
Is Hippocampal Resection Necessary for Low-Grade Epilepsy-Associated Tumors in the Temporal Lobe?

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Presurgical Evaluation
2.3. Surgical Resection
2.4. Postoperative Seizure Outcome
2.5. Antiseizure Medication (ASM) Reduction
2.6. Postoperative Cognitive Outcome
3. Results
3.1. Patient and Tumor Characteristics
3.2. Hippocampal Resection
3.3. Effects of Hippocampal Resection
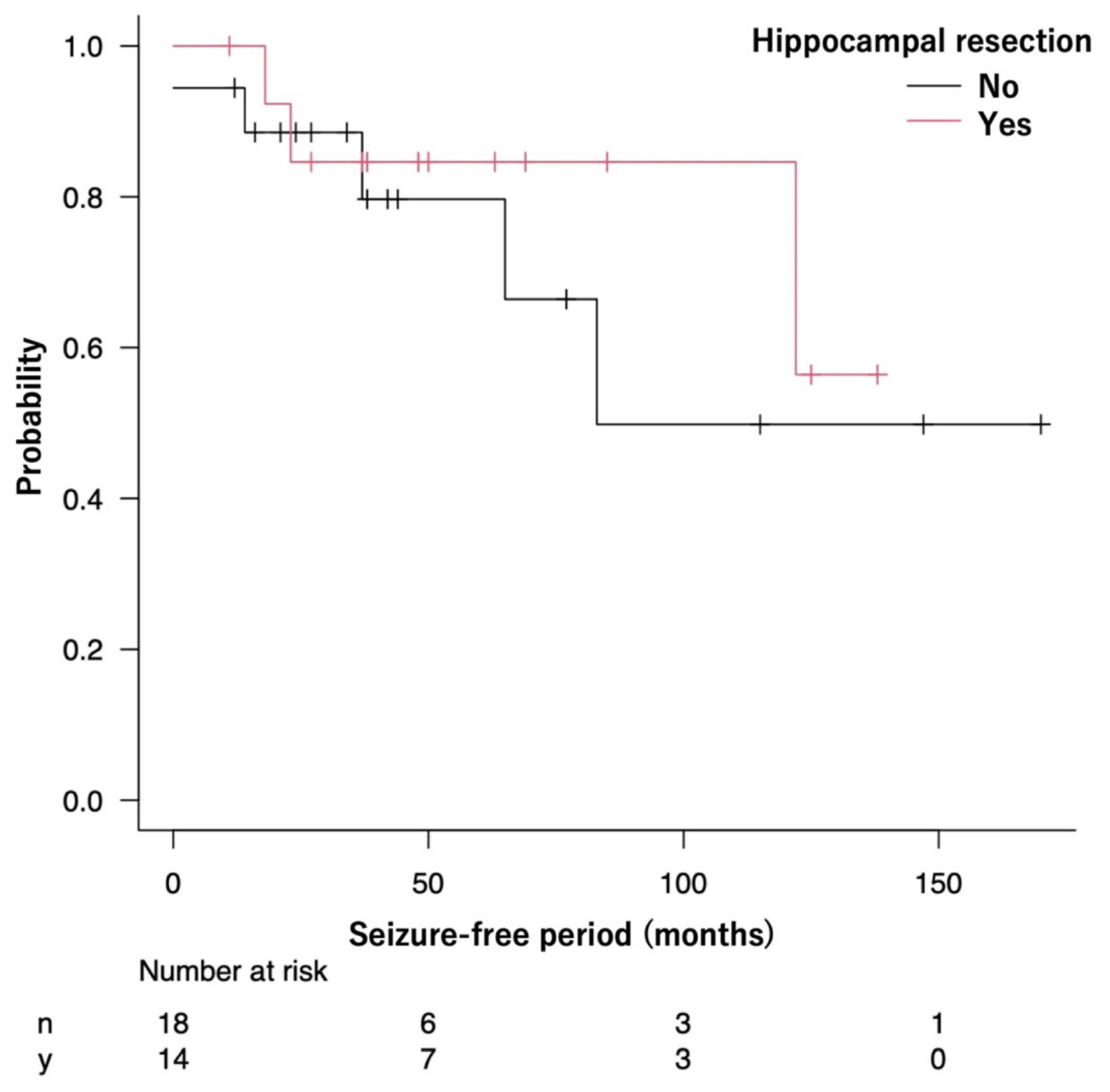
3.3.1. Seizure Outcome
3.3.2. ASM Reduction
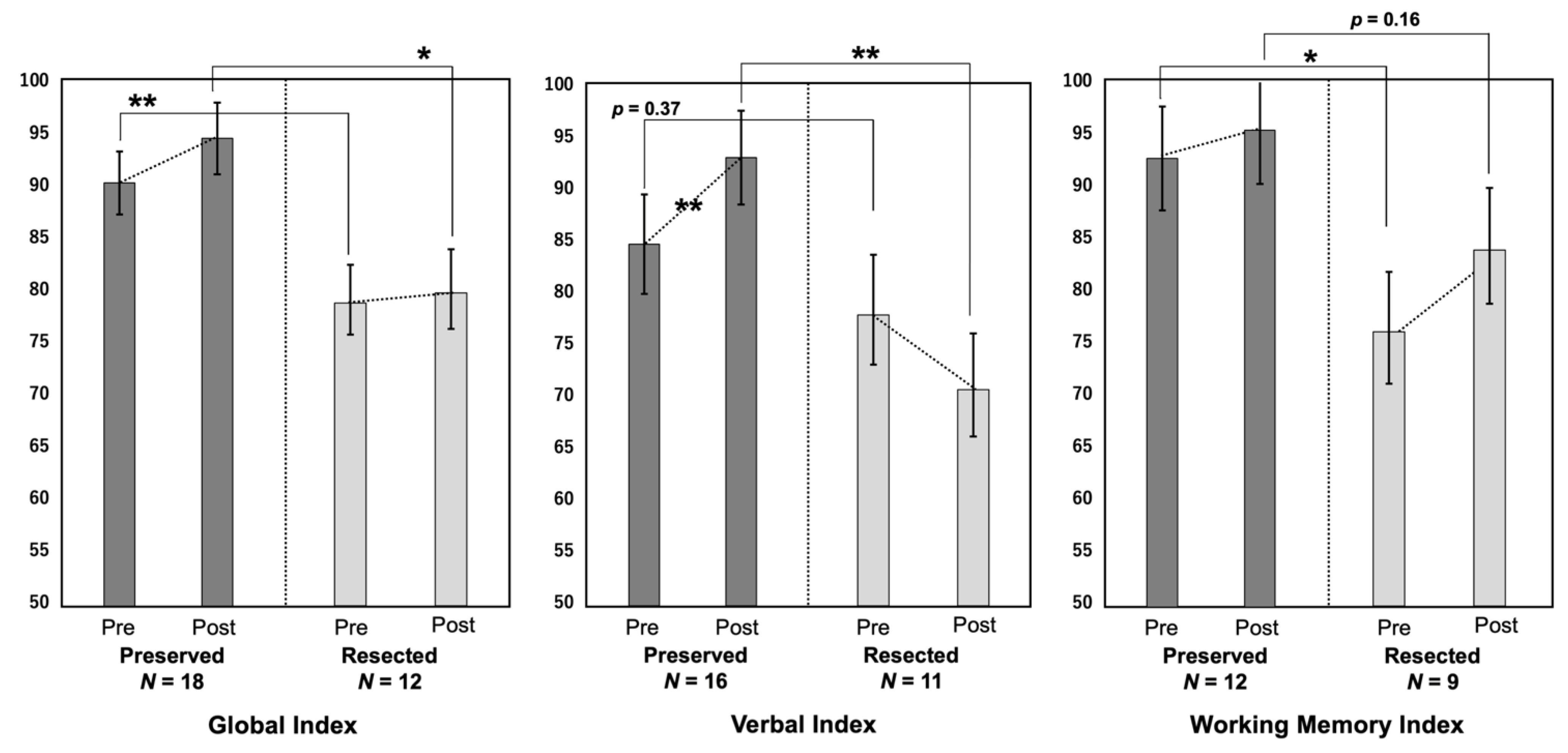
3.3.3. Cognitive Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pelliccia, V.; Deleo, F.; Gozzo, F.; Sartori, I.; Mai, R.; Cossu, M.; Tassi, L. Early and Late Epilepsy Surgery in Focal Epilepsies Associated With Long-Term Epilepsy-Associated Tumors. J. Neurosurg. 2017, 127, 1147–1152. [Google Scholar] [CrossRef]
- Kim, N.R.; Wang, K.C.; Bang, J.S.; Choe, G.; Park, Y.; Kim, S.K.; Cho, B.K.; Chi, J.G. Glioblastomatous Transformation of Ganglioglioma: Case Report With Reference to Molecular Genetic and Flow Cytometric Analysis. Pathol. Int. 2003, 53, 874–882. [Google Scholar] [CrossRef]
- Luyken, C.; Blümcke, I.; Fimmers, R.; Urbach, H.; Elger, C.E.; Wiestler, O.D.; Schramm, J. The Spectrum of Long-Term Epilepsy-Associated Tumors: Long-Term Seizure and Tumor Outcome and Neurosurgical Aspects. Epilepsia 2003, 44, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Englot, D.J.; Berger, M.S.; Barbaro, N.M.; Chang, E.F. Factors Associated With Seizure Freedom in the Surgical Resection of Glioneuronal Tumors. Epilepsia 2012, 53, 51–57. [Google Scholar] [CrossRef]
- Ravat, S.; Iyer, V.; Muzumdar, D.; Shah, U.; Pradhan, P.; Jain, N.; Godge, Y. Clinical Characteristics, Surgical and Neuropsychological Outcomes in Drug Resistant Tumoral Temporal Lobe Epilepsy. Int. J. Surg. 2016, 36, 436–442. [Google Scholar] [CrossRef]
