A Preliminary Study on Cranio-Facial Characteristics Associated with Minor Neurological Dysfunctions (MNDs) in Children with Autism Spectrum Disorders (ASD)

 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Methods
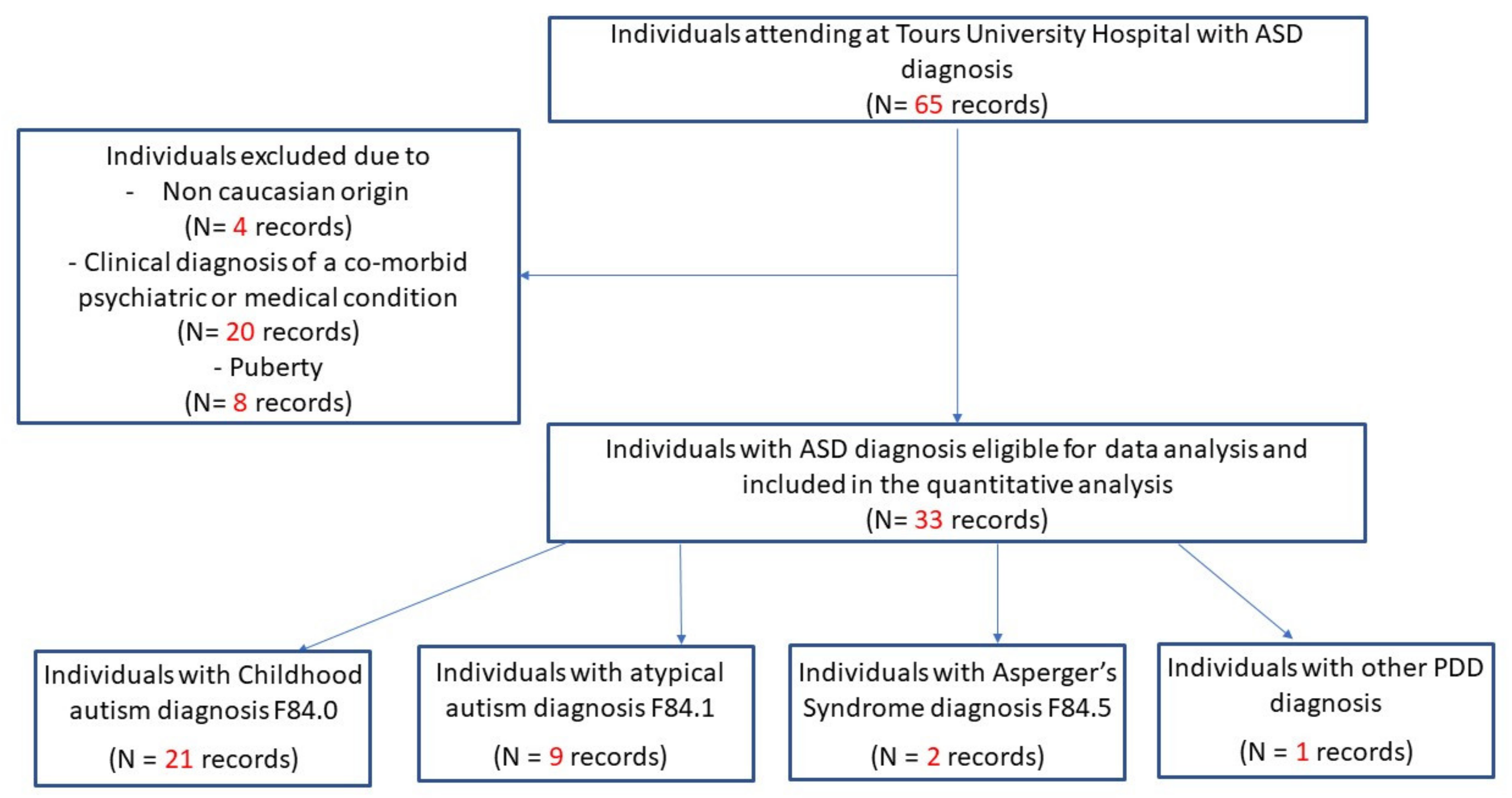
2.1. Participants
2.2. Morphological Assessment
2.3. Neurological Assessment
2.4. Statistical Methods
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rodier, P.M.; Bryson, S.E.; Welch, J.P. Minor Malformations and Physical Measurements in Autism: Data from Nova Scotia. Teratology 1997, 55, 319–325. [Google Scholar] [CrossRef]
- Gourion, D.; Gourevitch, R.; Le Provost, J.-B.; Olié, J.-P.; Lôo, H.; Krebs, M.-O. L’hypothèse neurodéveloppementale dans la schizophrénie. L’Encéphale 2004, 30, 109–118. [Google Scholar] [CrossRef]
- Keshavan, M.S.; Sanders, R.D.; Sweeney, J.A.; Diwadkar, V.A.; Goldstein, G.; Pettegrew, J.W.; Schooler, N.R. Diagnostic Specificity and Neuroanatomical Validity of Neurological Abnormalities in First-Episode Psychoses. Am. J. Psychiatry 2003, 160, 1298–1304. [Google Scholar] [CrossRef]
- Waldrop, M.F.; Pederson, F.A.; Bell, R.Q. Minor Physical Anomalies and Behavior in Preschool Children. Child Dev. 1968, 39, 391–400. [Google Scholar] [CrossRef]
- Özgen, H.M.; Hop, J.W.; Hox, J.J.; Beemer, F.A.; Van Engeland, H. Minor physical anomalies in autism: A meta-analysis. Mol. Psychiatry 2008, 15, 300–307. [Google Scholar] [CrossRef][Green Version]
- Tripi, G.; Roux, S.; Canziani, T.; Brilhault, F.B.; Barthélémy, C.; Canziani, F. Minor physical anomalies in children with autism spectrum disorder. Early Hum. Dev. 2008, 84, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.; McAlonan, G.; Fung, Y.Y.; Fung, G.; Yu, K.K.; Tai, K.-S.; Sham, P.C.; Chua, S.E. MRI Study of Minor Physical Anomaly in Childhood Autism Implicates Aberrant Neurodevelopment in Infancy. PLoS ONE 2011, 6, e20246. [Google Scholar] [CrossRef][Green Version]
- Boutrus, M.; Maybery, M.T.; Alvares, G.A.; Tan, D.W.; Varcin, K.J.; Whitehouse, A.J.O. Investigating Facial Phenotype in Autism Spectrum Conditions: The Importance of a Hypothesis Driven Approach. Autism Res. 2017, 10, 1910–1918. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, K.; George, I.D.; Cole, K.K.; Austin, J.R.; Takahashi, N.; Duan, Y.; Miles, J.H. Facial phenotypes in subgroups of prepubertal boys with autism spectrum disorders are correlated with clinical phenotypes. Mol. Autism 2011, 2, 15. [Google Scholar] [CrossRef]
