Surgical Navigation System for Transsphenoidal Pituitary Surgery Applying U-Net-Based Automatic Segmentation and Bendable Devices


Abstract
1. Introduction
2. Automatic Segmentation Using U-Net
2.1. U-Net
2.2. Preparation of Training Data
2.3. U-Net Training Phase
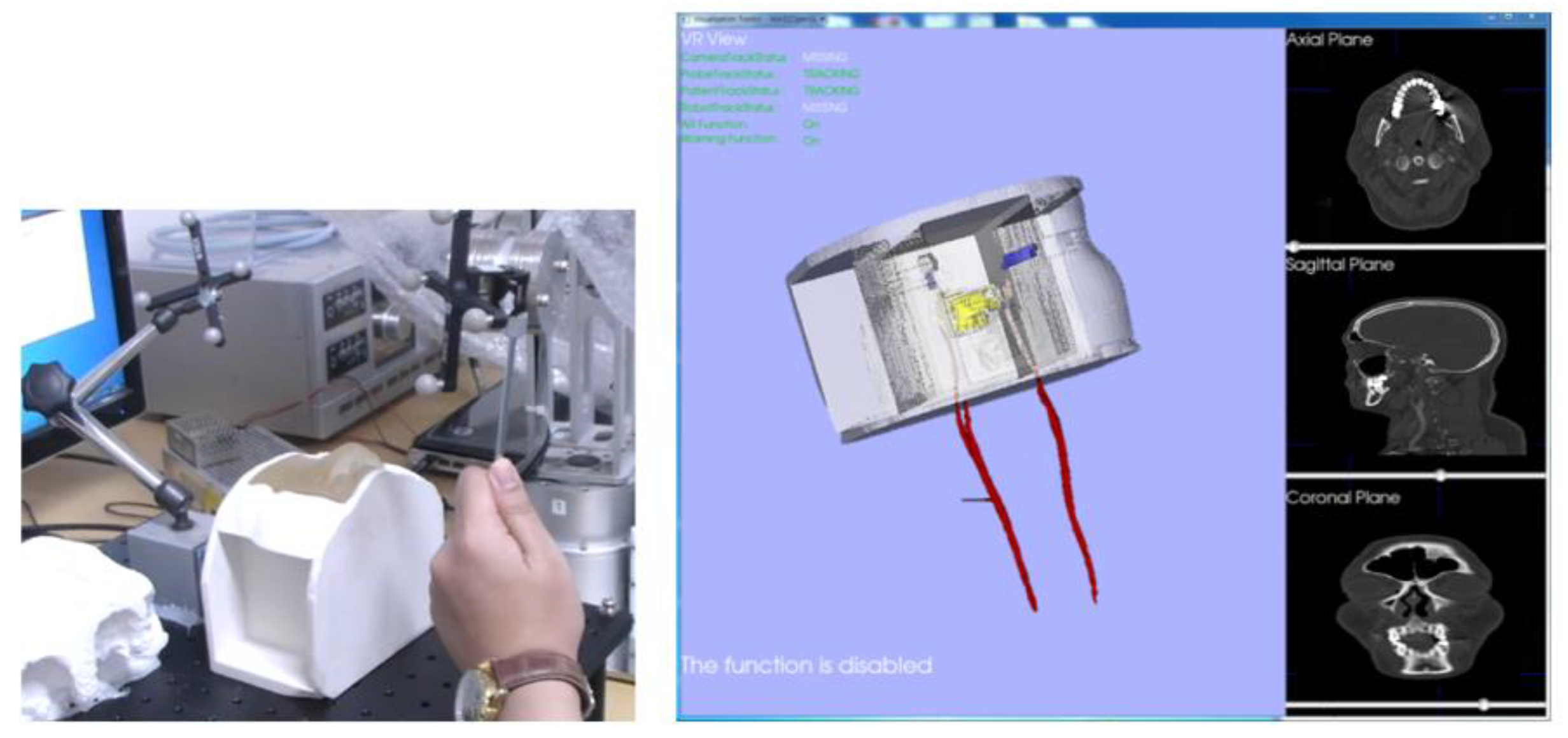
3. Surgical Navigation System
3.1. Proposed Surgical Navigation System
3.2. Registration for Construction of Navigation System
4. Design of the Bendable Endoscope, Surgical Tool and Phantom Design
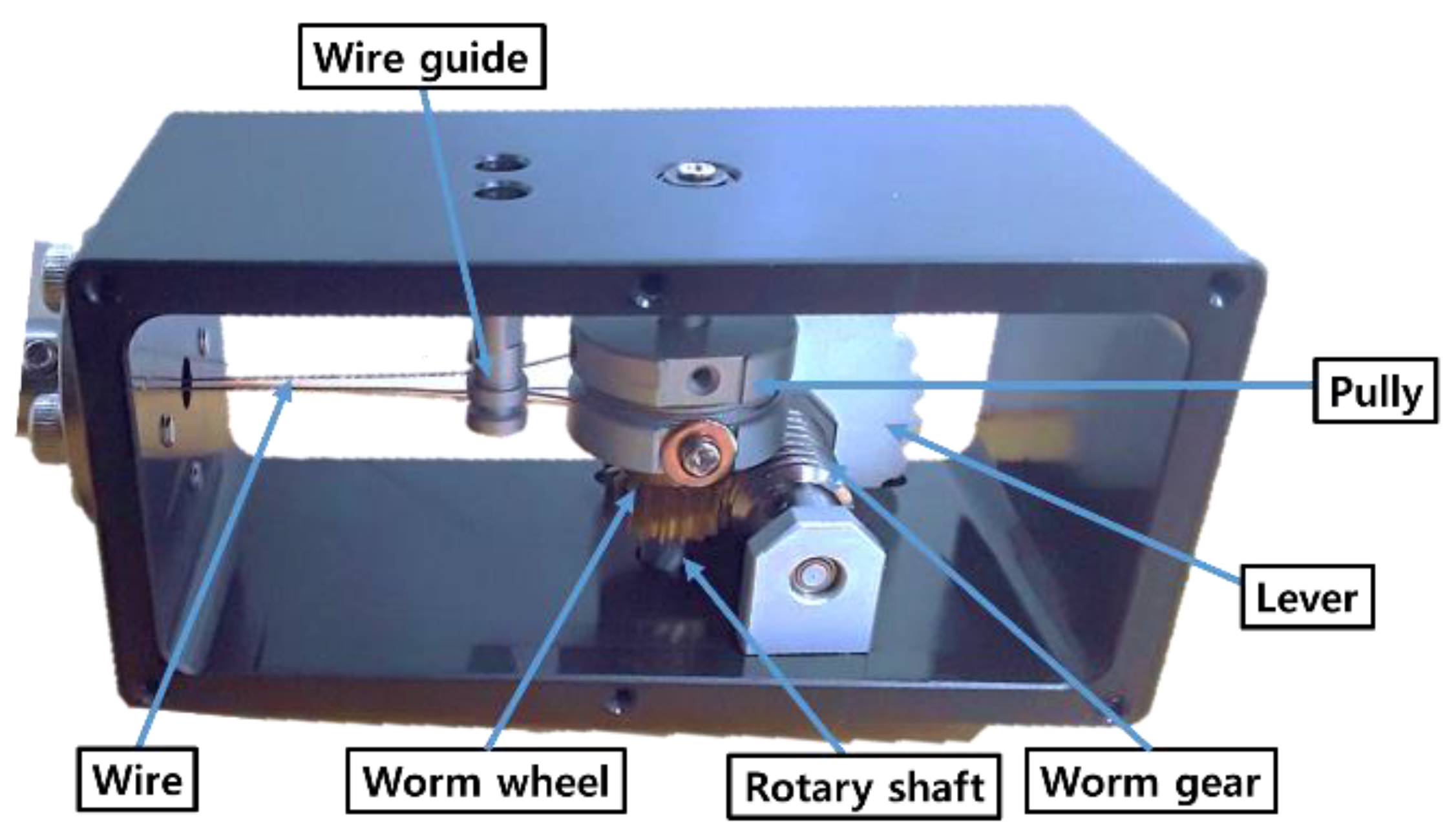
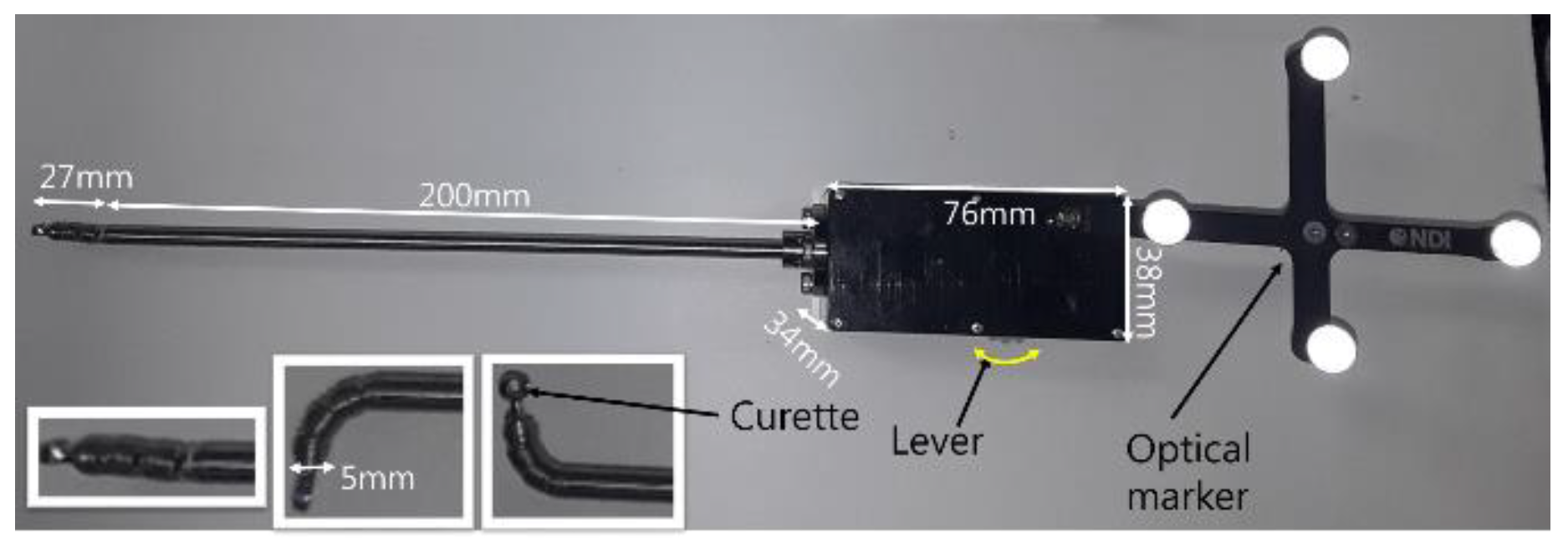
4.1. Design of Bendable Endoscope and Surgical Tool
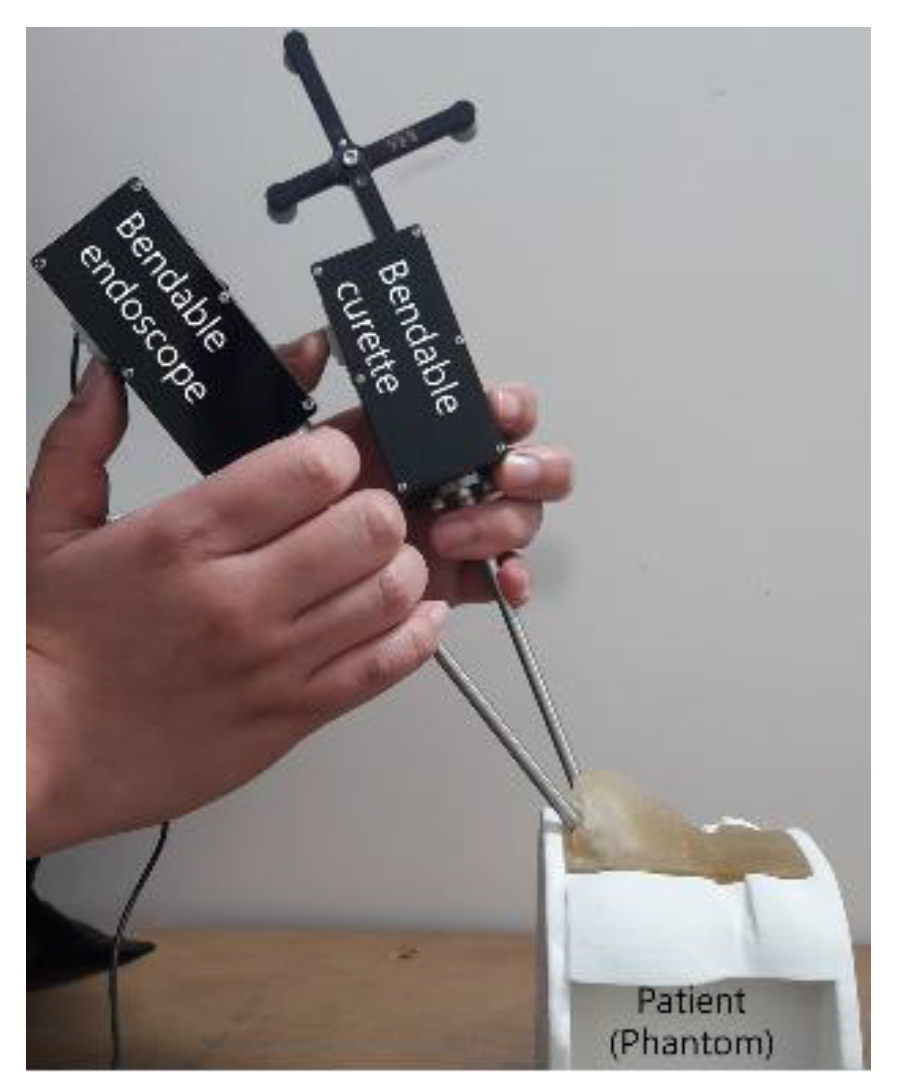
4.2. Design of the Phantom
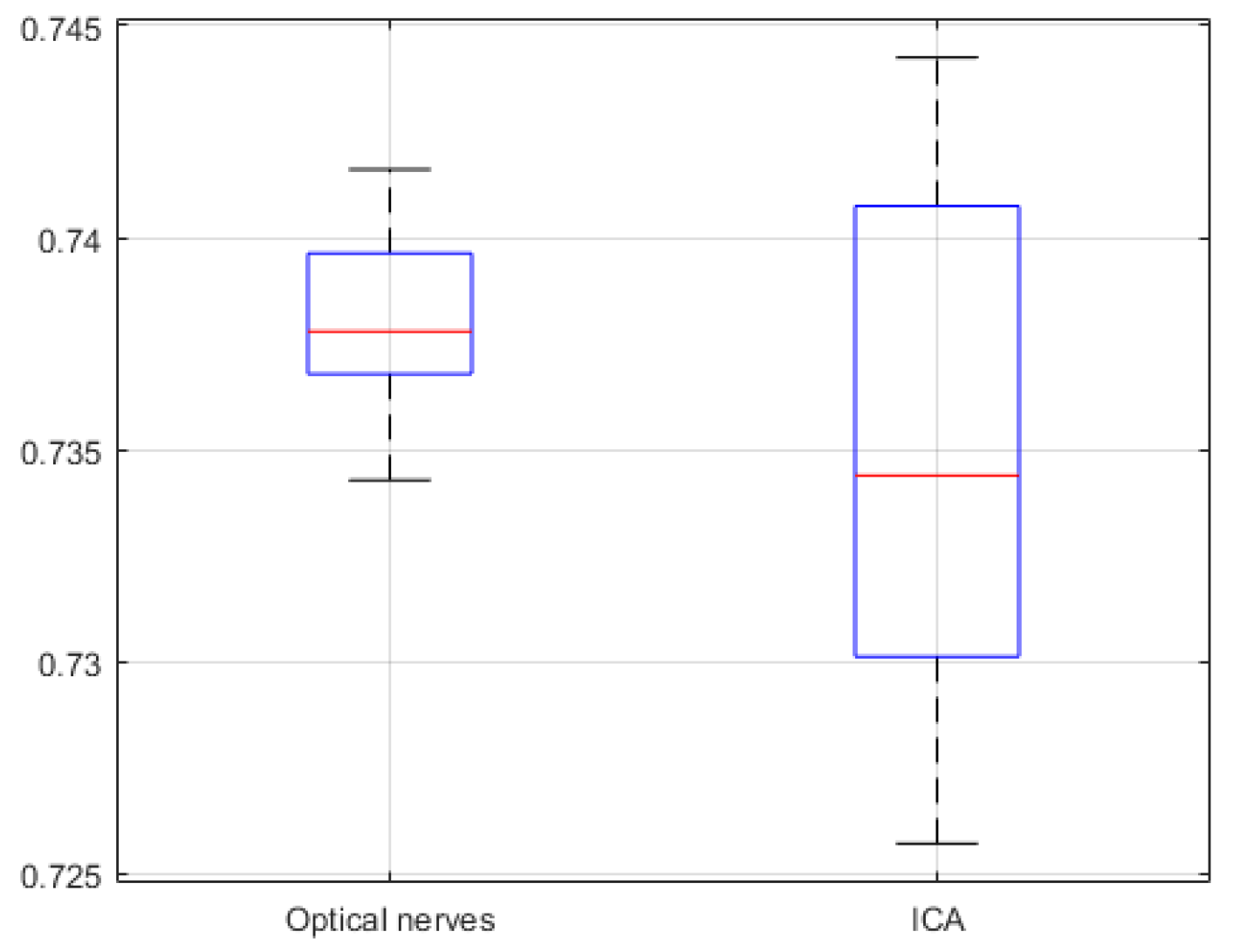
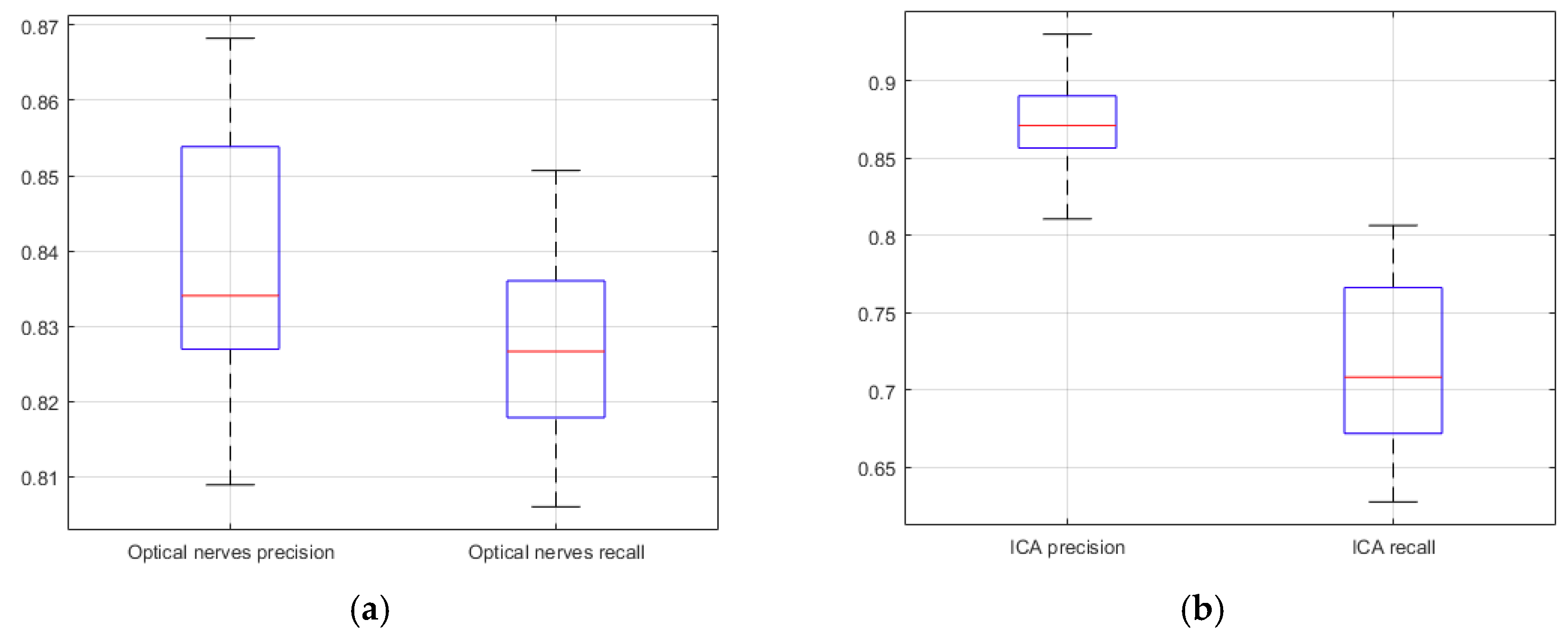
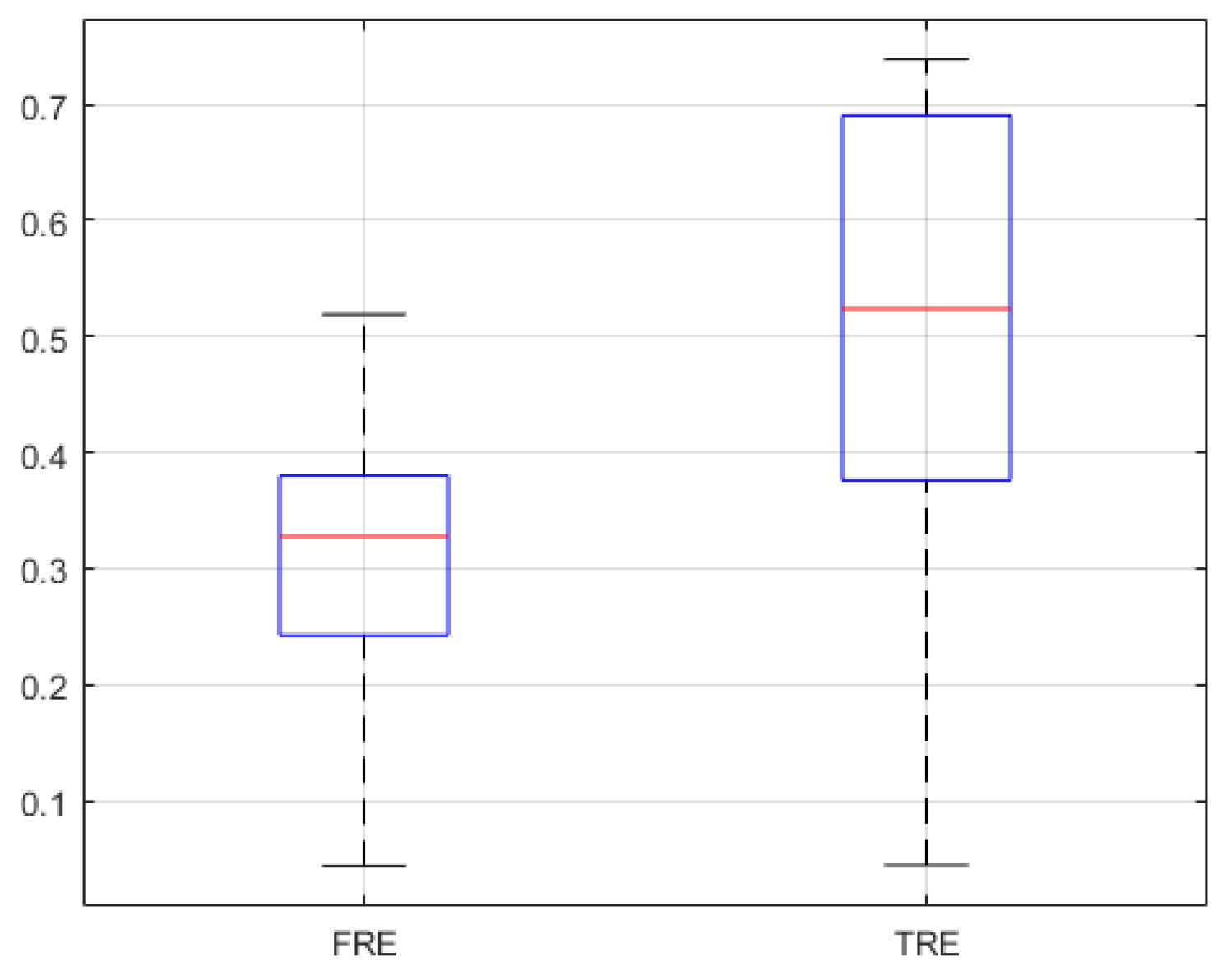
5. Experimental Results
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A




References
- Su, H.; Sandoval, J.; Vieyres, P.; Poisson, G.; Ferrigno, G.; De Momi, E. Safety-enhanced collaborative framework for tele-operated minimally invasive surgery using a 7-DOF torque-controlled robot. Int. J. Control. Autom. Syst. 2018, 16, 2915–2923. [Google Scholar] [CrossRef]
