1. Introduction
Lateral subluxation often results from abnormal soft tissue around the patella which may cause anterior knee pain or pain around the tibia, causing cartilage wear in the long term which further leads to joint hardening, deformation, and necrosis—which are common diseases in orthopedics and sports medicine clinics [
1]. Symptoms of patellar lateral subluxation arise due to the outward shifting of the patella, causing inflammation or discomfort in the knee joint of the patient. Cook et al. and many others have studied how to accurately diagnose and treat patellar lateral subluxation at an early stage in order to avoid the deterioration of the disease [
2]. In the clinical diagnosis, the test of patellar subluxation included the tracking path, contraction, muscle strength, palpation, and X-ray [
3].
The patella is located on the femur and humerus. While the knee is bending or straightening, the patella will move in a fixed tracking path. While the quadriceps are contracting, the hamstrings should be relaxed to straighten the knee. While the hamstrings are contracting, it is difficult to make the knee be straightened. The pressure of the cartilaginous joint also increased, leading to the knee pain. Vastus lateralis (VL) and VMO will not be balanced due to the reduced exercises and greater fatigue. The reduced exercises and greater fatigue also caused the problem of activation timing. The problem of activation timing might not be caused by insufficient VMO. Instead, it may be caused by the latter activation contraction and faster external activation contraction. Hence, the iliotibial band will be contracted. The medial muscle ligament will be weak. The patellar lateral tilt deteriorated. The cartilage pressure, the friction of cartilage, and the inflammation of cartilage all will deteriorate. The variation of fascia tension will change the tracking path of patella to lead to the friction and pain of the surrounding area. In the patellofemoral pain syndrome, PFPS, the patellar subluxation and the chondromalacia patella are often explored. In general, the training of quadriceps and the medial muscle could reduce the loading of the knee for rehabilitation. The training of medial muscle could enhance the tension of quadriceps in the upper side of the kneecap to reduce the incorrect action of the kneecap.
On the lower limb biomechanics, due to the muscle imbalance of VMO and VL on the quadriceps femoris muscle, the VMO on the quadriceps femoris muscle will be too weak or the outer structure of the iliotibial band will be too tight. Treatment methods for patellar lateral subluxation include physical therapy, medication, surgery, and orthodontic appliance. In principle, physiotherapy is the main focus and emphasizes strengthening the VMO or soothing the VL on the quadriceps femoris muscle. Ronald P. et al. attempted and aimed to reinforce quadriceps femoris muscle’s VMO to relieve the discomfort associated with patellar lateral subluxation [
4]. In [
5], it aimed to assess muscular activations of gluteus medius muscles, VMO, and VML, in electromyographic analysis during external rotator movements and hip abduction. It also aims to open and closed kinetic chain knee extension movements.
In [
6], the aim was to analyze surface electromyographic (SEMG) responses for biceps femoris (BF), rectus femoris (RF), VMO, and VL, as well as the VMO:VL ratio during an open-kinetic chain 45° angled leg press (LP45). The traditional LP45 technique was compared with 2 alternative LP45 exercise techniques that used a physioball and elastic band, respectively. Therefore, practitioners should consider placing a physioball between the knees during LP45 exercise as another technique when greater overall quadriceps activity is desired for the muscle strengthening program or clinical rehabilitation.
In [
7], the lower extremity injuries of the knee joint are affected by the excessive valgus and varus force. The corresponding rehabilitation and conditioning programs are often applied. As same as [
6], it also investigated LP45 by physioball and elastic band with submaximal loads on EMG amplitude and fatigue indices. Higher levels of CRMS (Coefficient of Root Mean Square) and Cf5 were noted for RF muscles, VL, and VM, respectively. It showed that both physioball and elastic band could be adopted to reduce excessive varus and valgus forces during leg press. It may increase quadriceps activation and improving the knee joint stabilization.
In [
6,
7], it sought to investigate the effect of performing leg press (LP) 45 degrees using a physioball and elastic band to reduce excessive varus and valgus forces, to increase quadriceps activation and improve knee joint stabilization. The use of surface electromyography is a widely accepted technique for measuring the electrical signals produced by muscle contractions and estimating the strength of muscle. It is suitable to apply in sports medicine research [
8]. The surface electromyogram is a general technology that is used to measure muscle strength by measuring the electric signal of muscle contraction. It is also applied for sport medicine.