- Vogt, V.L.; Witt, J.A.; Delev, D.; Grote, A.; von Lehe, M.; Becker, A.J.; Schramm, J.; Elger, C.E.; Helmstaedter, C. Cognitive Features and Surgical Outcome of Patients With Long-Term Epilepsy-Associated Tumors (LEATs) Within the Temporal Lobe. Epilepsy Behav. 2018, 88, 25–32. [Google Scholar] [CrossRef]
- Ghareeb, F.; Duffau, H. Intractable Epilepsy in Paralimbic Word Health Organization Grade II Gliomas: Should the Hippocampus Be Resected When Not Invaded by the Tumor? J. Neurosurg. 2012, 116, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Blümcke, I.; Aronica, E.; Urbach, H.; Alexopoulos, A.; Gonzalez-Martinez, J.A. A Neuropathology-Based Approach to Epilepsy Surgery in Brain Tumors and Proposal for a New Terminology Use for Long-Term Epilepsy-Associated Brain Tumors. Acta Neuropathol. 2014, 128, 39–54. [Google Scholar] [CrossRef] [PubMed]
- Wieser, H.G.; Blume, W.T.; Fish, D.; Goldensohn, E.; Hufnagel, A.; King, D.; Sperling, M.R.; Lüders, H.; Pedley, T.A. Commission on Neurosurgery of the International League Against Epilepsy (ILAE). ILAE Commission Report. Proposal for a New Classification of Outcome With Respect to Epileptic Seizures Following Epilepsy Surgery. Epilepsia 2001, 42, 282–286. [Google Scholar] [CrossRef]
- Suzuki, T. A Comparative Study of the Tanaka-Binet Intelligence Test and the Suzuki-Binet Intelligence Test. Jpn Assoc. Educ. Psychol. 1996, 38, 179. [Google Scholar] [CrossRef]
- Miyake, K.; Ohmura, M.; Takashima, M.; Yamanouchi, S.; Hashimoto, T.; Kobayashi, K. A New Test Developmental Screening Scale? Kinder Infant Development Scale? Hum. Dev. Res. 1990, 6, 147–163. [Google Scholar]
- Nakahara, J. Correlations of an Investigation Into the Development and the Level of Adaptability of Development With the Adaptability to Dental Treatment in Children Aged 3 Years. Jpn J. Pediatr. Dent. 2007, 45, 458–468. [Google Scholar] [CrossRef]
