
Chemobrain, Olfactory and Lifestyle Assessment in Onco-Geriatrics: Sex-Mediated Differences between Chemotherapy and Immunotherapy

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
1.1. The Chemobrain and Oncologic Therapy
1.2. Chemosensory Functions and Chemobrain
1.3. Geriatric and Nutritional Aspects of the Elderly Oncological Patient
2. Materials and Methods
2.1. Participants
2.2. Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bender, C.M.; Thelen, B.D. Cancer and Cognitive Changes: The Complexity of the Problem. Semin. Oncol. Nurs. 2013, 29, 232–237. [Google Scholar] [CrossRef]
- Joly, F.; Giffard, B.; Rigal, O.; Ruiter, M.B.D.; Small, B.J.; Dubois, M.; LeFel, J.; Schagen, S.B.; Ahles, T.A.; Wefel, J.S.; et al. Impact of Cancer and Its Treatments on Cognitive Function: Advances in Research From the Paris International Cognition and Cancer Task Force Symposium and Update Since 2012. J. Pain Symptom Manag. 2015, 50, 830–841. [Google Scholar] [CrossRef]
- Kovalchuk, A.; Kolb, B. Chemo Brain: From Discerning Mechanisms to Lifting the Brain Fog—An Aging Connection. Cell Cycle 2017, 16, 1345–1349. [Google Scholar] [CrossRef]
- Jim, H.S.L.; Phillips, K.M.; Chait, S.; Faul, L.A.; Popa, M.A.; Lee, Y.-H.; Hussin, M.G.; Jacobsen, P.B.; Small, B.J. Meta-Analysis of Cognitive Functioning in Breast Cancer Survivors Previously Treated With Standard-Dose Chemotherapy. J. Clin. Oncol. 2012, 30, 3578–3587. [Google Scholar] [CrossRef] [PubMed]
- Tannock, I.F.; Ahles, T.A.; Ganz, P.A.; Van Dam, F.S. Cognitive Impairment Associated with Chemotherapy for Cancer: Report of a Workshop. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 2233–2239. [Google Scholar] [CrossRef]
- Hodgson, K.D.; Hutchinson, A.D.; Wilson, C.J.; Nettelbeck, T. A Meta-Analysis of the Effects of Chemotherapy on Cognition in Patients with Cancer. Cancer Treat. Rev. 2013, 39, 297–304. [Google Scholar] [CrossRef]
- Argyriou, A.A.; Assimakopoulos, K.; Iconomou, G.; Giannakopoulou, F.; Kalofonos, H.P. Either Called “Chemobrain” or “Chemofog,” the Long-Term Chemotherapy-Induced Cognitive Decline in Cancer Survivors Is Real. J. Pain Symptom Manag. 2011, 41, 126–139. [Google Scholar] [CrossRef]
- Downie, F.P.; Mar Fan, H.G.; Houédé-Tchen, N.; Yi, Q.; Tannock, I.F. Cognitive Function, Fatigue, and Menopausal Symptoms in Breast Cancer Patients Receiving Adjuvant Chemotherapy: Evaluation with Patient Interview after Formal Assessment. Psychooncology 2006, 15, 921–930. [Google Scholar] [CrossRef]
- Myers, J.S. Cancer- and Chemotherapy-Related Cognitive Changes: The Patient Experience. Semin. Oncol. Nurs. 2013, 29, 300–307. [Google Scholar] [CrossRef]
- O’Farrell, E.; MacKenzie, J.; Collins, B. Clearing the Air: A Review of Our Current Understanding of “Chemo Fog”. Curr. Oncol. Rep. 2013, 15, 260–269. [Google Scholar] [CrossRef]
- Cheng, H.; Yang, Z.; Dong, B.; Chen, C.; Zhang, M.; Huang, Z.; Chen, Z.; Wang, K. Chemotherapy-Induced Prospective Memory Impairment in Patients with Breast Cancer. Psychooncology 2013, 22, 2391–2395. [Google Scholar] [CrossRef]
