Photoplethysmography-Based Continuous Systolic Blood Pressure Estimation Method for Low Processing Power Wearable Devices


 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
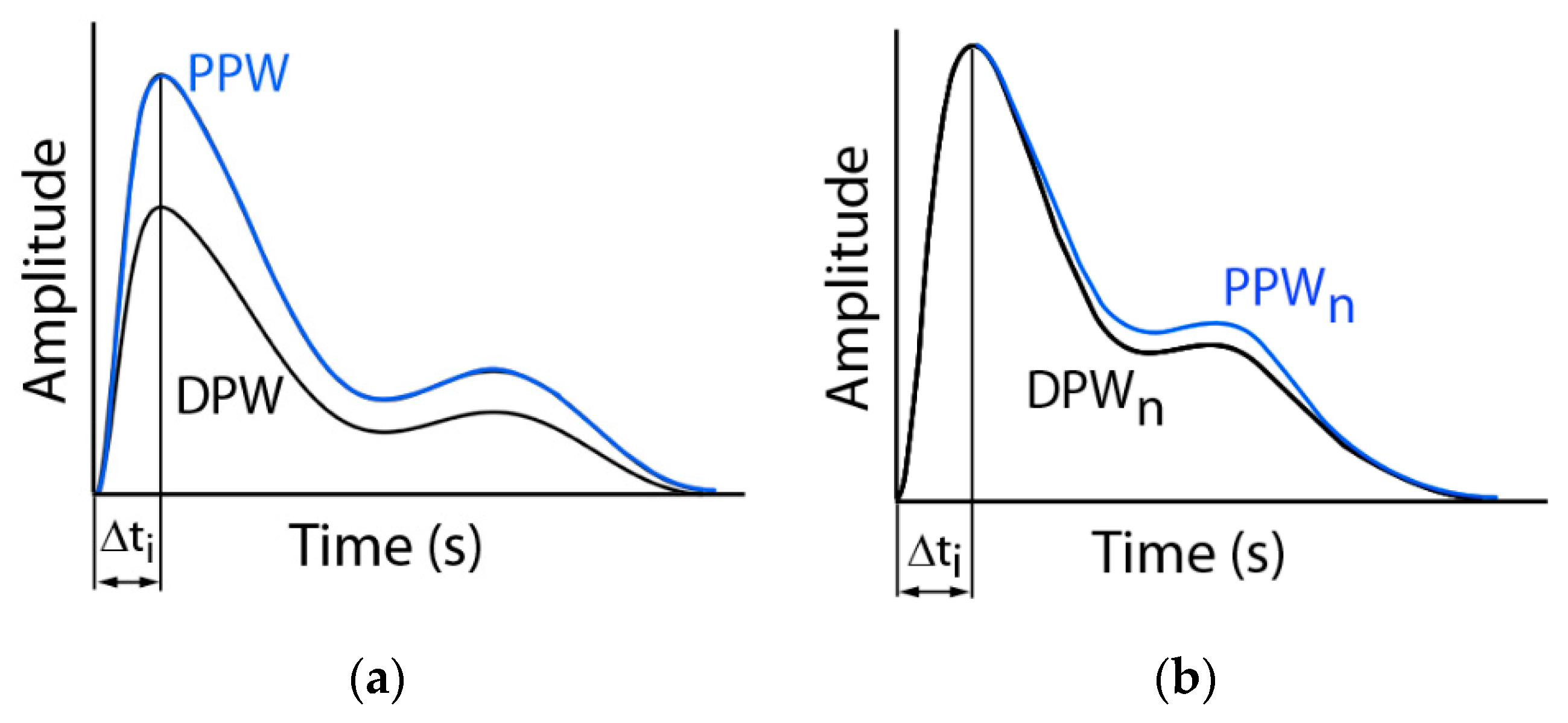
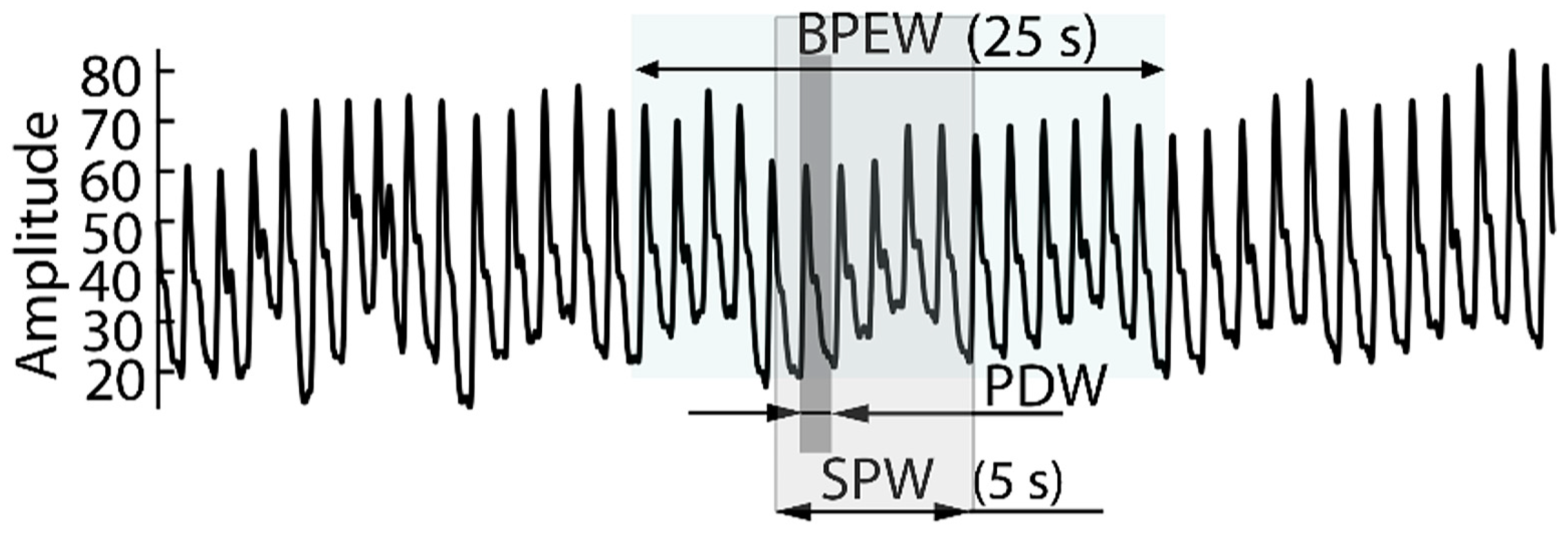
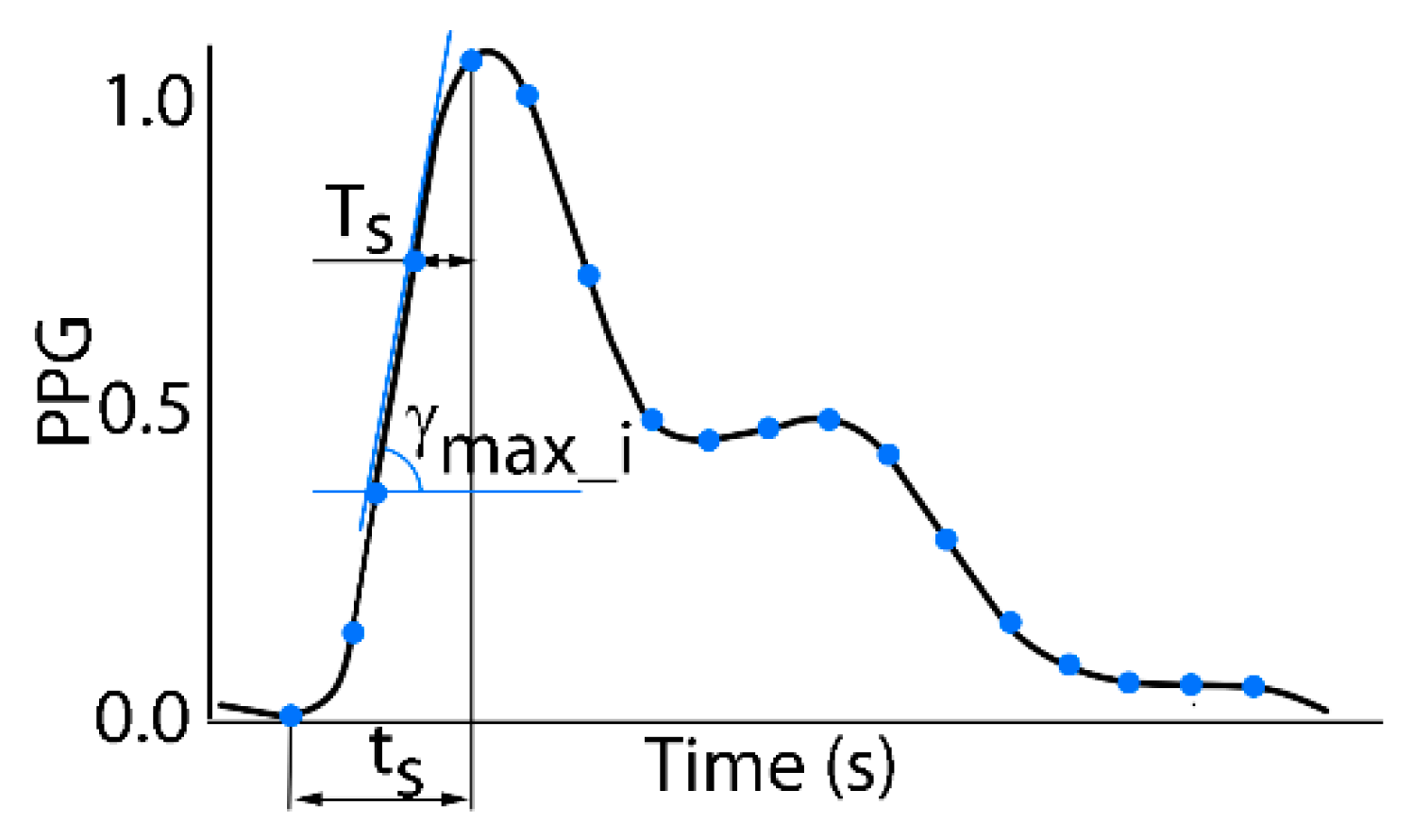
2.1. Systolic Blood Pressure Estimation Model
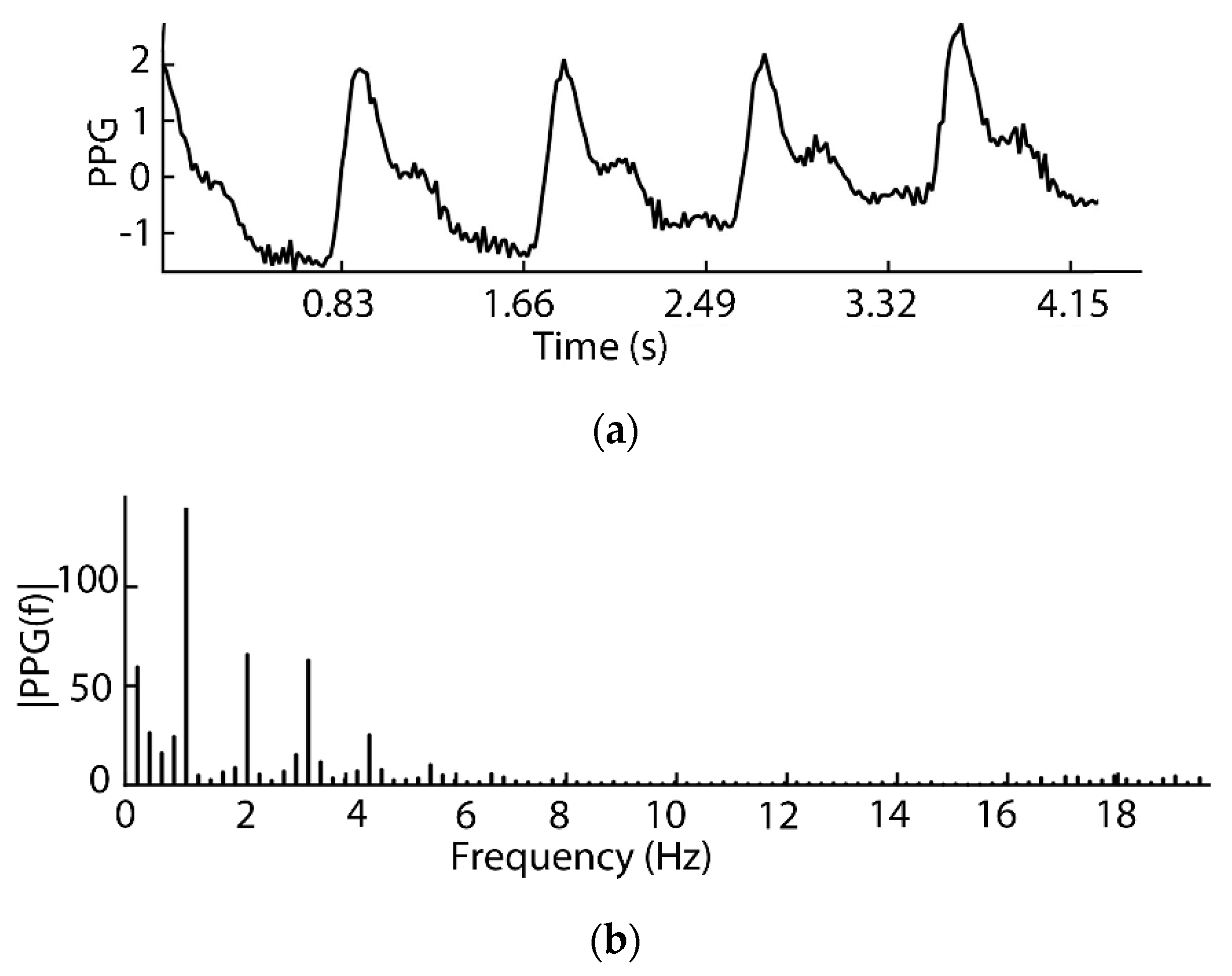
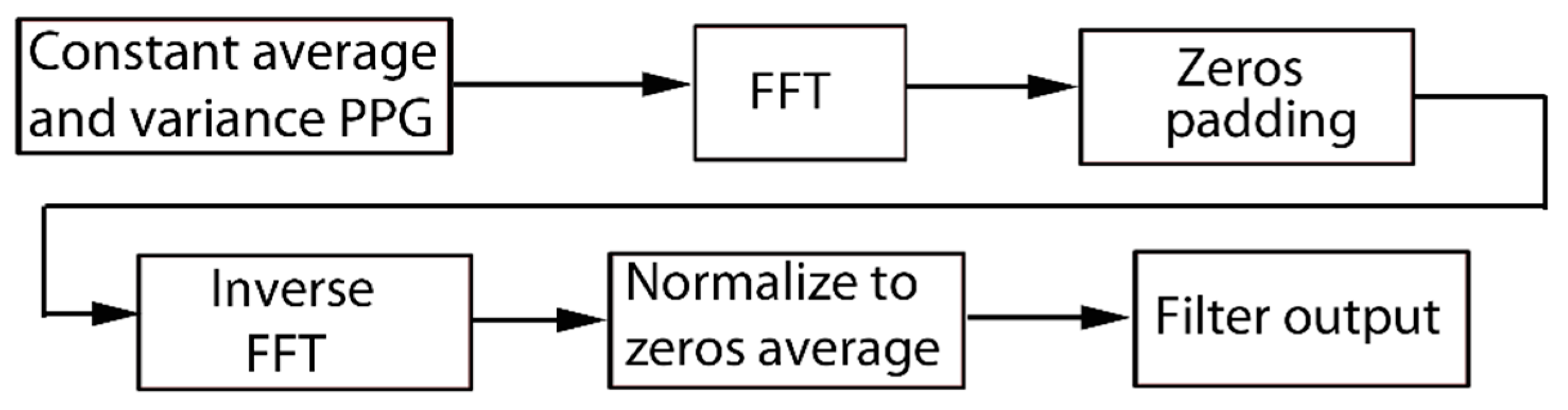
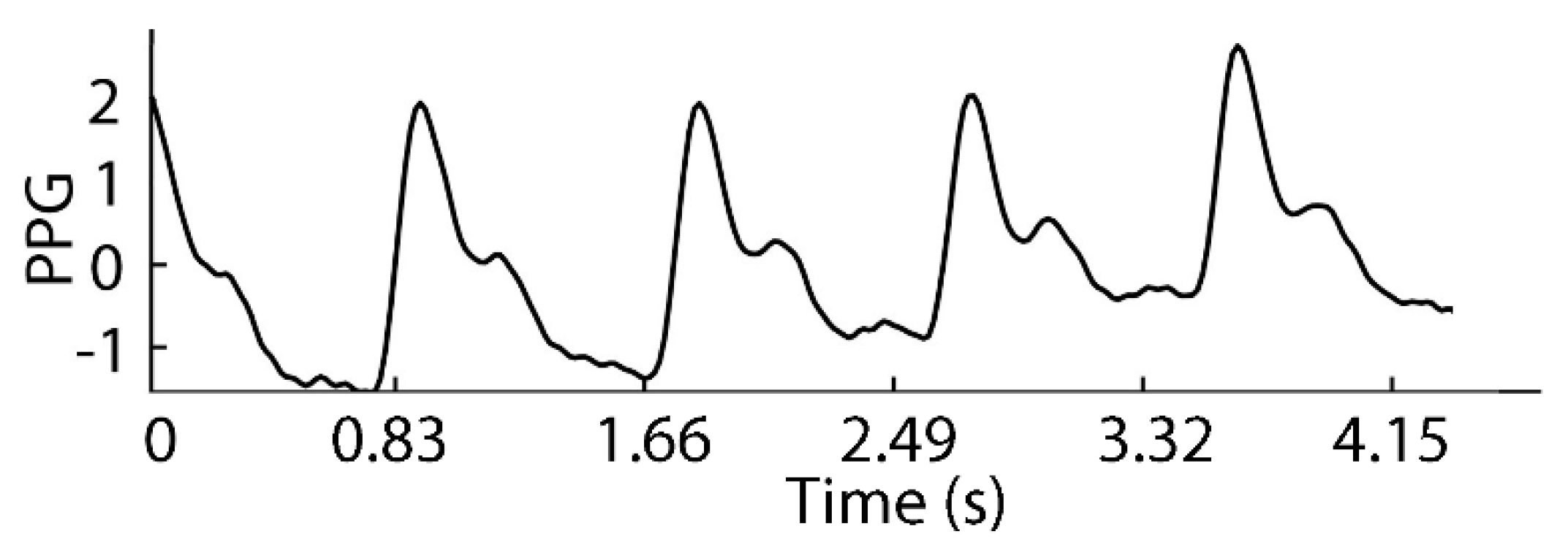
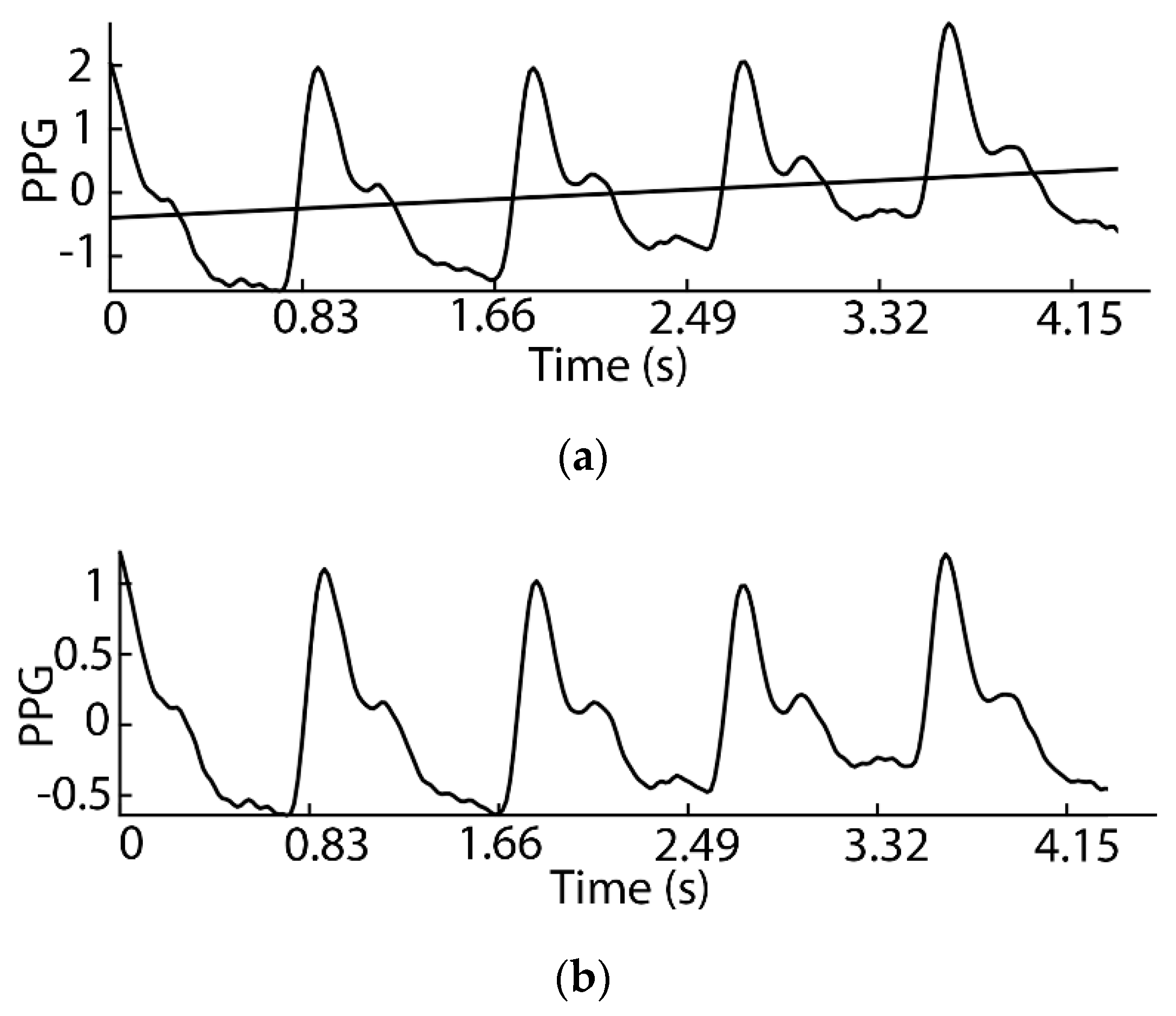
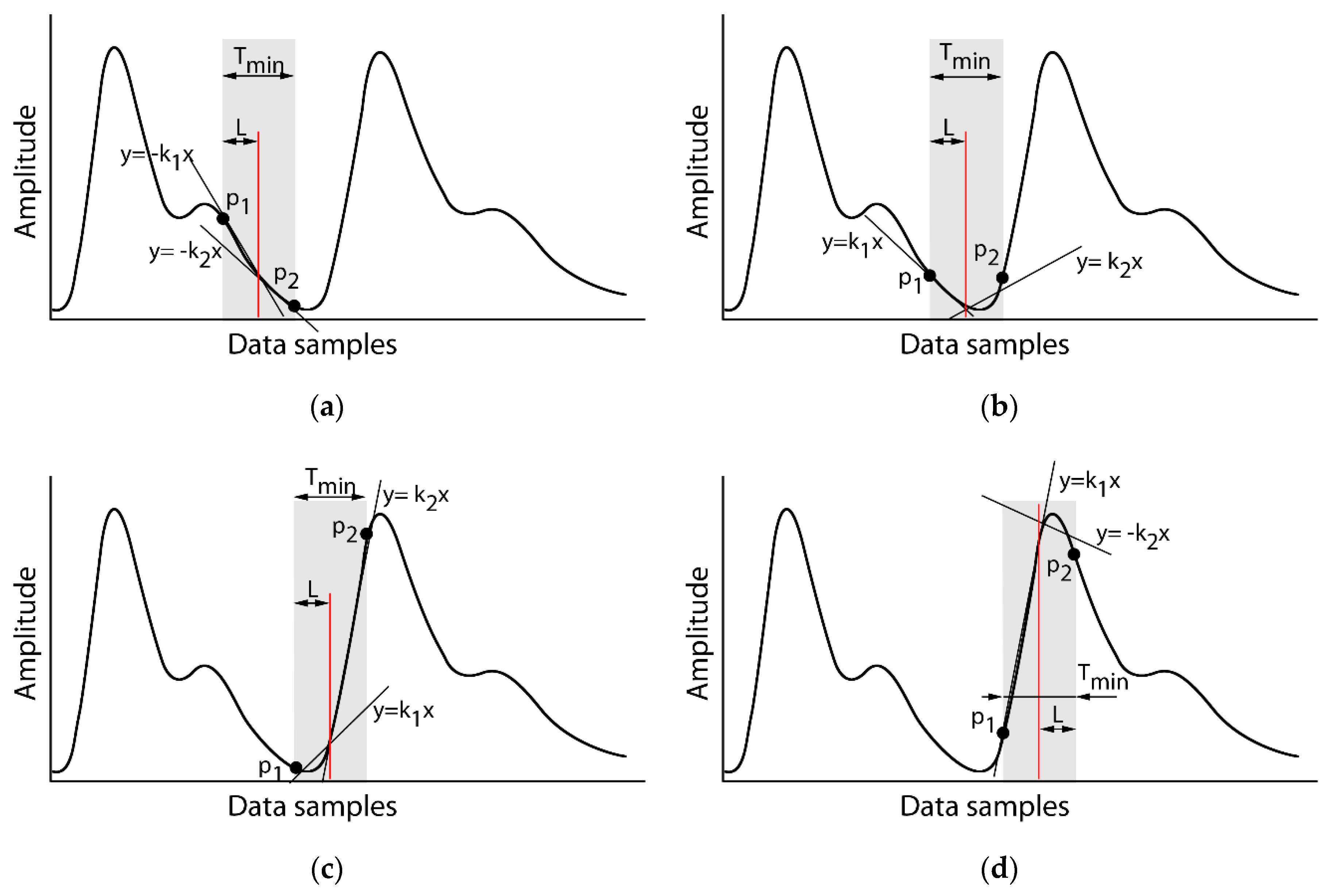
2.2. Signal Preprocessing
| Algorithm 1. PDW size calculation | |
| 1 | procedurepdw (p1, p2) ∇A: Input Signal |
| ∇ mHR: min Heart Rate | |
| 2 | Tmin = (1/mHR)*1/2; L = round(Tmin/Fs); |
| 3 | i = 1; N = length(A)/L; |
| 4 | while (i+1)*L <= N do |
| 5 | [k1, c] = linaprox(A(i*L-L+1: i*L)) |
| 6 | [k2, c] = linaprox(A(i*L:(i+1)*L)) |
| 7 | if k1 > 0 and k2 < 0 |
| 8 | then p1 =i*L-L+1; p2 = (i+1)*L; |
| 9 | goto 16 line |
| 10 | end |
| 11 | if (k1 < 0 and k2 < 0) or (k1 < 0 and k2 > 0) |
| 12 | then i = i + 1; goto 15 line |
| 13 | if (k1 > 0 and k2 > 0) |
| 14 | then L = L + 0.1*L; |
| 15 | end /*While*/ |
| 16 | end |
2.3. Systolic Blood Pressure Estimation Algorithm
2.4. Experiment Setup
3. Results
4. Discussion
4.1. Advantage
4.2. Limitation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jacob, V.; Chattopadhyay, S.K.; Proia, K.K.; Hopkins, D.P.; Reynolds, J.; Thota, A.B.; Jones, C.D.; Lackland, D.T.; Rask, K.J.; Pronk, N.P.; et al. Economics of self-measured blood pressure monitoring: A community guide systematic review. Am. J. Prev. Med. 2017, 53, e105–e113. [Google Scholar] [CrossRef] [PubMed]
- Sankar, J.; Mahesh, N.; Sharma, P.; Sankar, L.; Balasubramanian, A. Role of ambulatory blood pressure monitoring in chronic hypertensive patients on antihypertensive therapy-a cross-sectional study. J. Clin. Diagn. Res. 2018, 12, OC01–OC04. [Google Scholar] [CrossRef]
- Liu, Z.; Zhao, Y.; Lu, F.; Zhang, H.; Diao, Y. Day-by-day variability in self-measured blood pressure at home: Effects on carotid artery atherosclerosis, brachial flow-mediated dilation, and endothelin-1 in normotensive and mild–moderate hypertensive individuals. Blood Press. Monit. 2013, 18, 316–325. [Google Scholar] [CrossRef]
- Toriumi, S.; Hoshide, S.; Nagai, M.; Kario, K. Day-to-day blood pressure variability as a phenotype in a high-risk patient: Letters to the Editor. Geriatr. Gerontol. Int. 2014, 14, 1005–1006. [Google Scholar] [CrossRef]
- Pan, J.; Zhang, Y. Improved blood pressure estimation using photoplethysmography based on ensemble method. In Proceedings of the 2017 14th International Symposium on Pervasive Systems, Algorithms and Networks & 2017 11th International Conference on Frontier of Computer Science and Technology & 2017 Third International Symposium of Creative Computing (ISPAN-FCST-ISCC), Exeter, UK, 21–23 June 2017; pp. 105–111. [Google Scholar]
- Lewington, S.L.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [PubMed]
- Asia Pacific Cohort Studies Collaboration. Blood pressure indices and cardiovascular disease in the asia pacific region: A pooled analysis. Hypertension 2003, 42, 69–75. [Google Scholar] [CrossRef]
- Lawes, C.M.; Hoorn, S.V.; Rodgers, A. Global burden of blood-pressure-related disease, 2001. Lancet 2008, 371, 1513–1518. [Google Scholar] [CrossRef]
- Bose, S.S.N.; Kandaswamy, A. Sparse representation of photoplethysmogram using K-SVD for cuffless estimation of arterial blood pressure. In Proceedings of the 2017 4th International Conference on Advanced Computing and Communication Systems (ICACCS), Coimbatore, India, 6–7 January 2017; pp. 1–5. [Google Scholar]
- Mousavi, S.S.; Firouzmand, M.; Charmi, M.; Hemmati, M.; Moghadam, M.; Ghorbani, Y. Blood pressure estimation from appropriate and inappropriate PPG signals using A whole-based method. Biomed. Signal Process. Control 2019, 47, 196–206. [Google Scholar] [CrossRef]
- Taylor, B.C.; Wilt, T.J.; Welch, H.G. Impact of diastolic and systolic blood pressure on mortality: Implications for the definition of “normal”. J. Gen. Intern. Med. 2011, 26, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, P.M.; Howard, S.C.; Dolan, E.; O’Brien, E.; Dobson, J.E.; Dahlöf, B.; Sever, P.S.; Poulter, N.R. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet 2010, 375, 895–905. [Google Scholar] [CrossRef]
- Lin, W.-H.; Wang, H.; Samuel, O.W.; Li, G. Using a new PPG indicator to increase the accuracy of PTT-based continuous cuffless blood pressure estimation. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seogwipo, Korea, 11–15 July 2017; pp. 738–741. [Google Scholar]
- Khan, N.; Mikael Eklund, J. A Highly integrated computing platform for continuous, non-invasive bp estimation. In Proceedings of the 2018 IEEE Canadian Conference on Electrical & Computer Engineering (CCECE), Quebec City, QC, Canada, 13–16 May 2018; pp. 1–5. [Google Scholar]
- Ding, X.-R.; Zhang, Y.-T.; Liu, J.; Dai, W.-X.; Tsang, H.K. Continuous cuffless blood pressure estimation using pulse transit time and photoplethysmogram intensity ratio. IEEE Trans. Biomed. Eng. 2016, 63, 964–972. [Google Scholar] [CrossRef]
- Zhang, J.M.; Wei, P.F.; Li, Y. A LabVIEW based measure system for pulse wave transit time. In Proceedings of the 2008 International Conference on Technology and Applications in Biomedicine, Shenzhen, China, 18 July 2008; pp. 477–480. [Google Scholar]
- Liu, S.-H.; Cheng, D.-C.; Su, C.-H. A cuffless blood pressure measurement based on the impedance plethysmography technique. Sensors 2017, 17, 1176. [Google Scholar] [CrossRef]
- Liu, H.; Ivanov, K.; Wang, Y.; Wang, L. Toward a smartphone application for estimation of pulse transit time. Sensors 2015, 15, 27303–27321. [Google Scholar] [CrossRef]
- Khalid, S.G.; Zhang, J.; Chen, F.; Zheng, D. Blood pressure estimation using photoplethysmography only: comparison between different machine learning approaches. J. Healthc. Eng. 2018, 2018, 1–13. [Google Scholar] [CrossRef]
- Choudhury, A.D.; Banerjee, R.; Sinha, A.; Kundu, S. Estimating blood pressure using Windkessel model on photoplethysmogram. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 4567–4570. [Google Scholar]
- Xing, X.; Sun, M. Optical blood pressure estimation with photoplethysmography and FFT-based neural networks. Biomed. Opt. Express 2016, 7, 3007–3020. [Google Scholar] [CrossRef]
- Kurylyak, Y.; Barbe, K.; Lamonaca, F.; Grimaldi, D.; Van Moer, W. Photoplethysmogram-based Blood pressure evaluation using Kalman filtering and Neural Networks. In Proceedings of the 2013 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Gatineau, QC, Canada, 4–5 May 2013; pp. 170–174. [Google Scholar]
- Kao, Y.-H.; Chao, P.C.-P.; Tu, T.-Y.; Chiang, K.-Y.; Wey, C.-L. A new cuffless optical sensor for blood pressure measuring with self-adaptive signal processing. In Proceedings of the 2016 IEEE SENSORS, Orlando, FL, USA, 30 October–3 November 2016; pp. 1–3. [Google Scholar]
- Cohen, Z.; Haxha, S. Optical-based sensor prototype for continuous monitoring of the blood pressure. IEEE Sens. J. 2017, 17, 4258–4268. [Google Scholar] [CrossRef]
- Yan, Y.S.; Zhang, Y.T. Noninvasive estimation of blood pressure using photoplethysmographic signals in the period domain. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 3583–3584. [Google Scholar]
- Gaurav, A.; Maheedhar, M.; Tiwari, V.N.; Narayanan, R. Cuff-less PPG based continuous blood pressure monitoring—A smartphone based approach. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 607–610. [Google Scholar]
- Matsumura, K.; Rolfe, P.; Toda, S.; Yamakoshi, T. Cuffless blood pressure estimation using only a smartphone. Sci. Rep. 2018, 8, 7298. [Google Scholar] [CrossRef]
- Tobola, A.; Streit, F.J.; Espig, C.; Korpok, O.; Sauter, C.; Lang, N.; Schmitz, B.; Hofmann, C.; Struck, M.; Weigand, C.; et al. Sampling rate impact on energy consumption of biomedical signal processing systems. In Proceedings of the 2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015; pp. 1–6. [Google Scholar]
- Gircys, R.; Liutkevicius, A.; Vrubliauskas, A.; Kazanavicius, E. Blood pressure estimation accoording to photoplethysmographic signal steepness. Inf. Technol. Control 2015, 44, 443–450. [Google Scholar] [CrossRef]
- Harada, A.; Okada, T.; Niki, K.; Chang, D.; Sugawara, M. On-line noninvasive one-point measurements of pulse wave velocity. Heart Vessel. 2002, 17, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Diourté, B.; Siché, J.-P.; Comparat, V.; Baguet, J.-P.; Mallion, J.-M. Study of arterial blood pressure by a Windkessel-type model: Influence of arterial functional properties. Comput. Methods Programs Biomed. 1999, 60, 11–22. [Google Scholar] [CrossRef]
- Sugawara, M.; Niki, K.; Furuhata, H.; Ohnishi, S.; Suzuki, S. Relationship between the pressure and diameter of the carotid artery in humans. Heart Vessel. 2000, 15, 49–51. [Google Scholar] [CrossRef]
- Elgendi, M. Detection of c, d, and e waves in the acceleration photoplethysmogram. Comput. Methods Programs Biomed. 2014, 117, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Song, H.-S.; Lehrer, P.M. The effects of specific respiratory rates on heart rate and heart rate variability. Appl. Psychophysiol. Biofeedback 2003, 28, 13–23. [Google Scholar] [CrossRef] [PubMed]
- AL-Khalidi, F.Q.; Saatchi, R.; Burke, D.; Elphick, H.; Tan, S. Respiration rate monitoring methods: A review. Pediatric Pulmonol. 2011, 46, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Charlton, P.H.; Villarroel, M.; Salguiero, F. Waveform analysis to estimate respiratory rate. In Secondary Analysis of Electronic Health Records; Springer International Publishing: Cham, Switzerland, 2016; pp. 377–390. ISBN 978-3-319-43740-8. [Google Scholar]
- Jennings, J.R.; McKnight, J.D.; Molen, M. Phase-sensitive interaction of cardiac and respiratory timing in humans. Psychophysiology 1996, 33, 514–521. [Google Scholar] [CrossRef]
- Sadrawi, M.; Shieh, J.-S.; Fan, S.Z.; Lin, C.H.; Haraikawa, K.; Chien, J.C.; Abbod, M.F. Intermittent blood pressure prediction via multiscale entropy and ensemble artificial neural networks. In Proceedings of the 2016 IEEE EMBS Conference on Biomedical Engineering and Sciences (IECBES), Kuala Lumpur, Malaysia, 4–8 December 2016; pp. 356–359. [Google Scholar]
- Bhoi, A.K.; Sarkar, S.; Mishra, P.; Savita, G. Pre-processing of PPG signal with performance based methods. Int. J. Comput. Appl. 2012, 4, 251–256. [Google Scholar]
- Lee, C.M.; Zhang, Y.T. Reduction of motion artifacts from photoplethysmographic recordings using a wavelet denoising approach. In Proceedings of the IEEE EMBS Asian-Pacific Conference on Biomedical Engineering, Kyoto, Japan, 20–22 October 2003; pp. 194–195. [Google Scholar]
- Boloursaz Mashhadi, M.; Asadi, E.; Eskandari, M.; Kiani, S.; Marvasti, F. Heart rate tracking using wrist-type photoplethysmographic (PPG) signals during physical exercise with simultaneous accelerometry. IEEE Signal Process. Lett. 2016, 23, 227–231. [Google Scholar] [CrossRef]
- Wang, D.; Zhang, D.; Lu, G. A robust signal preprocessing framework for wrist pulse analysis. Biomed. Signal Process. Control 2016, 23, 62–75. [Google Scholar] [CrossRef]
- Alian, A.A.; Shelley, K.H. Photoplethysmography: Analysis of the pulse oximeter waveform. In Monitoring Technologies in Acute Care Environments; Ehrenfeld, J.M., Cannesson, M., Eds.; Springer: New York, NY, USA, 2014; pp. 165–178. ISBN 978-1-4614-8556-8. [Google Scholar]
- Kavsaoğlu, A.R.; Polat, K.; Bozkurt, M.R. An innovative peak detection algorithm for photoplethysmography signals: An adaptive segmentation method. Turk. J. Electr. Eng. Comput. Sci. 2016, 24, 1782–1796. [Google Scholar] [CrossRef]
- