Plasma Levels of Occludin and Claudin-5 in Acute Stroke Are Correlated with the Type and Location of Stroke but Not with the Neurological State of Patients—Preliminary Data

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
- Their age at first-in-life stroke;
- The presence of comorbidities, such as atrial fibrillation (AF), arterial hypertension (AH), coronary artery disease (CAD), myocardial infarction (MI) in the last month, diabetes mellitus (DM), lipid disorders (LD), >70% atherosclerotic carotid artery stenosis (CAS, ipsilaterally to the acute ischemic brain lesion);
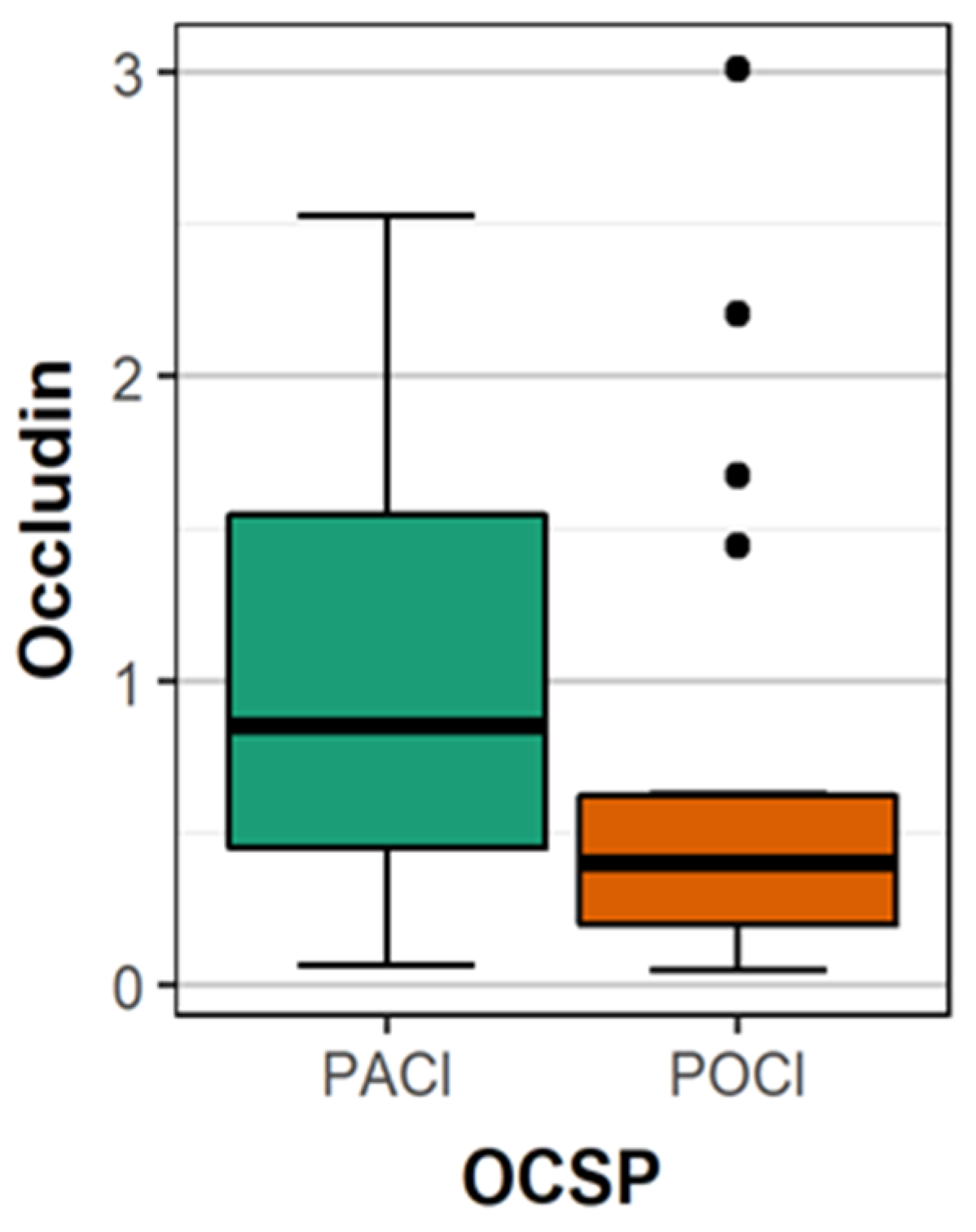
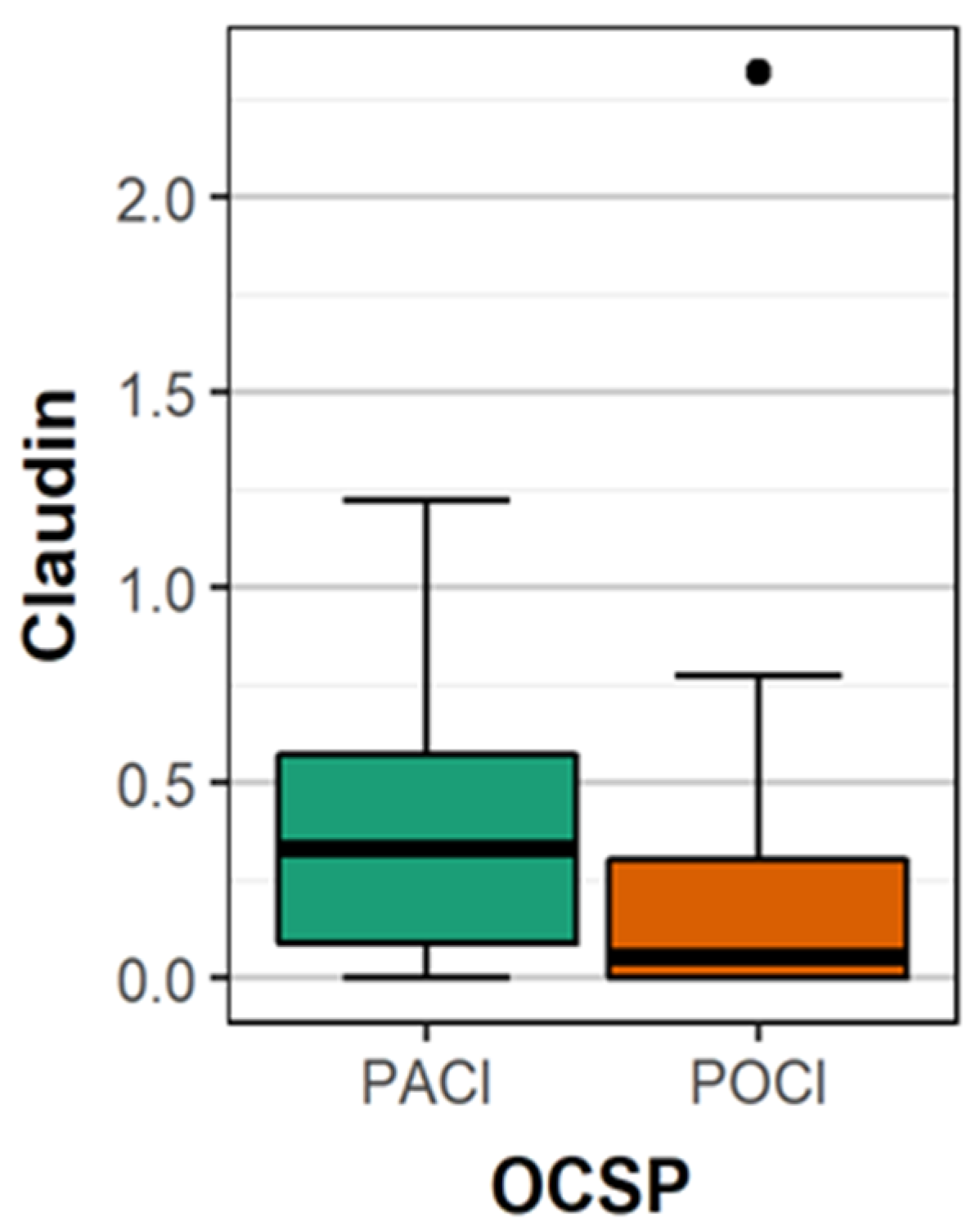
- Type of stroke using the Oxford Community Stroke Project classification (OCSP) [7];
- Treatment type on the first day of hospitalization (recombinant tissue plasminogen activator (rtPA), thrombectomy, no-reperfusion therapy (antiplatelet);
- Hemorrhagic transformation of infarct focus using the ECASS (European Cooperative Acute Stroke Study) scale [8];
- Their neurological status on the first day of stroke evaluated on the NIHSS (National Institute of Health Stroke Scale) [9];
- Plasma concentrations of the following markers on the first day of stroke: claudin-5, occludin, ZO-1;
- Their functional status on the ninth day following stroke onset according to the mRS scale [10].