Integrated Haptic Feedback (IHF) provided an over-ground gait training regimen for post-stroke ambulatory subjects. The effects of IHF system was trailed by six post-stroke ambulatory individuals in walking. It indicated that patients' body sway was not disturbed under the faster walking. Hence, IHF system was a valuable tool to assist physical therapist in gait rehabilitation of post-stroke individuals. Both using kinesthetic and tactile cues for the post-stroke gait rehabilitation is a novel concept. The symmetry, balance and muscle activation patterns imply that integration of haptic cues may benefit post-stroke gait rehabilitation to improve the symmetry and muscle activity simultaneously [
9,
10]. At present, most of the clinical examination methods use palpation or X-ray image to diagnose the positions of the patella and femur as well as to determine the cause of patellar lateral subluxation, and then finally decide whether surgery or non-surgical treatment is to be adopted. Cases like patella dysplasia, defects of femoral sulcus and femoral condyle, may be based on surgical treatment, while non-surgical treatments mainly consider strengthening the VMO of the quadriceps femoris muscle and protecting the patella [
11]. Understanding the VMO and VL muscle contraction patterns can improve rehabilitation actions and overall rehabilitation effects [
12].
Medical research attempting to find an effective treatment for the patellofemoral malalignment has found that kicking forward action could trigger a higher VMO, and therefore it became an effective treatment that helps patients to alleviate their symptoms [
13,
14]. Since the goosestep does not fit the ergonomics to hurt the brain due to the heel on the ground violently, the goosestep could not be used for patients. In order to compare the effects of the triggering time of VMO and VL on patellofemoral pain syndrome, observe the difference of muscle time under different movements and find the optimal relationship between VMO and VL, the study of Neptune RR. et al. showed that if the VMO nerve trigger time was reduced or was inappropriately five milliseconds later than that of the VL, it might result in significant lateral movement of the patella affecting the patella joint [
15].
In [
16], the presence of anterior knee pain (AKP) is a delay in the recruitment of VMO relative to VL. However, much fewer literature was regarding the recruitment of VMO within the AKP population. Both the systematic review and meta-analysis are only to examine the relative timing of onset for VMO and VL with AKP compared with the asymptomatic population. However, some patients with AKP may not have a VMO-VL dysfunction. Therefore, it is difficult for the clinical treatment.
In [
17], the temporal recruitment of VMO was compared with the one of VL during voluntary ankle movements and perturbed standing with patellofemoral pain. Elton C.T. et al. examined the trigger time difference between patient’s VMO and VL under active and passive motions. The effects of different reflex and voluntary postural exercise were determined for VMO facilitation. The unexpected perturbation activities are for facilitating VMO activation. Hence, the clinical rehabilitation exercise programs and the underlying mechanisms are needed for the further investigation.
Chester R. et al. showed that comparing the contraction time of patient’s VMO and VL, the time of VMO was more delayed. Such a change in trigger time might be due to fatigue, the inhibition or reflection of nerve conduction velocity and motor neurons [
16]. Elton C.T. et al. examined the trigger time difference between patient’s VMO and VL under active and passive motions. The results showed that the reflection contraction caused by disturbance could reverse the trigger time difference, while the earlier VMO contraction could prevent the lateral patella trajectory and protect the patella joints [
17]. On comparing the relationship between VMO and VL, Tang Z. et al.’s study used a Cybex Norm dynamometer, and the results showed that patients with patellar lateral subluxation or subluxation had a trend toward lower VMO. This study speculated that higher isokinetic exercise might improve patellar lateral subluxation [
18].
In the clinical examination, the patellar subluxation is determined to be surgically treated or not based on the position of patella and femur from palpation or an X-ray image. Once the patella experiences dysplasia symptoms, such as the defect of femoral groove and the defect of femoral condyle, the patellar subluxation may need surgical treatment. However, some research on the patellar subluxation without the surgical treatment addressed this by enhancing the quadriceps femoris muscle or protecting the patella to understand the contraction mode of VMO and VL. Hence, these methods could improve the rehabilitation [
11,
12].
