Statistical Permutation Test Reveals Progressive and Region-Specific Iron Accumulation in the Thalami of Children with Aspartylglucosaminuria



Abstract
:1. Introduction
2. Materials and Methods
2.1. MRI Acquisition
2.2. Image Registration and Segmentation of Thalamic Volume
2.3. Permutation Test-Based Location of the Iron Accumulation Regions
2.4. Statistical Analysis
3. Results
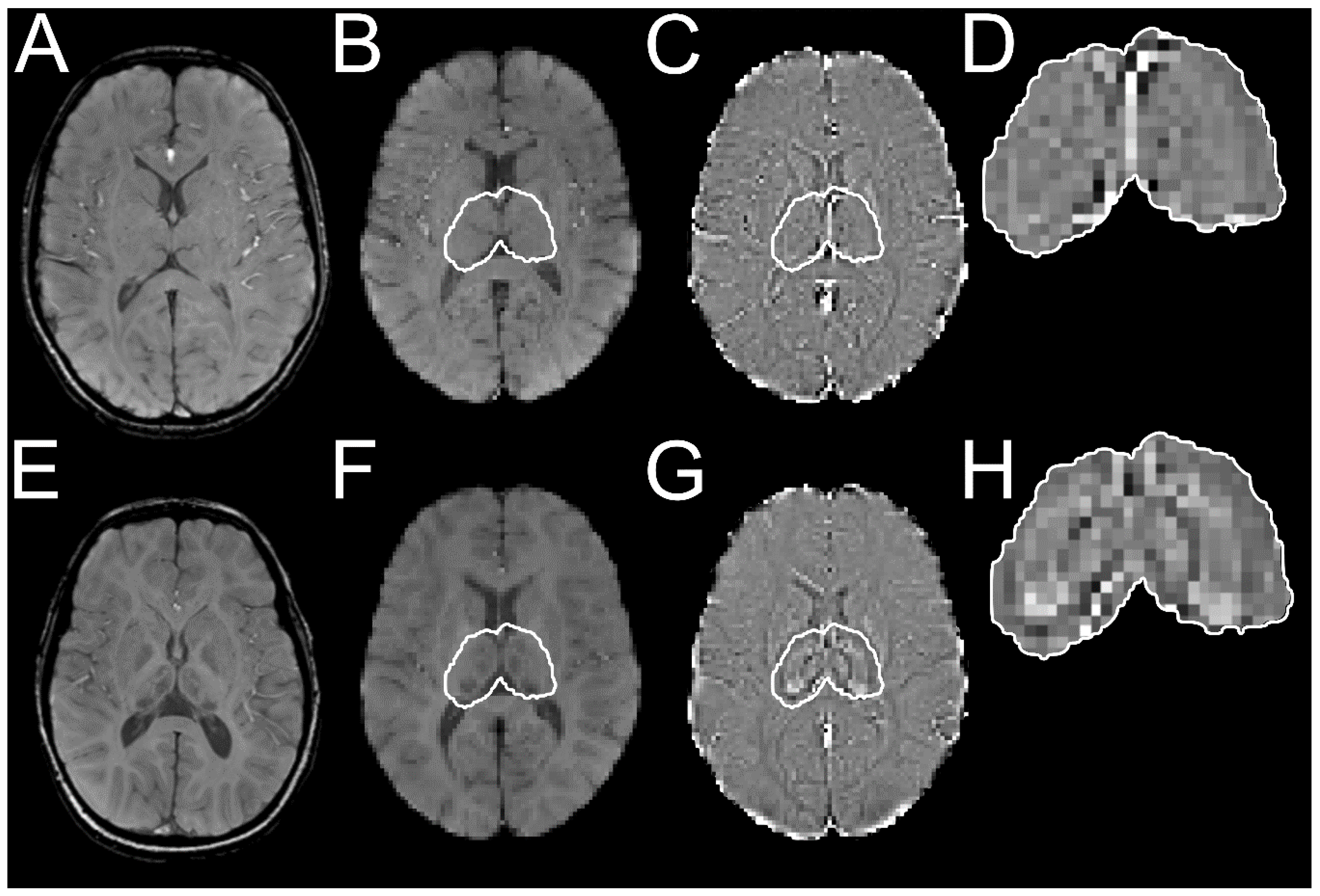
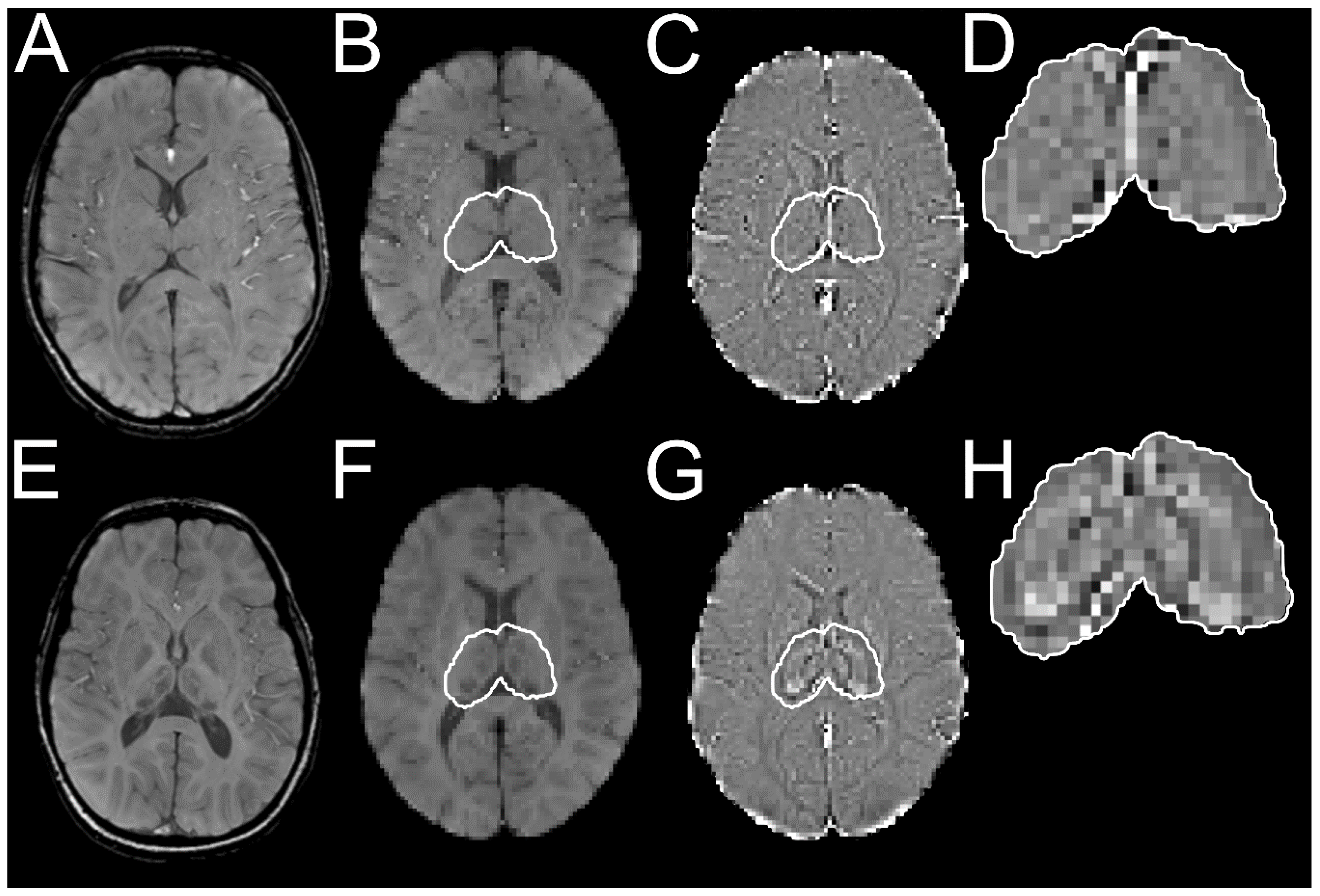
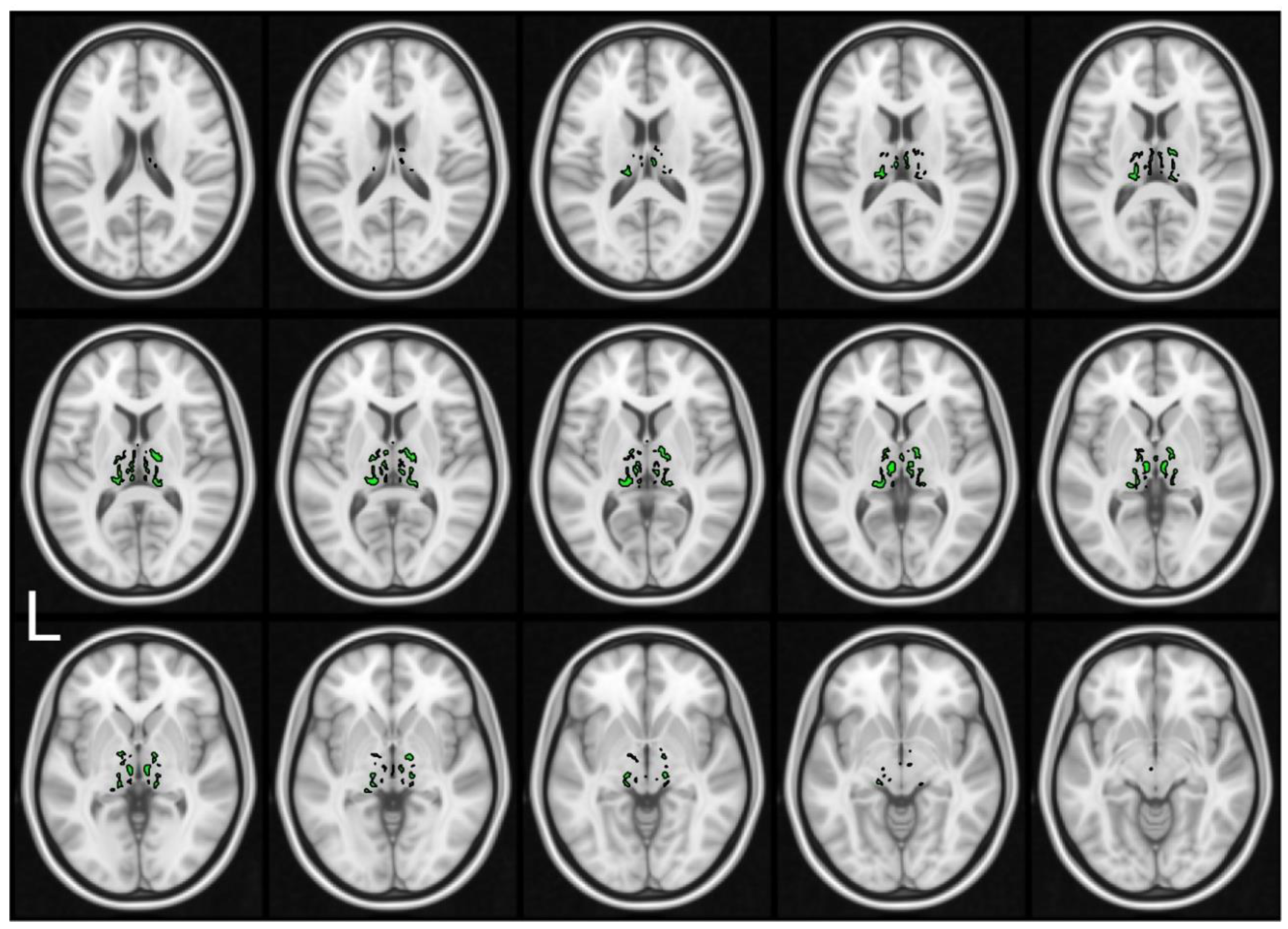
3.1. Segmentation and Permutation Test to the Locate Iron Accumulation Regions
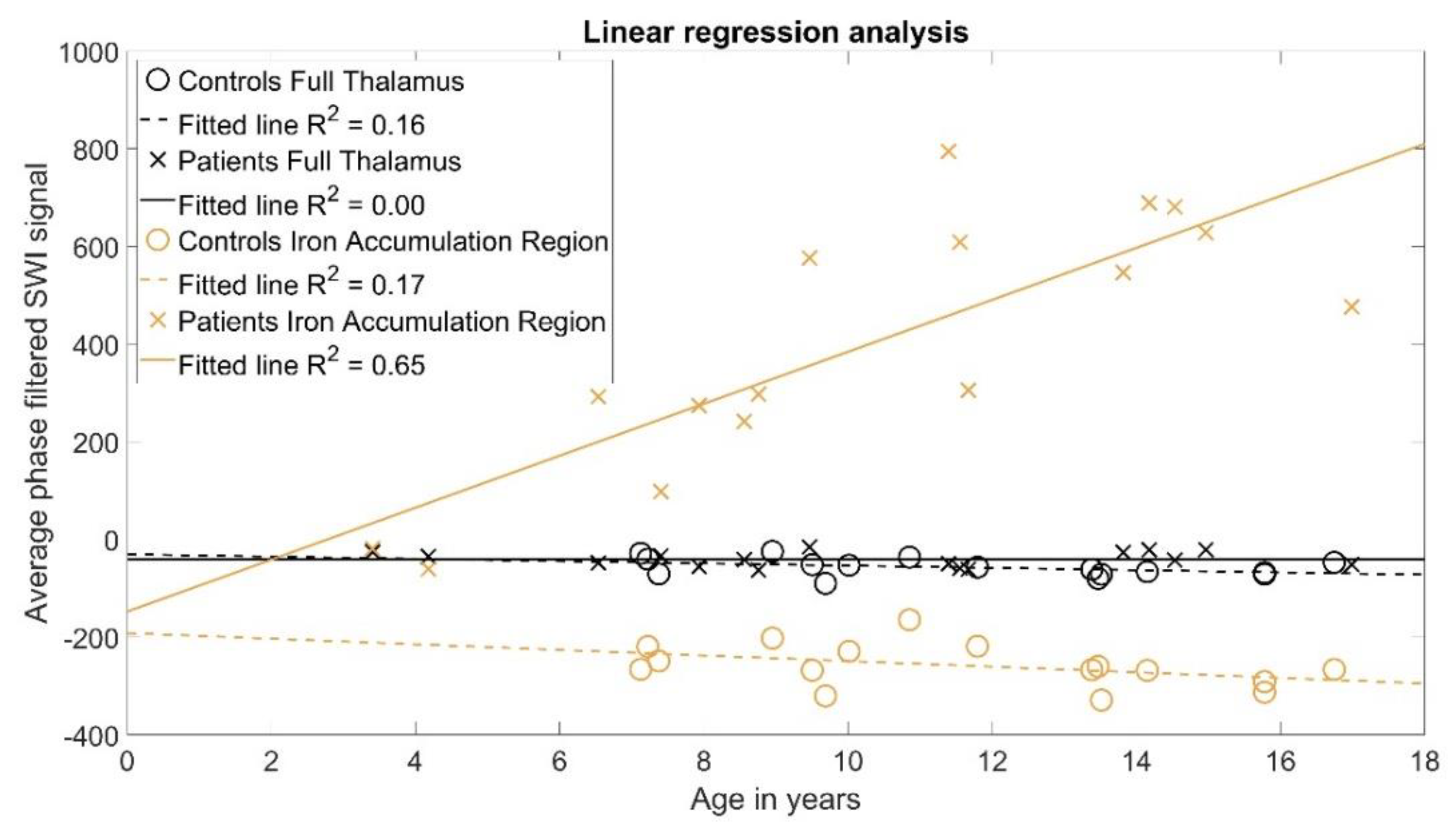
3.2. Statistical Analysis
4. Discussion
Limitations of This Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tokola, A.; Laine, M.; Tikkanen, R.; Autti, T. Susceptibility-weighted imaging findings in aspartylglucosaminuria. Am. J. Neuroradiol. 2019, 40, 1850–1854. [Google Scholar] [CrossRef] [PubMed]
- Arvio, M.; Mononen, I. Aspartylglycosaminuria: A review. Orphanet J. Rare Dis. 2016, 11, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harjunen, E.L.; Laine, M.; Tikkanen, R.; Helenius, P. Detailed profile of cognitive dysfunction in children with aspartylglucosaminuria. J. Inherit. Metab. Dis. 2020, 43, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Saarela, J. Molecular pathogenesis of a disease: Structural consequences of aspartylglucosaminuria mutations. Hum. Mol. Genet. 