Autism in Adulthood: Clinical and Demographic Characteristics of a Cohort of Five Hundred Persons with Autism Analyzed by a Novel Multistep Network Model


Abstract
1. Introduction
2. Materials and Methods
- (a)
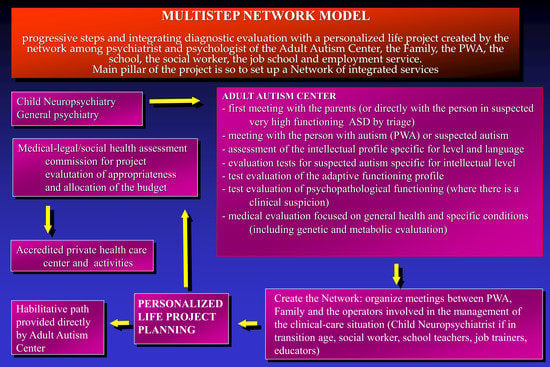
- First meeting with the parents: (i) careful collection of life history, (ii) all interventions carried out, (iii) needs and expectations—the direct meeting with the subject to be evaluated takes place only in the case of suspected high functioning PWA;
- (b)
- Meeting with the PWA or individual with suspected autism: (i) welcoming and creating a human supporting relationship, (ii) clinical evaluation of the symptoms presented, (iii) clinical evaluation of any psychopathological symptom in co-occurrence, (iv) objective neurological evaluation, and (v) clinical evaluation of cognitive functioning;
- (c)
- (d)
- Evaluation tests for suspected autism. The choice of tests to be performed is based on the clinical functioning and cognitive profile—Autism Diagnostic Interview-revised (ADIr) for all; Ritvo Autism and Asperger’s Diagnostic Scale-revised (RAADS) or Autism Diagnostic Observation Shedule-2nd Edition (ADOS 2) or Childhood Autism Rating Scale, Second Edition (CARS2-ST)depending on the level of functioning defined according to the clinical level and cognitive profile) [20,21,22,23];
- (e)
- Evaluation of the adaptive functioning profile (e.g., Vineland/Adaptive Behavior Assessment System – Second Edition) [24,25]; Test evaluation of psychopathological functioning—if there is a clinical suspicion—with scales for intellectual functioning evaluation (Structured Clinical Interview, Minnesota Multiphasic Personality Inventory-2, Systematic Psychopathological Assessment for persons with Intellectual and Developmental Disabilities - General screening, Rorschach) [26];
- (f)
- Medical evaluation focused on general health and specific conditions of neurodevelopment, including neuroimaging, genetic, metabolic evaluation, Electroencephalogram (EEG), depending on the individual’s situation;
- (g)
- Network meetings between operators of the Center for Autism in Adulthood and the patient’s family members. When possible, there should also be meetings between the PWA and the operators involved in the clinical management of the patient, i.e., the child neuropsychiatrist, and if in transition age, social workers, school teachers, job trainers, and educators. In addition, all personal information and that related to the life context should be collected. These meetings should ultimately lead to the creation of a life project through the integration of clinical information and that derived from the care network, above all taking into account the preferences and wishes of the PWA and their families;
- (h)
- The activation of a habilitative path provided directly by the center and/or presentation of the project to a Medico-Legal/Social Health Assessment Committee for evaluation of its appropriateness and allocation of the budget for the projects that will be delivered by accredited private healthcare centers.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Author Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Maenner, M.J.; Shaw, K.A.; Baio, J. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Bertelli, M.O. Autism spectrum disorder and intellectual disability. In Psychopathology in Adolescents and Adults with Autism Spectrum Disorders; Keller, R., Ed.; Springer Nature Switzerland: Basel, Switzerland, 2019; pp. 111–130. [Google Scholar]
