Synergistic Effects of Scalp Acupuncture and Repetitive Transcranial Magnetic Stimulation on Cerebral Infarction: A Randomized Controlled Pilot Trial


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Considerations
2.3. Participant Recruitment
2.4. Participation
2.5. Randomization and Blinding
2.6. Implementation
2.7. Intervention
2.8. Outcome Measurements
2.9. Sample Size Calculation
2.10. Statistical Analyses
3. Results
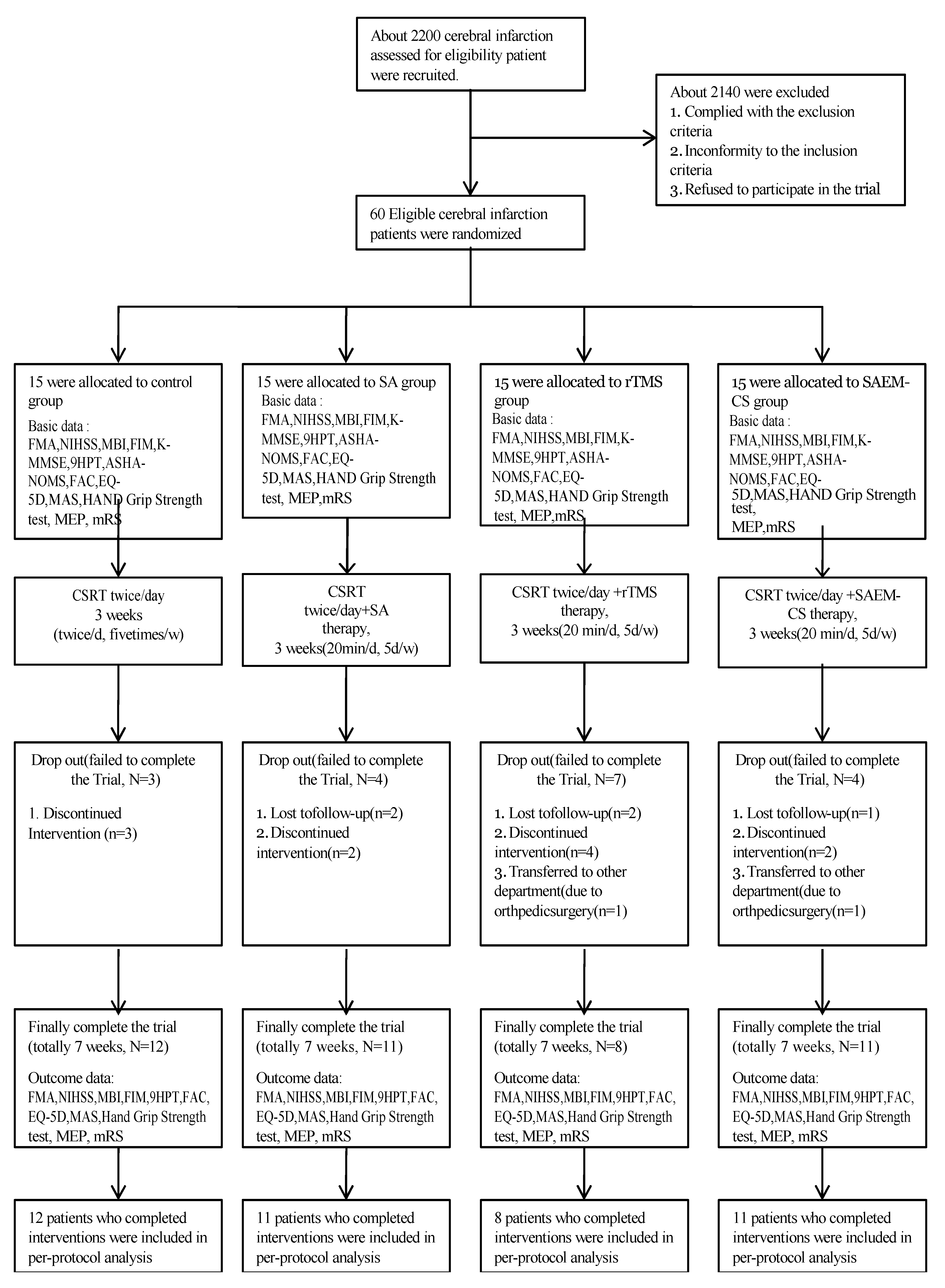
3.1. Participants
3.2. Baseline Characteristics
3.3. Efficacy of Primary and Secondary Outcomes
3.3.1. Changes in Outcome Measures in the Four Groups
3.3.2. Comparisons of Value Changes in Outcome Measures among the Four Groups
3.3.3. Multiple Comparisons of FMAUE, FMAT, MBI, FIM, and EQ-5D among the Four Groups
3.4. Safety Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Minino, A.M.; Murphy, S.L.; Xu, J.; Kochanek, K.D. Deaths: Final data for 2008. Natl. Vital Stat. Rep. 2011, 59, 1–126. [Google Scholar] [PubMed]
- Donnan, G.A.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Wang, J.; Pei, J.; Khiati, D.D.; Fu, Q.H.; Cui, X.; Song, Y.; Yan, M.; Shi, L.J.; Cai, Y.; Ma, Y.H. Acupuncture treatment on the motor area of the scalp for motor dysfunction in patients with ischemic stroke: Study protocol for a randomized controlled trial. Trials 2017, 18, 287. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Fang, J.; Ma, R.; Froym, R.; Gu, X.; Li, J.; Chen, L.; Xu, S.; Ji, C. Acupuncture for acute stroke: Study protocol for a multicenter, randomized, controlled trial. Trials 2014, 15, 214–219. [Google Scholar] [CrossRef]
- Murphy, T.H.; Corbett, D. Plasticity during stroke recovery from synapse to behaviour. Nat. Rev. Neurosci. 2009, 10, 861–872. [Google Scholar] [CrossRef]
- Dimyan, M.A.; Cohen, L.G. Neuroplasticity in the context of motor rehabilitation after stroke. Nat. Rev. Neurol. 2011, 7, 76–85. [Google Scholar] [CrossRef]
- Takeuchi, N.; Izumi, S.-I. Maladaptive Plasticity for Motor Recovery after Stroke: Mechanisms and Approaches. Neural Plast. 2012, 2012, 359728. [Google Scholar] [CrossRef]
- Takeuchi, N.; Izumi, S.-I. Combinations of stroke neurorehabilitation to facilitate motor recovery: Perspectives on Hebbian plasticity and homeostatic metaplasticity. Front. Hum. Neurosci. 2015, 9, 349. [Google Scholar] [CrossRef]
- Liu, Z.; Guan, L.; Wang, Y.; Xie, C.-L.; Lin, X.-M.; Zheng, G.-Q. History and Mechanism for Treatment of Intracerebral Hemorrhage with Scalp Acupuncture. Evid. Based Complement. Altern. Med. 2012, 2012, 895032. [Google Scholar] [CrossRef]
- Wang, W.W.; Xie, C.L.; Lu, L.; Zheng, G.Q. A systematic review and meta-analysis of Baihui (GV20)-based scalp acupuncture in experimental ischemic stroke. Sci. Rep. 2014, 4, 3981. [Google Scholar] [CrossRef]
- Zheng, G.Q.; Zhao, Z.M.; Wang, Y.; Gu, Y.; Li, Y.; Chen, X.M.; Fu, S.P.; Shen, J. Meta-analysis of scalp acupuncture for acute hypertensive intracerebral hemorrhage. J. Altern. Complement. Med. 2011, 17, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Hsing, W.T.; Imamura, M.; Weaver, K.; Fregni, F.; Azevedo Neto, R.S. Clinical effects of scalp electrical acupuncture in stroke: A sham-controlled randomized clinical trial. J. Altern. Complement. Med. 2012, 18, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shen, J.; Wang, X.M.; Fu, D.L.; Chen, C.Y.; Lu, L.Y.; Lu, L.; Xie, C.L.; Fang, J.Q.; Zheng, G.Q. Scalp acupuncture for acute ischemic stroke: A meta-analysis of randomized controlled trials. Evid. Based Complement. Altern Med. 2012, 2012, 480950. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Shin, B.C.; Lee, M.S.; Han, C.H.; Kim, J.I. Scalp acupuncture for stroke recovery: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Integr. Med. 2013, 5, 87–99. [Google Scholar] [CrossRef]