- Obafemi-Ajayi, T.; Miles, J.H.; Takahashi, T.N.; Qi, W.; Aldridge, K.; Zhang, M.; Xin, S.-Q.; He, Y.; Duan, Y. Facial Structure Analysis Separates Autism Spectrum Disorders into Meaningful Clinical Subgroups. J. Autism Dev. Disord. 2014, 45, 1302–1317. [Google Scholar] [CrossRef] [PubMed]
- Tripi, G.; Roux, S.; Matranga, D.; Maniscalco, L.; Glorioso, P.; Bonnet-Brilhault, F.; Roccella, M. Cranio-Facial Characteristics in Children with Autism Spectrum Disorders (ASD). J. Clin. Med. 2019, 8, 641. [Google Scholar] [CrossRef] [PubMed]
- Ming, X.; Brimacombe, M.; Wagner, G.C. Prevalence of motor impairment in autism spectrum disorders. Brain Dev. 2007, 29, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Touwen, B.C.L. Examination of the Child with Minor Neurological Dysfunction; Heinemann Medical Books: London, UK, 1979. [Google Scholar]
- Hadders-Algra, M. Two distinct forms of minor neurological dysfunction: Perspectives emerging from a review of data of the Groningen Perinatal Project. Dev. Med. Child Neurol. 2002, 44, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Kavas, N.; Arısoy, A.E.; Bayhan, A.; Kara, B.; Günlemez, A.; Türker, G.; Oruç, M.; Gökalp, A.S. Neonatal sepsis and simple minor neurological dysfunction. Pediatr. Int. 2017, 59, 564–569. [Google Scholar] [CrossRef]
- Fournier, K.A.; Hass, C.J.; Naik, S.K.; Lodha, N.; Cauraugh, J.H. Motor Coordination in Autism Spectrum Disorders: A Synthesis and Meta-Analysis. J. Autism Dev. Disord. 2010, 40, 1227–1240. [Google Scholar] [CrossRef]
- Hadders-Algra, M.; Touwen, B.C. Minor Neurological Dysfunction Is More Closely Related to Learning Difficulties than to Behavioral Problems. J. Learn. Disabil. 1992, 25, 649–657. [Google Scholar] [CrossRef]
- Compton, M.T.; Bollini, A.; Mack, L.M.; Kryda, A.D.; Rutland, J.; Weiss, P.S.; Bercu, Z.; Esterberg, M.L.; Walker, E.F. Neurological soft signs and minor physical anomalies in patients with schizophrenia and related disorders, their first-degree biological relatives, and non-psychiatric controls. Schizophr. Res. 2007, 94, 64–73. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Schopler, E.; Reichler, R.J.; Renner, B.R. The Childhood Autism Rating Scale (CARS); Western Psychological Services: Los Angeles, CA, USA, 1988. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children, 3rd ed.; The Psychological Corporation: San Antonio, TX, USA, 1991. [Google Scholar]
