Fatigue in Cancer and Neuroinflammatory and Autoimmune Disease: CNS Arousal Matters

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Questionnaires
2.3. EEG Recording and Preprocessing
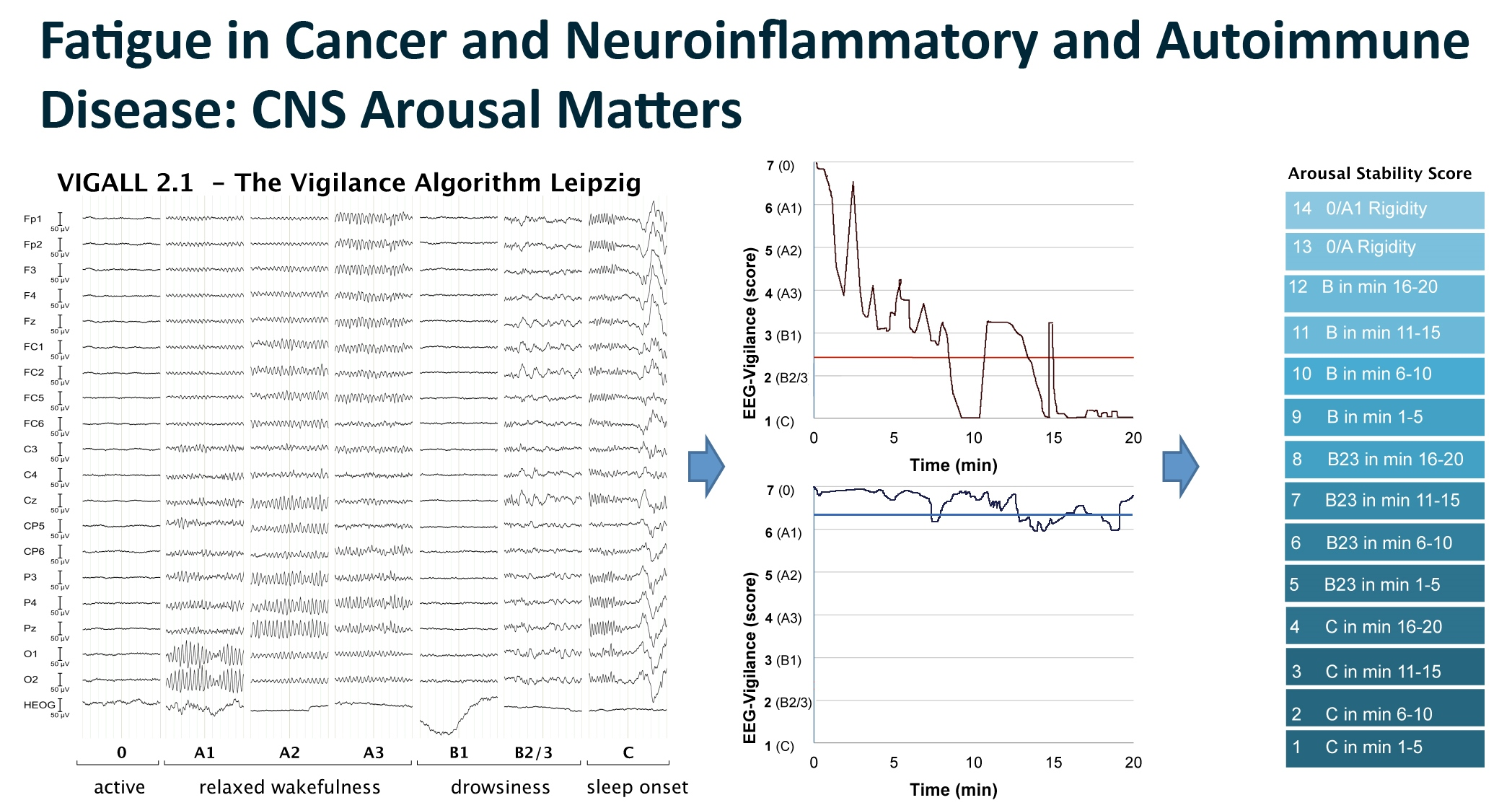
2.4. EEG-Vigilance Staging and Parameterization
2.5. Statistical Analyses
3. Results
3.1. Descriptive Analyses
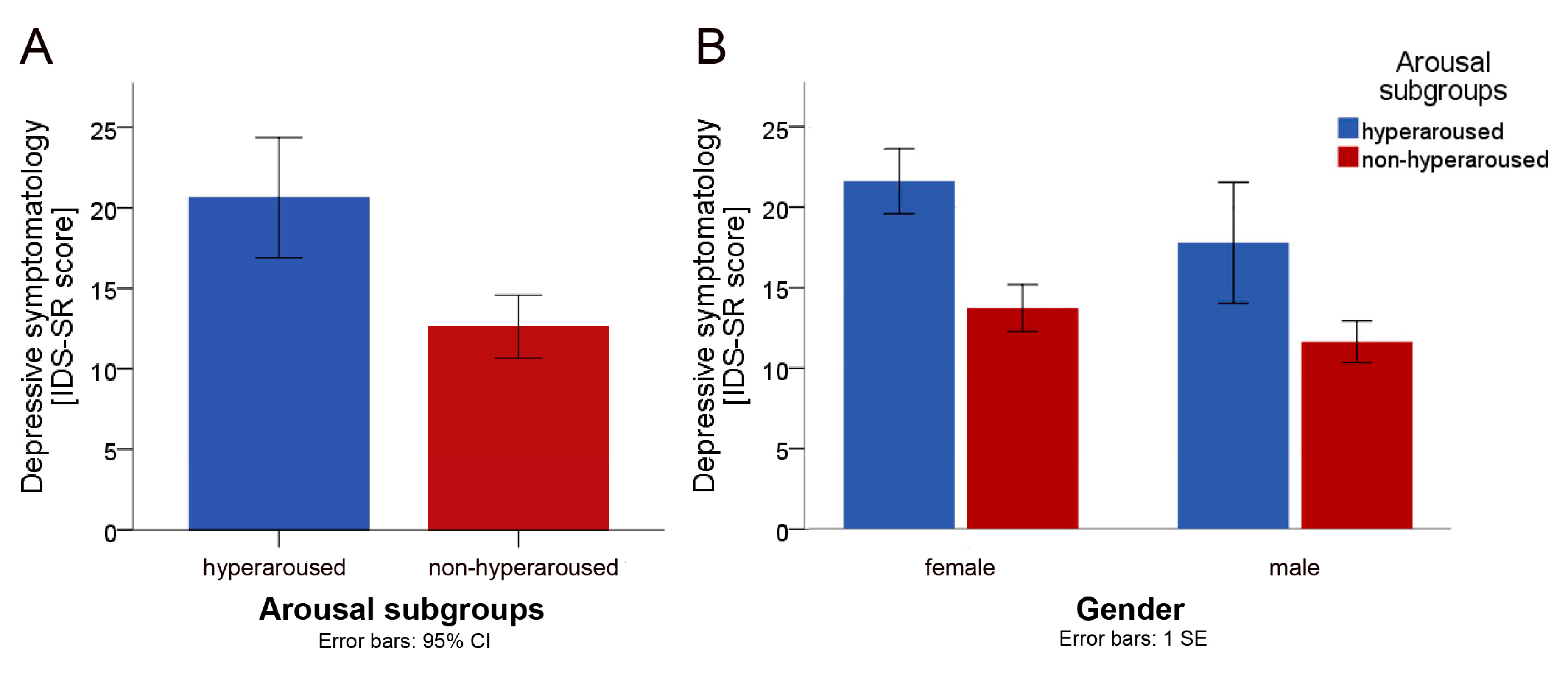
3.2. Main Analysis: Between-Group Comparisons of the Depression Score
3.3. Exploratory Sensitivity Analyses: Between-Group Comparisons of IDS-SR Items
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Overman, C.L.; Kool, M.B.; Da Silva, J.A.; Geenen, R. The prevalence of severe fatigue in rheumatic diseases: An international study. Clin. Rheumatol. 2016, 35, 409–415. [Google Scholar] [CrossRef]
- Segal, B.; Thomas, W.; Rogers, T.; Leon, J.M.; Hughes, P.; Patel, D.; Patel, K.; Novitzke, J.; Rohrer, M.; Gopalakrishnan, R. Prevalence, severity, and predictors of fatigue in subjects with primary Sjögren’s syndrome. Arthr. Care Res. 2008, 59, 1780–1787. [Google Scholar] [CrossRef] [PubMed]
- Weis, J. Cancer-related fatigue: Prevalence, assessment and treatment strategies. Expert Rev. Pharm. Outcomes Res. 2011, 11, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Beiske, A.G.; Loge, J.H.; Hjermstad, M.J.; Svensson, E. Fatigue in parkinson’s disease: Prevalence and associated factors. Mov. Disord. 2010, 25, 2456–2460. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.J.; Bacon, T.E.; Chamot, E.; Salter, A.R.; Cutter, G.R.; Kalina, J.T.; Kister, I. Prevalence of multiple sclerosis symptoms across lifespan: Data from the narcoms registry. Neurodegener. Dis. Manag. 2015, 5, 3–10. [Google Scholar]
- Ghanean, H.; Ceniti, A.K.; Kennedy, S.H. Fatigue in patients with major depressive disorder: Prevalence, burden and pharmacological approaches to management. CNS Drugs 2018, 32, 65–74. [Google Scholar] [CrossRef]
- Matcham, F.; Rayner, L.; Steer, S.; Hotopf, M. The prevalence of depression in rheumatoid arthritis: A systematic review and meta-analysis. Rheumatology 2013, 52, 2136–2148. [Google Scholar] [CrossRef]
- Caruso, R.; Nanni, M.; Riba, M.; Sabato, S.; Mitchell, A.; Croce, E.; Grassi, L. Depressive spectrum disorders in cancer: Prevalence, risk factors and screening for depression: A critical review. Acta Oncol. 2017, 56, 146–155. [Google Scholar] [CrossRef]
- Boeschoten, R.E.; Braamse, A.M.; Beekman, A.T.; Cuijpers, P.; van Oppen, P.; Dekker, J.; Uitdehaag, B.M. Prevalence of depression and anxiety in multiple sclerosis: A systematic review and meta-analysis. J. Neurol. Sci. 2017, 372, 331–341. [Google Scholar] [CrossRef]
- Goodarzi, Z.; Mrklas, K.J.; Roberts, D.J.; Jette, N.; Pringsheim, T.; Holroyd-Leduc, J. Detecting depression in parkinson disease: A systematic review and meta-analysis. Neurology 2016, 87, 426–437. [Google Scholar] [CrossRef]