2001, 10, 983–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banning, A.; Gülec, C.; Rouvinen, J.; Gray, S.J.; Tikkanen, R. Identification of Small Molecule Compounds for Pharmacological Chaperone Therapy of Aspartylglucosaminuria. Sci. Rep. 2016, 6, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunder, U.; Valtonen, P.; Kelo, E.; Mononen, I. Early initiation of enzyme replacement therapy improves metabolic correction in the brain tissue of aspartylglycosaminuria mice. J. Inherit. Metab. Dis. 2010, 33, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Virta, S.; Rapola, J.; Jalanko, A.; Laine, M. Use of nonviral promoters in adenovirus-mediated gene therapy: Reduction of lysosomal storage in the aspartylglucosaminuria mouse. J. Gene Med. 2006, 8, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Banning, A.; Schiff, M.; Tikkanen, R. Amlexanox provides a potential therapy for nonsense mutations in the lysosomal storage disorder Aspartylglucosaminuria. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Bras, J.M. Lysosomal Storage Disorders and Iron. In International Review of Neurobiology; Academic Press Inc.: Cambridge, MA, USA, 2013; Volume 110, pp. 251–275. [Google Scholar]
- Sehgal, V.; Delproposto, Z.; Haacke, E.M.; Tong, K.A.; Wycliffe, N.; Kido, D.K.; Xu, Y.; Neelavalli, J.; Haddar, D.; Reichenbach, J.R. Clinical applications of neuroimaging with susceptibility-weighted imaging. J. Magn. Reson. Imaging 2005, 22, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Haacke, E.M.; Xu, Y.; Cheng, Y.C.N.; Reichenbach, J.R. Susceptibility weighted imaging (SWI). Magn. Reson. Med. 2004, 52, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Ropele, S.; Enzinger, C.; Fazekas, F. Iron Mapping in Multiple Sclerosis. Neuroimaging Clin. N. Am. 2017, 27, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Halefoglu, A.M.; Yousem, D.M. Susceptibility weighted imaging: Clinical applications and future directions. World J. Radiol. 2018, 10, 30–45. [Google Scholar] [CrossRef] [PubMed]
- Haacke, E.M.; Makki, M.; Ge, Y.; Maheshwari, M.; Sehgal, V.; Hu, J.; Selvan, M.; Wu, Z.; Latif, Z.; Xuan, Y.; et al. Characterizing iron deposition in multiple sclerosis lesions using susceptibility weighted imaging. J. Magn. Reson. Imaging 2009, 29, 537–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avants, B.B.; Tustison, N.; Johnson, H. Advanced Normalization Tools (ANTS) Release 2.x. Insight J. 2009, 2, 1–35. [Google Scholar]