- Rotenberg, B.; Tam, S.; Ryu, W.H.A.; Duggal, N. Microscopic versus endoscopic pituitary surgery: A systematic review. Laryngoscope 2010, 120, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Jaydeep, P.H. Robotic assisted minimally invasive surgery. J. Minimal Access Surg. 2009, 5, 1–7. [Google Scholar]
- Yoon, H.-S.; Song, H.-S. Preliminary study for Transsphenoidal pituitary surgery. In Proceedings of the Asian Conference on Computer Aided Surgery (ACCAS2017), Changhua, Taiwan, 26–28 November 2017. [Google Scholar]
- Velasquez, C.A.; Kim, Y.S.; Lendvay, T.S.; Hannaford, B.; Yoon, W.J. RAVEN Eyes Around the Instrument from Modular Axis Sharing. Int. J. Control. Autom. 2019, 17, 454–464. [Google Scholar] [CrossRef]
- Yoon, H.; Jeong, J.H.; Yi, B.-J. Image-guided dual master–slave robotic system for Maxillary sinus surgery. IEEE Trans. Robot. 2018, 34, 1098–1111. [Google Scholar] [CrossRef]
- Kwon, S.; Choi, W.; Ryu, G.; Kang, S.; Kim, K. Endoscopic Endonasal Skull Based Surgery System. In Proceedings of the 14th International Conference on Ubiquitous Robots and Ambient Intelligence, Jeju, Korea, 28 June–1 July 2017; pp. 544–545. [Google Scholar]
- Burgner, J.; Rucker, D.C.; Gilbert, H.B.; Swaney, P.J.; Russell, P.T.; Weaver, K.D.; Webster, R.J. A telerobotic system for Transnasal surgery. IEEE-ASME Trans. Mechatron. 2014, 19, 996–1006. [Google Scholar] [CrossRef]
