, L.; Almeida, Q.; Fraser, S.; Hunter, S.; Li, K.; Liu-Ambrose, T.; McGibbon, C.A.; McIlroy, W.; et al. Guidelines for Gait Assessments in the Canadian Consortium on Neurodegeneration in Aging (CCNA). Can. Geriatr. J. 2018, 21, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Lowry, K.A.; Brach, J.S.; Nebes, R.D.; Studenski, S.A.; VanSwearingen, J.M. Contributions of Cognitive Function to Straight- and Curved-Path Walking in Older Adults. Arch. Phys. Med. Rehabil. 2012, 93, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Mazaheri, M.; Roerdink, M.; Bood, R.J.; Duysens, J.; Beek, P.J.; Peper, C.E. Attentional costs of visually guided walking: Effects of age, executive function and stepping-task demands. Gait Posture 2014, 40, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Schott, N.; Klotzbier, T. The motor–cognitive connection: Indicator of future developmental success in children and adolescents? In Physical Activity and Educational Achievement; Routledge: London, UK, 2018; pp. 133–151. [Google Scholar]
- Beurskens, R.; Bock, O. Age-related decline of peripheral visual processing: The role of eye movements. Exp. Brain Res. 2012, 217, 117–124. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Al-Yahya, E.; Dawes, H.; Smith, L.; Dennis, A.; Howells, K.; Cockburn, J. Cognitive motor interference while walking: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2011, 35, 715–728. [Google Scholar] [CrossRef]
- Schott, N. Trail Walking Test zur Erfassung der motorisch-kognitiven Interferenz bei älteren Erwachsenen. Z. Für Gerontol. Geriatr. 2015, 48, 722–733. [Google Scholar] [CrossRef]
- Belghali, M.; Chastan, N.; Cignetti, F.; Davenne, D.; Decker, L.M. Loss of gait control assessed by cognitive-motor dual-tasks: Pros and cons in detecting people at risk of developing Alzheimer’s and Parkinson’s diseases. GeroScience 2017, 39, 305–329. [Google Scholar] [CrossRef]
- Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease. The unified Parkinson’s disease rating scale (UPDRS): Status and recommendations. Mov. Disord. 2003, 18, 738–750. [Google Scholar] [CrossRef]
- Bloem, B.R.; Marinus, J.; Almeida, Q.; Dibble, L.; Nieuwboer, A.; Post, B.; Schrag, A.; Movement Disorders Society Rating Scales Committee. Measurement instruments to assess posture, gait, and balance in Parkinson’s disease: Critique and recommendations. Mov. Disord. 2016, 31, 1342–1355. [Google Scholar] [CrossRef]
- Klotzbier, T.J.; Schott, N. Cognitive-Motor Interference during Walking in Older Adults with Probable Mild Cognitive Impairment. Front. Aging Neurosci. 2017, 9, 350. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stebbins, G.T.; Stern, M.B.; Tilley, B.C.; Dodel, R.; Dubois, B.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Process, format, and clinimetric testing plan. Mov. Disord. 2007, 22, 41–47. [Google Scholar] [CrossRef]
- Jankovic, J.; McDermott, M.; Carter, J.; Gauthier, S.; Goetz, C.; Golbe, L.; Huber, S.; Koller, W.; Olanow, C.; Shoulson, I.; et al. Variable expression of Parkinson’s disease A base-line analysis of the DAT ATOP cohort. Neurol. 1990, 40, 1529. [Google Scholar] [CrossRef]
- Blin, O.; Ferrandez, A.M.; Pailhous, J.; Serratrice, G. Dopa-sensitive and dopa-resistant gait parameters in Parkinson’s disease. J. Neurol. Sci. 1991, 103, 51–54. [Google Scholar] [CrossRef]