- Esteso Orduña, B.; de la Fournier del Castillo, M.C.; Cámara Barrio, S.; García Fernández, M.; Andrés Esteban, E.M.; Álvarez-Linera Prado, J.; Budke, M.; Maldonado Belmonte, M.J.; González Marqués, J.; Pérez Jiménez, M.Á. Cognitive and Behavioral Profiles of Pediatric Surgical Candidates With Frontal and Temporal Lobe Epilepsy. Epilepsy Behav. 2021, 117, 107808. [Google Scholar] [CrossRef]
- Ikegaya, N.; Iwasaki, M.; Kaneko, Y.; Kaido, T.; Kimura, Y.; Yamamoto, T.; Sumitomo, N.; Saito, T.; Nakagawa, E.; Sugai, K.; et al. Cognitive and Developmental Outcomes After Pediatric Insular Epilepsy Surgery for Focal Cortical Dysplasia. J. Neurosurg. Pediatr. 2020, 26, 543–551. [Google Scholar] [CrossRef]
- Fried, I.; Kim, J.H.; Spencer, D.D. Limbic and Neocortical Gliomas Associated With Intractable Seizures: A Distinct Clinicopathological Group. Neurosurgery. 1994, 34, 815–823. [Google Scholar] [CrossRef]
- Morris, H.H.; Matkovic, Z.; Estes, M.L.; Prayson, R.A.; Comair, Y.G.; Turnbull, J.; Najm, I.; Kotagal, P.; Wyllie, E. Ganglioglioma and Intractable Epilepsy: Clinical and Neurophysiologic Features and Predictors of Outcome After Surgery. Epilepsia. 1998, 39, 307–313. [Google Scholar] [CrossRef]
- Cataltepe, O.; Turanli, G.; Yalnizoglu, D.; Topçu, M.; Akalan, N. Surgical Management of Temporal Lobe Tumor-Related Epilepsy in Children. J. Neurosurg. 2005, 102 (Suppl. 3), 280–287. [Google Scholar] [CrossRef]
- Mintzer, S.; Sperling, M.R. When Should a Resection Sparing Mesial Structures Be Considered for Temporal Lobe Epilepsy? Epilepsy Behav. 2008, 13, 7–11. [Google Scholar] [CrossRef]
- Morioka, T.; Hashiguchi, K.; Nagata, S.; Miyagi, Y.; Yoshida, F.; Shono, T.; Mihara, F.; Koga, H.; Sasaki, T. Additional Hippocampectomy in the Surgical Management of Intractable Temporal Lobe Epilepsy Associated With Glioneuronal Tumor. Neurol. Res. 2007, 29, 807–815. [Google Scholar] [CrossRef]