The purpose of this study was to develop an evaluation system that could prospectively explore which posture of kick training could enhance the muscle strength of VMO, and thus improve the anterior knee pain or pain around the patella caused by patellar lateral subluxation.
This paper aims to investigate a pilot study for improving the dislocation of knee-cap problem by increasing the medial muscle strength. By calculating the relationship between the medial muscle strength and the external muscle strength from electromyography, it aims to indicate that the medial muscle strength could be increased by kicking actions. Moreover, it evaluated the medial muscle strength by kicking actions between the standing and sitting postures. Finally, we will continue to increase the number of patients, the range of clinical pathology, the number of research items to prove our proposal and the equipment that could be used for evaluating the medial muscle strength by kick training between the standing and sitting postures.
2. Methods
2.1. Experimental Design
The purpose of this paper is to assess the feasibility of developing hardware and software systems for enhancing the strength of VMO on the quadriceps femoris muscle. Assessment of the medical effectiveness is not within the scope of this research. The study was conducted with informed consent and improved on the training methods of previous studies [
19]. The main targets were college students or postgraduates and general office workers. The ratio of male and female participants was 45 to 38. The age ranged from 20 to 50 years old. All of them were normal people without a medical history of knee joints, and they all had no movement disorders in daily life or in exercise. The muscle data were collected from July to December in 2017. To ensure the consistency of the muscle data, all of the subjects do not have any medical history of knee joints and lower limb. Moreover, they have no movement disorders in daily life or in exercise.
The detection action involved walking, standing, and sitting. The angle of kicking was from 10 to 90 degrees. We calculated the average value with 6 same actions, where the angle of each action is 10 degrees. Subject needed to relax the muscle to avoid the noise signal while the subject is kicking the leg. After kicking the leg, the angle of calf needed to be vertical to the ground and then the knee needed to be straightened to press on the toes. The strength of kicking must be the same. The detection action consisted of normal gait, sitting posture and standing posture, in which the angle of the lifting leg was 10°–90° and the movement was performed every 10°. Each movement was repeated 6 times and the average value was then taken. When performing kick-lifting, subjects must keep their muscles relaxed to prevent noise from affecting the signal quality, and the legs should be relaxed and perpendicular to the ground after extending the legs to the set angle and extended to the movement of swinging kick. The toes should be pressed down when kicking out until the knees are straight. The strength of the kicking process must be consistent and sudden change must be avoided.
2.2. Measurement Module
The sensing module for signals of muscle force and angle was conducted by two sets of EMG sensors and nine-axis sensors, which then transmitted the collected data to the back-end computer directly or via Bluetooth communication through a microcontroller for signal recording and analysis in
Figure 1. The signal processing module mainly processed by EMG signal, and the collected data were processed by software programs written from the LabVIEW (National Instruments, Austin, TX, USA) for digital filtering, full-wave rectification, and normalization, which would be used for subsequent analysis. The data analysis and evaluation were used to interpret the required index parameters of the signal analysis, and then presented in a graphical user interface (GUI) to provide feedback for doctors and subjects and to help understand the current state.
The system used an Arduino UNO (HAOYU Electronics, Shenzhen, China) development board as a microcontroller unit (MCU). This platform adopted the ATmega series, which is equipped with a multi-channel Analog-to-Digital Converter (ADC) with a 10-bit resolution conversion voltage value, combined with the EMG signal sensing module to convert the voltage, displayed with 0–1023 integer. After referring to the sampling frequency of EMG myoelectric signal frequency band that concentrated at 20–400 Hz [
20], the sampling frequency of this study was set to 1 kHz in order to meet the data acquisition requirements.
The EMG signal was composed of two sets of SHIELD-EKG-EMG (Olimex Ltd., Plovdiv, Bulgaria) which could measure electromyography (EMG) and electrocardiogram (ECG) signal along with an expansion module compatible with the Arduino UNO development board.
Up to 6 groups could be stacked for 6-channel reception to measure myoelectric signals or electrocardiograms during movement. The locations of the study were VMO and VL to monitor and record the EMG signal between them, and the SHIELD-EKG-EMG-PRO was used to connect the SHIELD-EKG-EMG module.