- Di Pino, G.; Pellegrino, G.; Assenza, G.; Capone, F.; Ferreri, F.; Formica, D.; Ranieri, F.; Tombini, M.; Ziemann, U. Modulation of brain plasticity in stroke: A novel model for neurorehabilitation. Nat. Rev. Neurol. 2014, 10, 597–608. [Google Scholar] [CrossRef]
- Siebner, H.R.; Rothwell, J. Transcranial magnetic stimulation: New insight into representational cortical plasticity. Exp. Brain Res. 2003, 148, 1–16. [Google Scholar] [CrossRef]
- Rossini, P.M.; Rossi, S. Transcranial magnetic stimulation: Diagnostic, therapeutic, and research potential. Neurology 2007, 68, 484–488. [Google Scholar] [CrossRef]
- Peinemann, A.; Reimer, B.; Loer, C.; Quartarone, A.; Munchau, A.; Conrad, B.; Seibner, H.R. Long-lasting increase in corticospinal excitability after 1800 pulses of subthreshold 5 Hz repetitive TMS to the primary motor cortex. Clin. Neurophysiol. 2004, 11, 1519–1526. [Google Scholar] [CrossRef]
- Mansur, C.G.; Fregni, F.; Boggio, P.S.; Riberto, M.; Gallucci Neto, J.; Santos, C.M.; Wagner, T.; Riqonatti, S.P.; Marcolin, M.A.; Pacual-Leone, A. A sham stimulation-controlled trial of rTMS of the unaffected hemisphere in stroke patients. Neurology 2005, 64, 1802–1804. [Google Scholar] [CrossRef]
- Fregni, F.; Boggio, P.S.; Valle, A.C.; Rocha, R.R.; Duarte, J.; Ferreira, M.J.; Wagner, T.; Fecteau, S.; Riberto, M.; Freedman, S.D.; et al. A sham-controlled trial of a 5-day course of repetitive transcranial magnetic stimulation of the unaffected hemisphere in stroke patients. Stroke 2006, 37, 2115–2122. [Google Scholar] [CrossRef]
- Sasaki, N.; Mizutani, S.; Kakuda, W.; Abo, M. Comparison of the effects of high- and low-frequency repetitive transcranial magnetic stimulation on upper limb hemiparesis in the early phase of stroke. J. Stroke Cereb. Dis. 2013, 22, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Abdel-Fadeil, M.R.; Farghali, A.; Qaid, M. Role of 1 and 3 Hz repetitive transcranial magnetic stimulation on motor function recovery after acute ischemic stroke. Eur. J. Neurol. 2009, 16, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.Y.; Cheng, C.H.; Liao, K.K.; Lee, I.H.; Lin, Y.Y. Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke a meta-analysis. Stroke 2012, 43, 1849–1857. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, N.; Tada, T.; Toshima, M.; Matsuo, Y.; Ikoma, K. Repetitive transcranial magnetic stimulation over bilateral hemispheres enhances motor function and training effect of paretic hand in patients after stroke. J. Rehabil. Med. 2009, 41, 1049–1054. [Google Scholar] [CrossRef] [PubMed]
- Han, J.Y.; Kim, J.H.; Park, J.H.; Song, M.Y.; Song, M.K.; Kim, D.J.; You, Y.N.; Park, G.C.; Cho, M.R.; Shin, J.C.; et al. Scalp acupuncture and electromagnetic convergence stimulation for patients with cerebral infarction: Study protocol for a randomized controlled trial. Trials 2016, 17, 490. [Google Scholar] [CrossRef]