- Jin, S.; Lee, S.K.; Lee, J.; Han, S. Kinematic Model and Real-Time Path Generator for a Wire-Driven Surgical Robot Arm with Articulated Joint Structure. Appl. Sci. 2019, 9, 4114. [Google Scholar] [CrossRef]
- He, Y.; Hu, Y.; Zhang, P.; Zhao, B.; Qi, X.; Zhang, J. Human–Robot Cooperative Control Based on Virtual Fixture in Robot-Assisted Endoscopic Sinus Surgery. Appl. Sci. 2019, 9, 1659. [Google Scholar] [CrossRef]
- Yoon, H.; Oh, S.M.; Jeong, J.H.; Lee, S.H.; Tae, K.; Koh, K.; Yi, B. Active Bending Endoscope Robot System for Navigation through Sinus Area. In Proceedings of the 2011 IEEE/RSJ International Conference on Intelligent Robots and Systems, San Francisco, CA, USA, 25–30 September 2011; pp. 967–972. [Google Scholar]
- Mark, M.; Levine, H.L.; Mester, S.J.; Schaitkin, B. Complications of endoscopic sinus surgery: Analysis of 2108 patients—Incidence and prevention. Laryngoscope 1994, 104, 1080–1083. [Google Scholar]
- Kong, X.; Duan, X.; Wang, Y. An integrated system for planning navigation and robotic assistance for mandible reconstruction surgery. Intell. Serv. Robot. 2016, 9, 113–121. [Google Scholar] [CrossRef]
- Lee, S.; Kim, J.Y.; Hong, J.; Baek, S.H.; Kim, S.Y. CT-based navigation system using a patient-specific instrument for Femoral component positioning: An experimental in vitro study with a Sawbone model. Yonsei Med. J. 2018, 59, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Chung, G.B.; Kim, S.; Lee, S.G.; Yi, B.