In this study, the myoelectric signals of the VL and on quadriceps femoris muscle were also taken. The position of the electrodes was placed according to the sensing points described in Basmajian and Blumenstein [
21], which were mainly for the detection of the medial and lateral femoral muscles. Considering the difference in signal, each electrode was fixed in place on the front end of the VMO and VL muscle lines as the sensing point placement position that could be clearly identified with the naked eye or palpation. If the front end portion failed to be seen from the naked eye during the placement process, the VMO sensing point would then be placed at about 6 cm away from the patella where the inner side of the patella and the femur was intersected at 40°, and the VL sensing point would be placed at about 9 cm away from the patella where the outer side of the patella and the femur was intersected at 30°, while the reference electrode patch was attached to the tibia of the calf [
22].
In order to match the EMG measurement on user’s leg movement, the system was equipped with GY-85 (HAOYU Electronics, Shenzhen, China) of nine-axis acceleration Inertial Measurement Units (IMU), which was fixed on the flat upper part of the femur. This has the ability to calculate angle and acceleration as well as to simultaneously record the disturbance of the patella and myoelectric signals.
2.3. Signal Processing
The method of muscle evaluation is to express the activity of the muscle by changing the potential of the electromyogram. When the EMG signal is analyzed out of the time domain and the frequency domain, the following three types of message can be obtained: the temporal signal represents the start time and end time of the muscle contraction triggered, and shows the change of muscle contraction at a certain point in time; the force signal represents the proportional relationship between the myoelectric signal and the contractile force produced by the muscle, explaining the state of muscle activity by the amplitude; the fatigue signal represents the fatigue condition of exhausted muscle, in which the high frequency part of the EMG signal is reduced, and the relatively low frequency part is increased, which also represents a significant decrease in the overall frequency [
23,
24]. The EMG characteristics and parameters for assessing muscle function were mainly in the EMG time domain. The value obtained by the integral is proportional to the strength of the muscle contraction force. This was used to calculate the muscle contraction activity per unit time and expressed by integral electromyography (iEMG), as the root mean square value (Root Mean Square, RMS) was calculated as well. Once the fatigue is happened, the high frequency of EMG decreased but the low frequency of EMG increased. It showed that the signal of electromyography is calculated in time domain of EMG. Then the integrated electromyography (iEMG) and the root mean square (RMS) are also calculated based on the integral value and the strength of muscle contraction. Equations (1) and (2) indicates the amplitude index of myoelectric signals; it sums the signals in the time period to evaluate the strength of the EMG signal [
25]. The larger the sum value, the larger the myoelectric signal during the cycle time.
The frequency domain analysis is based on the frequency variation characteristics of the EMG signal. It performs Short-Time Fourier Transform (STFT) on the EMG signal to obtain the Power Spectral Density (PSD) of the EMG signal and shows the myoelectric signal at those frequencies and at their distribution ratio. Frequency domain analysis is usually based on Mean Frequency (MNF) and Median Frequency (MDF), as shown in Equations (3) and (4) [
26]. They were used to judge the fatigue of the muscles and show a linear decline in the dynamic process. This feature can be used as a reference for the development of muscle fatigue.
Muscle fatigue occurs due to long-term muscle contraction. In the frequency domain, MNF or MDF frequencies that show the occurrence of muscle fatigue caused by lower frequency shift should be reminded to avoid injury [
27]. The signal processing is based on the references. Compared with the walking state, the VMO increase and the VL decrease occur in the running state indicated that the VMO would be weak in the walking condition. Currently, there is no evidence of whether the distribution of these muscle forces will cause pain or result in illness but increasing co-contraction can improve knee joint stability and helps to adjust the patella’s gliding trajectory.
The Contraction Threshold (CT) was defined as the level of static level signal plus 3 times Standard Deviation (σ), as shown in Equation (5). The CT value was used to extract the segment caused by the action in the myoelectric signal, and the static level signal portion was excluded to reduce the total number of signal calculations and also to highlight the myoelectric signal caused by the action. Within a set of approximate normal probability distribution data, about 99.7% of the values were distributed within 3 times of the standard deviation range, about 95% of the values were within 2 times of the standard deviation range, and about 68% were within 1 time of the standard deviation range. Assuming that a set of stationary horizontal signals was 10 and the standard deviation was 2, the range within 3 times of the standard deviation was equal to 10 ± 6 or 4–16, and the value of +16 was set to CT, as shown in Equation (6).