- Yu, H.Y.; Lin, C.F.; Chou, C.C.; Lu, Y.J.; Hsu, S.P.C.; Lee, C.C.; Chen, C. Outcomes of Hippocampus-Sparing Lesionectomy for Temporal Lobe Epilepsy and the Significance of Intraoperative Hippocampography. Clin. Neurophysiol. 2021, 132, 746–755. [Google Scholar] [CrossRef]
- Varotto, G.; Burini, A.; Didato, G.; Deleo, F.; Pastori, C.; Dominese, A.; Tringali, G.; Panzica, F.; de Curtis, M.; Di Giacomo, R. Impaired Awareness in Mesial Temporal Lobe Epilepsy: Network Analysis of Foramen Ovale and Scalp EEG. Clin. Neurophysiol. 2021, 132, 3084–3094. [Google Scholar] [CrossRef] [PubMed]
- Sugano, H.; Shimizu, H.; Sunaga, S. Efficacy of Intraoperative Electrocorticography for Assessing Seizure Outcomes in Intractable Epilepsy Patients With Temporal-Lobe-Mass Lesions. Seizure 2007, 16, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Kashida, Y.; Usui, N.; Matsuda, K.; Terada, K.; Baba, K.; Kondo, A.; Hirozawa, D.; Tottori, T.; Mihara, T.; Hanaya, R.; et al. Is Additional Mesial Temporal Resection Necessary for Intractable Epilepsy With Cavernous Malformations in the Temporal Neocortex? Epilepsy Behav. 2019, 92, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Wagner, K.; Uherek, M.; Horstmann, S.; Kadish, N.E.; Wisniewski, I.; Mayer, H.; Buschmann, F.; Metternich, B.; Zentner, J.; Schulze-Bonhage, A. Memory Outcome After Hippocampus Sparing Resections in the Temporal Lobe. J. Neurol. Neurosurg. Psychiatry. 2013, 84, 630–636. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients without Hippocampal Resection | ||||||||
|---|---|---|---|---|---|---|---|---|
| Case No. | Sex | Age (Years) at Epilepsy Onset (Mean: 10.2) | Age (Years) at Surgery (Mean: 21.6) | Follow-Up Period (Months) | Side of Surgery | Handedness | Seizure Classification | Seizure Frequency |
| 1 | M | 14 | 22 | 92 | L | R | FIAS | Monthly |
| 2 | M | 6 | 26 | 34 | L | R | FIAS > FBTCS | rare |
| 3 | F | 17 | 55 | 38 | L | R (corrected) | FIAS | Monthly |
| 4 | M | 9 | 31 | 16 | L | R | FIAS | Weekly |
| 5 | M | 15 | 30 | 170 | L | R | FIAS | Monthly |