- Abraham, J.; Haut, M.W.; Moran, M.T.; Filburn, S.; Lemiuex, S.; Kuwabara, H. Adjuvant Chemotherapy for Breast Cancer: Effects on Cerebral White Matter Seen in Diffusion Tensor Imaging. Clin. Breast Cancer 2008, 8, 88–91. [Google Scholar] [CrossRef]
- Ferguson, R.J.; McDonald, B.C.; Saykin, A.J.; Ahles, T.A. Brain Structure and Function Differences in Monozygotic Twins: Possible Effects of Breast Cancer Chemotherapy. J. Clin. Oncol. 2007, 25, 3866–3870. [Google Scholar] [CrossRef]
- Wieneke, M.H.; Dienst, E.R. Neuropsychological Assessment of Cognitive Functioning Following Chemotherapy for Breast Cancer. Psychooncology 1995, 4, 61–66. [Google Scholar] [CrossRef]
- Chen, X.; Li, J.; Ren, J.; Hu, X.; Zhu, C.; Tian, Y.; Hu, P.; Ma, H.; Yu, F.; Wang, K. Selective Impairment of Attention Networks in Breast Cancer Patients Receiving Chemotherapy Treatment. Psychooncology 2014, 23, 1165–1171. [Google Scholar] [CrossRef]
- Ahles, T.A.; Saykin, A.J.; McDonald, B.C.; Li, Y.; Furstenberg, C.T.; Hanscom, B.S.; Mulrooney, T.J.; Schwartz, G.N.; Kaufman, P.A. Longitudinal Assessment of Cognitive Changes Associated With Adjuvant Treatment for Breast Cancer: Impact of Age and Cognitive Reserve. J. Clin. Oncol. 2010, 28, 4434–4440. [Google Scholar] [CrossRef]
- Wigmore, P. The Effect of Systemic Chemotherapy on Neurogenesis, Plasticity and Memory. In Neurogenesis and Neural Plasticity; Belzung, C., Wigmore, P., Eds.; Current Topics in Behavioral Neurosciences; Springer: Berlin/Heidelberg, Germany, 2013; pp. 211–240. ISBN 978-3-642-36232-3. [Google Scholar]
- Dietrich, J.; Monje, M.; Wefel, J.; Meyers, C. Clinical Patterns and Biological Correlates of Cognitive Dysfunction Associated with Cancer Therapy. Oncologist 2008, 13, 1285–1295. [Google Scholar] [CrossRef]
- Nelson, C.J.; Nandy, N.; Roth, A.J. Chemotherapy and Cognitive Deficits: Mechanisms, Findings, and Potential Interventions. Palliat. Support. Care 2007, 5, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Seigers, R.; Fardell, J.E. Neurobiological Basis of Chemotherapy-Induced Cognitive Impairment: A Review of Rodent Research. Neurosci. Biobehav. Rev. 2011, 35, 729–741. [Google Scholar] [CrossRef]
- Linden, W.; Vodermaier, A.; MacKenzie, R.; Greig, D. Anxiety and Depression after Cancer Diagnosis: Prevalence Rates by Cancer Type, Gender, and Age. J. Affect. Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef]
- Patrick, D.L.; Unützer, J. RESPONSE: Re: National Institutes of Health State-of-the-Science Conference Statement: Symptom Management in Cancer: Pain, Depression, and Fatigue, July 15–17, 2002. JNCI J. Natl. Cancer Inst. 2004, 96, 1110. [Google Scholar] [CrossRef][Green Version]
- Hurria, A.; Li, D.; Hansen, K.; Patil, S.; Gupta, R.; Nelson, C.; Lichtman, S.M.; Tew, W.P.; Hamlin, P.; Zuckerman, E.; et al. Distress in Older Patients With Cancer. J. Clin. Oncol. 2009, 27, 4346–4351. [Google Scholar] [CrossRef]
- Bower, J.E. Cancer-Related Fatigue—Mechanisms, Risk Factors, and Treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef]