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Liu, J.; Jin, X.; Liu, K.J.; Liu, W. Matrix metalloproteinase-2-mediated occludin degradation and caveolin-1-mediated claudin-5 redistribution contribute to blood-brain barrier damage in early ischemic stroke stage. J. Neurosci. 2012, 32, 3044–3057. [Google Scholar] [CrossRef] [PubMed]
- Jiao, H.; Wang, Z.; Liu, Y.; Wang, P.; Xue, Y. Specific role of tight junction proteins claudin-5, occludin, and ZO-1of the blood–brain barrier in a focal cerebral ischemic insult. J. Mol. Neurosci. 2011, 44, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Liang, W.; Lei, C.; Kinden, R.; Sang, H.; Xie, Y.; Huang, Y.; Qu, Y.; Xiong, L. Combination of HBO and memantine in focal cerebral ischemia: Is there a synergistic effect? Mol. Neurobiol. 2015, 52, 1458–1466. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Wang, X.; Yu, Z. Ischemia-reperfusion injury in the brain: Mechanisms and potential therapeutic strategies. Biochem. Pharmacol. 2016, 5, 213. [Google Scholar] [CrossRef]
- Pan, R.; Yu, K.; Weatherwax, T.; Zheng, H.; Liu, W.; Liu, K.J. Blood occludin level as a potential biomarker for early blood brain barrier damage following ischemic stroke. Sci. Rep. 2017, 7, 40331. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; Roig, H.; Rossich, R.; Martínez, E.; García-Eroles, L. Differences between hypertensive and non-hypertensive ischemic stroke. Eur. J. Neurol. 2004, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Moradiya, Y.; Janjua, N. Presentation and outcomes of “wake-up strokes” in a large randomized stroke trial: Analysis of data from the International Stroke Trial. J. Stroke Cerebrovasc. Dis. 2013, 22, 286–292. [Google Scholar] [CrossRef]
- Von Kummer, R.; Broderick, J.P.; Campbell, B.C.V.; Demchuk, A.; Goyal, M.; Hill, M.D.; Treurniet, K.M.; Majoie, C.B.L.M.; Marquering, H.A.; Mazya, M.V.; et al. The Heidelberg bleeding classification: Classification of Bleeding events after ischemic stroke and reperfusion therapy. Stroke 2015, 46, 2981–2986. [Google Scholar] [CrossRef]
- Young, F.B.; Weir, C.J.; Lees, K.R. GAIN international trial steering committee and investigators. Comparison of the National Institutes of Health Stroke Scale with disability outcome measures in acute stroke trials. Stroke 2005, 36, 2187–2192. [Google Scholar] [CrossRef]
- Weisscher, N.; Vermeulen, M.; Roos, Y.B.; de Haan, R.J. What should be defined as good outcome in stroke trials; A modified Rankin score of 0-1 or 0-2? J. Neurol. 2008, 255, 867–874. [Google Scholar] [CrossRef]
- Catapano, A.L.; Graham, I.; de Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. ESC Scientific document group. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef]
- Liakos, C.I.; Grassos, C.A.; Babalis, D.K. European Society of Hypertension, European Society of Cardiology. 2013 ESH/ESC guidelines for the management of arterial hypertension: What has changed in daily clinical practice? High Blood Press. Cardiovasc. Prev. 2015, 22, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Gionfriddo, M.R.; McCoy, R.G.; Lipska, K.J. The 2013 American Association of Clinical Endocrinologists’ diabetes mellitus management recommendations: Improvements needed. JAMA Intern. Med. 2014, 174, 179–180. [Google Scholar] [CrossRef]