- Hegerl, U.; Lam, R.W.; Malhi, G.S.; McIntyre, R.S.; Demyttenaere, K.; Mergl, R.; Gorwood, P. Conceptualising the neurobiology of fatigue. Aust. N. Z. J. Psychiatry 2013, 47, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Hegerl, U.; Ulke, C. Fatigue with up-vs downregulated brain arousal should not be confused. Prog. Brain Res. 2016, 229, 239–254. [Google Scholar] [PubMed]
- Hegerl, U.; Hensch, T. Why do stimulants not work in typical depression? Aust. N. Z. J. Psychiatry 2017, 51, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, B.N.; Insel, T.R. Toward the future of psychiatric diagnosis: The seven pillars of RDOC. BMC Med. 2013, 11, 126. [Google Scholar] [CrossRef] [PubMed]
- Olbrich, S.; Sander, C.; Minkwitz, J.; Chittka, T.; Mergl, R.; Hegerl, U.; Himmerich, H. EEG-vigilance regulation patterns and their discriminative power to separate patients with major depression from healthy controls. Neuropsychobiology 2012, 65, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Sander, C.; Hensch, T.; Wittekind, D.A.; Bottger, D.; Hegerl, U. Assessment of wakefulness and brain arousal regulation in psychiatric research. Neuropsychobiology 2015, 72, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Hegerl, U.; Sander, C.; Ulke, C.; Böttger, D.; Hensch, T.; Huang, J.; Mauche, N.; Olbrich, S. Vigilance Algorithm Leipzig (VIGALL) Version 2.1—Manual. Available online: http://research.uni-leipzig.de/vigall/ (accessed on 20 July 2020).