-J.; Kim, W.; Oh, S.M.; Kim, Y.S.; So, B.R.; Park, J.I.; Oh, S.H. An image-guided robotic surgery system for spinal fusion. Int. J. Control. Autom. Syst. 2006, 4, 30–41. [Google Scholar]
- Chung, J.; Kim, S.; Yi, B.-J.; Kim, Y.S. Cadaver study for spinal fusion surgery using an image-guided surgical robot system. Int. J. Control. Autom. Syst. 2010, 8, 564–573. [Google Scholar] [CrossRef]
- van Oosterom, M.N.; van der Poel, H.G.; Navab, N.; van de Velde, C.J.; van Leeuwen, F.W. Computer-assisted surgery: Virtual-and augmented-reality displays for navigation during urological interventions. Curr. Opin. Urol. 2018, 31, 205–213. [Google Scholar] [CrossRef]
- Chen, X.; Xu, L.; Wang, H.; Wang, F.; Wang, Q.; Kikinis, R. Development of a surgical navigation system based on 3D Slicer for intraoperative implant placement surgery. Med. Eng. Phys. 2017, 41, 81–89. [Google Scholar] [CrossRef]
- Hasan, W.; Daly, M.J.; Chan, H.H.L.; Qiu, J.; Irish, J.C. Intraoperative cone-beam CT-guided osteotomy navigation in mandible and maxilla surgery. Laryngoscope 2019, 1–7. [Google Scholar] [CrossRef]
- Forbes, K.; Karis, J.; White, W.L. Imaging of the pituitary gland. Barrow Q. 2002, 18, 9–19. [Google Scholar]