- Loh, K.P.; Janelsins, M.C.; Mohile, S.G.; Holmes, H.M.; Hsu, T.; Inouye, S.K.; Karuturi, M.S.; Kimmick, G.G.; Lichtman, S.M.; Magnuson, A.; et al. Chemotherapy-Related Cognitive Impairment in Older Patients with Cancer. J. Geriatr. Oncol. 2016, 7, 270–280. [Google Scholar] [CrossRef]
- Kaiser, J.; Bledowski, C.; Dietrich, J. Neural Correlates of Chemotherapy-Related Cognitive Impairment. Cortex 2014, 54, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Monje, M.; Dietrich, J. Cognitive Side Effects of Cancer Therapy Demonstrate a Functional Role for Adult Neurogenesis. Behav. Brain Res. 2012, 227, 376–379. [Google Scholar] [CrossRef]
- Castellon, S.A.; Ganz, P.A.; Bower, J.E.; Petersen, L.; Abraham, L.; Greendale, G.A. Neurocognitive Performance in Breast Cancer Survivors Exposed to Adjuvant Chemotherapy and Tamoxifen. J. Clin. Exp. Neuropsychol. 2004, 26, 955–969. [Google Scholar] [CrossRef]
- Mandelblatt, J.S.; Hurria, A.; McDonald, B.C.; Saykin, A.J.; Stern, R.A.; VanMeter, J.W.; McGuckin, M.; Traina, T.; Denduluri, N.; Turner, S.; et al. Cognitive Effects of Cancer and Its Treatments at the Intersection of Aging: What Do We Know; What Do We Need to Know? Semin. Oncol. 2013, 40, 709–725. [Google Scholar] [CrossRef]
- Ahles, T.A.; Saykin, A.J. Candidate Mechanisms for Chemotherapy-Induced Cognitive Changes. Nat. Rev. Cancer 2007, 7, 192–201. [Google Scholar] [CrossRef]
- Kroschinsky, F.; Stölzel, F.; von Bonin, S.; Beutel, G.; Kochanek, M.; Kiehl, M.; Schellongowski, P.; Intensive Care in Hematological and Oncological Patients (iCHOP) Collaborative Group. New Drugs, New Toxicities: Severe Side Effects of Modern Targeted and Immunotherapy of Cancer and Their Management. Crit. Care 2017, 21, 89. [Google Scholar] [CrossRef]
- Ranpura, V.; Hapani, S.; Wu, S. Treatment-Related Mortality with Bevacizumab in Cancer Patients: A Meta-Analysis. JAMA 2011, 305, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Capuron, L.; Ravaud, A.; Dantzer, R. Timing and Specificity of the Cognitive Changes Induced by Interleukin-2 and Interferon-Alpha Treatments in Cancer Patients. Psychosom. Med. 2001, 63, 376–386. [Google Scholar] [CrossRef] [PubMed]
- McGinnis, G.J.; Friedman, D.; Young, K.H.; Torres, E.R.S.; Thomas, C.R.; Gough, M.J.; Raber, J. Neuroinflammatory and Cognitive Consequences of Combined Radiation and Immunotherapy in a Novel Preclinical Model. Oncotarget 2017, 8, 9155–9173. [Google Scholar] [CrossRef]
- Joly, F.; Castel, H.; Tron, L.; Lange, M.; Vardy, J. Potential Effect of Immunotherapy Agents on Cognitive Function in Cancer Patients. JNCI J. Natl. Cancer Inst. 2020, 112, 123–127. [Google Scholar] [CrossRef]
- Cuzzubbo, S.; Javeri, F.; Tissier, M.; Roumi, A.; Barlog, C.; Doridam, J.; Lebbe, C.; Belin, C.; Ursu, R.; Carpentier, A.F. Neurological Adverse Events Associated with Immune Checkpoint Inhibitors: Review of the Literature. Eur. J. Cancer 2017, 73, 1–8. [Google Scholar] [CrossRef]
- Farkona, S.; Diamandis, E.P.; Blasutig, I.M. Cancer Immunotherapy: The Beginning of the End of Cancer? BMC Med. 2016, 14, 73. [Google Scholar] [CrossRef]
- Dougan, M.; Dranoff, G. Immune Therapy for Cancer. Annu. Rev. Immunol. 2009, 27, 83–117. [Google Scholar] [CrossRef]
