Autonomic Changes in Juvenile-Onset Huntington’s Disease


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Statistical Analyses
3. Results
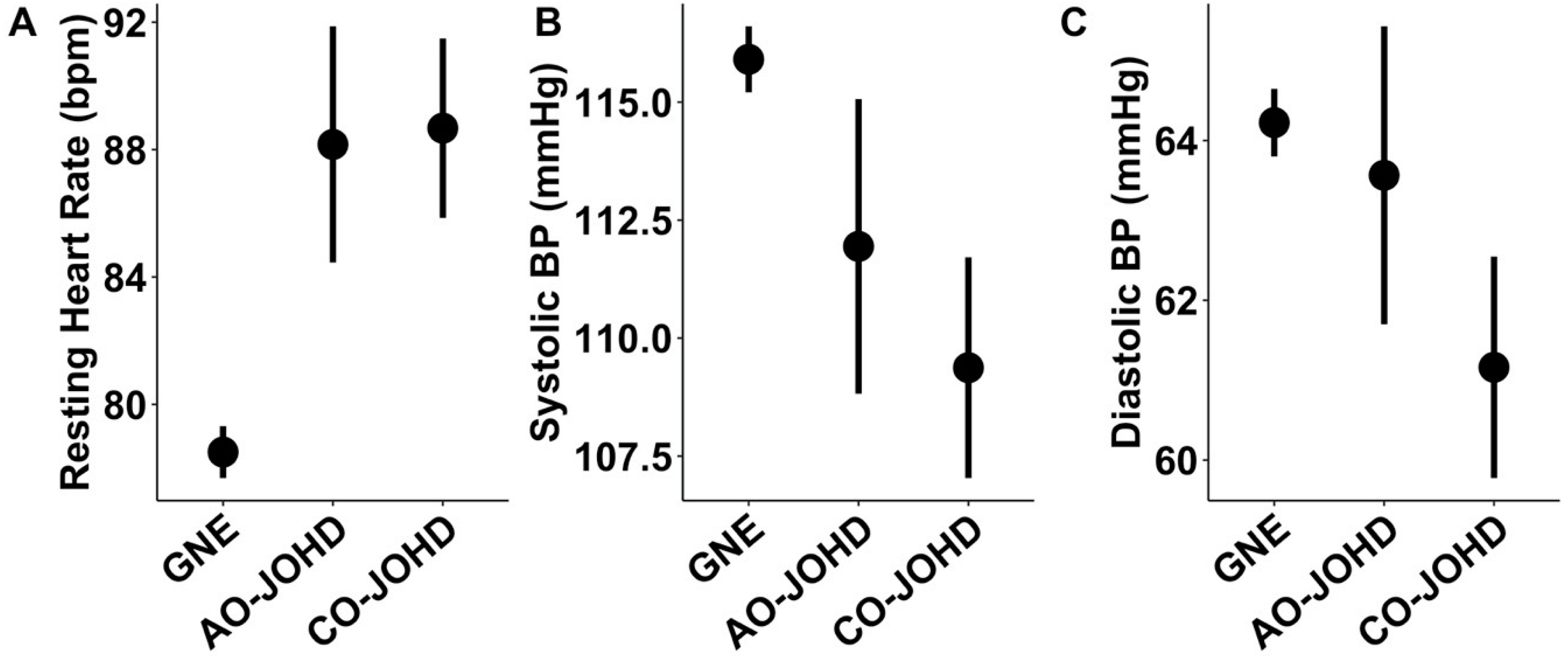
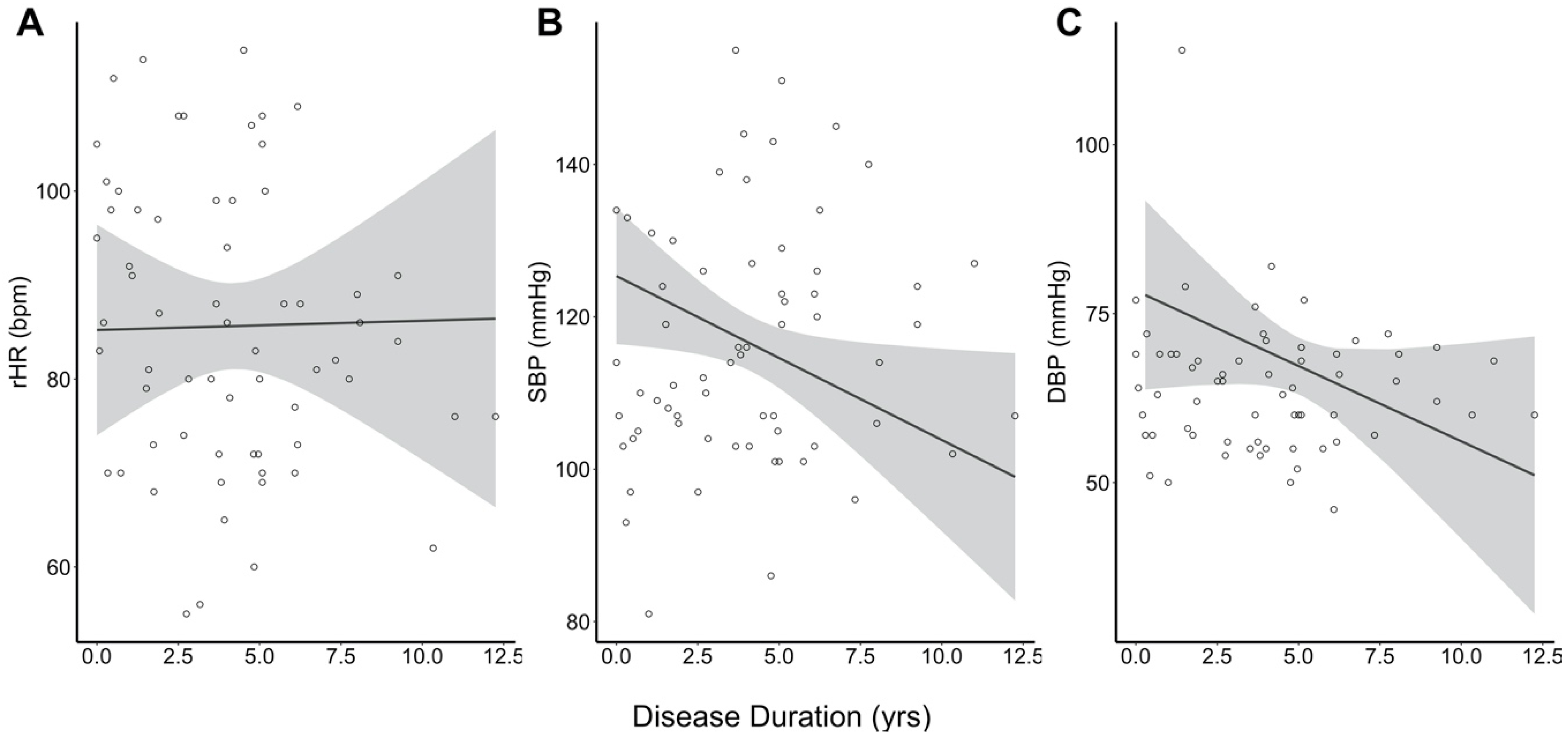
Primary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- MacDonald, M.E.; Ambrose, C.M.; Duyao, M.P.; Myers, R.H.; Lin, C.; Srinidhi, L.; Barnes, G.; Taylor, S.A.; James, M.; Groot, N.; et al. A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. The Huntington’s Disease Collaborative Research Group. Cell 1993, 72, 971–983. [Google Scholar] [CrossRef]
- Tabrizi, S.J.; Scahill, R.I.; Owen, G.; Durr, A.; Leavitt, B.R.; Roos, R.A.; Borowsky, B.; Landwehrmeyer, B.; Frost, C.; Johnson, H.; et al. Predictors of phenotypic progression and disease onset in premanifest and early-stage Huntington’s disease in the TRACK-HD study: Analysis of 36-month observational data. Lancet Neurol. 2013, 12, 637–649. [Google Scholar] [CrossRef]
- Paulsen, J.S.; Long, J.D.; Ross, C.A.; Harrington, D.L.; Erwin, C.J.; Williams, J.K.; Westervelt, H.J.; Johnson, H.J.; Aylward, E.H.; Zhang, Y.; et al. Prediction of manifest Huntington’s disease with clinical and imaging measures: A prospective observational study. Lancet Neurol. 2014, 13, 1193–1201. [Google Scholar] [CrossRef]
- Andrich, J.; Schmitz, T.; Saft, C.; Postert, T.; Kraus, P.; Epplen, J.T.; Przuntek, H.; Agelink, M.W. Autonomic nervous system function in Huntington’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 72, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Den Heijer, J.C.; Bollen, W.L.; Reulen, J.P.; van Dijk, J.G.; Kramer, C.G.; Roos, R.A.; Buruma, O.J. Autonomic nervous function in Huntington’s disease. Arch. Neurol. 1988, 45, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Kobal, J.; Meglic, B.; Mesec, A.; Peterlin, B. Early sympathetic hyperactivity in Huntington’s disease. Eur. J. Neurol. 2004, 11, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Kobal, J.; Melik, Z.; Cankar, K.; Bajrovic, F.F.; Meglic, B.; Peterlin, B.; Zaletel, M. Autonomic dysfunction in presymptomatic and early symptomatic Huntington’s disease. Acta Neurol. Scand. 