This study used CT to capture the start and end positions of the threshold beyond and expressed it as a segment from a point to b point. The starting position higher than the threshold value was set to point a, and the ending position lower than the threshold value was set to point b. As shown in Equation (7), the average value calculated for this section was taken as the average of the amplitude and time. In the VL and VMO sections, the segment between points of a and b was the same, and the average intensity of the VL and VMO myoelectric signals was calculated in the same section. To evaluate the difference in the average intensity of the signals between the two, the composite signal was calculated for evaluation which could visually show each other’s relevance. As shown in Equation (8), the results of the VMO VL Ratio (VVR) were calculated to compare the sum of intramuscular muscles signal strengths of the two groups, where the average number of electrical signals
of VMO was compared with that of
of VL. When VVR is greater than 1, the average VMO EMG signal was higher than VL, which indicates the VMO of the rehabilitation training action that was higher than VL should be able to achieve the purpose of rehabilitation. Conversely, less than 1 meant that the VL EMG average was higher than VMO [
28].
2.4. Pretest
If all subjects were to conduct walking with measurement actions of left and right feet lifting and kicking (sitting and standing) between 10°–90°, each subject would need to perform 336 actions. In this case, not only would the measurement time be too long and result in an unbearable load on the subject’s body, but also might lead to data dispersion and excessive errors.
If each subject needs to be lift and kick the right and left legs on both of standing and sitting postures with walking for our experiment, the number of training action for each subject is 336. In this situation, the measuring time will be too long and it is an overload for subjects. Moreover, the data may be dispersed and the risk of error would increase. Therefore, in the preliminary test, there are 10 subjects, where the number of male and female is 5 and 5, respectively. The actions included the common walking, leg lifting, and kicking. The responding angle of the common walking, leg lifting, and kicking is 30, 60, and 90 degrees. Based on the above presetting, if the difference of the medial muscle strength between the right and left legs is almost the same, we will focus on the medial muscle strength of the right lower limb, where the angle of the common walking, leg lifting, and kicking is from 10 to 90 degrees.
2.5. Statistical Analysis
The experimental results were based on the commonly used IBM SPSS 22.0 for Windows (IBM SPSS Statistics; IBM Corporation, Somers, NY, USA) to determine the difference between the data of each group, with a p value less than α = 0.05 being considered statistically significant.
3. Results and Discussion
3.1. Pretest
The biggest advantage of the nonparametric statistics is that, when the parent population distribution is unknown or not normal, or the sample number is not large enough, the pretest can be performed in the preset verification of nonparametric statistics in SPSS. First, the reliability analysis of the data was performed, and the results showed 14 actions in the left and right foot measurement item scale of walking mode, leg raising and kicking (30°, 60°, and 90°). The smallest total average of the statistics occurred in the walking mode (M = 0.612) and the largest total average of 60 0 (M = 1.031) in the kick mode indicated that, for 10 subjects in walking pretest mode, the average contribution of VVR force value of the quadriceps femoris muscle was 0.612, which was close to the VMO mean contribution of 26% in the walking mode, 45% of VL Contribution, and 0.578 of the converted ratio indicated in the paper of Besier T.F. et al. [
29]. In the kick mode, the force contribution ratio of VMO on the quadriceps femoris muscle was greater than that of the VL on the quadriceps femoris muscle; the smallest standard deviation occurs in the leg lift mode 30° (SD = 0.076) and the maximum standard deviation value and the maximum variability were both 90° (SD = 0.156) in the leg raising mode. The difference in the value might reflect that it was difficult or prone to generating fatigue when the leg was raised by 90°. The relevant values are shown in
Table 1. However, this was only the result of the pretest, and more follow-up data is needed for verification.