- Wefel, J.S.; Witgert, M.E.; Meyers, C.A. Neuropsychological Sequelae of Non-Central Nervous System Cancer and Cancer Therapy. Neuropsychol. Rev. 2008, 18, 121–131. [Google Scholar] [CrossRef]
- Valentine, A.D.; Meyers, C.A. Neurobehavioral Effects of Interferon Therapy. Curr. Psychiatry Rep. 2005, 7, 391–395. [Google Scholar] [CrossRef]
- Hummel, T.; Nordin, S. Olfactory Disorders and Their Consequences for Quality of Life. Acta Otolaryngol. 2005, 125, 116–121. [Google Scholar] [CrossRef]
- Croy, I.; Negoias, S.; Novakova, L.; Landis, B.N.; Hummel, T. Learning about the Functions of the Olfactory System from People without a Sense of Smell. PLoS ONE 2012, 7, e33365. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Bromley, S.M. Effects of Drugs on Olfaction and Taste. Otolaryngol. Clin. N. Am. 2004, 37, 1229–1254. [Google Scholar] [CrossRef]
- Patel, R.M.; Pinto, J.M. Olfaction: Anatomy, physiology, and disease. Clin. Anat. 2013, 27, 54–60. [Google Scholar] [CrossRef]
- Cohen, J.; Wakefield, C.E.; Laing, D.G. Smell and Taste Disorders Resulting from Cancer and Chemotherapy. Curr. Pharm. Des. 2016, 22, 2253–2263. [Google Scholar] [CrossRef]
- Comeau, T.B.; Epstein, J.B.; Migas, C. Taste and Smell Dysfunction in Patients Receiving Chemotherapy: A Review of Current Knowledge. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2001, 9, 575–580. [Google Scholar] [CrossRef]
- Faure, F.; Da Silva, S.V.; Jakob, I.; Pasquis, B.; Sicard, G. Peripheral Olfactory Sensitivity in Rodents after Treatment with Docetaxel. Laryngoscope 2010, 120, 690–697. [Google Scholar] [CrossRef]
- Kai, K.; Satoh, H.; Kajimura, T.; Kato, M.; Uchida, K.; Yamaguchi, R.; Tateyama, S.; Furuhama, K. Olfactory Epithelial Lesions Induced by Various Cancer Chemotherapeutic Agents in Mice. Toxicol. Pathol. 2004, 32, 701–709. [Google Scholar] [CrossRef]
- Croy, I.; Nordin, S.; Hummel, T. Olfactory Disorders and Quality of Life—An Updated Review. Chem. Senses 2014, 39, 185–194. [Google Scholar] [CrossRef]
- Boesveldt, S.; Postma, E.M.; Boak, D.; Welge-Luessen, A.; Schöpf, V.; Mainland, J.D.; Martens, J.; Ngai, J.; Duffy, V.B. Anosmia-A Clinical Review. Chem. Senses 2017, 42, 513–523. [Google Scholar] [CrossRef]
- Soudry, Y.; Lemogne, C.; Malinvaud, D.; Consoli, S.-M.; Bonfils, P. Olfactory System and Emotion: Common Substrates. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2011, 128, 18–23. [Google Scholar] [CrossRef]
- Croy, I.; Symmank, A.; Schellong, J.; Hummel, C.; Gerber, J.; Joraschky, P.; Hummel, T. Olfaction as a Marker for Depression in Humans. J. Affect. Disord. 2014, 160, 80–86. [Google Scholar] [CrossRef]
- Walliczek-Dworschak, U.; Gudziol, V.; Mitzschke, C.; Froehner, M.; Hummel, T. Testicular Cancer Patients Undergoing Cisplatin Based Chemotherapy Exhibit Temporary Olfactory Threshold Scores Changes. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 2813–2818. [Google Scholar] [CrossRef]