| 6 | M | 13 | 22 | 147 | L | R | FIAS | Monthly |
| 7 | M | 17 | 27 | 77 | L | R | FIAS | rare |
| 8 | M | 0 | 0.7 | 115 | L | Unknown | FIAS | Weekly |
| 9 | M | 12 | 13 | 12 | L | L | FIAS | Monthly |
| 10 | F | 18 | 32 | 30 | L | R | FIAS | Weekly |
| 11 | M | 4 | 27 | 27 | R | R | FIAS | Weekly |
| 12 | F | 15 | 17 | 24 | R | R | FIAS | Weekly |
| 13 | F | 9 | 15 | 64 | R | R | FIAS | Monthly |
| 14 | F | 13 | 14 | 21 | R | R | FIAS | Weekly |
| 15 | M | 10 | 23 | 16 | R | R | FIAS | Weekly |
| 16 | M | 8 | 29 | 44 | R | R | FIAS | Weekly |
| 17 | M | 0 | 1 | 160 | R | Unknown | FIAS | Weekly |
| 18 | F | 3 | 4 | 42 | R | R | FIAS | rare |
| Patients with hippocampal resection | ||||||||
| Case No. | Sex | Age (Years) at Epilepsy Onset (Mean: 5.4) | Age (Years) at Surgery (Mean: 14.6) | Follow-Up Period (Months) | Side of Surgery | Handedness | Seizure Classification | Seizure Frequency |
| 19 | F | 1 | 8 | 69 | L | R | FIAS | Monthly |
| 20 | F | 14 | 15 | 156 | L | L | FIAS | Monthly |
| 21 | M | 8 | 25 | 85 | L | L | FIAS | Weekly |
| 22 | M | 13 | 18 | 38 | L | R | FIAS > FBTCS | rare |
| 23 | F | 0 | 13 | 138 | L | R | FIAS | Daily |
| 24 | M | 10 | 10.8 | 127 | L | R | FIAS | Weekly |
| 25 | M | 0 | 0.5 | 125 | L | Unknown | FIAS | Weekly |
| 26 | M | 8 | 42 | 63 | L | Ambiguous | FIAS | Monthly |
| 27 | F | 4 | 7 | 37 | L | R | FIAS | Weekly |
| 28 | F | 3 | 6 | 50 | L | R | FIAS | Weekly |
| 29 | F | 0 | 9 | 59 | R | R | FIAS + visual aura | Daily |
| 30 | F | 1 | 1.8 | 27 | R | Unknown | spasm | Daily |
| 31 | M | 8 | 11 | 48 | R | R | FIAS | Weekly |
| 32 | M | 6 | 38 | 11 | R | R | FIAS | Monthly |
| Patients without Hippocampal Resection | ||||||
|---|---|---|---|---|---|---|
| Case No. | Rationale of Hippocampal Preservation | Histology | ILAE Class | Follow-Up Duration (Months) | Number of Preoperative ASMs | Number of Postoperative ASMs |
| 1 | Unidentified | GNT/astrocytoma | 3 | 92 | 3 | 3 |