- Hall, G.H.; Froster, U.G.; Allanson, J.E. Handbook of Normal Physical Measurements; Oxford Medical Publications; Oxford University Press: Cary, NC, USA, 1989. [Google Scholar]
- Farkas, L.G.; Munro, I.R.; Kolar, J.C. Anthropometric Facial Proportions in Medicine; Charles Thomas Publisher Ltd.: Springfield, IL, USA, 1987. [Google Scholar]
- Peters, L.H.; Maathuis, K.G.; Kouw, E.; Hamming, M.; Hadders-Algra, M. Test-retest, inter-assessor and intra-assessor reliability of the modified Touwen examination. Eur. J. Paediatr. Neurol. 2008, 12, 328–333. [Google Scholar] [CrossRef]
- Rapin, I. Preschool Children with Inadequate Communication: Developmental Language Disorder, Autism, Low IQ; Mac Keith Press: London, UK, 1996. [Google Scholar]
- Militerni, R.; Bravaccio, C.; Falco, C.; Fico, C. Palermo MT Repetitive Behaviors in Autistic Disorder. Eur. Child Adolesc. Psychiatry 2002, 11, 210–218. [Google Scholar] [CrossRef]
- Miles, J.H. Autism subgroups from a medical genetics perspective. In Autism Spectrum Disorders; Oxford University Press: Oxford, UK, 2011; pp. 705–721. [Google Scholar]
- Miles, J.H.; Hillman, R.E. Value of a Clinical Morphology Examination in Autism. Am. J. Med. Genet. 2000, 91, 245–253. [Google Scholar] [CrossRef]
- Yirmiya, N.; Charman, T. The prodrome of autism: Early behavioral and biological signs, regression, peri- and post-natal development and genetics. J. Child Psychol. Psychiatry 2010, 51, 432–458. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.B.; Enticott, P.G.; Rinehart, N.J. Motor Development and Delay: Advances in Assessment of Motor Skills in Autism Spectrum Disorders. Curr. Opin. Neurol. 2018, 31, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Bonnet-Brilhault, F.; Rajerison, T.A.; Paillet, C.; Guimard-Brunault, M.; Saby, A.; Ponson, L.; Tripi, G.; Malvy, J.; Roux, S. Autism is a prenatal disorder: Evidence from late gestation brain overgrowth. Autism Res. 2018, 11, 1635–1642. [Google Scholar] [CrossRef]