The Kolmogorov-Smirnov One Sample Test showed that the distribution, mean and standard deviation of each measurement item was normal. The alpha (α) coefficient of pretest was 0.715. Overall, the subject’s performance in the measurement action was consistent with Cronbach’s internal consistency [
30].
The independent sample Mann-Whitney U test was used to compare whether the average number of continuous variables in the two independent groups was significantly different in the nonparametric analysis. In order to simplify the experimental procedure and shorten the measurement time, it was assumed that there was no significant difference between the left and right feet of the subject, and an independent measurement was performed on the measurement results of the left and right feet of the walking mode, lifting leg and kicking leg (30°, 60°, 90°).As a result, the difference between the left and right feet in the state of walking, lifting the legs by 30°, lifting the legs by 60°, lifting the legs by 90°, kicking the legs by 30°, kicking the legs by 60°, kicking the legs by 90° was 0.393, 0.739, 1.000, 0.853, 0.481, 0.684 and 0.631, respectively, showing no statistically significant difference at α ≥ 0.05. The box plot of pretest male and female left and right feet average in each mode of walking, lifting legs and kicking (30°, 60°, 90°) is shown in
Figure 2 and
Figure 3.
The purpose of the paired sample T test is to determine whether the average of the two related samples is significantly different or not. Compared with lift mode(30°/60°/90°), the walking mode of subjects were with the mean (M) of −0.168, −0.186, and −0.237, the standard deviation SD = 0.111/0.179/0.168, T = −6.791, −4.647, and -6.336, and α ≤ 0.05; when compared with kick mode, the walking mode of subjects were with the mean of −0.372/−0.419/−0.373, the standard deviation (SD) of 0.173/0.172/0.152, T = −9.628, −10.906, and −11.007, and α ≤ 0.05. Since the leg-lifting of kicking action was significant (p < 0.05) with respect to the walking pattern, there was a statistically significant difference. The results showed that the walking mode in accordance with the values listed in the reference was not statistically significant in difference. There was a significant difference between both the leg lift and kick leg mode and the walking mode, and the kicking mode had a greater difference than the leg lift mode.
Overall, for each mode of walk contrasting leg raising and kicking (30°, 60°, 90°), subjects in the pretest had a better effect in the right foot than the left foot in each mode of walking. Moreover, the leg kicking had a better effect than the leg lifting, and the higher the angle in the leg lift mode, the higher the average value; in the kick mode, the average of 60° was better, and it might be because of 30° and 90° were not easy to kick; therefore, the subsequent rehabilitation actions would be based on the kicking action of the right foot as the main discussion target.
3.2. Kick Training
The number of subjects in this experiment was 83 (45 males; 38 female). The age range of the female subjects is from 26 to 50 years old. The data samples were more than 30, which were analyzed by the parametric method. The reliability evaluation results of the overall measurement operation showed that the male subjects had an average number of M = 1.148 to 1.512 in a total of 18 kick items such as 10°, 20°, …, 90° in terms of sitting and standing positions, with 0.256–0.592 of standard deviation and 0.962 of alpha value; the mean number of female subjects was M = 0.791–1.168, the standard deviation SD was 0.368–0.498, and the alpha value was 0.977, as shown in
Table 2. Overall, the total reliability of the entire scale of the male and female subjects in the measurement operation was above 0.7, which was consistent with the internal consistency of “Cronbach’s α”.
In this study, a single sample t-test was performed on the data of 45 male subjects and the male pre-test walking right-foot average of 0.666 to compare whether the 18 kick angles and the 18 postures of the two postures were significantly different and to observe the degree of effect. The results of the sitting posture mean were: M = 1.370–1.512, standard deviation SD = 0.451–0.592, α ≤ 0.05, d = 1.623–1.948, with significant difference. The effect statistics were of a large level, wherein the Q1/Q3 quartile was located at 0.979–1.927 and the minimum/maximum outlier was 0.422/2.594; the average number of standing positions was 1.148–1.253, wherein the standard deviation was 0.256–0.397, α ≤ 0.05, d = 1.387–2.031, with significant difference. The effect statistics were large level, the Q1/Q3 quartile was located at 0.966–1.415, with 2.520 of the maximum outliers. Overall, there was a significant amount of effect greater than 1 regardless of whether a sitting or standing position was employed or the angle employed. Compared with 0.57338 of female subjects’ pretest test right foot average, the average sitting posture was 0.791–0.906, with standard deviation of 0.372–0.498, α ≤ 0.05, d = 0.626–0.801. There was a statistically significant difference, the effect statistic was medium to large level, the Q1/Q3 quartile was located at 0.502–1.037, and the maximum outlier was 2.554. The average standing position was 0.966–1.168, the standard deviation was 0.368~0.441, α ≤ 0.05, d = 0.997–1.438, with statistically significant difference. The effect statistic was a large level, Q1/Q3 quartile position located from 0.670 to 1.456, and the maximum outlier was 2.326. Overall, the average sitting posture of the 18 motion items was 0.791 or more, and the average standing value was about 0.966. The result showed that the standing posture was superior to the sitting posture.