- Zhao, N.; Zhang, J.; Qiu, M.; Wang, C.; Xiang, Y.; Wang, H.; Xie, J.; Liu, S.; Wu, J. Scalp acupuncture plus low-frequency rTMS promotes repair of brain white matter tracts in stroke patients: A DTI study. J. Integr. Neurosci. 2018, 17, 61–69. [Google Scholar] [CrossRef]
- Kakuda, W.; Abo, M.; Shimizu, M.; Sasanuma, J.; Okamoto, T.; Yokoi, A.; Taquchi, K.; Mitani, S.; Harashima, H.; Urushidani, N.; et al. NEURO Investigators. A multi-center study on low-frequency rTMS combined with intensive occupational therapy for upper limb hemiparesis in post-stroke patients. J. Neuroeng. Rehabil. 2012, 9, 4–14. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar]
- Adams, H.P.; Davis, P.H.; Leira, E.C.; Chang, K.C.; Bendixen, B.H.; Clarke, W.R.; Woolson, R.F.; Hansen, M.D. Baseline NIH stroke scale score strongly predicts outcome after stroke a report of the Trial of Org 10172 in Acute Stroke Treatment(TOAST). Neurology 1999, 53, 126–131. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Dodds, T.A.; Martin, D.P.; Stolov, W.C.; Deyo, R.A. A validation of the functional independence measurement and its performance among rehabilitation inpatients. Arch. Phys. Med. Rehabil. 1993, 74, 531–536. [Google Scholar] [CrossRef]
- Han, C.; Jo, S.A.; Jo, I.; Kim, E.; Park, M.H.; Kang, Y. An adaptation of the Korean mini-mental state examination (K-MMSE) in elderly Koreans: Demographic influence and population-based norms (the AGE study). Arch. Gerontol. Geriatr. 2008, 47, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.B.; Lee, H.J.; Yoo, J.; Kwon, Y.G. Effect of low-frequency rTMS and NMES on subacute unilateral hemispheric stroke with dysphagia. Ann. Rehabil. Med. 2014, 38, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Doruk, P. The impact of knee osteoarthritis on rehabilitation outcomes in hemiparetic stroke patients. J. Back Musculoskelet. Rehabil. 2013, 26, 207–211. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lioyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Kakuda, W.; Abo, M.; Kobayashi, K.; Momosaki, R.; Yokoi, A.; Fukuda, A.; Ito, H.; Tominaga, A.; Umemori, T.; Kameda, Y. Anti-spastic effect of low-frequency rTMS applied with occupational therapy in post-stroke patients with upper limb hemiparesis. Brain INJ 2011, 25, 496–502. [Google Scholar] [CrossRef]
- Lim, K.B.; Kim, J.A. Activity of daily living and motor evoked potentials in the subacute stroke patients. Ann. Rehabil. Med. 2013, 37, 82–87. [Google Scholar] [CrossRef]
- Quinn, T.J.; McArthur, K.; Dawson, J.; Walters, M.R.; Lees, K.R. Reliability of structured modified Rankin Scale assessment. Stroke 2010, 41, 602–603. [Google Scholar] [CrossRef]
- Talelli, P.; Wallace, A.; Dileone, M.; Hoad, D.; Cheeran, B.; Oliver, R.; Bos, M.V.D.; Hammerbeck, U.; Barratt, K.; Gillini, C.; et al. Theta Burst Stimulation in the Rehabilitation of the Upper Limb: A Semirandomized, Placebo-Controlled Trial in Chronic Stroke Patients. Neurorehabilit. Neural Repair 2012, 26, 976–987. [Google Scholar] [CrossRef]
- Khedr, E.M.; Fetoh, N.A.-E. Short- and long-term effect of rTMS on motor function recovery after ischemic stroke. Restor. Neurol. Neurosci. 2010, 28, 545–559. [Google Scholar] [CrossRef]