| 2 | Distant from hippocampus | GNT | 1a | 34 | 2 | 2 |
| 3 | Distant from hippocampus | FCD + LGG | 1a | 38 | 3 | 2 |
| 4 | Distant from hippocampus | LGG | 3 | 16 | 6 | 5 |
| 5 | Unidentified | DNT | 1a | 170 | 2 | 0 |
| 6 | Distant from hippocampus | GG | 1a | 147 | 2 | 2 |
| 7 | No preoperative cognitive decline | GG | 1a | 77 | 2 | 2 |
| 8 | Unidentified | GG | 1a | 115 | 1 | 0 |
| 9 | Distant from hippocampus | LGG | 1a | 12 | 1 | 1 |
| 10 | Distant from hippocampus | PXA | 1 | 30 | 1 | 1 |
| 11 | Distant from hippocampus | GG | 1a | 27 | 3 | 1 |
| 12 | Distant from hippocampus | GG | 1a | 24 | 2 | 2 |
| 13 | Distant from hippocampus | GG | 1 | 64 | 1 | 0 |
| 14 | No preoperative cognitive decline | LGG | 1a | 21 | 1 | 0 |
| 15 | No preoperative cognitive decline | GG | 1a | 16 | 2 | 2 |
| 16 | Intraoperative ECoG findings | GG | 1a | 44 | 2 | 0 |
| 17 | Unidentified | LGG | 1 | 160 | 1 | 1 |
| 18 | Distant from hippocampus | astrocytoma | 1a | 42 | 1 | 1 |
| Patients with Hippocampal Resection | ||||||
| Case No. | Histology | ILAE Class | Follow-Up Duration (Months) | Number of Preoperative ASMs | Number of Postoperative ASMs | |
| 19 | LGG | 1a | 69 | 1 | 1 | |
| 20 | LGG | 4 | 156 | 1 | 1 | |
| 21 | LGG | 1a | 85 | 1 | 1 | |
| 22 | LGG | 1a | 38 | 1 | 1 | |
| 23 | GG | 1a | 138 | 3 | 1 | |
| 24 | GG | 5 | 127 | 2 | 3 | |
| 25 | GG | 1a | 125 | 2 | 1 | |
| 26 | GG | 1a | 63 | 2 | 2 | |
| 27 | FCD + LGG | 1a | 37 | 2 | 1 | |
| 28 | GG | 1a | 50 | 2 | 1 | |
| 29 | GG | 1 | 59 | 3 | 1 | |
| 30 | astrocytoma | 1a | 27 | 1 | 0 | |
| 31 | GG | 1a | 48 | 1 | 1 | |
| 32 | LGG | 1a | 11 | 1 | 1 | |
| Preoperative Score (Mean ± SE) | Postoperative Score (Mean ± SE) | |||||
|---|---|---|---|---|---|---|
| GI | VI | WMI | GI | VI | WMI | |
| Overall (n = 32) | 85.7 ± 2.5 | 81.9 ± 3.7 | 85.6 ± 4.0 | 88.7 ± 2.9 | 83.9 ±4.0 | 90.5 ± 3.9 |
| Preserved group (n = 18) | 90.3 ± 3.0 | 84.7 ± 4.8 | 92.8 ± 4.9 | 94.6 ± 3.4 | 93.0 ± 4.5 | 95.4 ± 5.1 |