- Haacke, E.M.; Mittal, S.; Wu, Z.; Neelavalli, J.; Cheng, Y.-C.N. Susceptibility-Weighted Imaging: Technical Aspects and Clinical Applications, part 1. AJNR Am. J. Neuroradiol 2009, 30, 19–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.M.; Nichols, T.E. Threshold-free cluster enhancement: Addressing problems of smoothing, threshold dependence and localisation in cluster inference. Neuroimage 2009, 44, 83–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najdenovska, E.; Alemán-Gómez, Y.; Battistella, G.; Descoteaux, M.; Hagmann, P.; Jacquemont, S.; Maeder, P.; Thiran, J.P.; Fornari, E.; Cuadra, M.B. In-vivo probabilistic atlas of human thalamic nuclei based on diffusion-weighted magnetic resonance imaging. Sci. Data 2018, 5, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iglesias, J.E.; Insausti, R.; Lerma-Usabiaga, G.; Bocchetta, M.; Van Leemput, K.; Greve, D.N.; van der Kouwe, A.; Fischl, B.; Caballero-Gaudes, C.; Paz-Alonso, P.M. A probabilistic atlas of the human thalamic nuclei combining ex vivo MRI and histology. Neuroimage 2018, 183, 314–326. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| (A). Multivariate regression coefficients f(x) = A × x + b | |||||