- Seniow, J.; Bilik, M.; Lesniak, M.; Waldowski, K.; Iwanski, S.; Czlonkowska, A. Transcranial magnetic stimulation combined with physiotherapy in rehabilitation of poststroke hemiparesis: A randomized, double-blind, placebo-controlled study. Neurorehabilit. Neural Repair 2012, 26, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Koski, L.; Xie, H. Combining rTMS and Task-Oriented Training in the Rehabilitation of the Arm after Stroke: A Pilot Randomized Controlled Trial. Stroke Res. Treat. 2013, 2013, 539146. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.K.; Patten, C. Does inhibitory repetitive transcranial magnetic stimulation augment functional task practice to improve arm recovery in chronic stroke? Stroke Res. Treat. 2014, 2014, 305236. [Google Scholar] [CrossRef]
- Fitzgerald, P.; Fountain, S.; Daskalakis, Z. A comprehensive review of the effects of rTMS on motor cortical excitability and inhibition. Clin. Neurophysiol. 2006, 117, 2584–2596. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Kim, Y.H.; Bang, O.Y.; Kim, S.T.; Park, Y.H.; Lee, P.K. Long-term effects of rTMS on motor recovery in patients after subacute stroke. J. Rehabil. Med. 2010, 42, 758–764. [Google Scholar] [PubMed]
- Khedr, E.M.; Etraby, A.E.; Hemeda, M.; Nasef, A.M.; Razek, A.A.E. Long-term effect of repetitive transcranial magnetic stimulation on motor function recovery after acute ischemic stroke. Acta Neurol. Scand. 2010, 121, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Shi, G.X.; Yang, X.M.; Liu, C.Z.; Wang, L.P. Factors contributing to therapeutic effects evaluated in acupuncture clinical trials. Trials 2012, 13, 42. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for the Western Pacific. WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region; World Health Organization Regional Office for the Western Pacific: Manila, Philippines, 2007. [Google Scholar]
- Li, L.; Zhang, H.; Meng, S.-Q.; Qian, H.-Z. An Updated Meta-Analysis of the Efficacy and Safety of Acupuncture Treatment for Cerebral Infarction. PLoS ONE 2014, 9, e114057. [Google Scholar] [CrossRef]
- Chen, L.; Fang, J.; Ma, R.; Gu, X.; Chen, L.; Li, J.; Xu, S. Additional effects of acupuncture on early comprehensive rehabilitation in patients with mild to moderate acute ischemic stroke: A multicenter randomized controlled trial. BMC Complement. Altern. Med. 2016, 16, 226. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Y.; Zhang, H.; Wu, P.; Huang, W. The effect of acupuncture on the motor function and white matter microstructure in ischemic stroke patients. Evid. Based Complement. Altern. Med. 2015, 2015, 164792. [Google Scholar] [CrossRef]
- Qiu, X.H.; Lu, S.K. Discussion on reinforcing-reducing manipulations of acupuncture in Internal Classic. Zhongguo Zhen Jiu 2009, 29, 850–853. [Google Scholar] [PubMed]
- Wang, L.; Jing, M.X.; Zhi, J.M.; Lu, J.; Wang, C.Y.; Liu, Q.G. Effects of reinforcing and reducing methods by twirling and rotating the needle on contents of CGRP and NO in rats with stress-induced hypertension. Zhongguo Zhen Jiu 2011, 31, 337–341. [Google Scholar] [PubMed]
- Fan, G.Q.; Zhao, Y.; Fu, Z.H. Acupuncture analgesia and the direction, angle and depth of needle insertion. Zhongguo Zhen Jiu 2010, 30, 965–968. [Google Scholar] [PubMed]
- Lu, L.; Zhang, X.G.; Zhong, L.L.; Chen, Z.X.; Li, Y.; Zheng, G.Q.; Bian, Z.X. Acupuncture for neurogenesis in experimental ischemic stroke: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 19521. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Roth, A.; Kuo, M.F.; Fischer, A.K.; Liebetanz, D.; Lang, N.; Tergau, F.; Paulus, W. Timing-dependent modulation of associative plasticity by general network excitability in the human motor cortex. J. Neurosci. 2007, 27, 3807–3812. [Google Scholar] [CrossRef]