- Janelsins, M.C.; Kesler, S.R.; Ahles, T.A.; Morrow, G.R. Prevalence, Mechanisms, and Management of Cancer-Related Cognitive Impairment. Int. Rev. Psychiatry 2014, 26, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Schneider, J.A.; Arnold, S.E.; Tang, Y.; Boyle, P.A.; Bennett, D.A. Olfactory Identification and Incidence of Mild Cognitive Impairment in Older Age. Arch. Gen. Psychiatry 2007, 64, 802–808. [Google Scholar] [CrossRef]
- Invitto, S.; Piraino, G.; Ciccarese, V.; Carmillo, L.; Caggiula, M.; Trianni, G.; Nicolardi, G.; Di Nuovo, S.; Balconi, M. Potential Role of OERP as Early Marker of Mild Cognitive Impairment. Front. Aging Neurosci. 2018, 10, 272. [Google Scholar] [CrossRef]
- Invitto, S.; Calcagnì, A.; Piraino, G.; Ciccarese, V.; Balconi, M.; De Tommaso, M.; Toraldo, D.M. Obstructive Sleep Apnea Syndrome and Olfactory Perception: An OERP Study. Respir. Physiol. Neurobiol. 2019, 259, 37–44. [Google Scholar] [CrossRef]
- Eibenstein, A.; Fioretti, A.B.; Simaskou, M.N.; Sucapane, P.; Mearelli, S.; Mina, C.; Amabile, G.; Fusetti, M. Olfactory Screening Test in Mild Cognitive Impairment. Neurol. Sci. 2005, 26, 156–160. [Google Scholar] [CrossRef]
- Wang, Q.-S.; Tian, L.; Huang, Y.-L.; Qin, S.; He, L.-Q.; Zhou, J.-N. Olfactory Identification and Apolipoprotein E Ε4 Allele in Mild Cognitive Impairment. Brain Res. 2002, 951, 77–81. [Google Scholar] [CrossRef]
- Frasnelli, J.; Schuster, B.; Hummel, T. Interactions between Olfaction and the Trigeminal System: What Can Be Learned from Olfactory Loss. Cereb. Cortex 2007, 17, 2268–2275. [Google Scholar] [CrossRef]
- Lötsch, J.; Hähner, A.; Gossrau, G.; Hummel, C.; Walter, C.; Ultsch, A.; Hummel, T. Smell of Pain: Intersection of Nociception and Olfaction. PAIN 2016, 157, 2152–2157. [Google Scholar] [CrossRef]
- Gudziol, H.; Schubert, M.; Hummel, T. Decreased Trigeminal Sensitivity in Anosmia. ORL 2001, 63, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; MacFarlane, J.; MacDonald, M.; Thompson, J.; Dube, M.-P.; Mattice, M.; Fraser, R.; Young, C.; Hossain, S.; Pape, T.; et al. Loss-of-Function Mutations in the Nav1.7 Gene Underlie Congenital Indifference to Pain in Multiple Human Populations. Clin. Genet. 2007, 71, 311–319. [Google Scholar] [CrossRef]
- Zufall, F.; Pyrski, M.; Weiss, J.; Leinders-Zufall, T. Link between Pain and Olfaction in an Inherited Sodium Channelopathy. Arch. Neurol. 2012, 69, 1119–1123. [Google Scholar] [CrossRef][Green Version]
- Cicerchia, M.; Raffaele, M.; Pinna, G.; Repetto, L. Oncologia geriatrica. Riv. Ital. Della Med. Lab. 2011, 7, 122–126. [Google Scholar] [CrossRef]
- Basso, U.; Monfardini, S. Multidimensional Geriatric Evaluation in Elderly Cancer Patients: A Practical Approach. Eur. J. Cancer Care 2004, 13, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Brunello, A.; Sandri, R.; Extermann, M. Multidimensional Geriatric Evaluation for Older Cancer Patients as a Clinical and Research Tool. Cancer Treat. Rev. 2009, 35, 487–492. [Google Scholar] [CrossRef]
- Caro, M.M.M.; Laviano, A.; Pichard, C. Nutritional Intervention and Quality of Life in Adult Oncology Patients. Clin. Nutr. 2007, 26, 289–301. [Google Scholar] [CrossRef]