- Simonoff, E.; Jones, C.R.G.; Baird, G.; Pickles, A.; Happé, F.; Charman, T. The persistence and stability of psychiatric problems in adolescents with autism spectrum disorders: Stability of psychiatric symptoms in autism spectrum disorders. J. Child Psychol. Psychiatry 2013, 54, 186–194. [Google Scholar] [CrossRef]
- Milen, M.T.; Nicholas, D.B. Examining transitions from youth to adult services for young persons with autism. Soc. Work Health Care 2017, 56, 636–648. [Google Scholar] [CrossRef]
- Płatos, M.; Pisula, E. Service use, unmet needs, and barriers to services among adolescents and young adults with autism spectrum disorder in Poland. BMC Health Serv. Res. 2019, 19, 587. [Google Scholar] [CrossRef]
- Eaves, L.C.; Ho, H.H. Young adult outcome of autism spectrum disorders. J. Autism Dev. Disord. 2008, 38, 739–747. [Google Scholar] [CrossRef]
- Howlin, P.; Moss, P.; Savage, S.; Rutter, M. Social outcomes in mid- to later adulthood among individuals diagnosed with autism and average nonverbal IQ as children. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 572–581. [Google Scholar] [CrossRef]
- Howlin, P.; Magiati, I. Autism spectrum disorder: Outcomes in adulthood. Curr. Opin. Psychiatry 2017, 30, 69–76. [Google Scholar] [CrossRef]
- Lugnegård, T.; Hallerbäck, M.U.; Gillberg, C. Psychiatric comorbidity in young adults with a clinical diagnosis of Asperger syndrome. Res. Dev. Disabil. 2011, 32, 1910–1917. [Google Scholar] [CrossRef]
- Hofvander, B.; Delorme, R.; Chaste, P.; Nydén, A.; Wentz, E.; Ståhlberg, O.; Herbrecht, E.; Stopin, A.; Anckarsäter, H.; Gillberg, C.; et al. Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry 2009, 9, 1–9. [Google Scholar] [CrossRef]
- Anderson, K.A.; Sosnowy, C.; Kuo, A.A.; Shattuck, P.T. Transition of Individuals With Autism to Adulthood: A Review of Qualitative Studies. Pediatrics 2018, 141, S318–S327. [Google Scholar] [CrossRef]
- Cidav, Z.; Lawer, L.; Marcus, S.C.; Mandell, D.S. Age-Related Variation in Health Service Use and Associated Expenditures Among Children with Autism. J. Autism Dev. Disord. 2013, 43, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, P.; Mathew, M.; Shea, L.L.; Brusilovskiy, E.; Nonnemacher, S.L. Service needs across the lifespan for individuals with autism. J. Autism Dev. Disord. 2016, 46, 2480–2489. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism spectrum disorder. Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef]
- King, C.; Merrick, H.; Le Couteur, A. How should we support young people with ASD and mental health problems as they navigate the transition to adult life including access to adult healthcare services. Epidemiol. Psychiatr. Sci. 2020, 29, e90. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV); NCS Pearson: San Antonio, TX, USA, 2008. [Google Scholar]
- Raven, J.C. Standardization of progressive matrices, 1938. Br. J. Med. Psychol. 1941, 19, 137–150. [Google Scholar] [CrossRef]
- Roid, G.H.; Miller, L.J. Leiter International Performance Scale-Revised (Leiter-R); Stoelting: Wood Dale, IL, USA, 1997. [Google Scholar]
- Rutter, M.; Le Couteur, A.; Lord, C. ADI-R. Autism Diagnostic Interview Revised. Manual; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Ritvo, R.A.; Ritvo, E.R.; Guthrie, N.; Ritvo, M.J.; Hufnagel, D.H.; McMahon, W.; Tonge, B.J.; Mataix-Cols, D.; Jassi, A.; Attwood, T.; et al. The Ritvo Autism Asperger Diagnostic Scale-Revised (RAADS-R): A Scale to Assist the Diagnosis of Autism Spectrum Disorder in Adults: An International Validation Study. J. Autism Dev. Disord. 2011, 41, 1076–1089. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule: ADOS; Western Psychological Services: Los Angeles, CA, USA, 2002. [Google Scholar]