- Rossi, C.; Sallustio, F.; Di Legge, S.; Stanzione, P.; Koch, G. Transcranial direct current stimulation of the affected hemisphere does not accelerate recovery of acute stroke patients. Eur. J. Neurol. 2013, 20, 202–204. [Google Scholar] [CrossRef]
- Zhang, L.; Xing, G.; Shuai, S.; Guo, Z.; Chen, H.; McClure, M.A.; Chen, X.; Mu, Q. Low-Frequency Repetitive Transcranial Magnetic Stimulation for Stroke-Induced Upper Limb Motor Deficit: A Meta-Analysis. Neural Plast. 2017, 2017, 2758097. [Google Scholar] [CrossRef]
- Kim, S.Y.; Shin, S.B.; Lee, S.J.; Kim, T.U.; Hyun, J.K. Factors associated with upper extremity functional recovery following low-frequency repetitive transcranial magnetic stimulation in stroke patients. Ann. Rehabil. Med. 2016, 40, 373–382. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, S.B.; Lee, K.W.; Kim, M.A.; Lee, S.J.; Choi, S.J. Factors associated with upper extremity motor recovery after repetitive transcranial magnetic stimulation in stroke patients. Ann. Rehabil. Med. 2015, 39, 268–276. [Google Scholar] [CrossRef][Green Version]
- Hoyer, E.H.; Celnik, P.A. Understanding and enhancing motor recovery after stroke using transcranial magnetic stimulation. Restor. Neurol. Neurosci. 2011, 29, 395–409. [Google Scholar] [CrossRef]


{kind=link}
| Time Point | Enrolment | Allocation | Post-Allocation | Close-Out | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Visit1 | Visit2~Visit6 | Visit7~Visit11 | Visit12~Visit16 | Visit17 | ||||||||||||||
| Week | 1 | 2 | 3 | |||||||||||||||
| Enrolment | ||||||||||||||||||
| Informed consent | X | |||||||||||||||||
| Demographic characteristics | X | |||||||||||||||||
| Medical history | X | |||||||||||||||||
| Vital signs | X | |||||||||||||||||
| Inclusion/exclusion criteria | X | |||||||||||||||||
| Random allocation | X | X | ||||||||||||||||
| Treatment |  | |||||||||||||||||
| Assessment | ||||||||||||||||||
| Change of medical history | X | X | X | |||||||||||||||
| Safety assessment | X | X | X | |||||||||||||||
| FMA | X | X | X | |||||||||||||||
| NIHSS | X | X | X | |||||||||||||||
| MBI | X | X | X | |||||||||||||||
| FIM | X | X | X | |||||||||||||||
| K-MMSE | X | X | ||||||||||||||||
| 9 HPT | X | X | X | |||||||||||||||
| ASHA-NOMS | X | X | ||||||||||||||||
| FAC | X | X | ||||||||||||||||
| EQ-5D | X | X | X | |||||||||||||||
| MAS | X | X | X | |||||||||||||||
| Hand grip strength test | X | X | X | |||||||||||||||
| MEP | X | X | X | |||||||||||||||
| mRS | X | X | X | X | ||||||||||||||
| Dependent Variables | Control Group (n = 12) | SA Group (n = 11) | rTMS Group (n = 8) | SAEM-CS Group (n = 11) | F or χ2 (p) |
|---|---|---|---|---|---|
| Mean (SD) or n (%) | Mean (SD) or n (%) | Mean (SD) or n (%) | Mean (SD) or n (%) | ||
| Age (y) | 62.17 (16.25) | 64.45 (14.75) | 67.00 (12.92) | 67.55 (12.53) | 84.69 (0.458) * |
| Sex (Male) | 7 (58.3%) | 7 (63.6%) | 5 (62.5%) | 4 (36.4%) | 2.11 (0.550) * |
| Hemiparesis (Lt side) | 8 (66.7%) | 5 (45.5%) | 5 (62.50%) | 7 (63.67%) | 1.26 (0.738) * |
| FMA Upper Extremity | 44.42 (26.57) | 26.18 (29.20) | 33.13 (19.40) | 42.64 (27.21) | 1.163 (0.337) † |
| FMA Lower Extremity | 19.33 (11.22) | 19.27 (8.97) | 19.63 (8.77) | 19.45 (12.89) | 0.01 (1.000) † |
| FMA Total | 63.75 (36.00) | 45.45 (36.05) | 52.75 (25.02) | 62.09 (39.03) | 0.66 (0.584) † |