- North American Symptomatic Carotid Endarterectomy Trial Collaborators; Barnett, H.J.M.; Taylor, D.W.; Haynes, R.B.; Sackett, D.L.; Peerless, S.J.; Ferguson, G.G.; Fox, A.J.; Rankin, R.N.; Hachinski, V.C.; et al. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N. Engl. J. Med. 1991, 325, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Milatz, S.; Krug, S.M.; Rosenthal, R.; Gunzel, D.; Muller, D.; Schulzke, J.; Amasheh, S.; Fromm, M. Claudin-3 acts as a sealing component of the tight junction for ions of either charge and uncharged solutes. Biochim. Biophys. Acta 2010, 1798, 2048–2057. [Google Scholar] [CrossRef]
- Kobayashi, K.; Kumura, H. Distinct behavior of claudin-3 and -4 around lactation period in mammary alveolus in mice. Histochem. Cell Biol. 2011, 136, 587–594. [Google Scholar] [CrossRef]
- Berndt, P.; Winkler, L.; Cording, J.; Breitkreuz-Korff, O.; Rex, A.; Dithmer, S.; Rausch, V.; Blasig, R.; Richter, M.; Sporbert, A.; et al. Tight junction proteins at the blood-brain barrier: Far more than claudin-5. Cell. Mol. Life Sci. 2019, 76, 1987–2002. [Google Scholar] [CrossRef]
- Ronaldson, P.T.; Demarco, K.M.; Sanchez-Covarrubias, L.; Solinsky, C.M.; Davis, T.P. Transforming growth factor-beta signalling alters substrate permeability and tight junction protein expression at the blood-brain barrier during inflammatory pain. J. Cereb. Blood Flow Metab. 2009, 29, 1084–1098. [Google Scholar] [CrossRef]
- Lochhead, J.J.; McCaffrey, G.; Quigley, C.E.; Finch, J.; DeMarco, K.M.; Nametz, N.; Davis, T.P. Oxidative stress increases blood-brain barrier permeability and induces alterations in occludin during hypoxia-reoxygenation. J. Cereb. Blood Flow Metab. 2010, 30, 1625–1636. [Google Scholar] [CrossRef]
- Cording, J.; Gunther, R.; Vigolo, E.; Tscheik, C.; Winkler, L.; Schlattner, I.; Lorenz, D.; Haseloff, R.F.; Schmidt-Ott, K.M.; Wolburg, H.; et al. Redox regulation of cell contacts by tricellulin and occludin: Redox-Sensitive cysteine sites in tricellulin regulate both tri- and bicellular junctions in tissue barriers as shown in hypoxia and ischemia. Antioxid. Redox Signal. 2015, 23, 1035–1049. [Google Scholar] [CrossRef]
- Bellmann, C.; Schreivogel, S.; Gunther, R.; Dabrowski, S.; Schumann, M.; Wolburg, H.; Blasig, I.E. Highly conserved cysteines are involved in the oligomerization of occludin-redox dependency of the second extracellular loop. Antioxid. Redox Signal. 2014, 20, 855–867. [Google Scholar] [CrossRef]
- Buschmann, M.M.; Shen, L.; Rajapakse, H.; Raleigh, D.R.; Wang, Y.; Wang, Y.; Lingaraju, A.; Zha, J.; Abbott, E.; McAuley, E.M.; et al. Occludin OCEL-domain interactions are required for maintenance and regulation of the tight junction barrier to macromolecular flux. Mol. Biol. Cell 2013, 24, 3056–3068. [Google Scholar] [CrossRef]
- Williams, D.W.; Calderon, T.M.; Lopez, L.; Carvallo-Torres, L.; Gaskill, P.J.; Eugenin, E.A.; Morgello, S.; Berman, J.W. Mechanisms of HIV entry into the CNS: Increased sensitivity of HIV infected CD14+CD16+ monocytes to CCL2 and key roles of CCR2, JAM-A, and ALCAM in diapedesis. PLoS ONE 2013, 8, e69270. [Google Scholar] [CrossRef]