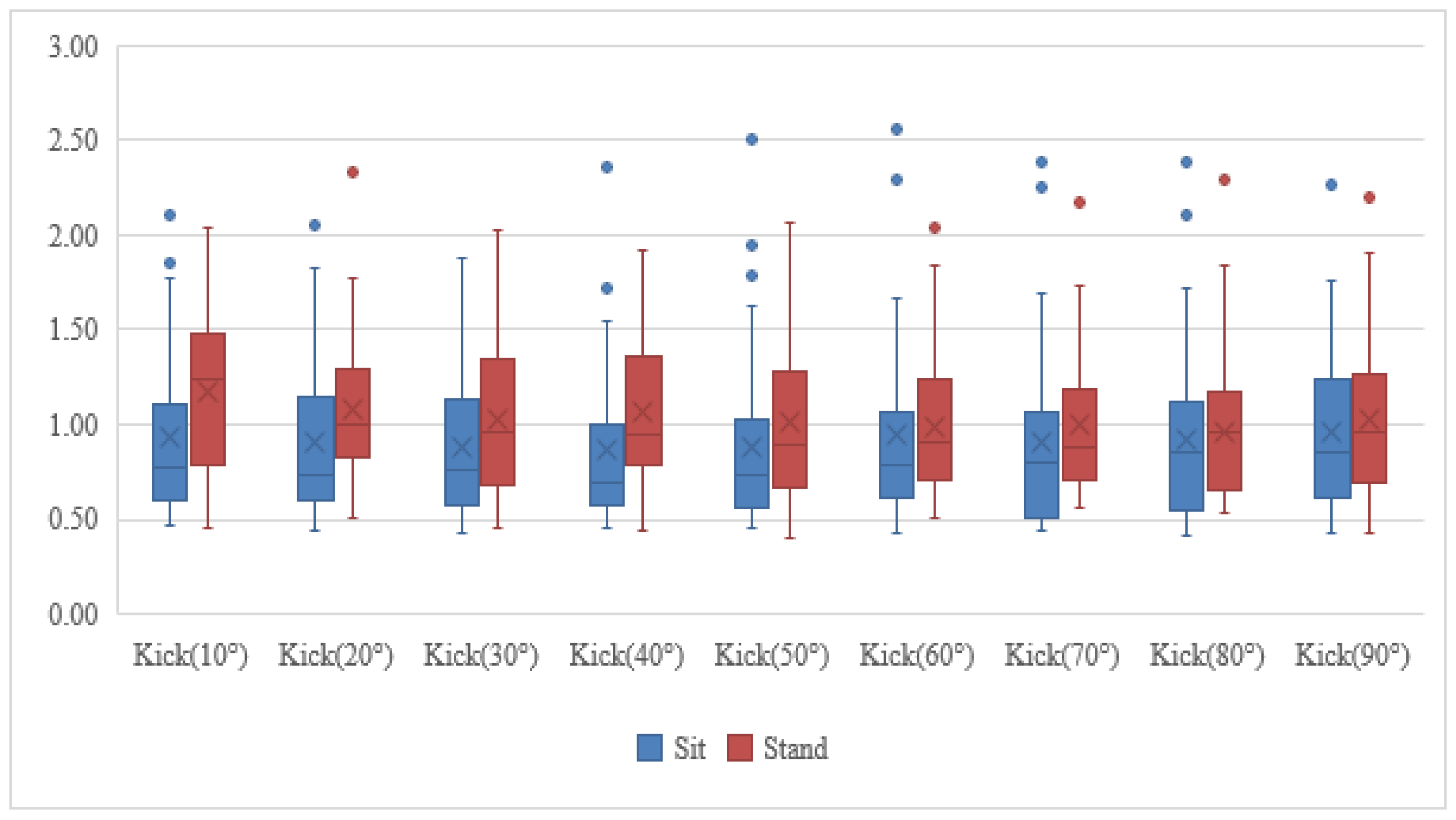
The paired sample T test was used to explore the differences between the different postures of the subjects. The results of male subjects was between 10°–30 °, with α ≤ 0.05, d = 0.742~0.831 and statistically significant difference, and the effect statistics were medium to large level. In the 40° kicking action, there was no statistically significant difference with α ≥ 0.05 and d = 0.405, and the effect statistic was middle level; there was a statistically significant difference between 50° and 90°, α ≤ 0.05, d = 0.569~0.0.709, and the effect statistic was above the middle level. For the male subjects as a whole, there was no significant difference except at 40°, the others were significantly different at all angles, and the sitting posture was better than the standing posture. Female subjects had a statistically significant difference in α ≤ 0.05, d = −0.550 when the 10° kicking action was performed, and the effect statistic was middle level; when the kicking action was 20°~90° with α ≥ 0.05 and d = −0.101~−0.494, there was no statistically significant difference, and the effect statistics are small to medium grade, and the effect statistic was small to middle level. In terms of female subjects, except for significant differences at 10°, the rest were not significantly different at all angles, and the d value was negative, indicating that the standing posture was better than the sitting posture. The box plot of each position and angle average of male and female samples are shown in
Figure 4 and
Figure 5.
In the case of a single subject where 45 male subjects were in a 10°~90° sitting and standing kick, the percentage of times of the sitting effect that was greater than the standing position was 75%~85%. In the overall kick training, 60.44% of the sitting posture was larger than the standing position, the force value of 74.31% of VMO/VL on Quadriceps Femoris Muscle was greater than 1, and 97.78% of the force value of VMO/VL on quadriceps femoris muscle was greater than the walking pattern of the pretest, indicating that the kicking action contributed to the muscle training of the VMO, with 40° being the best. Among the 38 female subjects, the