| NIHSS | 3.50 (4.46) | 5.73 (3.77) | 5.13 (3.23) | 4.18 (4.77) | 0.62 (0.604) † |
| MBI | 65.58 (18.92) | 55.36 (23.08) | 41.63 (22.60) | 57.55 (30.27) | 1.60 (0.205) † |
| FIM | 93.83 (16.72) | 87.36 (21.46) | 75.38 (13.20) | 85.73 (35.99) | 0.96 (0.423) † |
| 9HPT | 93.65 (39.18) | 89.43 (42.73) | 108.75 (31.83) | 81.90 (42.01) | 0.73 (0.538) † |
| AHSA-NOMS | 6.83 (0.58) | 6.45 (0.93) | 5.38 (1.92) | 6.45 (0.82) | 3.00 (0.043) † |
| FAC | 2.08 (1.83) | 1.18 (1.78) | 1.38 (1.51) | 1.73 (1.68) | 0.60 (0.622) † |
| mRS | 3.08 (0.90) | 3.45 (0.69) | 3.63 (0.52) | 3.27 (0.79) | 0.95 (0.425) † |
| EQ-5D | 9.75 (2.73) | 9.73 (3.41) | 12.13 (1.64) | 10.09 (3.27) | 1.34 (0.275) † |
| K-MMSE | 26.42 (3.75) | 25.00 (4.56) | 26.13 (3.52) | 23.00 (4.29) | 1.56 (0.216) † |
| MAS elbow | 0.08 (0.29) | 0.45 (0.93) | 0.13 (0.35) | 0.27 (0.47) | 0.92 (0.442) † |
| MAS ankle | 0.25 (0.62) | 0.36 (0.67) | 0.00 (0.00) | 0.36 (0.50) | 0.87 (0.466) † |
| Grip test, dominant hand | 31.17 (18.15) | 27.91 (9.68) | 25.63 (13.74) | 20.55 (9.72) | 1.26 (0.302) † |
| Grip test, non-dominant hand | 13.50 (15.56) | 10.91 (16.18) | 6.50 (9.35) | 10.64 (10.27) | 0.43 (0.733) † |
| APB recording cortical stim latency | 11.83 (12.43) | 8.31 (11.56) | 9.45 (13.12) | 12.33 (11.86) | 0.27 (0.848) † |
| APB recording cortical stim amplitude | 258.33 (412.71) | 372.73 (567.00) | 188.00 (449.58) | 576.73 (781.20) | 0.89 (0.458) † |
| AH recording cortical stim latency | 22.68 (22.58) | 23.47 (22.63) | 20.53 (24.30) | 14.52 (20.20) | 0.37 (0.778) † |
| AH recording cortical stim amplitude | 294.50 (471.46) | 144.09 (181.25) | 201.63 (353.65) | 238.55 (362.56) | 0.35 (0.791) † |
| Groups | Dependent Variables | Week 0 (M ± SD) | Week 3 (M ± SD) | Week 7 (M ± SD) | Deference (W3-W0) | Deference (W7-W0) | χ2 (p) |
|---|---|---|---|---|---|---|---|
| Control group | FMA upper affected side | 44.42 ± 26.57 | 49.58 ± 24.33 | 50.25 ± 23.64 | 5.17 ± 10.53 | 5.83 ± 11.30 | 9.15 (0.010) |
| FMA lower affected side | 19.33 ± 11.22 | 24.50 ± 10.41 | 24.67 ± 10.19 | 5.17 ± 4.17 | 5.33 ± 6.40 | 8.83 (0.012) | |
| FMA total affected side | 63.75 ± 36.00 | 74.08 ± 33.22 | 74.92 ± 31.13 | 10.33 ± 12.87 | 11.17 ± 13.07 | 11.87(0.003) | |
| MBI | 65.58 ± 18.92 | 72.42 ± 23.19 | 81.50 ± 18.53 | 6.83 ± 13.16 | 15.92 ± 11.94 | 17.55 (<0.001) | |
| FIM | 93.83 ± 16.72 | 101.00 ± 20.53 | 107.33 ± 17.52 | 7.17 ± 13.54 | 13.50 ± 11.44 | 6.53 (0.038) | |
| 9HPT | 93.65 ± 39.18 | 66.59 ± 35.87 | 58.72 ± 38.28 | −27.06 ± 33.08 | −34.93 ± 37.61 | 12.67 (0.002) | |
| SA group | FMA upper affected side | 26.18 ± 29.20 | 35.27 ± 24.41 | 39.36 ± 25.24 | 9.09 ± 8.60 | 13.18 ± 15.72 | 14.00 (0.001) |
| FMA lower affected side | 19.27 ± 8.97 | 25.27 ± 10.11 | 24.55 ± 10.53 | 6.00 ± 4.67 | 5.27 ± 4.41 | 9.14(0.010) | |
| FMA total affected side | 45.45 ± 36.05 | 60.55 ± 32.15 | 63.91 ± 35.02 | 15.09 ± 11.89 | 18.45 ± 17.01 | 12.05 (0.002) | |
| NIHSS | 5.73 ± 3.77 | 3.09 ± 3.91 | 3.36 ± 4.08 | −2.64 ± 2.69 | −2.36 ± 2.46 | 9.56 (0.008) | |
| MBI | 55.36 ± 23.08 | 69.73 ± 29.07 | 74.00 ± 29.36 | 14.36 ± 11.74 | 18.64 ± 18.21 | 11.46 (0.003) | |
| FIM | 87.36 ± 21.46 | 98.00 ± 23.23 | 102.45 ± 23.70 | 10.64 ± 8.63 | 15.09 ± 15.12 | 10.369 (0.006) | |
| rTMS group | FMA upper affected side | 33.13 ± 19.40 | 50.13 ± 10.78 | 56.50 ± 9.70 | 17.00 ± 13.89 | 23.38 ± 14.70 | 13.61 (0.001) |
| FMA lower affected side | 19.63 ± 8.77 | 24.50 ± 5.86 | 28.25 ± 6.78 | 4.88 ± 6.49 | 8.63 ± 5.24 | 10.13 (0.006) | |