- Sladojevic, N.; Stamatovic, S.M.; Keep, R.F.; Grailer, J.J.; Sarma, J.V.; Ward, P.A.; Andjelkovic, A.V. Inhibition of junctional adhesion molecule-A/LFA interaction attenuates leukocyte trafficking and inflammation in brain ischemia/reperfusion injury. Neurobiol. Dis. 2014, 67, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Fang, H.; Chen, Y.; Liang, S.; Zhu, Z.; Zeng, Q.; Li, J.; Xu, H.; Shao, B.; He, J.; et al. Idazoxan reduces blood-brain barrier damage during experimental autoimmune encephalomyelitis in mouse. Eur. J. Pharmacol. 2014, 736, 70–76. [Google Scholar] [CrossRef]
- Haarmann, A.; Deiss, A.; Prochaska, J.; Foerch, C.; Weksler, B.; Romero, I.; Couraud, P.O.; Stoll, G.; Rieckmann, P.; Buttmann, M. Evaluation of soluble junctional adhesion Molecule-A as a biomarker of human brain endothelial barrier breakdown. PLoS ONE 2010, 5, e13568. [Google Scholar] [CrossRef]
- Abbruscato, T.J.; Lopez, S.P.; Mark, K.S.; Hawkins, B.T.; Davis, T.P. Nicotine and cotinine modulate cerebral microvascular permeability and protein expression of ZO-1 through nicotinic acetylcholine receptors expressed on brain endothelial cells. J. Pharm. Sci. 2002, 91, 2525–2538. [Google Scholar] [CrossRef]
- Won, S.; Lee, J.H.; Wali, B.; Stein, D.G.; Sayeed, I. Progesterone attenuates hemorrhagic transformation after delayed tPA treatment in an experimental model of stroke in rats: Involvement of the VEGF–MMP pathway. J. Cereb. Blood Flow Metab. 2014, 34, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Haseloff, R.F.; Dithmer, S.; Winkler, L.; Wolburg, H.; Blasig, I.E. Transmembrane proteins of the tight junctions at the blood-brain barrier: Structural and functional aspects. Semin. Cell Dev. Biol. 2015, 38, 16–25. [Google Scholar] [CrossRef]
- Blasig, I.E.; Bellmann, C.; Cording, J.; Del Vecchio, G.; Zwanziger, D.; Huber, O.; Haselof, R.F. Occludin protein family: Oxidative stress and reducing conditions. Antioxid. Redox Signal. 2011, 15, 1195–1219. [Google Scholar] [CrossRef]
- Arboix, A.; Blanco-Rojas, L.; Martí-Vilalta, J. Advancements in understanding the mechanisms of symptomatic lacunar ischemic stroke: Translation of knowledge to prevention strategies. Expert Rev. Neurother. 2014, 261–276. [Google Scholar] [CrossRef]
- Fan, Y.; Yang, X.; Tao, Y.; Lan, L.; Zheng, L.; Sun, J. Tight junction disruption of blood-brain barrier in white matter lesions in chronic hypertensive rats. NeuroReport 2015, 26, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Kaur, J.; Tuor, U.I.; Zhao, Z.; Barber, P.A. Quantitative MRI reveals the elderly ischemic brain is susceptible to increased early blood-brain barrier permeability following tissue plasminogen activator related to claudin 5 and occludin disassembly. J. Cereb. Blood Flow Metab. 2011, 31, 1874–1885. [Google Scholar] [CrossRef]
- Kazmierski, R.; Michalak, S.; Wencel-Warot, A.; Nowinski, W.L. Serum tight-junction proteins predict hemorrhagic transformation in ischemic stroke patients. Neurology 2012, 79, 1677–1685. [Google Scholar] [CrossRef]
- Honda, M.; Nakagawa, S.; Hayashi, K.; Kitagawa, N.; Tsutsumi, K.; Nagata, I.; Niwa, M. Adrenomedullin improves the blood–brain barrier function through the expression of claudin-5. Cell. Mol. Neurobiol. 2006, 26, 109–118. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Group n = 88 |
|---|---|
| Age (years), mean ± SD [min, max] | 73.11 ± 11.48 |
| [36–103] | |