- Patino-Alonso, M.C.; Recio-Rodríguez, J.I.; Belio, J.F.M.; Colominas-Garrido, R.; Lema-Bartolomé, J.; Arranz, A.G.; Agudo-Conde, C.; Gomez-Marcos, M.A.; García-Ortiz, L. Factors Associated with Adherence to the Mediterranean Diet in the Adult Population. J. Acad. Nutr. Diet. 2014, 114, 583–589. [Google Scholar] [CrossRef]
- Frisoni, G.B.; Rozzini, R.; Bianchetti, A.; Trabucchi, M. Principal Lifetime Occupation and MMSE Score in Elderly Persons. J. Gerontol. 1993, 48, S310–S314. [Google Scholar] [CrossRef] [PubMed]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A Normative Study in Italian Elderly Population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Soubeyran, P.; Bellera, C.A.; Gregoire, F.; Blanc, J.; Ceccaldi, J.; Blanc-Bisson, C.; Mertens, C.; Mathoulin-Pélissier, S.; Fonck, M.; Rainfray, M. Validation of a Screening Test for Elderly Patients in Oncology. J. Clin. Oncol. 2008, 26, 20568. [Google Scholar] [CrossRef]
- Kenis, C.; Decoster, L.; Van Puyvelde, K.; De Grève, J.; Conings, G.; Milisen, K.; Flamaing, J.; Lobelle, J.-P.; Wildiers, H. Performance of Two Geriatric Screening Tools in Older Patients With Cancer. J. Clin. Oncol. 2014, 32, 19–26. [Google Scholar] [CrossRef]
- Hamaker, M.E.; Jonker, J.M.; de Rooij, S.E.; Vos, A.G.; Smorenburg, C.H.; van Munster, B.C. Frailty Screening Methods for Predicting Outcome of a Comprehensive Geriatric Assessment in Elderly Patients with Cancer: A Systematic Review. Lancet Oncol. 2012, 13, e437–e444. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Repetto, L.; Venturino, A.; Fratino, L.; Serraino, D.; Troisi, G.; Gianni, W.; Pietropaolo, M. Geriatric Oncology: A Clinical Approach to the Older Patient with Cancer. Eur. J. Cancer 2003, 39, 870–880. [Google Scholar] [CrossRef]
- Pal, S.K.; Katheria, V.; Hurria, A. Evaluating the Older Patient with Cancer: Understanding Frailty and the Geriatric Assessment. CA Cancer J. Clin. 2010, 60, 120–132. [Google Scholar] [CrossRef]
- Extermann, M. Integrating a Geriatric Evaluation in the Clinical Setting. Semin. Radiat. Oncol. 2012, 22, 272–276. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.G.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients with Cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef]
- Flannery, M.; Mohile, S.G.; Dale, W.; Arora, N.K.; Azar, L.; Breslau, E.S.; Cohen, H.J.; Dotan, E.; Eldadah, B.A.; Leach, C.R.; et al. Interventions to Improve the Quality of Life and Survivorship of Older Adults with Cancer: The Funding Landscape at NIH, ACS and PCORI. J. Geriatr. Oncol. 2016, 7, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Magnuson, A.; Allore, H.; Cohen, H.J.; Mohile, S.G.; Williams, G.R.; Chapman, A.; Extermann, M.; Olin, R.L.; Targia, V.; Mackenzie, A.; et al. Geriatric assessment with management in cancer care: Current evidence and potential mechanisms for future research. J. Geriatr. Oncol. 2016, 7, 242–248. [Google Scholar] [CrossRef]
- Steinbach, S.; Hummel, T.; Böhner, C.; Berktold, S.; Hundt, W.; Kriner, M.; Heinrich, P.; Sommer, H.; Hanusch, C.; Prechtl, A.; et al. Qualitative and Quantitative Assessment of Taste and Smell Changes in Patients Undergoing Chemotherapy for Breast Cancer or Gynecologic Malignancies. J. Clin. Oncol. 2009, 27, 1899–1905. [Google Scholar] [CrossRef]