2010, 121, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Kobal, J.; Melik, Z.; Cankar, K.; Strucl, M. Cognitive and autonomic dysfunction in presymptomatic and early Huntington’s disease. J. Neurol. 2014, 261, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Mielcarek, M.; Inuabasi, L.; Bondulich, M.K.; Muller, T.; Osborne, G.F.; Franklin, S.A.; Smith, D.L.; Neueder, A.; Rosinski, J.; Rattray, I.; et al. Dysfunction of the CNS-heart axis in mouse models of Huntington’s disease. PLoS Genet. 2014, 10, e1004550. [Google Scholar] [CrossRef]
- Critchley, B.J.; Isalan, M.; Mielcarek, M. Neuro-Cardio Mechanisms in Huntington’s Disease and Other Neurodegenerative Disorders. Front. Physiol. 2018, 9, 559. [Google Scholar] [CrossRef] [PubMed]
- Moser, A.D.; Epping, E.; Espe-Pfeifer, P.; Martin, E.; Zhorne, L.; Mathews, K.; Nance, M.; Hudgell, D.; Quarrell, O.; Nopoulos, P. A survey-based study identifies common but unrecognized symptoms in a large series of juvenile Huntington’s disease. Neurodegener Dis. Manag. 2017, 7, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Tereshchenko, A.; McHugh, M.; Lee, J.K.; Gonzalez-Alegre, P.; Crane, K.; Dawson, J.; Nopoulos, P. Abnormal Weight and Body Mass Index in Children with Juvenile Huntington’s Disease. J. Huntingt. Dis. 2015, 4, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Tereshchenko, A.; Magnotta, V.; Epping, E.; Mathews, K.; Espe-Pfeifer, P.; Martin, E.; Dawson, J.; Duan, W.; Nopoulos, P. Brain structure in juvenile-onset Huntington disease. Neurology 2019, 92, e1939–e1947. [Google Scholar] [CrossRef] [PubMed]
- van der Plas, E.; Langbehn, D.R.; Conrad, A.L.; Koscik, T.R.; Tereshchenko, A.; Epping, E.A.; Magnotta, V.A.; Nopoulos, P.C. Abnormal brain development in child and adolescent carriers of mutant huntingtin. Neurology 2019, 93, e1021–e1030. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.B.; Bates, G.P.; Steffan, J.; Saft, C.; Tabrizi, S.J. Treating the whole body in Huntington’s disease. Lancet Neurol. 2015, 14, 1135–1142. [Google Scholar] [CrossRef]