- Wang, C.; Zhao, Z.; Ren, Q.; Xu, Y.; Yu, Y. Dense U-net Based on Patch-Based Learning for Retinal Vessel Segmentation. Entropy 2019, 21, 168. [Google Scholar] [CrossRef]
- Xu, Y.; Mo, T.; Feng, Q.W.; Zhong, P.L.; Lai, M.D.; Chang, E.I.-C. Deep learning of feature representation with multiple instance learning for medical image analysis. In Proceedings of the 2014 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Florence, Italy, 4–9 May 2014; pp. 1626–1630. [Google Scholar]
- Visentini-Scarzanella, M.; Sugiura, T.; Kaneko, T.; Koto, S. Deep monocular 3d reconstruction for assisted navigation in bronchoscopy. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 1089–1099. [Google Scholar] [CrossRef]
- Laina, I.; Rieke, N.; Rupprecht, C.; Vizcaíno, J.P.; Eslami, A.; Tombari, F.; Navab, N. Concurrent segmentation and localization for tracking of surgical instruments. In Medical Image Computing and Computer-Assisted Intervention—MICCAI 2017; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Esfandiari, H.; Newell, R.; Anglin, C.; Street, J.; Hodgson, A.J. A deep learning framework for segmentation and pose estimation of pedicle screw implants based on C-arm fluoroscopy. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 1269–1282. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Medical Image Computing and Computer-Assisted Intervention—MICCAI 2015; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. arXiv 2017, arXiv:1702.05747. [Google Scholar] [CrossRef] [PubMed]