- Olbrich, S.; Mulert, C.; Karch, S.; Trenner, M.; Leicht, G.; Pogarell, O.; Hegerl, U. EEG-vigilance and bold effect during simultaneous EEG/fMRI measurement. NeuroImage 2009, 45, 319–332. [Google Scholar] [CrossRef]
- Jawinski, P.; Kittel, J.; Sander, C.; Huang, J.; Spada, J.; Ulke, C.; Wirkner, K.; Hensch, T.; Hegerl, U. Recorded and reported sleepiness: The association between brain arousal in resting state and subjective daytime sleepiness. Sleep 2017, 40, zsx099. [Google Scholar] [CrossRef]
- Huang, J.; Hensch, T.; Ulke, C.; Sander, C.; Spada, J.; Jawinski, P.; Hegerl, U. Evoked potentials and behavioral performance during different states of brain arousal. BMC Neurosci. 2017, 18, 21. [Google Scholar] [CrossRef]
- Ulke, C.; Huang, J.; Schwabedal, J.T.C.; Surova, G.; Mergl, R.; Hensch, T. Coupling and dynamics of cortical and autonomic signals are linked to central inhibition during the wake-sleep transition. Sci. Rep. 2017, 7, 11804. [Google Scholar] [CrossRef]
- Huang, J.; Ulke, C.; Sander, C.; Jawinski, P.; Hegerl, U.; Hensch, T. Impact of brain arousal and time-on-task on autonomic nervous system activity in the wake-sleep transition. BMC Neurosci. 2018, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Marqui, R.-D. Loreta (low resolution brain electromagnetic tomography): New authentic 3d functional images of the brain. ISBET Newsl. Issue 1994, 5, 4–8. [Google Scholar]
- Hegerl, U.; Wilk, K.; Olbrich, S.; Schoenknecht, P.; Sander, C. Hyperstable regulation of vigilance in patients with major depressive disorder. World J. Biol. Psychiatry 2012, 13, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, F.M.; Pschiebl, A.; Sander, C.; Kirkby, K.C.; Thormann, J.; Minkwitz, J.; Chittka, T.; Weschenfelder, J.; Holdt, L.M.; Teupser, D.; et al. Impact of serum cytokine levels on EEG-measured arousal regulation in patients with major depressive disorder and healthy controls. Neuropsychobiology 2016, 73, 1–9. [Google Scholar] [CrossRef]
- Ulke, C.; Tenke, C.E.; Kayser, J.; Sander, C.; Böttger, D.; Wong, L.Y.; Alvarenga, J.E.; Fava, M.; McGrath, P.J.; Deldin, P.J. Resting EEG measures of brain arousal in a multisite study of major depression. Clin. EEG Neurosci. 2018, 50, 3–12. [Google Scholar] [CrossRef]
- Ulke, C.; Wittekind, D.A.; Spada, J.; Franik, K.; Jawinski, P.; Hensch, T.; Hegerl, U. Brain arousal regulation in SSRI-medicated patients with major depression. J. Psychiatr. Res. 2018, 108, 34–39. [Google Scholar] [CrossRef]
- Jawinski, P.; Kirsten, H.; Sander, C.; Spada, J.; Ulke, C.; Huang, J.; Burkhardt, R.; Scholz, M.; Hensch, T.; Hegerl, U. Human brain arousal in the resting state: A genome-wide association study. Mol. Psychiatry 2018, 24, 1599–1609. [Google Scholar] [CrossRef]
- Kayumov, L.; Rotenberg, V.; Buttoo, K.; Auch, C.; Pandi-Perumal, S.R.; Shapiro, C.M. Interrelationships between nocturnal sleep, daytime alertness, and sleepiness: Two types of alertness proposed. J. Neuropsychiatry Clin. Neurosci. 2000, 12, 86–90. [Google Scholar] [CrossRef]