- De Jong, M.; Punt, M.; De Groot, E.; Minderaa, R.B.; Hadders-Algra, M. Minor neurological dysfunction in children with autism spectrum disorder. Dev. Med. Child Neurol. 2011, 53, 641–646. [Google Scholar] [CrossRef]
- Alamiri, B.; Nelson, C.; Fitzmaurice, G.M.; Murphy, J.M.; Gilman, S.E. Neurological Soft Signs and Cognitive Performance in Early Childhood. Dev. Psychol. 2018, 54, 2043–2052. [Google Scholar]
- Armony, J.; Servanschreiber, D.; Cohen, J.; Le Doux, J. Computational modeling of emotion: Explorations through the anatomy and physiology of fear conditioning. Trends Cogn. Sci. 1997, 1, 28–34. [Google Scholar] [CrossRef]
- Sagaspe, P.; Schwartz, S.; Vuilleumier, P. Fear and stop: A role for the amygdala in motor inhibition by emotional signals. Neuroimage 2011, 55, 1825–1835. [Google Scholar] [CrossRef]
- Gibbard, C.R.; Ren, J.; Skuse, D.H.; Clayden, J.D.; Clark, C.A. Structural connectivity of the amygdala in young adults with autism spectrum disorder. Hum. Brain Mapp. 2017, 39, 1270–1282. [Google Scholar] [CrossRef]
- Angkustsiri, K.; Krakowiak, P.; Moghaddam, B.; Wardinsky, T.; Gardner, J.; Kalamkarian, N.; Hertz-Picciotto, I.; Hansen, R.L.; Wardisky, T. Minor physical anomalies in children with autism spectrum disorders. Autism 2011, 15, 746–760. [Google Scholar] [CrossRef]
- Del Campo, M.; Jones, K.L. A review of the physical features of the fetal alcohol spectrum disorders. Eur. J. Med. Genet. 2017, 60, 55–64. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic and Clinical Variables | Anthropometric Variables | |||
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Z-Score | ||
| Age in months | 91.5 (26.7) | Cephalic Index | 74.2 (5.1) | −0.51 (1.2) |
| CARS | 30.4 (5.3) | Facial Index | 83.9 (6.6) | −0.17 (1.3) |
| Global QI | 59.9 (24.2) | Intercanthal Index | 38.7 (2.2) | 0.20 (1.0) |
| VQ | 50 (24.4) | Nasal Index | 72.5 (5.9) | 0.27 (0.9) |
| nVQ | 70 (26.8) | Mouth-Face Index | 36.7 (2.1) | −0.09 (0.9) |
| MND Total | 2.2 (1.5) | |||
| Type of Mild Neurological Dysfunction | |
|---|---|
| n (%) | |
| Posture and muscle tone | 10 (30%) |
| Reflex abnormalities | 1 (3%) |
| Involuntary movements | 3 (9%) |
| Coordination and balance | 10 (30%) |
| Fine motor dysfunction | 11 (33%) |
| Associated Movements | 19 (58%) |