- Fausto, M.; Nassir, N.; Ahmad, S. V-net: Fully convolutional neural networks for volumetric medical image segmentation. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar]
- Badrinarayanan, V.; Kendall, A.; Cipolla, B. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef]
- Knott, P.D.; Batra, P.S.; Butler, R.S.; Citardi, M.J. Contour and paired-point registration in a model for image-guided surgery. Laryngoscope 2006, 116, 1877–1881. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, J.M. Fiducial registration error and target registration error are uncorrelated. SPIE Med. Imaging Vis. Image Guided Proced. Model 2009, 7261. [Google Scholar] [CrossRef]
- Azarmehr, I.; Stokbro, K.; Bell, R.B.; Thygesen, T. Surgical navigation: A systematic review of indications, treatments, and outcomes in oral and maxillofacial surgery. J. Oral Maxillofac. Surg. 2017, 75, 1987–2005. [Google Scholar] [CrossRef] [PubMed]
- Shamir, R.R.; Joskowicz, L.; Shoshan, Y. Fiducial optimization for minimal target registration error in image-guided neurosurgery. IEEE Trans. Med. Imaging 2012, 31, 725–737. [Google Scholar] [CrossRef] [PubMed]
- West, J.B.; Fitzpatrick, J.M. The distribution of target registration error in rigid-body point-based registration. IEEE Trans. Med. Imaging 2001, 20, 917–927. [Google Scholar]
- Qin, C.; Cao, Z.; Fan, S.; Wu, Y.; Sun, Y.; Politis, C.; Wang, C.; Chen, X. An oral and maxillofacial navigation system for implant placement with automatic identification of fiducial points. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 281–289. [Google Scholar] [CrossRef]
- Xue, R.; Ren, B.; Huang, J.; Yan, Z.; Du, Z. Design and Evaluation of FBG-Based Tension Sensor in Laparoscope Surgical Robots. Sensors 2018, 18, 2067. [Google Scholar] [CrossRef]
- Gibson, E.; Li, W.; Sudre, C.; Fidon, L.; Shakir, D.I.; Wang, G.; Eaton-Rosen, Z.; Gray, R.; Doel, T.; Hu, Y.; et al. Niftynet: A deep-learning platform for medical imaging. Comput. Methods Programs Biomed. 2018, 158, 113–122. [Google Scholar] [CrossRef]
- Chen, L.C.; Papandreou, G.; Schro, F.; Adam, H. Rethinking Atrous Convolution for Semantic Image Segmentation. arXiv 2017, arXiv:1706.05587. [Google Scholar]



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Required [s] | |
|---|---|
| Manual | 518 |
| U-Net | 13 |
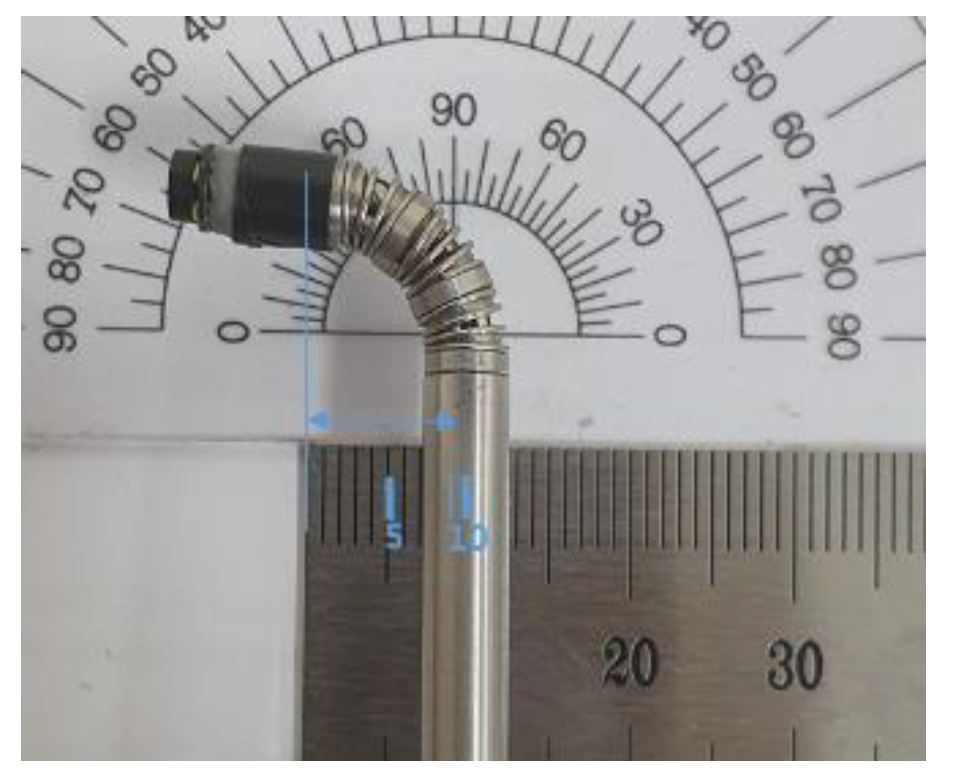
| Design Parameters | |||||
|---|---|---|---|---|---|