- Ulke, C.; Sander, C.; Jawinski, P.; Mauche, N.; Huang, J.; Spada, J.; Wittekind, D.; Mergl, R.; Luck, T.; Riedel-Heller, S.; et al. Sleep disturbances and upregulation of brain arousal during daytime in depressed versus non-depressed elderly subjects. World J. Biol. Psychiatry 2017, 18, 633–640. [Google Scholar] [CrossRef]
- Carney, R.M.; Freedland, K.E.; Veith, R.C. Depression, the autonomic nervous system, and coronary heart disease. Psychosom. Med. 2005, 67, 29–33. [Google Scholar] [CrossRef]
- Pariante, C.M.; Lightman, S.L. The hpa axis in major depression: Classical theories and new developments. Trends Neurosci. 2008, 31, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Olbrich, S.; Sander, C.; Jahn, I.; Eplinius, F.; Claus, S.; Mergl, R.; Schonknecht, P.; Hegerl, U. Unstable EEG-vigilance in patients with cancer-related fatigue (CRF) in comparison to healthy controls. World J. Biol. Psychiatry 2012, 13, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, R.; Heijnen, C.J.; Kavelaars, A.; Laye, S.; Capuron, L. The neuroimmune basis of fatigue. Trends Neurosci. 2014, 37, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Heesen, C.; Nawrath, L.; Reich, C.; Bauer, N.; Schulz, K.H.; Gold, S.M. Fatigue in multiple sclerosis: An example of cytokine mediated sickness behaviour? J. Neurol. Neurosurg. Psychiatry 2006, 77, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Lamkin, D.M. Inflammation and cancer-related fatigue: Mechanisms, contributing factors, and treatment implications. Brain Behav. Immun. 2013, 30, S48–S57. [Google Scholar] [CrossRef]
- Krueger, J.M.; Majde, J.A.; Rector, D.M. Cytokines in immune function and sleep regulation. Handb. Clin. Neurol. 2011, 98, 229–240. [Google Scholar] [PubMed]
- Stanton, B.; Barnes, F.; Silber, E. Sleep and fatigue in multiple sclerosis. Mult. Scler. 2006, 12, 481–486. [Google Scholar] [CrossRef]
- Sater, R.; Gudesblatt, M.; Kresa-Reahl, K.; Brandes, D.; Sater, P. The relationship between objective parameters of sleep and measures of fatigue, depression, and cognition in multiple sclerosis. Mult. Scler. J.—Exp. Transl. Clin. 2015, 1, 2055217315577828. [Google Scholar] [CrossRef]
- Gottschalk, M.; Kümpfel, T.; Flachenecker, P.; Uhr, M.; Trenkwalder, C.; Holsboer, F.; Weber, F. Fatigue and regulation of the hypothalamo-pituitary-adrenal axis in multiple sclerosis. Arch. Neurol. 2005, 62, 277–280. [Google Scholar] [CrossRef]
- Stoppe, M.; Meyer, K.; Schlingmann, M.; Olbrich, S.; Bergh, F.T. Hyperstable arousal regulation in multiple sclerosis. Psychoneuroendocrinology 2019, 110, 104417. [Google Scholar] [CrossRef]
- Loeffler, M.; Engel, C.; Ahnert, P.; Alfermann, D.; Arelin, K.; Baber, R.; Beutner, F.; Binder, H.; Brähler, E.; Burkhardt, R. The life-adult-study: Objectives and design of a population-based cohort study with 10,000 deeply phenotyped adults in Germany. BMC Public Health 2015, 15, 691. [Google Scholar] [CrossRef] [PubMed]
- Smets, E.M.; Garssen, B.; Bonke, B.; De Haes, J.C. The multidimensional fatigue inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef]
- First, M.B. Structured clinical interview for the DSM (SCID). Encycl. Clin. Psychol. 1995. [Google Scholar] [CrossRef]
- Drieling, T.; Scharer, L.O.; Langosch, J.M. The inventory of depressive symptomatology: German translation and psychometric validation. Int. J. Methods Psychiatr. Res. 2007, 16, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Glaesmer, H.; Brähler, E.; Löffler, M.; Engel, C.; Enzenbach, C.; Hegerl, U.; Sander, C. Sleep quality in the general population: Psychometric properties of the Pittsburgh sleep quality index, derived from a German community sample of 9284 people. Sleep Med. 2017, 30, 57–63. [Google Scholar] [CrossRef]
- Bloch, K.E.; Schoch, O.D.; Zhang, J.N.; Russi, E.W. German version of the Epworth sleepiness scale. Respiration 1999, 66, 440–447. [Google Scholar] [CrossRef]
- Sander, C.; Hegerl, U.; Wirkner, K.; Walter, N.; Kocalevent, R.-D.; Petrowski, K.; Glaesmer, H.; Hinz, A. Normative values of the epworth sleepiness scale (ess), derived from a large German sample. Sleep Breath. 2016, 20, 1337–1345. [Google Scholar] [CrossRef]
- Makeig, S.; Bell, A.J.; Jung, T.-P.; Sejnowski, T.J. Independent Component Analysis of Electroencephalographic Data. In Advances in Neural Information Processing Systems; MIT Press: Cambridge, MA, USA, 1996; pp. 145–151. [Google Scholar]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Gold, P.; Chrousos, G. Melancholic and atypical subtypes of depression represent distinct pathophysiological entities: CRH, neural circuits, and the diathesis for anxiety and depression. Mol. Psychiatry 2013, 18, 632. [Google Scholar] [CrossRef]
- Hegerl, U.; Hensch, T. The vigilance regulation model of affective disorders and ADHD. Neurosci. Biobehav. Rev. 2014, 44, 45–57. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Score | Scoring Criteria | EEG Block | Operational Definition |
|---|---|---|---|
| 14 | More than 2/3 of all segments in each 1 min epoch classified as 0/A1- or 0/A-stages | 1–4 | Predominant classification of 0 and A1 |
| 13 | 1–4 | Predominant classification of 0 and A | |
| 12 | At least 1/3 of all segments in a 1 min epoch classified as B1-stages | 4 | Stage B1 emerged in min 16–20 |
| 11 | 3 | Stage B1 emerged in min 11–15 | |
| 10 | 2 | Stage B1 emerged in min 6–10 | |
| 9 | 1 | Stage B1 emerged in min 1–5 | |
| 8 | At least 1/3 of segments in a 1 min epoch | 4 | Stage B2/3 emerged in min 16–20 |
| 7 | classified as B2/3-stages | 3 | Stage B2/3 emerged in min 11–15 |
| 6 | 2 | Stage B2/3 emerged in min 6–10 | |
| 5 | 1 | Stage B2/3 emerged in min 1–5 | |