- Colombari, E.; Sato, M.A.; Cravo, S.L.; Bergamaschi, C.T.; Campos, R.R., Jr.; Lopes, O.U. Role of the medulla oblongata in hypertension. Hypertension 2001, 38, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Rub, U.; Hentschel, M.; Stratmann, K.; Brunt, E.; Heinsen, H.; Seidel, K.; Bouzrou, M.; Auburger, G.; Paulson, H.; Vonsattel, J.P.; et al. Huntington’s disease (HD): Degeneration of select nuclei, widespread occurrence of neuronal nuclear and axonal inclusions in the brainstem. Brain Pathol. 2014, 24, 247–260. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| JOHD Group | Controls | p-Value | |
|---|---|---|---|
| N (Visits) | 27 (64) | 259 (395) | NA |
| Female, % (n) | 55.6 (15) | 53.5 (138) | 0.998 |
| Age (years), Mean ± SD | 15.89 ± 6.06 | 12.34 ± 3.76 | <0.001 |
| CAG Repeats, Mean ± SD | 72.19 ± 14.18 | 20.29 ± 3.91 | <0.001 |
| Parental SES, % (n) | 0.356 | ||
| 1 | 0.0 (0) | 0.8 (2) | |
| 2 | 48.0 (12) | 58.0 (149) | |
| 3 | 40.0 (10) | 37.4 (96) | |
| 4 | 8.0 (2) | 3.1 (8) | |
| 5 | 4.0 (1) | 0.8 (2) | |
| Missing | N = 2 | N = 2 | |
| BP Increasing Meds, % (n) | 11.1 (3) | 2.7 (7) | 0.087 |
| BP Decreasing Meds, % (n) | 14.8 (4) | 1.2 (3) | <0.001 |
| Disease Duration (years), | 3.38 ± 3.04 | NA | NA |
| Mean ± SD |
| JOHD Group | Controls | p-Value | |
|---|---|---|---|
| rHR, Mean ± SE | 88.56 ± 2.36 | 78.50 ± 0.83 | <0.0001 |
| SBP, Mean ± SE | 109.96 ± 1.99 | 115.99 ± 0.71 | 0.0053 |
| DBP, Mean ± SE | 61.88 ± 1.17 | 64.25 ± 0.42 | 0.060 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schultz, J.L.; Nopoulos, P.C. Autonomic Changes in Juvenile-Onset Huntington’s Disease. Brain Sci. 2020, 10, 589. https://doi.org/10.3390/brainsci10090589
Schultz JL, Nopoulos PC. Autonomic Changes in Juvenile-Onset Huntington’s Disease. Brain Sciences. 2020; 10(9):589. https://doi.org/10.3390/brainsci10090589
Chicago/Turabian StyleSchultz, Jordan L., and Peg C. Nopoulos. 2020. "Autonomic Changes in Juvenile-Onset Huntington’s Disease" Brain Sciences 10, no. 9: 589. https://doi.org/10.3390/brainsci10090589
APA StyleSchultz, J. L., & Nopoulos, P. C. (2020). Autonomic Changes in Juvenile-Onset Huntington’s Disease. Brain Sciences, 10(9), 589. https://doi.org/10.3390/brainsci10090589