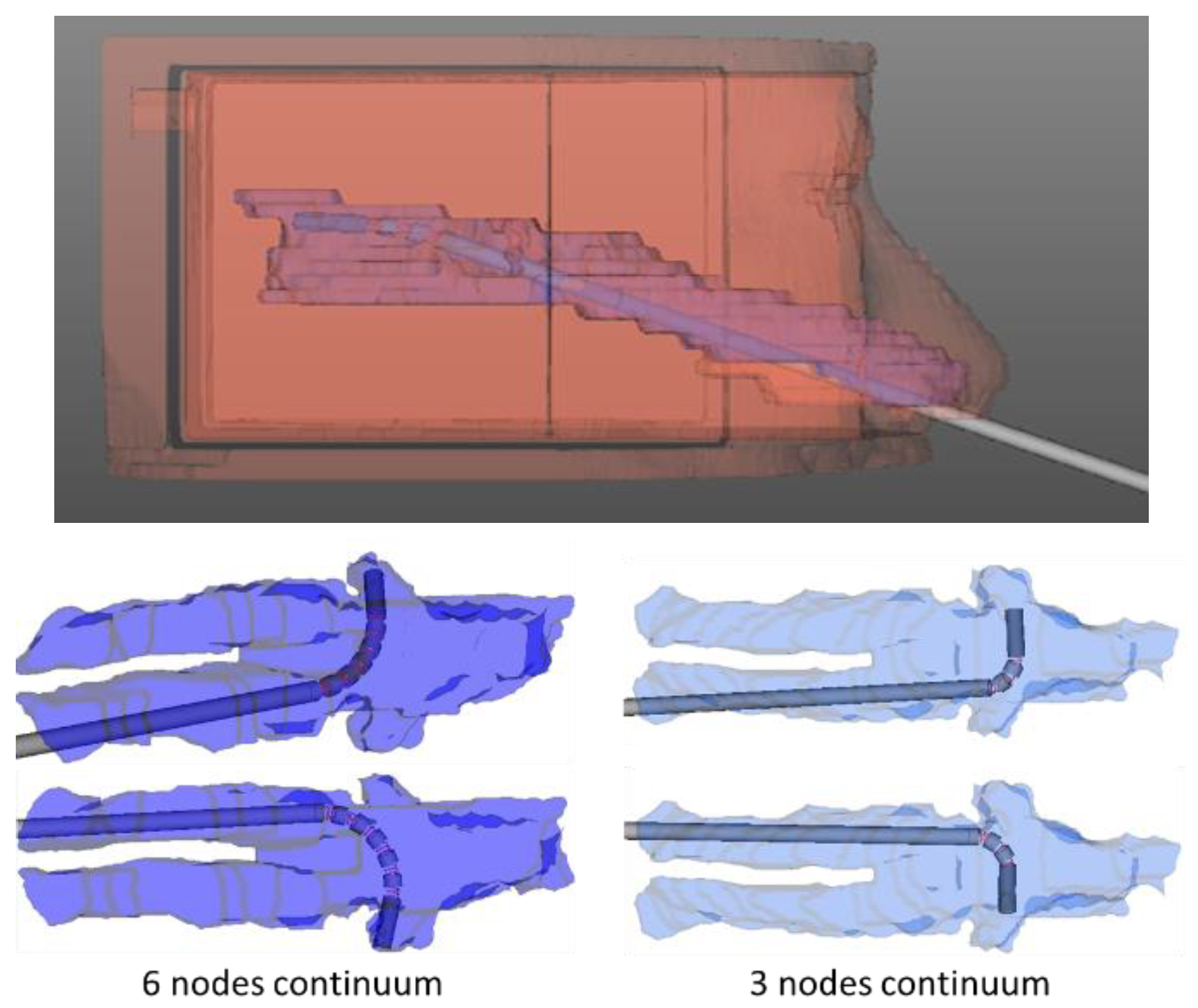
| Bending Angl#e | Radius of Curvature | Cylinder Diameter | Length of Cylinder | Number of Nodes | Length of Spring |
| 90° | 9.5 mm | 5 mm | 1.1 mm | 3 | 3.8 mm |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, H.-S.; Yoon, H.-S.; Lee, S.; Hong, C.-K.; Yi, B.-J. Surgical Navigation System for Transsphenoidal Pituitary Surgery Applying U-Net-Based Automatic Segmentation and Bendable Devices. Appl. Sci. 2019, 9, 5540. https://doi.org/10.3390/app9245540
Song H-S, Yoon H-S, Lee S, Hong C-K, Yi B-J. Surgical Navigation System for Transsphenoidal Pituitary Surgery Applying U-Net-Based Automatic Segmentation and Bendable Devices. Applied Sciences. 2019; 9(24):5540. https://doi.org/10.3390/app9245540
Chicago/Turabian StyleSong, Hwa-Seob, Hyun-Soo Yoon, Seongpung Lee, Chang-Ki Hong, and Byung-Ju Yi. 2019. "Surgical Navigation System for Transsphenoidal Pituitary Surgery Applying U-Net-Based Automatic Segmentation and Bendable Devices" Applied Sciences 9, no. 24: 5540. https://doi.org/10.3390/app9245540
APA StyleSong, H.-S., Yoon, H.-S., Lee, S., Hong, C.-K., & Yi, B.-J. (2019). Surgical Navigation System for Transsphenoidal Pituitary Surgery Applying U-Net-Based Automatic Segmentation and Bendable Devices. Applied Sciences, 9(24), 5540. https://doi.org/10.3390/app9245540