| 4 | At least one C-stage classified | 4 | Stage C emerged in min 16–20 |
| 3 | 3 | Stage C emerged in min 11–15 | |
| 2 | 2 | Stage C emerged in min 6–10 | |
| 1 | 1 | Stage C emerged in min 1–5 |
| All (n = 60) | Hyperaroused (n = 19) | Non-Hyperaroused (n = 41) | |
|---|---|---|---|
| Demographics | |||
| Age, median years | 67.5 | 68.0 | 67.0 |
| Sex, f/m (%) | 33/27 (55.0/45.0) | 14/5 (73.7/26.3) | 19/22 (46.3/53.7) |
| Cancer, n (%) | 30 (50.0) | 10 (52.6) | 20 (48.8) |
| Skin cancer | 10 | 4 | 6 |
| Breast cancer | 9 | 3 | 6 |
| Prostata cancer | 4 | 0 | 4 |
| Bladder cancer | 2 | 1 | 1 |
| Colon cancer | 2 | 1 | 1 |
| Kidney cancer | 1 | 0 | 1 |
| Lymphoma | 1 | 1 | 0 |
| Thyroid cancer | 1 | 0 | 1 |
| Neuroinflammatory/autoimmune, n (%) | 30 (50.0) | 9 (47.4) | 21 (51.2) |
| Rheumatoid arthritis | 19 | 7 | 12 |
| SLE/Sjogren syndrome | 10 | 1 | 9 |
| Multiple sclerosis | 2 | 1 | 1 |
| Parkinson’s disease | 2 | 1 | 1 |
| Fatigue | |||
| MFI, median sum-score | 52.0 | 55.0 | 51.0 |
| All (n = 60) | Hyperaroused (n = 19) | Non-Hyperaroused (n = 41) | |
|---|---|---|---|
| Arousal Stability Score, median | 10.0 | 13.0 | 9.0 |
| ESS, mean score (SD) | 7.9 ± 3.4 | 6.8 ± 3.0 | 8.3 ± 3.6 |
| PSQI, mean score (SD) | 6.5 ± 3.5 | 8.4 ± 3.6 | 5.6 ± 3.1 |
| Good sleep quality, n (%) | 26 (47.3) | 5 (29.4) | 21 (55.3) |
| Poor sleep quality, n (%) | 19 (34.6) | 7 (41.2) | 12 (31.6) |
| Potentially clinically relevant sleep disorder, n (%) | 10 (18.2) | 5 (29.4) | 5 (13.2) |
| Total time in bed, median hours (range) | 8.6 (4.0–12.5) | 9.0 (6.5–12.5) | 8.5 (4.0–10.0) |
| EEG-Related Variables | |||
| Time of EEG recording, median, hh:mm | 9:00 | 9:00 | 9:00 |
| Coffee prior to EEG, yes (%) | 51 (85.0) | 16 (84.2) | 35 (85.4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulke, C.; Surova, G.; Sander, C.; Engel, C.; Wirkner, K.; Jawinski, P.; Hensch, T.; Hegerl, U. Fatigue in Cancer and Neuroinflammatory and Autoimmune Disease: CNS Arousal Matters. Brain Sci. 2020, 10, 569. https://doi.org/10.3390/brainsci10090569
Ulke C, Surova G, Sander C, Engel C, Wirkner K, Jawinski P, Hensch T, Hegerl U. Fatigue in Cancer and Neuroinflammatory and Autoimmune Disease: CNS Arousal Matters. Brain Sciences. 2020; 10(9):569. https://doi.org/10.3390/brainsci10090569
Chicago/Turabian StyleUlke, Christine, Galina Surova, Christian Sander, Christoph Engel, Kerstin Wirkner, Philippe Jawinski, Tilman Hensch, and Ulrich Hegerl. 2020. "Fatigue in Cancer and Neuroinflammatory and Autoimmune Disease: CNS Arousal Matters" Brain Sciences 10, no. 9: 569. https://doi.org/10.3390/brainsci10090569
APA StyleUlke, C., Surova, G., Sander, C., Engel, C., Wirkner, K., Jawinski, P., Hensch, T., & Hegerl, U. (2020). Fatigue in Cancer and Neuroinflammatory and Autoimmune Disease: CNS Arousal Matters. Brain Sciences, 10(9), 569. https://doi.org/10.3390/brainsci10090569