- Schopler, E.; Reichler, R.J.; DeVellis, R.F.; Daly, K. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J. Autism Dev. Disord. 1980, 10, 91–103. [Google Scholar] [CrossRef]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.A. The Vineland Adaptive Behavior Scales. Major Psychol. Assess. Instrum. 1989, 2, 199–231. [Google Scholar]
- Harrison, P.; Oakland, T. ABAS-3: Adaptive Behavior Assessment System; Western Psychological Services: Los Angeles, CA, USA, 2015. [Google Scholar]
- Keller, R.; Bari, S.; Fratianni, B.; Piedimonte, A.; Freilone, F. Response to Rorschach test in autism spectrum disorders in adulthood: A pilot study. J. Psychopathol. 2018, 24, 224–229. [Google Scholar]
- Bennett, A.E.; Miller, J.S.; Stollon, N.; Prasad, R.; Blum, N.J. Autism Spectrum Disorder and Transition-Aged Youth. Curr. Psychiatry Rep. 2018, 20, 103. [Google Scholar] [CrossRef]
- Van Schalkwyk, G.I.; Volkmar, F.R. Autism Spectrum Disorders: Challenges and Opportunities for Transition to Adulthood. Child Adolesc. Psychiatr. Clin. N. Am. 2017, 26, 329–339. [Google Scholar] [CrossRef]
- Baron-Cohen, S. Empathizing, systemizing, and the extreme male brain theory of autism. Prog. Brain Res. 2010, 186, 167–175. [Google Scholar]
- Rynkiewicz, A.; Janas-Kozik, M.; Słopień, A. Girls and women with autism. Psychiatr. Pol. 2019, 53, 737–752. [Google Scholar] [CrossRef]
- Lai, M.-C.; Lombardo, M.V.; Auyeung, B.; Chakrabarti, B.; Baron-Cohen, S. Sex/gender differences and autism: Setting the scene for future research. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 11–24. [Google Scholar] [CrossRef]
- Wang, C.; Geng, H.; Liu, W.; Zhang, G. Prenatal, perinatal, and postnatal factors associated with autism. Medicine 2017, 96, e6696. [Google Scholar] [CrossRef]
- Gladfelter, A.; Barron, K.L. How Children with Autism Spectrum Disorder, Developmental Language Disorder, and Typical Language Learn to Produce Global and Local Semantic Features. Brain Sci. 2020, 10, 231. [Google Scholar] [CrossRef]
- Lai, M.-C.; Baron-Cohen, S. Identifying the lost generation of adults with autism spectrum conditions. Lancet Psychiatry 2015, 2, 1013–1027. [Google Scholar] [CrossRef]
- Valkanova, V.; Rhodes, F.; Allan, C.L. Diagnosis and management of autism in adults. Practitioner 2013, 257, 13–16. [Google Scholar]
- Luciano, C.; Keller, R. Misdiagnosis of High Function Autism Spectrum Disorders in Adults: An Italian Case Series. Autism Open Access 2014, 4, 2. [Google Scholar] [CrossRef]
- Sistema Italiano Linee Guida. Linea Guida n. 21, Il Trattamento dei Disturbi Dello Spettro Autistico nei Bambini e Negli Adolescent; Sistema Italiano Linee Guida: Roma, Italy, 2011. [Google Scholar]
- Lai, M.C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Craig, F.; Lamanna, A.L.; Margari, F.; Matera, E.; Simone, M.; Margari, L. Overlap Between Autism Spectrum Disorders and Attention Deficit Hyperactivity Disorder: Searching for Distinctive/Common Clinical Features. Autism Res. 2015, 8, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Postorino, V.; Kerns, C.M.; Vivanti, G.; Bradshaw, J.; Siracusano, M.; Mazzone, L. Anxiety Disorders and Obsessive-Compulsive Disorder in Individuals with Autism Spectrum Disorder. Curr. Psychiatry Rep. 2017, 19, 92. [Google Scholar] [CrossRef] [PubMed]
- Keller, R.; Bari, S. Psychosis and Autism Spectrum Disorder. In Psychopathology in Adolescents and Adults with Autism Spectrum Disorders; Keller, R., Ed.; Springer Nature Switzerland: Basel, Switzerland, 2019; pp. 51–65. [Google Scholar]
- Cauda, F.; Nani, A.; Costa, T.; Palermo, S.; Tatu, K.; Manuello, J.; Duca, S.; Fox, P.T.; Keller, R. The morphometric co-atrophy networking of schizophrenia, autistic and obsessive spectrum disorders. Hum. Brain Mapp. 2018, 39, 1898–1928. [Google Scholar] [CrossRef] [PubMed]