- Morris, M.E.; Huxham, F.; McGinley, J.; Dodd, K.; Iansek, R. The biomechanics and motor control of gait in Parkinson disease. Clin. Biomech. 2001, 16, 459–470. [Google Scholar] [CrossRef]
- Bloem, B.R.; Grimbergen, Y.A.; van Dijk, J.G.; Munneke, M. The “posture second” strategy: A review of wrong priorities in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 196–204. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. Do we always prioritize balance when walking? Towards an integrated model of task prioritization. Mov. Disord. 2012, 27, 765–770. [Google Scholar] [CrossRef]
- Johansson, H.; Ekman, U.; Rennie, L.; Peterson, D.S.; Leavy, B.; Franzén, E. Dual-Task Effects During a Motor-Cognitive Task in Parkinson’s Disease: Patterns of Prioritization and the Influence of Cognitive Status. Neurorehabilit. Neural Repair 2021, 35, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Duffin, J.T.; Collins, D.R.; Coughlan, T.; O’Neill, D.; Roche, R.A.P.; Commins, S. Subtle memory and attentional deficits revealed in an Irish stroke patient sample using domain-specific cognitive tasks. J. Clin. Exp. Neuropsychol. 2012, 34, 864–875. [Google Scholar] [CrossRef]
- Kenny, R.A.; Coen, R.F.; Frewen, J.; Donoghue, O.A.; Cronin, H.; Savva, G.M. Normative Values of Cognitive and Physical Function in Older Adults: Findings from The Irish Longitudinal Study on Ageing. J. Am. Geriatr. Soc. 2013, 61, S279–S290. [Google Scholar] [CrossRef]
- Reitan, R. Validity of TMT as an indication of organic brain damage. Percept. Mot. Ski. 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Schott, N.; El-Rajab, I.; Klotzbier, T. Cognitive-motor interference during fine and gross motor tasks in children with Developmental Coordination Disorder (DCD). Res. Dev. Disabil. 2016, 57, 136–148. [Google Scholar] [CrossRef]
- Powell, L.E.; Myers, A.M. The activities-specific balance confidence (ABC) scale. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1995, 50, M28–M34. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Allison, L.K.; Painter, J.A.; Emory, A.; Whitehurst, P.; Raby, A. Participation Restriction, Not Fear of Falling, Predicts Actual Balance and Mobility Abilities in Rural Community-Dwelling Older Adults. J. Geriatr. Phys. Ther. 2013, 36, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Klusman, L.E.; Cripe, L.I.; Dodrill, C.B. Analysis of Errors on the Trail Making Test. Percept. Mot. Ski. 1989, 68 (Suppl. S3), 1199–1204. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2007; Volume 5, pp. 481–498. [Google Scholar]
- Eplummer, P.; A Eskes, G. Measuring treatment effects on dual-task performance: A framework for research and clinical practice. Front. Hum. Neurosci. 2015, 9, 225. [Google Scholar] [CrossRef]
- Gaudino, E.A.; Geisler, M.W.; Squires, N.K. Construct validity in the trail making test: What makes part B harder? J. Clin. Exp. Neuropsychol. 1995, 17, 529–535. [Google Scholar] [CrossRef]
- Fleiss, J.L. Reliability of Measurement. In The Design and Analysis of Clinical Experiments; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 1999; pp. 1–32. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the sem. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Nevill, A.M. Statistical Methods for Assessing Measurement Error (Reliability) in Variables Relevant to Sports Medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Swets, J.A. Measuring the accuracy of diagnostic systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Hilden, J.; Glasziou, P. Regret graphs, diagnostic uncertainty and Youden’s Index. Stat. Med. 1996, 15, 969–986. [Google Scholar] [CrossRef]