| Sensory deficits | 17 (52%) |
| Cranial nerve dysfunction | 3 (9%) |
| s-MND | 15 (45%) |
| c-MND | 14 (42%) |
| Cephalic Index Z-Score | Facial Index Z-Score | Intercanthal Index Z-Score | Nasal Index Z-Score | Mouth-Face Index Z-Score | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | r | p-Value | |
| Age | 0.330 | 0.060 | −0.061 | 0.732 | 0.143 | 0.426 | −0.044 | 0.807 | 0.001 | 0.999 |
| CARS | 0.315 | 0.073 | −0.505 | 0.002 | 0.384 | 0.027 | −0.274 | 0.122 | −0.029 | 0.870 |
| Global IQ | −0.231 | 0.194 | 0.348 | 0.046 | −0.121 | 0.499 | 0.137 | 0.444 | 0.074 | 0.678 |
| VQ | −0.290 | 0.101 | 0.316 | 0.072 | −0.253 | 0.154 | 0.119 | 0.506 | 0.058 | 0.747 |
| nVQ | −0.182 | 0.308 | 0.328 | 0.061 | 0.012 | 0.944 | 0.208 | 0.244 | 0.036 | 0.838 |
| Posture and muscle tone | 0.432 | 0.012 | −0.293 | 0.097 | 0.278 | 0.116 | −0.196 | 0.272 | 0.192 | 0.283 |
| Reflex abnormalities | 0.186 | 0.299 | 0.049 | 0.785 | 0.381 | 0.028 | −0.259 | 0.145 | 0.174 | 0.332 |
| Involuntary movements | 0.042 | 0.812 | −0.145 | 0.419 | 0.276 | 0.118 | 0.184 | 0.304 | −0.205 | 0.252 |
| Coordination and balance | 0.203 | 0.255 | −0.081 | 0.652 | 0.132 | 0.461 | −0.233 | 0.191 | −0.015 | 0.933 |
| Fine motor dysfunction | −0.094 | 0.609 | 0.011 | 0.948 | 0.296 | 0.096 | −0.093 | 0.604 | −0.322 | 0.067 |
| Associated Movements | 0.158 | 0.378 | −0.298 | 0.091 | 0.154 | 0.391 | −0.021 | 0.906 | −0.048 | 0.788 |
| Sensory deficits | 0.547 | <0.001 | −0.532 | 0.001 | 0.064 | 0.720 | −0.088 | 0.626 | 0.206 | 0.248 |
| Cranial nerve dysfunction | 0.034 | 0.846 | −0.015 | 0.931 | 0.175 | 0.329 | 0.278 | 0.116 | −0.099 | 0.581 |
| s-MND | −0.448 | 0.008 | 0.271 | 0.126 | −0.244 | 0.170 | 0.118 | 0.511 | −0.083 | 0.644 |
| c-MND | 0.469 | 0.005 | −0.468 | 0.005 | 0.245 | 0.168 | −0.150 | 0.403 | 0.013 | 0.941 |
| Coef | 95%CI | p-Value | ||
|---|---|---|---|---|
| Cephalic Index | ||||
| Intercept | −5.455 | −10.786 | −0.125 | 0.045 |
| Fine motor dysfunction | −0.899 | −1.827 | 0.028 | 0.056 |
| Sensory deficits | 1.100 | 0.253 | 1.948 | 0.013 |
| Facial Index | ||||
| Intercept | 4.017 | −1.591 | 9.626 | 0.150 |
| CARS | −0.118 | −0.227 | −0.009 | 0.035 |
| Reflex abnormalities | 2.070 | −0.355 | 4.497 | 0.090 |
| Sensory deficits | −1.332 | −2.225 | −0.441 | 0.005 |