percentage of standing postures greater than sitting posture was 64% to 76%. In the overall kick training, 84.34% of the standing posture was larger than the sitting posture, showing that the standing posture had a better effect for female subjects. In addition, 37.71% of the VMO/VL force value was greater than 1 and 84.34% of VMO/VL force value of quadriceps femoris muscle was greater than the pretest walking mode, indicating that the kicking action could not immediately strengthen VMO muscle greater than the VL effect, but could still contribute to VMO muscle strength training, which was maximized at 20°, as shown in
Figure 6.
Based on the preliminarily estimation at 10° and 90°, VVR of the quadriceps femoris muscle was more scattered because the leg lift was not obvious, or the lift was not easy. The VVR of the quadriceps femoris muscle was more scattered. The remaining angles were analyzed by ANOVA, and the results showed no significant difference between the angles. However, the average VVR of the kick was best at about 50°–60° compared with the normal gait, and the difference was up to 52%, in which the leg kick was more effective than the leg lift. The overall subject was also more than normal gait at 20°–90°.The male subject’s leg kick training could clearly reach the effect of VMO on quadriceps femoris muscle larger than VL on the quadriceps femoris muscle, and the sitting position was better than the standing position. Although the female subject’s leg kick training cannot immediately achieve the effect of VMO on quadriceps femoris muscle larger than VL on quadriceps femoris muscle, it enhanced VMO on the quadriceps femoris muscle as well, and the effect was better for standing.
The experiment examined the difference of each experimental results by IBM SPSS 22.0 for Window, where the value of p is less than the value of α which its value is set to 0.05. While the quantity of pretest factor is less than 30, the nonparametric method was used. While the quantity of pretest factor is larger than 30, the parametric method was used. Once the parametric method is used, reliability analysis will be used for the experimental results.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}