- Lord, S.; Rochester, L.; Hetherington, V.; Allcock, L.M.; Burn, D. Executive dysfunction and attention contribute to gait interference in ‘off’ state Parkinson’s Disease. Gait Posture 2010, 31, 169–174. [Google Scholar] [CrossRef]
- Spildooren, J.; Vercruysse, S.; Desloovere, K.; Vandenberghe, W.; Kerckhofs, E.; Nieuwboer, A. Freezing of gait in Parkinson’s disease: The impact of dual-tasking and turning. Mov. Disord. 2010, 25, 2563–2570. [Google Scholar] [CrossRef]
- Wild, L.B.; De Lima, D.B.; Balardin, J.B.; Rizzi, L.; Giacobbo, B.L.; Oliveira, H.B.; Argimon, I.; Peyré-Tartaruga, L.A.; Rieder, C.R.; Bromberg, E. Characterization of cognitive and motor performance during dual-tasking in healthy older adults and patients with Parkinson’s disease. J. Neurol. 2013, 260, 580–589. [Google Scholar] [CrossRef]
- Kelly, V.E.; Shumway-Cook, A. The ability of people with Parkinson’s disease to modify dual-task performance in response to instructions during simple and complex walking tasks. Exp. Brain Res. 2014, 232, 263–271. [Google Scholar] [CrossRef] [PubMed]
- LaPointe, L.L.; Stierwalt, J.A.; Maitland, C.G. Talking while walking: Cognitive loading and injurious falls in Parkinson’s disease. Int. J. Speech-Lang. Pathol. 2010, 12, 455–459. [Google Scholar] [CrossRef]
- Yogev, G.; Plotnik, M.; Peretz, C.; Giladi, N.; Hausdorff, J.M. Gait asymmetry in patients with Parkinson’s disease and elderly fallers: When does the bilateral coordination of gait require attention? Exp. Brain Res. 2007, 177, 336–346. [Google Scholar] [CrossRef]
- Lord, S.; Baker, K.; Nieuwboer, A.; Burn, D.; Rochester, L. Gait variability in Parkinson’s disease: An indicator of non-dopaminergic contributors to gait dysfunction? J. Neurol. 2011, 258, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Galletly, R.; Brauer, S.G. Does the type of concurrent task affect preferred and cued gait in people with Parkinson’s disease? Aust. J. Physiother. 2005, 51, 175–180. [Google Scholar] [CrossRef]
- O’Shea, S.; Morris, M.; Iansek, R. Dual Task Interference during Gait in People with Parkinson Disease: Effects of Motor Versus Cognitive Secondary Tasks. Phys. Ther. 2002, 82, 888–897. [Google Scholar] [CrossRef]
- Tombu, M.; Jolicœur, P. A central capacity sharing model of dual-task performance. J. Exp. Psychol. Hum. Percept. Perform. 2003, 29, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Maetzler, W.; Hausdorff, J.M. Motor signs in the prodromal phase of Parkinson’s disease. Mov. Disord. 2012, 27, 627–633. [Google Scholar] [CrossRef]
- Mirelman, A.; Ben Or Frank, M.; Melamed, M.; Granovsky, L.; Nieuwboer, A.; Rochester, L.; Del Din, S.; Avanzino, L.; Pelosin, E.; Bloem, B.R.; et al. Detecting Sensitive Mobility Features for Parkinson’s Disease Stages Via Machine Learning. Mov. Disord. 2021, 36, 2144–2155. [Google Scholar] [CrossRef] [PubMed]
- Bridenbaugh, S.A.; Kressig, R.W. Motor cognitive dual tasking. Z. Für Gerontol. Geriatr. 2015, 48, 15–21. [Google Scholar] [CrossRef]
- Vance, R.C.; Healy, D.G.; Galvin, R.; French, H.P. Dual Tasking with the Timed “Up & Go” Test Improves Detection of Risk of Falls in People with Parkinson Disease. Phys. Ther. 2015, 95, 95–102. [Google Scholar] [CrossRef]