- Cauda, F.; Costa, T.; Nani, A.; Fava, L.; Palermo, S.; Bianco, F.; Duca, S.; Tatu, K.; Keller, R. Are schizophrenia, autistic, and obsessive spectrum disorders dissociable on the basis of neuroimaging morphological findings?: A voxel-based meta-analysis. Autism Res. 2017, 10, 1079–1095. [Google Scholar] [CrossRef]
- Keller, R.; Piedimonte, A.; Bianco, F.; Bari, S.; Cauda, F. Diagnostic Characteristics of Psychosis and Autism Spectrum Disorder in Adolescence and Adulthood. A Case Series. Autism Open Access 2015, 6, 159. [Google Scholar] [CrossRef]
- Alfageh, B.H.; Man, K.K.C.; Besag, F.M.C.; Alhawassi, T.M.; Wong, I.C.K.; Brauer, R. Psychotropic Medication Prescribing for Neuropsychiatric Comorbidities in Individuals Diagnosed with Autism Spectrum Disorder (ASD) in the UK. J. Autism Dev. Disord. 2020, 50, 625–633. [Google Scholar] [CrossRef]
- Di Sarro, R.; Varrucciu, N.; Di Santantonio, A.; Fioritti, A. Indagine sulle terapie farmacologiche e sulle diagnosi psichiatriche nei pazienti con diagnosi di disturbo dello spettro autistico registrati nei sistemi informativi territoriali. G. Ital. Disturbi Neurosviluppo 2020, 5, 100–107. [Google Scholar]
- Keller, R.; Basta, R.; Salerno, L.; Elia, M. Autism, epilepsy, and synaptopathies: A not rare association. Neurol. Sci. 2017, 38, 1353–1361. [Google Scholar] [CrossRef]
- Biamino, E.; Di Gregorio, E.; Belligni, E.F.; Keller, R.; Riberi, E.; Gandione, M.; Calcia, A.; Mancini, C.; Giorgio, E.; Cavalieri, S.; et al. A novel 3q29 deletion associated with autism, intellectual disability, psychiatric disorders, and obesity. Am. J. Med Genet. Part B Neuropsychiatr. Genet. 2016, 171, 290–299. [Google Scholar] [CrossRef]
- Bertelli, M.; Merli, M.P.; Bradley, E.; Keller, R.; Varrucciu, N.; Del Furia, C.; Panocchia, N. The diagnostic boundary between autism spectrum disorder, intellectual developmental disorder and schizophrenia spectrum disorders. Adv. Ment. Heal. Intellect. Disabil. 2015, 9, 243–264. [Google Scholar] [CrossRef]
- Deslauriers, N. The Empty Fortress: Infantile Autism and the Birth of the Self. Arch. Gen. Psychiatry 1967, 17, 510–512. [Google Scholar] [CrossRef]
- Fink, E.; Olthof, T.; Goossens, F.; Van Der Meijden, S.; Begeer, S. Bullying-related behaviour in adolescents with autism: Links with autism severity and emotional and behavioural problems. Autism 2018, 22, 684–692. [Google Scholar] [CrossRef]
- Smith, I.C.; White, S.W. Socio-emotional determinants of depressive symptoms in adolescents and adults with autism spectrum disorder: A systematic review. Autism 2020, 24, 995–1010. [Google Scholar] [CrossRef] [PubMed]
- Bari, S.; Tisci, R.; Burlando, R.; Keller, R. Caring for Autistic Adults. A Qualitative Analysis Under the Lens of Capability Approach. Ital. Sociol. Rev. 2018, 8, 243–264. [Google Scholar]
- Gorenstein, M.; Giserman-Kiss, I.; Feldman, E.; Isenstein, E.L.; Donnelly, L.; Wang, A.T.; Foss-Feig, J. Brief Report: A Job-Based Social Skills Program (JOBSS) for Adults with Autism Spectrum Disorder: A Pilot Randomized Controlled Trial. J. Autism Dev. Disord. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Sample | n | % | |
| Male | 388 | 77.5 | |
| Female | 112 | 22.5 | |
| Age | M = 31.7 | SD = 10.7 | Range: 18–82 years |
| Place of Residence | n | % | |
| Turin | 262 | 52.9 | |
| (Rural) Canavese Area | 34 | 6.9 | |
| Nichelino/Moncalieri and Carmagnola (Periurban areas) | 55 | 11.1 | |
| Medico-Legal Assessment of Professional Competences | n | % | |
| 302 | 65.4 | ||
| In Details | |||
| 46% civil disability level (CD) | 2.1 | ||