| Intercanthal Index | ||||
| Intercept | −4.229 | −9.392 | 0.933 | 0.102 |
| Global IQ | 0.025 | −0.001 | 0.051 | 0.063 |
| Mouth-Face Index | ||||
| Intercept | 0.016 | −5.156 | 5.188 | 0.995 |
| Fine motor dysfunction | −0.842 | −1.742 | 0.059 | 0.065 |
| Coef | 95%CI | p-Value | ||
|---|---|---|---|---|
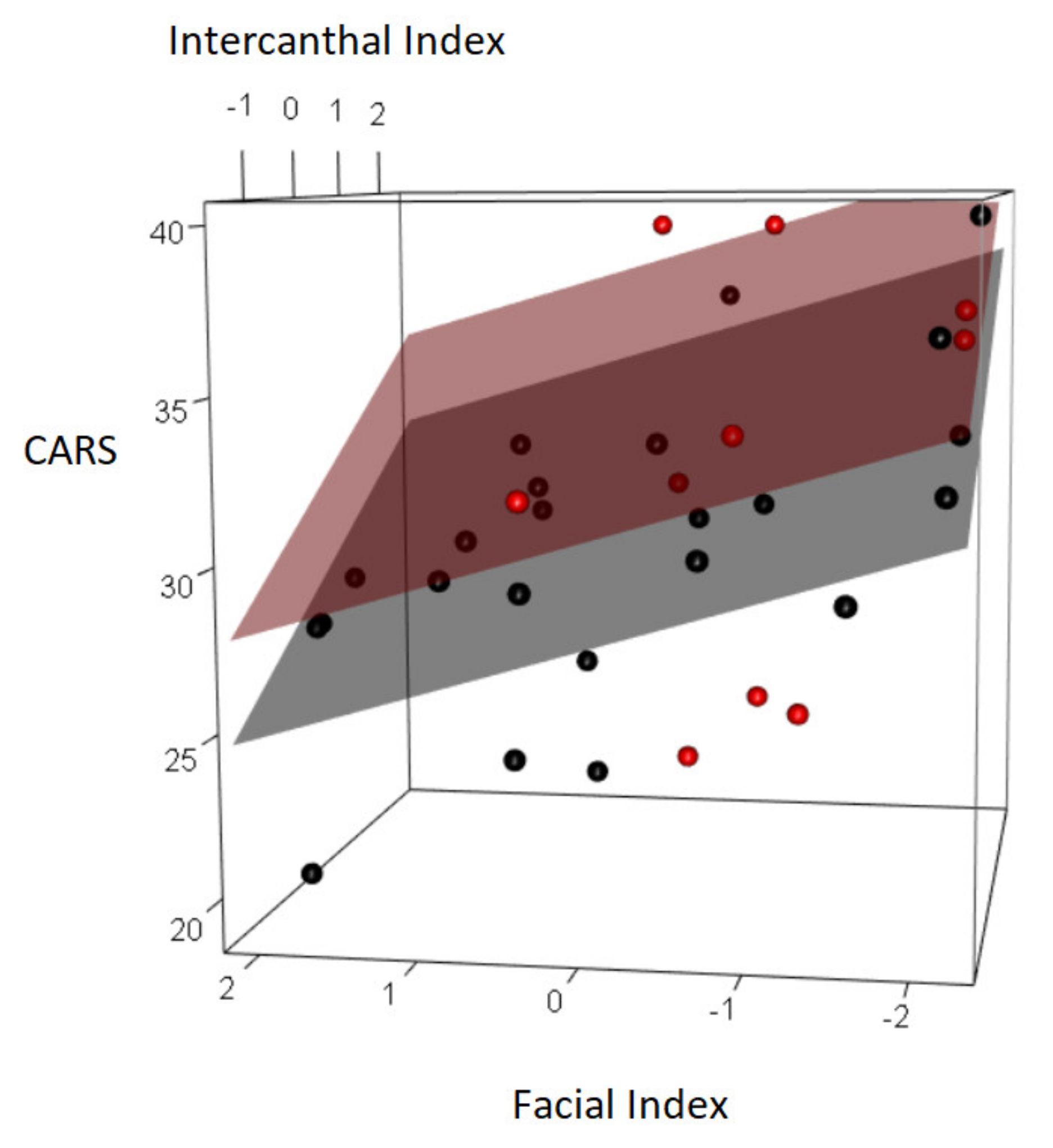
| CARS | ||||
| Intercept | 39.035 | 35.286 | 42.784 | <0.001 |
| Global QI | −0.138 | −0.191 | −0.085 | <0.001 |
| Posture and muscle tone | −3.155 | −5.944 | −0.367 | 0.027 |
| Facial Index | −1.410 | −2.338 | −0.482 | 0.004 |
| Intercanthal Index | 1.877 | 0.751 | 3.004 | 0.001 |
| Global QI | ||||
| Intercept | 162.072 | 126.819 | 197.326 | <0.001 |
| CARS | −2.674 | −3.894 | −1.455 | <0.001 |
| Total MND | −11.646 | −16.631 | −6.663 | <0.001 |
| Coordination and balance | 9.262 | −3.752 | 22.278 | 0.155 |
| Facial Index | −4.016 | −8.620 | 0.587 | 0.084 |
| Intercanthal Index | 8.805 | 3.281 | 14.331 | 0.002 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maniscalco, L.; Frédérique, B.-B.; Roccella, M.; Matranga, D.; Tripi, G. A Preliminary Study on Cranio-Facial Characteristics Associated with Minor Neurological Dysfunctions (MNDs) in Children with Autism Spectrum Disorders (ASD). Brain Sci. 2020, 10, 566. https://doi.org/10.3390/brainsci10080566
Maniscalco L, Frédérique B-B, Roccella M, Matranga D, Tripi G. A Preliminary Study on Cranio-Facial Characteristics Associated with Minor Neurological Dysfunctions (MNDs) in Children with Autism Spectrum Disorders (ASD). Brain Sciences. 2020; 10(8):566. https://doi.org/10.3390/brainsci10080566
Chicago/Turabian StyleManiscalco, Laura, Bonnet-Brilhault Frédérique, Michele Roccella, Domenica Matranga, and Gabriele Tripi. 2020. "A Preliminary Study on Cranio-Facial Characteristics Associated with Minor Neurological Dysfunctions (MNDs) in Children with Autism Spectrum Disorders (ASD)" Brain Sciences 10, no. 8: 566. https://doi.org/10.3390/brainsci10080566
APA StyleManiscalco, L., Frédérique, B.-B., Roccella, M., Matranga, D., & Tripi, G. (2020). A Preliminary Study on Cranio-Facial Characteristics Associated with Minor Neurological Dysfunctions (MNDs) in Children with Autism Spectrum Disorders (ASD). Brain Sciences, 10(8), 566. https://doi.org/10.3390/brainsci10080566