- Heinzel, S.; Maechtel, M.; Hasmann, S.E.; Hobert, M.A.; Heger, T.; Berg, D.; Maetzler, W. Motor dual-tasking deficits predict falls in Parkinson’s disease: A prospective study. Parkinsonism Relat. Disord. 2016, 26, 73–77. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control | TD | PIGD | |
|---|---|---|---|
| Inclusion criteria |
|
|
|
| Exclusion criteria |
|
|
|
| UPDRS | |||
|---|---|---|---|
| N Items | Tremor-Dominant (TD) | N Items | Postural Instability and Gait Difficulty (PIGD) |
| Part 2—Activities of daily living (ADL) | |||
| 1 | 2.16 Tremor | 3 | 2.13 Falling (independent of rigidity) 2.14 Freezing during walking 2.15 Walking |
| Part 3—Motor examination | |||
| 7 | 3.20 Rest Tremor, F 3.20 Rest Tremor, RH 3.20 Rest Tremor, LH 3.20 Rest Tremor, RF 3.20 Rest Tremor, LF 3.21 Action or posture tremor of the hands, L 3.21 Action or posture tremor of the hands, R | 2 | 3.29 Gait 3.30 Postural Stability * |
| Control | TD Ratio ≤ 1.5 | PIGD Ratio ≥ 1.0 | Stat. Analyses | |
|---|---|---|---|---|
| (n = 20) | (n = 16) | (n = 27) | ||
| sex | 7 men, 13 women | 11 men, 5 women | 23 men, 4 women | CHI2(2) = 14.2 ** |
| age (years) | 72.4 (5.53) | 68.2 (8.94) | 69.7 (8.68) | F(2, 60) = 1.32, ɳ2p = 0.042 |
| BMI (kg/m2) Under-, Normal-, Obesity (n) | 27.9 (4.73); 0, 6, 6, 5 | 24.2 (4.40) ŧ; 2, 6, 6, 1 | 27.4 (4.07); 0, 8, 12, 5 | F(2, 57) = 3.79 *, ɳ2p = 0.117 |
| UPDRS-III (Score; max = 108) | - | 22.53 (7.47) | 23.7 (7.97) | t(41) = 0.646, d = 0.147 |
| Duration of the disease (years) | - | 6.19 (4.92) | 4.93 (4.37) | t(41) = 0.388, d = 0.275 |
| Activities Specific Balance Confidence (ABC)Scale, % | 95.3 (3.77) | 89.7 (8.24) | 79.3 (19.9) ŧ | F(2, 59) = 8.05 **, ɳ2p = 0.214 |
| Fall experience last year (n persons; n in %, n falls) | 3 persons (15%); 3 falls | 4 persons (26.7%); 6 falls | 9 persons (33%); 31 falls | F(2, 14) = 1.68, ɳ2p = 0.222 |
| Timed Up-and-Go test (TUG), seconds | 8.55 (1.29) | 9.19 (2.28) | 11.1 (2.99) ŧ | F(2, 61) = 7.29 *, ɳ2p = 0.198 |
| Montreal Cognitive Assessment (MoCA), score | 27.9 (1.48) | 26.9 (3.23) | 27.6 (1.95) | F(2, 60) = 0.854, ɳ2p = 0.028 |
| 2 participants with a score below 26 | 4 participants with a score below 26 | 6 participants with a score below 26 | CHI2(2) = 1.61 | |
| Education (years) | 10.5 (0.76) | 13.7 (4.17) | 13.5 (3.40) ŧ | F(2, 61) = 6.62 **, ɳ2p = 0.189 |
| Geriatric Depression Scale (GDS), n | 20 normal 0 mild to moderate 0 severe | 15 normal 1 mild to moderate 0 severe | 22 normal 5 mild to moderate 0 severe | CHI2(2) = 3.21 |
| Control | TD | PIGD | |||||||
|---|---|---|---|---|---|---|---|---|---|
| ICC (95% CI) | SEM/ SEM (%) | MDC95/MDC95% | ICC (95% CI) | SEM/ SEM (%) | MDC95/MDC95% | ICC (95% CI) | SEM/ SEM (%) | MDC95/MDC95% | |
| TWT-M | 0.974 (0.95–0.99) | 0.26/ 0.68 | 0.76/ 1.89 | 0.987 (0.97–0.99) | 0.22/ 0.51 | 0.62/ 1.41 | 0.959 (0.92–0.98) | 0.43/ 0.74 | 1.18/ 2.05 |
| TWT-A | 0.894 (0.78–0.96) | 1.15/ 2.31 | 3.19/ 6.39 | 0.959 (0.90–0.98) | 0.72/ 1.33 | 1.99/ 3.68 | 0.939 (0.88–0.97) | 1.03/ 1.63 | 2.86/ 4.54 |
| TWT-B | 0.870 (0.72–0.94) | 2.68/ 4.05 | 7.43/ 11.21 | 0.886 (0.74–0.96) | 3.20/ 4.14 | 8.88/ 11.48 | 0.918 (0.84–0.96) | 2.18/ 2.59 | 6.02/ 7.17 |
| PIGD (n = 27) | TD (n = 16) | Control (n = 20) | Statistical Analysis | |