| Sex, F (n) | 42 (47.72%) |
| DM, n (%) | 22 (25%) |
| AH, n (%) | 68 (77.27%) |
| AF, n (%) | 31 (35.22%) |
| MI, n (%) | 6 (6.81%) |
| CAD, n (%) | 29 (32.95%) |
| CAS, n (%) | 11 (12.5%) |
| LD, n (%) | 55 (62.5%) |
| Location of stroke, n (%) | |
| TACI | 37 (42.04%) |
| PACI | 22 (25%) |
| LACI | 24 (27.27%) |
| POCI | 5 (5.68%) |
| NIHSS, median (IQR) | 3 (5) |
| [min, max] | [0–29] |
| Therapy, n (%) | |
| rtPA | 22 (25%) |
| MT | 8 (9.09%) |
| no reperfusion therapy | 58 (65.9%) |
| ECASS classification, | |
| n (%) | |
| HI1 | 4 (4.54) |
| PH2 | 2 (2.27) |
| mRS, median (IQR) | 2 (4) |
| [min, max] | [0–6] |
| Parameter | ICA Supply | VA Supply | p |
|---|---|---|---|
| occludin (ng/mL) | 1.036 | 0.660 | 0.009 |
| claudin 5 (ng/mL) | 0.373 | 0.249 | 0.011 |
| zonulin (ng/mL) | 0.693 | 0.236 | 0.105 |
| Parameter | lacunar Stroke | Non-Lacunar Stroke | p |
|---|---|---|---|
| occludin (ng/ml) | 0.708 | 1.028 | 0.026 |
| claudin 5 (ng/ml) | 0.293 | 0.359 | 0.128 |
| zonulin (ng/ml) | 0.249 | 0.704 | 0.102 |
| Parameter/ NIHSS | NIHSS (A) 0–4 n = 48 | NIHSS (B) 5–12 n = 20 | NIHSS (C) >12 n = 20 | NIHSS A vs. B; p | NIHSS B vs. C; p | NIHSS A vs. C; p |
|---|---|---|---|---|---|---|
| occludin (ng/mL) | 1.002 | 0.717 | 0.955 | 0.261 | 0.580 | 0.909 |
| claudin 5 (ng/mL) | 0.378 | 0.265 | 0.283 | 0.625 | 0.903 | 0.625 |
| zonulin (ng/mL) | 0.492 | 0.596 | 0.875 | 0.904 | 0.914 | 0.939 |
| Parameter/mRS | mRS 0–2 n = 51 | mRS 3–6 n = 37 | p |
|---|---|---|---|
| occludin (ng/mL) | 0.984 | 0.799 | 0.503 |
| claudin 5 (ng/mL) | 0.304 | 0.454 | 0.618 |
| Zonulin (ng/mL) | 0.404 | 0.812 | 0.183 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lasek-Bal, A.; Kokot, A.; Gendosz de Carrillo, D.; Student, S.; Pawletko, K.; Krzan, A.; Puz, P.; Bal, W.; Jędrzejowska-Szypułka, H. Plasma Levels of Occludin and Claudin-5 in Acute Stroke Are Correlated with the Type and Location of Stroke but Not with the Neurological State of Patients—Preliminary Data. Brain Sci. 2020, 10, 831. https://doi.org/10.3390/brainsci10110831
Lasek-Bal A, Kokot A, Gendosz de Carrillo D, Student S, Pawletko K, Krzan A, Puz P, Bal W, Jędrzejowska-Szypułka H. Plasma Levels of Occludin and Claudin-5 in Acute Stroke Are Correlated with the Type and Location of Stroke but Not with the Neurological State of Patients—Preliminary Data. Brain Sciences. 2020; 10(11):831. https://doi.org/10.3390/brainsci10110831
Chicago/Turabian StyleLasek-Bal, Anetta, Anna Kokot, Daria Gendosz de Carrillo, Sebastian Student, Katarzyna Pawletko, Aleksandra Krzan, Przemysław Puz, Wiesław Bal, and Halina Jędrzejowska-Szypułka. 2020. "Plasma Levels of Occludin and Claudin-5 in Acute Stroke Are Correlated with the Type and Location of Stroke but Not with the Neurological State of Patients—Preliminary Data" Brain Sciences 10, no. 11: 831. https://doi.org/10.3390/brainsci10110831
APA StyleLasek-Bal, A., Kokot, A., Gendosz de Carrillo, D., Student, S., Pawletko, K., Krzan, A., Puz, P., Bal, W., & Jędrzejowska-Szypułka, H. (2020). Plasma Levels of Occludin and Claudin-5 in Acute Stroke Are Correlated with the Type and Location of Stroke but Not with the Neurological State of Patients—Preliminary Data. Brain Sciences, 10(11), 831. https://doi.org/10.3390/brainsci10110831