- Amézaga, J.; Alfaro, B.; Ríos, Y.; Larraioz, A.; Ugartemendia, G.; Urruticoechea, A.; Tueros, I. Assessing Taste and Smell Alterations in Cancer Patients Undergoing Chemotherapy According to Treatment. Support. Care Cancer 2018, 26, 4077–4086. [Google Scholar] [CrossRef]
- Bernhardson, B.-M.; Tishelman, C.; Rutqvist, L.E. Olfactory Changes among Patients Receiving Chemotherapy. Eur. J. Oncol. Nurs. 2009, 13, 9–15. [Google Scholar] [CrossRef]
- Bernhardson, B.-M.; Tishelman, C.; Rutqvist, L.E. Chemosensory Changes Experienced by Patients Undergoing Cancer Chemotherapy: A Qualitative Interview Study. J. Pain Symptom Manag. 2007, 34, 403–412. [Google Scholar] [CrossRef]
- Bernhardson, B.-M.; Tishelman, C.; Rutqvist, L.E. Self-Reported Taste and Smell Changes during Cancer Chemotherapy. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2008, 16, 275–283. [Google Scholar] [CrossRef]
- Hutchinson, A.D.; Hosking, J.R.; Kichenadasse, G.; Mattiske, J.K.; Wilson, C. Objective and Subjective Cognitive Impairment Following Chemotherapy for Cancer: A Systematic Review. Cancer Treat. Rev. 2012, 38, 926–934. [Google Scholar] [CrossRef]
- Matthews, F.; Marioni, R.; Brayne, C. Medical Research Council Cognitive Function and Ageing Study Examining the Influence of Gender, Education, Social Class and Birth Cohort on MMSE Tracking over Time: A Population-Based Prospective Cohort Study. BMC Geriatr. 2012, 12, 45. [Google Scholar] [CrossRef]
- Rodrigues, M.A.P.; Facchini, L.A.; Thumé, E.; Maia, F. Gender and Incidence of Functional Disability in the Elderly: A Systematic Review. Cad. Saúde Pública 2009, 25, S464–S476. [Google Scholar] [CrossRef]
- Sentandreu-Mañó, T.; Badenes-Ribera, L.; Fernández, I.; Oliver, A.; Burks, D.J.; Tomás, J.M. Frailty in the Old Age as a Direct Marker of Quality of Life and Health: Gender Differences. Soc. Indic. Res. 2022, 160, 429–443. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cases | df | Approx. F | Trace Pillai | Num df | Den df | p |
|---|---|---|---|---|---|---|
| THERAPY | 2 | 1.108 | 0.061 | 8 | 280.000 | 0.358 |
| SEX | 1 | 5.172 | 0.130 | 4 | 139.000 | <0.001 |
| THERAPY ✻ SEX | 2 | 0.560 | 0.032 | 8 | 280.000 | 0.810 |
| Residuals | 142 |
| Cases | Sum of Squares | df | Mean Square | F | p | |
|---|---|---|---|---|---|---|
| MMSE | THERAPY | 22.509 | 2 | 11.255 | 1.257 | 0.288 |
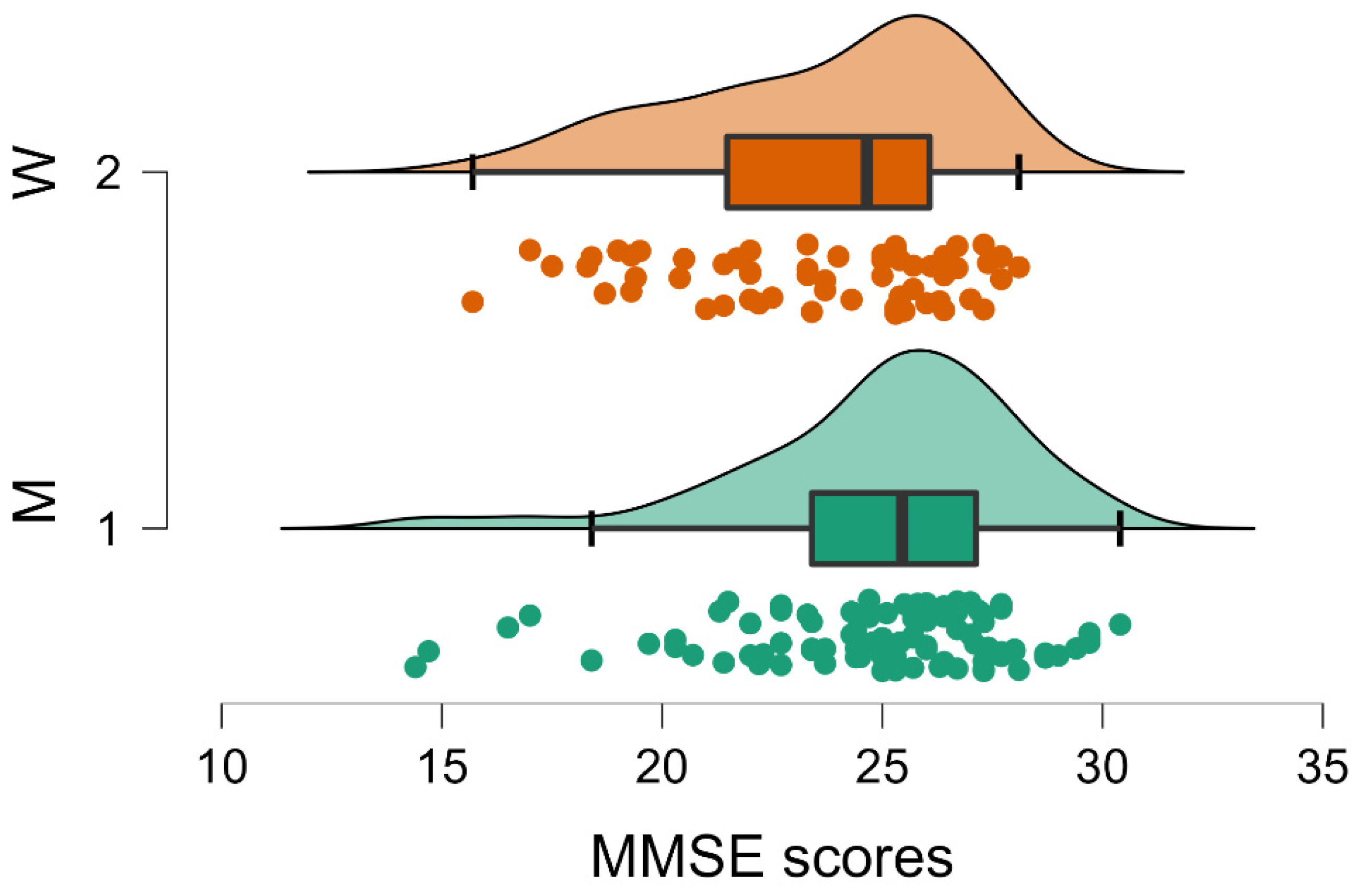
| SEX | 121.966 | 1 | 121.966 | 13.618 | <0.001 | |
| THERAPY ✻ SEX | 2.181 | 2 | 1.090 | 0.122 | 0.885 | |
| Residuals | 1271.776 | 142 | 8.956 | |||
| G8 | THERAPY | 1.569 | 2 | 0.784 | 0.163 | 0.850 |
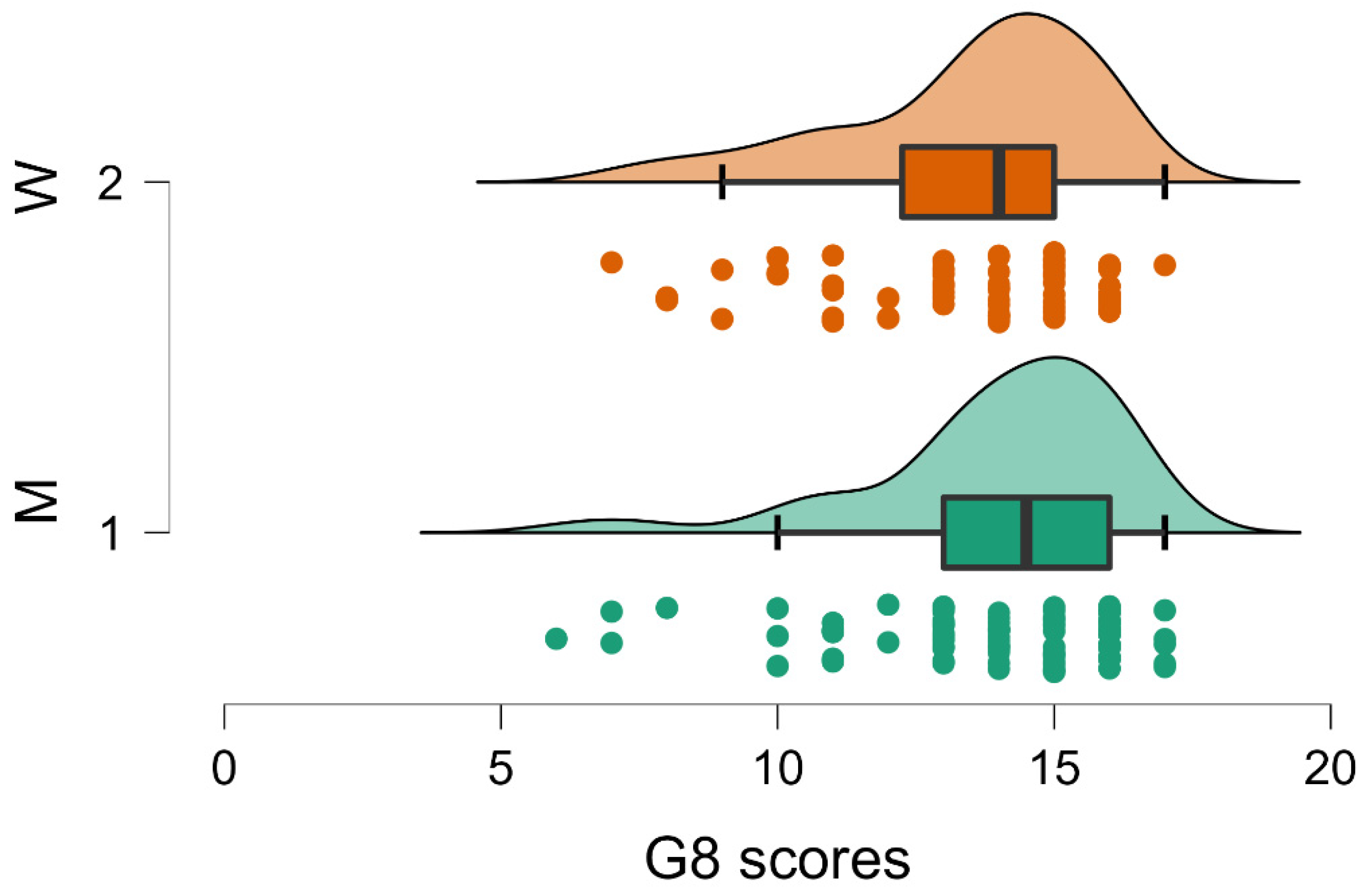
| SEX | 18.195 | 1 | 18.195 | 3.785 | 0.054 | |
| THERAPY ✻ SEX | 4.849 | 2 | 2.425 | 0.504 | 0.605 | |
| Residuals | 682.685 | 142 | 4.808 | |||
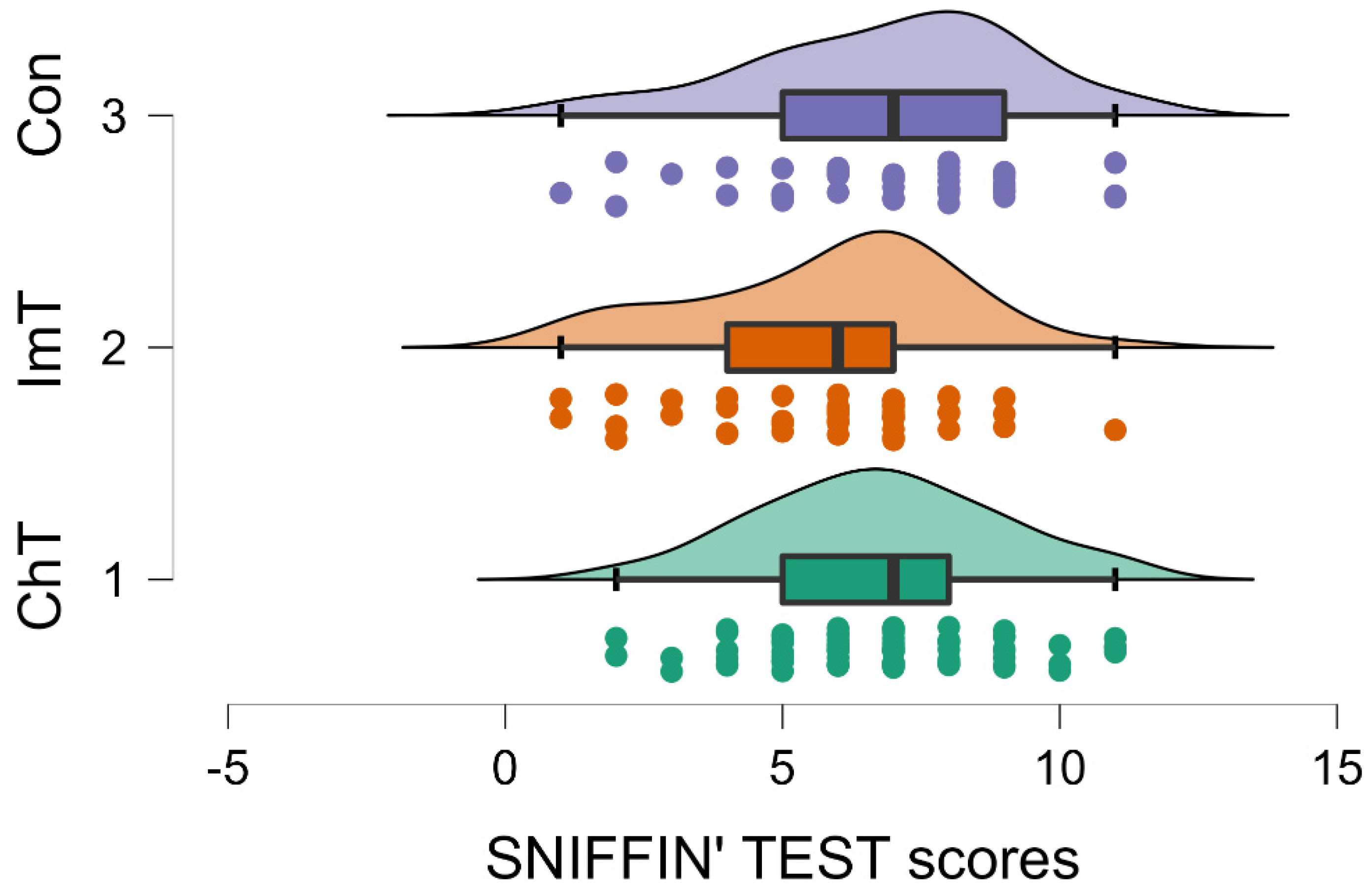
| Sniffin’ Sticks | THERAPY | 31.685 | 2 | 15.842 | 3.054 | 0.050 |
| SEX | 2.541 | 1 | 2.541 | 0.490 | 0.485 | |
| THERAPY ✻ SEX | 16.242 | 2 | 8.121 | 1.566 | 0.213 | |
| Residuals | 736.525 | 142 | 5.187 | |||
| Diet | THERAPY | 3.261 | 2 | 1.630 | 0.481 | 0.619 |