|---|---|---|---|---|
| Motor DTC TWT-A | −29.9 (18.4) | −29.7 (18.7) | −26.6 (17.6) | F(2, 60) = 0.220, p = 0.803, ɳ2p = 0.007 |
| Motor DTC TWT-B | −65.4 (31.9) | −75.4 (43.1) | −58.1 (26.8) | F(2, 33) = 1.16, p = 0.320, ɳ2p = 0.037 |
| Cognitive DTC TWT-A | −431 (543) | −430 (417) | −317 (284) | F(2, 33) = 0.445, p = 0.643, ɳ2p = 0.015 |
| Cognitive DTC TWT-B | −61.2 (62.2) | −118 (126) | −103 (90.8) | F(2, 33) = 2.33, p = 0.106, ɳ2p = 0.072 |
| Condition | Groups | n | Youden Index | Sensitivity | Specificity | Threshold | AUC | p |
|---|---|---|---|---|---|---|---|---|
| TWT-M | PIGD vs. TD | 27/16 | 0.326 | 0.889 | 0.438 | 1.05 | 0.685 | 0.044 |
| PIGD vs. Control | 27/20 | 0.530 | 0.630 | 0.900 | 0.891 | 0.791 | <0.001 | |
| TD vs. Control | 16/20 | 0.288 | 0.436 | 0.850 | 0.914 | 0.553 | 0.588 | |
| TWT-A | PIGD vs TD | 27/16 | 0.352 | 0.852 | 0.500 | 0.778 | 0.662 | 0.079 |
| PIGD vs. Control | 27/20 | 0.652 | 0.852 | 0.800 | 0.776 | 0.831 | <0.001 | |
| TD vs. Control | 16/20 | 0.400 | 0.500 | 0.900 | 0.711 | 0.638 | 0.161 | |
| TWT-B | PIGD vs. TD | 27/16 | 0.303 | 0.741 | 0.563 | 0.593 | 0.623 | 0.183 |
| PIGD vs. Control | 27/20 | 0.541 | 0.741 | 0.800 | 0.567 | 0.783 | <0.001 | |
| TD vs. Control | 16/20 | 0.325 | 0.375 | 0.950 | 0.503 | 0.613 | 0.252 | |
| Motor DTC TWT-A | PIGD vs. TD | 27/16 | 0.234 | 0.296 | 0.938 | −16.52 | 0.588 | 0.340 |
| PIGD vs. Control | 27/20 | 0.356 | 0.556 | 0.800 | −37.81 | 0.659 | 0.064 | |
| TD vs. Control | 16/20 | 0.300 | 0.500 | 0.800 | −38.13 | 0.597 | 0.324 | |
| Motor DTC TWT-B | PIGD vs. TD | 27/16 | −0.093 | 0.407 | 0.500 | −241.1 | 0.479 | 0.821 |
| PIGD vs. Control | 27/20 | −0.089 | 0.111 | 0.800 | −133.7 | 0.513 | 0.880 | |
| TD vs. Control | 16/20 | 0.188 | 0.938 | 0.250 | −378.7 | 0.541 | 0.679 | |
| Cognitive DTC TWT-A | PIGD vs. TD | 27/16 | 0.264 | 0.889 | 0.625 | −823.6 | 0.528 | 0.763 |
| PIGD vs. Control | 27/20 | −0.219 | 0.481 | 0.300 | −493.3 | 0.431 | 0.426 | |
| TD vs. Control | 16/20 | −0.375 | 0.625 | 0.000 | −786.5 | 0.413 | 0.373 | |
| Cognitive DTC TWT-B | PIGD vs. TD | 27/16 | 0.215 | 0.778 | 0.438 | −35.53 | 0.567 | 0.466 |
| PIGD vs. Control | 27/20 | 0.344 | 0.444 | 0.900 | 2.65 | 0.615 | 0.182 | |
| TD vs. Control | 16/20 | 0.225 | 0.375 | 0.850 | −3.94 | 0.544 | 0.656 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klotzbier, T.J.; Schott, N.; Almeida, Q.J. Profiles of Motor-Cognitive Interference in Parkinson’s Disease—The Trail-Walking-Test to Discriminate between Motor Phenotypes. Brain Sci. 2022, 12, 1217. https://doi.org/10.3390/brainsci12091217
Klotzbier TJ, Schott N, Almeida QJ. Profiles of Motor-Cognitive Interference in Parkinson’s Disease—The Trail-Walking-Test to Discriminate between Motor Phenotypes. Brain Sciences. 2022; 12(9):1217. https://doi.org/10.3390/brainsci12091217
Chicago/Turabian StyleKlotzbier, Thomas J., Nadja Schott, and Quincy J. Almeida. 2022. "Profiles of Motor-Cognitive Interference in Parkinson’s Disease—The Trail-Walking-Test to Discriminate between Motor Phenotypes" Brain Sciences 12, no. 9: 1217. https://doi.org/10.3390/brainsci12091217
APA StyleKlotzbier, T. J., Schott, N., & Almeida, Q. J. (2022). Profiles of Motor-Cognitive Interference in Parkinson’s Disease—The Trail-Walking-Test to Discriminate between Motor Phenotypes. Brain Sciences, 12(9), 1217. https://doi.org/10.3390/brainsci12091217