| FMA total affected side | 52.75 ± 25.02 | 74.63 ± 15.22 | 84.88 ± 14.24 | 21.88 ± 17.67 | 32.13 ± 17.27 | 12.25 (0.002) | |
| NIHSS | 5.13 ± 3.23 | 2.88 ± 2.36 | 2.00 ± 1.85 | −2.25 ± 1.75 | −3.13 ± 1.73 | 12.29 (0.002) | |
| MBI | 41.63 ± 22.60 | 67.38 ± 19.94 | 85.13 ± 11.68 | 25.75 ± 10.01 | 43.50 ± 16.64 | 15.55 (<0.001) | |
| FIM | 75.38 ± 13.20 | 97.75 ± 14.74 | 111.50 ± 8.49 | 22.38 ± 4.66 | 36.13 ± 6.88 | 15.55 (<0.001) | |
| 9HPT | 108.75 ± 31.83 | 83.30 ± 40.88 | 68.56 ± 37.29 | −25.45 ± 34.42 | −40.19 ± 35.61 | 11.27 (0.004) | |
| mRS | 3.63 ± 0.52 | 2.88 ± 1.36 | 2.63 ± 1.06 | −0.75 ± 1.16 | −1.00 ± 0.76 | 7.52 (0.023) | |
| EQ-5D | 12.13 ± 1.64 | 10.00 ± 2.45 | 9.13 ± 1.25 | 11.00 ± 2.27 | 10.13 ± 1.46 | 11.47 (0.003) | |
| APB recording cortical stim amplitude | 188.00 ± 449.58 | 297.75 ± 459.71 | 441.75 ± 416.07 | 109.75 ± 138.34 | 253.75 ± 573.24 | 6.35 (0.042) | |
| SAEM-CS group | FMA upper affected side | 42.64 ± 27.21 | 44.91 ± 27.72 | 47.64 ± 25.32 | 2.27 ± 7.28 | 5.00 ± 6.80 | 7.60 (0.022) |
| FMA lower affected side | 19.45 ± 12.89 | 23.64 ± 11.24 | 25.36 ± 10.57 | 4.18 ± 5.65 | 5.91 ± 6.50 | 10.07 (0.007) | |
| FMA total affected side | 62.09 ± 39.03 | 68.55 ± 38.39 | 73.00 ± 35.56 | 6.45 ± 12.11 | 10.91 ± 12.43 | 9.63 (0.008) | |
| MBI | 57.55 ± 30.27 | 73.09 ± 25.99 | 80.55 ± 27.19 | 15.55 ± 14.98 | 23.00 ± 16.12 | 17.05 (<0.001) | |
| FIM | 85.73 ± 35.99 | 101.64 ± 22.55 | 107.91 ± 23.36 | 15.91 ± 21.14 | 22.18 ± 20.84 | 16.60 (<0.001) | |
| 9HPT | 81.90 ± 42.01 | 63.19 ± 39.08 | 64.56 ± 45.76 | −18.70 ± 36.07 | −17.34 ± 51.43 | 7.00 (0.030) | |
| EQ-5D | 10.09 ± 3.27 | 9.00 ± 3.13 | 9.45 ± 3.70 | 9.73 ± 2.65 | 10.18 ± 3.19 | 7.40 (0.025) |
| Dependent Variables | Source of Variation | SS | df Mean Square | F | p | Significant | Scheffé Post hoc Test F (p) | ||
|---|---|---|---|---|---|---|---|---|---|
| W3-W0 | W7-W0 | ||||||||
| FMA upper extremity | Time | 3043.44 | 2 | 1521.72 | 31.91 | <0.001 | S | 3.68 (0.020) c > d | 4.32 (0.010) a < c > d |
| Group × Time | 1092.10 | 6 | 182.02 | 3.82 | 0.002 | S | |||
| FMA lower extremity | Time | 910.07 | 2 | 455.03 | 33.56 | <0.001 | S | 0.23 (0.875) | 0.66 (0.580 |
| Group × Time | 64.01 | 6 | 10.67 | 0.79 | 0.583 | NS | |||
| FMA total | Time | 7283.95 | 2 | 3641.97 | 47.61 | <0.001 | S | 2.27 (0.096) | 4.02 (0.014) a < c > d |
| Group × Time | 1446.48 | 6 | 241.08 | 3.15 | 0.008 | S | |||
| NIHSS | Time | 799.59 | 2 | 393.79 | 40.75 | <0.001 | S | 2.70 (0.059) | 2.57 (0.069) |
| Group × Time | 85.92 | 6 | 14.32 | 1.46 | 0.203 | NS | |||
| MBI | Time | 13,331.52 | 2 | 6665.76 | 75.70 | <0.001 | S | 3.51 (0.024) a < c | 5.58 (0.003) a < c, b < c |
| Group × Time | 2254.59 | 6 | 375.77 | 4.27 | 0.001 | S | |||
| FIM | Time | 9950.21 | 2 | 4975.11 | 59.62 | <0.001 | S | 2.17 (0.108) | 4.36 (0.010) a < c, b < c |
| Group × Time | 1533.92 | 6 | 255.65 | 3.06 | 0.010 | S | |||
| 9HPT | Time | 12,277.83 | 2 | 6318.91 | 14.98 | <0.001 | S | 1.63 (0.199) | 2.48 (0.076) |
| Group × Time | 533.35 | 6 | 889.73 | 2.17 | 0.055 | NS | |||
| mRS | Time | 10.69 | 2 | 5.35 | 7.71 | 0.001 | S | 0.62 (0.607) | 0.20 (0.897) |
| Group × Time | 1.55 | 6 | 0.26 | 0.37 | 0.894 | NS | |||
| EQ-5D | Time | 20.51 | 2 | 10.25 | 4.52 | 0.014 | S | 0.94 (0.429) | 1.00 (0.403) |
| Group × Time | 36.10 | 6 | 6.02 | 2.65 | 0.022 | S | |||
| MAS elbow | Time | 0.96 | 2 | 0.48 | 2.43 | 0.094 | NS | 0.95 (0.424) | 3.02 (0.041) |
| Group × Time | 1.65 | 6 | 0.28 | 1.40 | 0.226 | NS | |||
| MAS ankle | Time | 0.59 | 2 | 0.29 | 1.71 | 0.088 | NS | 1.38 (0.265) | 1.11 (0.357) |
| Group × Time | 1.18 | 6 | 0.20 | 1.15 | 0.345 | NS | |||
| Grip test, dominant hand | Time | 52.03 | 2 | 26.01 | 0.85 | 0.433 | NS | 1.10 (0.362) | 0.60 (0.619) |
| Group × Time | 152.97 | 6 | 25.50 | 0.83 | 0.550 | NS | |||
| Grip test, non-dominant hand | Time | 101.67 | 2 | 50.83 | 1.70 | 0.189 | NS | 0.34 (0.795) | 0.42 (0.742) |
| Group × Time | 106.96 | 6 | 17.83 | 0.60 | 0.732 | NS | |||
| APB recording cortical stim latency | Time | 234.74 | 2 | 117.37 | 3.07 | 0.052 | NS | 1.01 (0.401) | 2.37 (0.085) |
| Group × Time | 319.45 | 6 | 53.24 | 1.39 | 0.229 | NS | |||
| APB recording cortical stim amplitude | Time | 842,196.62 | 2 | 421,098.31 | 2.66 | 0.077 | NS | 2.08 (0.119) | 0.81 (0.495) |
| Group × Time | 186,621.834 | 6 | 301,103.64 | 1.90 | 0.092 | NS | |||
| AH recording cortical stim latency | Time | 130.68 | 2 | 66.34 | 0.40 | 0.670 | NS | 0.23 (0.873) | 0.68 (0.568) |
| Group × Time | 679.84 | 6 | 113.31 | 0.70 | 0.652 | NS | |||
| AH recording cortical stim amplitude | Time | 26,926.60 | 2 | 13,463.30 | 0.35 | 0.708 | NS | 1.10 (0.362) | 0.94 (0.430) |
| Group × Time | 254,560.64 | 6 | 42,426.77 | 1.094 | 0.374 | NS | |||
| Groups | FMAU p Value | FMAT p Value | MBI p Value | FIM p Value | EQ-5D p Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| w3-w0 | w7-w0 | w3-w0 | w7-w0 | w3-w0 | w7-w0 | w3-w0 | w7-w0 | w3-w0 | w7-w0 | |
| SA vs. Control | 0.419 | 0.494 | 0.281 | 0.459 | 0.109 | 0.666 | 0.497 | 0.758 | 0.292 | 0.171 |
| rTMS vs. Control | 0.069 | 0.015 | 0.153 | 0.023 | 0.005 | 0.002 | 0.030 | <0.001 | 0.318 | 0.666 |
| SAEM-CS vs. Control | 0.238 | 0.757 | 0.228 | 0.497 | 0.277 | 0.255 | 0.216 | 0.267 | 0.827 | 0.620 |
| SA vs. SAEM-CS | 0.050 | 0.197 | 0.087 | 0.236 | 0.646 | 0.669 | 0.921 | 0.693 | 0.286 | 0.336 |
| rTMS vs. SAEM-CS | 0.026 | 0.016 | 0.069 | 0.012 | 0.043 | 0.026 | 0.063 | 0.012 | 0.405 | 0.868 |
| SA vs. rTMS | 0.147 | 0.374 | 0.321 | 0.266 | 0.057 | 0.016 | 0.004 | 0.008 | 0.966 | 0.242 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Han, J.-Y.; Song, M.-K.; Park, G.-C.; Lee, J.-S. Synergistic Effects of Scalp Acupuncture and Repetitive Transcranial Magnetic Stimulation on Cerebral Infarction: A Randomized Controlled Pilot Trial. Brain Sci. 2020, 10, 87. https://doi.org/10.3390/brainsci10020087
Kim J-H, Han J-Y, Song M-K, Park G-C, Lee J-S. Synergistic Effects of Scalp Acupuncture and Repetitive Transcranial Magnetic Stimulation on Cerebral Infarction: A Randomized Controlled Pilot Trial. Brain Sciences. 2020; 10(2):87. https://doi.org/10.3390/brainsci10020087
Chicago/Turabian StyleKim, Jae-Hong, Jae-Young Han, Min-Keun Song, Gwang-Cheon Park, and Jeong-Soon Lee. 2020. "Synergistic Effects of Scalp Acupuncture and Repetitive Transcranial Magnetic Stimulation on Cerebral Infarction: A Randomized Controlled Pilot Trial" Brain Sciences 10, no. 2: 87. https://doi.org/10.3390/brainsci10020087
APA StyleKim, J.-H., Han, J.-Y., Song, M.-K., Park, G.-C., & Lee, J.-S. (2020). Synergistic Effects of Scalp Acupuncture and Repetitive Transcranial Magnetic Stimulation on Cerebral Infarction: A Randomized Controlled Pilot Trial. Brain Sciences, 10(2), 87. https://doi.org/10.3390/brainsci10020087