| SEX | 5.570 | 1 | 5.570 | 1.642 | 0.202 | |
| THERAPY ✻ SEX | 1.132 | 2 | 0.566 | 0.167 | 0.847 | |
| Residuals | 481.787 | 142 | 3.393 |
| MMSE | SNIFFIN’ TEST | G8 | DIET | |||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 1 | 2 | 1 | 2 | 1 | 2 | |
| Valid | 92 | 62 | 92 | 62 | 92 | 62 | 86 | 62 |
| Missing | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 0 |
| Mean | 24.963 | 23.587 | 6.315 | 6.774 | 14.011 | 13.452 | 7.884 | 7.565 |
| Std. Deviation | 3.154 | 3.151 | 2.223 | 2.432 | 2.265 | 2.317 | 1.704 | 1.989 |
| Minimum | 14.400 | 15.700 | 1.000 | 1.000 | 6.000 | 7.000 | 4.000 | 4.000 |
| Maximum | 30.400 | 28.100 | 11.000 | 11.000 | 17.000 | 17.000 | 13.000 | 15.000 |
| MMSE | SNIFFIN’ TEST | G8 | DIET | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | |
| Valid | 70 | 43 | 41 | 70 | 43 | 41 | 70 | 43 | 41 | 67 | 40 | 41 |
| Missing | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 3 | 0 |
| Mean | 24.276 | 23.942 | 25.127 | 6.729 | 5.791 | 6.854 | 13.843 | 13.767 | 13.707 | 7.746 | 7.550 | 7.951 |
| Std. Deviation | 3.253 | 3.375 | 2.918 | 2.153 | 2.356 | 2.424 | 2.124 | 2.213 | 2.686 | 1.726 | 1.632 | 2.167 |
| Minimum | 14.400 | 14.700 | 17.000 | 2.000 | 1.000 | 1.000 | 7.000 | 7.000 | 6.000 | 4.000 | 4.000 | 4.000 |
| Maximum | 29.700 | 30.400 | 29.700 | 11.000 | 11.000 | 11.000 | 17.000 | 16.000 | 17.000 | 13.000 | 10.000 | 15.000 |
| Variable | MMSE | SNIFFIN’ STICKS | G8 | |
|---|---|---|---|---|
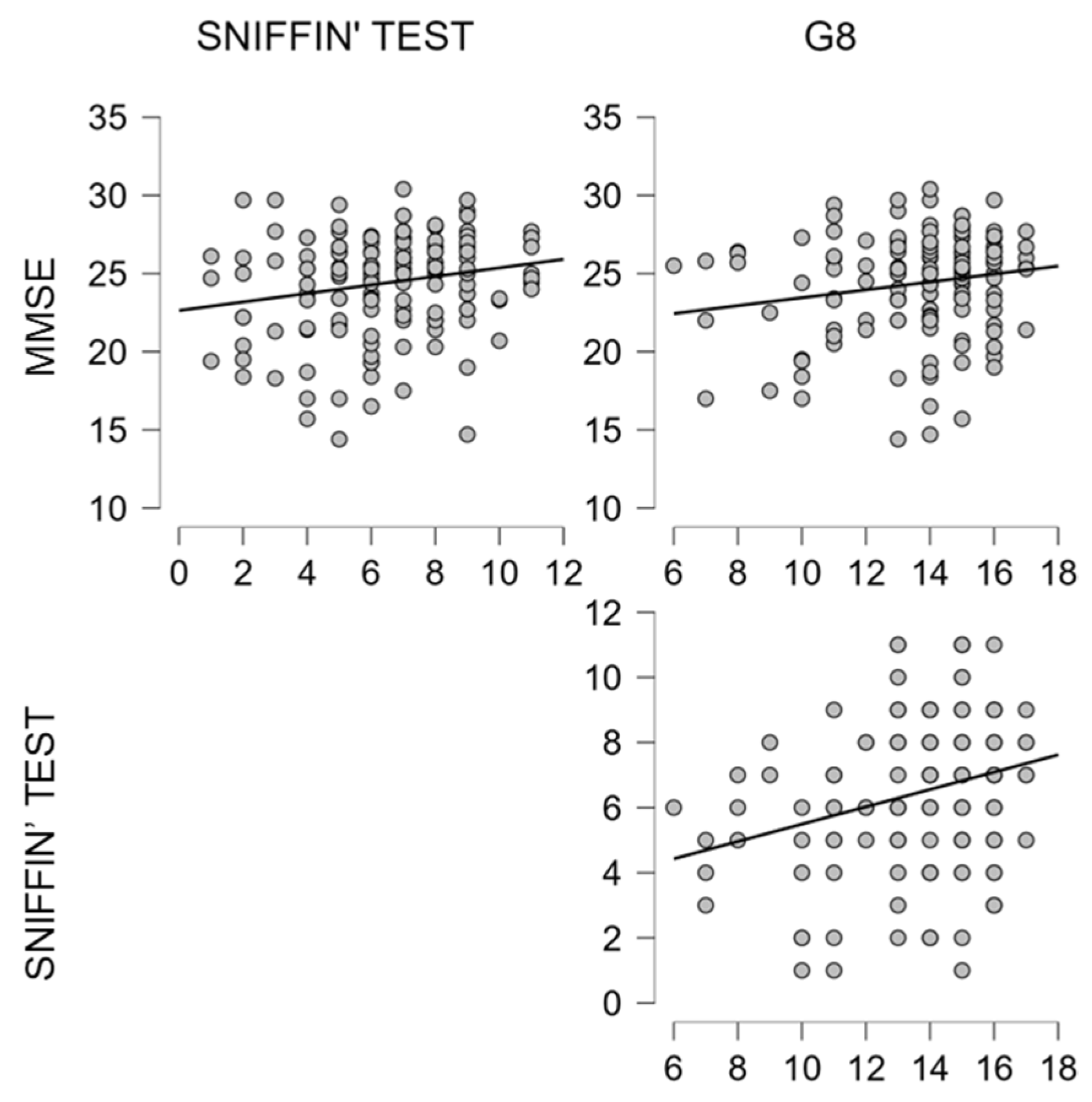
| MMSE | Pearson’s r p-value | – | ||
| SNIFFIN’ STICKS | Pearson’s r p-value | 0.226 ** 0.005 | – | |
| G8 | Pearson’s r p-value | 0.163 * 0.045 | 0.279 *** <0.001 | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Invitto, S.; Leucci, M.; Accogli, G.; Schito, A.; Nestola, C.; Ciccarese, V.; Rinaldi, R.; Boscolo Rizzo, P.; Spinato, G.; Leo, S. Chemobrain, Olfactory and Lifestyle Assessment in Onco-Geriatrics: Sex-Mediated Differences between Chemotherapy and Immunotherapy. Brain Sci. 2022, 12, 1390. https://doi.org/10.3390/brainsci12101390
Invitto S, Leucci M, Accogli G, Schito A, Nestola C, Ciccarese V, Rinaldi R, Boscolo Rizzo P, Spinato G, Leo S. Chemobrain, Olfactory and Lifestyle Assessment in Onco-Geriatrics: Sex-Mediated Differences between Chemotherapy and Immunotherapy. Brain Sciences. 2022; 12(10):1390. https://doi.org/10.3390/brainsci12101390
Chicago/Turabian StyleInvitto, Sara, Mariangela Leucci, Giuseppe Accogli, Andrea Schito, Claudia Nestola, Vincenzo Ciccarese, Ross Rinaldi, Paolo Boscolo Rizzo, Giacomo Spinato, and Silvana Leo. 2022. "Chemobrain, Olfactory and Lifestyle Assessment in Onco-Geriatrics: Sex-Mediated Differences between Chemotherapy and Immunotherapy" Brain Sciences 12, no. 10: 1390. https://doi.org/10.3390/brainsci12101390
APA StyleInvitto, S., Leucci, M., Accogli, G., Schito, A., Nestola, C., Ciccarese, V., Rinaldi, R., Boscolo Rizzo, P., Spinato, G., & Leo, S. (2022). Chemobrain, Olfactory and Lifestyle Assessment in Onco-Geriatrics: Sex-Mediated Differences between Chemotherapy and Immunotherapy. Brain Sciences, 12(10), 1390. https://doi.org/10.3390/brainsci12101390