| 67% civil disability level (CD) | 0.9 | ||
| 75% civil disability level (CD) | 7.1 |
| Co-Occurrence | n | % |
|---|---|---|
| personality disorders | 79 | 24% |
| challenging/problem behaviour | 66 | 19.6% |
| Attention Deficit Hyperactivity Disorder (ADHD) | 32 | 9.5% |
| epilepsy | 23 | 6.8% |
| obsessive compulsive disorder | 23 | 6.8% |
| major depressive disorder | 21 | 6.3% |
| psychosis | 19 | 5.7% |
| bipolar disorder | 8 | 2.4% |
| anxiety disorder | 6 | 1.8% |
| specific learning disorder. | 6 | 1.8% |
| tic disorder | 6 | 1.8% |
| oppositional defiant disorder | 5 | 1.5% |
| deafness | 5 | 1.5% |
| Down syndrome | 5 | 1.5% |
| social phobia | 5 | 1.5% |
| Tourette syndrome | 5 | 1.5% |
| eating disorder | 4 | 1.2% |
| blindness | 3 | 0.9% |
| movement disorder | 3 | 0.9% |
| substance abuse disorder | 3 | 0.9% |
| dyspraxia | 2 | 0.6% |
| language disorder | 2 | 0.6% |
| X fragile syndrome | 2 | 0.6% |
| tuberous sclerosis | 1 | 0.3% |
| Turner syndrome | 1 | 0.3% |
| XXY syndrome | 1 | 0.3% |
| Personality Disorders Co-Occurrence in ASD (PD) | n | % |
|---|---|---|
| paranoid PD | 19 | 5.7% |
| borderline PD | 18 | 5.4% |
| personality disorder not otherwise specified | 7 | 2.1% |
| schizotypical PD | 7 | 2.1% |
| avoidant PD | 6 | 1.8% |
| obsessive PD | 6 | 1.8% |
| narcissistic PD | 5 | 1.5% |
| schizoid PD | 5 | 1.5% |
| aggressive passive PD | 3 | 0.9% |
| histrionic PD | 2 | 0.6% |
| dependant PD | 1 | 0.3% |
| Total | 79 | 24% |
| Complications | n | % | Note |
|---|---|---|---|
| During pregnancy | 72 | 15.5 | including 5.8% risk of abortion (n = 27) |
| Gestosis | 12 | 2.5 | |
| Twin pregnancy | 7 | 1.5 | |
| Depressive disorder | 3 | 0.6 | |
| Diabetes | 1 | 0.2 | |
| Thyroid disorder | 1 | 0.2 | |
| Toxoplasmosis | 2 | 0.4 |
| The Age When Symptoms Worried the Family | % PWA |
|---|---|
| 6 Months | 3.8 |
| 12 Months | 11.3 |
| 18 Months | 19.5 |
| 24 Months | 42.6 |
| 30 Months | 47.2 |
| 42 Months | 80.3 |
| 48 Months | 84.3 |
| 60 Months | 97.8 |
| 72 Months | 93.8 |
| Intervention Type | n | % |
|---|---|---|
| Psychotherapy | 143 | 29.9 |
| Speech Therapy | 200 | 42.1 |
| Educational Interventions | 117 | 24.6 |
| Psychomotor skills Treatment | 183 | 38.6 |
| Delacato method | 4 | 0.8 |
| Portage method | 13 | 2.7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keller, R.; Chieregato, S.; Bari, S.; Castaldo, R.; Rutto, F.; Chiocchetti, A.; Dianzani, U. Autism in Adulthood: Clinical and Demographic Characteristics of a Cohort of Five Hundred Persons with Autism Analyzed by a Novel Multistep Network Model. Brain Sci. 2020, 10, 416. https://doi.org/10.3390/brainsci10070416
Keller R, Chieregato S, Bari S, Castaldo R, Rutto F, Chiocchetti A, Dianzani U. Autism in Adulthood: Clinical and Demographic Characteristics of a Cohort of Five Hundred Persons with Autism Analyzed by a Novel Multistep Network Model. Brain Sciences. 2020; 10(7):416. https://doi.org/10.3390/brainsci10070416
Chicago/Turabian StyleKeller, Roberto, Silvia Chieregato, Stefania Bari, Romina Castaldo, Filippo Rutto, Annalisa Chiocchetti, and Umberto Dianzani. 2020. "Autism in Adulthood: Clinical and Demographic Characteristics of a Cohort of Five Hundred Persons with Autism Analyzed by a Novel Multistep Network Model" Brain Sciences 10, no. 7: 416. https://doi.org/10.3390/brainsci10070416
APA StyleKeller, R., Chieregato, S., Bari, S., Castaldo, R., Rutto, F., Chiocchetti, A., & Dianzani, U. (2020). Autism in Adulthood: Clinical and Demographic Characteristics of a Cohort of Five Hundred Persons with Autism Analyzed by a Novel Multistep Network Model. Brain Sciences, 10(7), 416. https://doi.org/10.3390/brainsci10070416