| Resected group (n = 14) | 76.8 ± 3.7 | 77.9 ± 5.8 | 76.1 ± 5.7 | 79.8 ± 4.2 | 70.7 ± 5.4 | 83.9 ± 5.9 |
| Estimate | Standard Error | F Value | T Value | p Value | ||
|---|---|---|---|---|---|---|
| GI | Intercept | 22.22 | 13.87 | 1.60 | 0.12 | |
| (n = 30) | Pre-GI | 0.77 | 0.16 | 22.41 | 4.73 | <0.0001 |
| HR | 2.97 | 2.23 | 1.76 | 1.33 | 0.20 | |
| VI | Intercept | 36.15 | 12.83 | 2.82 | 0.01 | |
| (n = 27) | Pre-VI | 0.56 | 0.15 | 13.37 | 3.66 | 0.001 |
| HR | 9.23 | 2.92 | 9.98 | 3.16 | 0.004 | |
| WMI | Intercept | 27.92 | 14.82 | 1.88 | 0.08 | |
| (n = 21) | Pre-WMI | 0.73 | 0.17 | 18.01 | 4.24 | <0.001 |
| HR | −0.32 | 3.18 | 0.01 | −0.10 | 0.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takayama, Y.; Ikegaya, N.; Iijima, K.; Kimura, Y.; Kosugi, K.; Yokosako, S.; Kaneko, Y.; Yamamoto, T.; Iwasaki, M. Is Hippocampal Resection Necessary for Low-Grade Epilepsy-Associated Tumors in the Temporal Lobe? Brain Sci. 2022, 12, 1381. https://doi.org/10.3390/brainsci12101381
Takayama Y, Ikegaya N, Iijima K, Kimura Y, Kosugi K, Yokosako S, Kaneko Y, Yamamoto T, Iwasaki M. Is Hippocampal Resection Necessary for Low-Grade Epilepsy-Associated Tumors in the Temporal Lobe? Brain Sciences. 2022; 12(10):1381. https://doi.org/10.3390/brainsci12101381
Chicago/Turabian StyleTakayama, Yutaro, Naoki Ikegaya, Keiya Iijima, Yuiko Kimura, Kenzo Kosugi, Suguru Yokosako, Yuu Kaneko, Tetsuya Yamamoto, and Masaki Iwasaki. 2022. "Is Hippocampal Resection Necessary for Low-Grade Epilepsy-Associated Tumors in the Temporal Lobe?" Brain Sciences 12, no. 10: 1381. https://doi.org/10.3390/brainsci12101381
APA StyleTakayama, Y., Ikegaya, N., Iijima, K., Kimura, Y., Kosugi, K., Yokosako, S., Kaneko, Y., Yamamoto, T., & Iwasaki, M. (2022). Is Hippocampal Resection Necessary for Low-Grade Epilepsy-Associated Tumors in the Temporal Lobe? Brain Sciences, 12(10), 1381. https://doi.org/10.3390/brainsci12101381