| Estimate | Std. Err. | T | p-Value | ||
| Intercept b | −35.38 | 10.15 | −3.49 | <0.01 | |
| Δb Controls | +4.86 | 10.15 | +0.48 | 0.64 | |
| Δb Patients with AGU | −4.86 | 10.15 | −0.48 | 0.64 | |
| Slope a | −1.17 | 0.87 | −1.34 | 0.19 | |
| Δa Controls | −1.14 | 0.87 | −1.30 | 0.20 | |
| Δa Patients with AGU | +1.14 | 0.87 | +1.30 | 0.20 | |
| (B).Analysis of Covariance | |||||
| df | Sum. sq. | Mean sq. | F | p-Value | |
| Group | 1 | 1861.50 | 1861.50 | 6.56 | 0.02 |
| Age | 1 | 338.20 | 338.20 | 1.19 | 0.28 |
| Group × Age | 1 | 480.74 | 480.74 | 1.69 | 0.20 |
| Error | 28 | 7945.12 | 283.75 | ||
| A. Multivariate Regression Coefficients f(x) = a × x + b | |||||
| Estimate | Std. Err. | T | p-Value | ||
| Intercept b | −169.77 | 70.22 | −2.42 | 0.02 | |
| Δb Controls | −22.02 | 70.22 | −0.31 | 0.76 | |
| Δb Patients with AGU | +22.02 | 70.22 | +0.31 | 0.76 | |
| Slope a | 23.73 | 6.04 | 3.93 | <0.01 | |
| Δa Controls | −29.46 | 6.04 | −4.87 | <0.01 | |
| Δa Patients with AGU | +29.46 | 6.04 | +4.87 | <0.01 | |
| B.Analysis of Covariance | |||||
| df | Sum. sq. | Mean sq. | F | p-Value | |
| Group | 1 | 3,771,650.55 | 3,771,650.55 | 277.69 | <0.01 |
| Age | 1 | 349,463.43 | 349,463.43 | 25.73 | <0.01 |
| Group × Age | 1 | 322,764.71 | 322,764.71 | 23.76 | <0.01 |
| Error | 28 | 380,303.90 | 13,582.28 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sairanen, V.; Tokola, A.; Tikkanen, R.; Laine, M.; Autti, T. Statistical Permutation Test Reveals Progressive and Region-Specific Iron Accumulation in the Thalami of Children with Aspartylglucosaminuria. Brain Sci. 2020, 10, 677. https://doi.org/10.3390/brainsci10100677
Sairanen V, Tokola A, Tikkanen R, Laine M, Autti T. Statistical Permutation Test Reveals Progressive and Region-Specific Iron Accumulation in the Thalami of Children with Aspartylglucosaminuria. Brain Sciences. 2020; 10(10):677. https://doi.org/10.3390/brainsci10100677
Chicago/Turabian StyleSairanen, Viljami, Anna Tokola, Ritva Tikkanen, Minna Laine, and Taina Autti. 2020. "Statistical Permutation Test Reveals Progressive and Region-Specific Iron Accumulation in the Thalami of Children with Aspartylglucosaminuria" Brain Sciences 10, no. 10: 677. https://doi.org/10.3390/brainsci10100677
APA StyleSairanen, V., Tokola, A., Tikkanen, R., Laine, M., & Autti, T. (2020). Statistical Permutation Test Reveals Progressive and Region-Specific Iron Accumulation in the Thalami of Children with Aspartylglucosaminuria. Brain Sciences, 10(10), 677. https://doi.org/10.3390/brainsci10100677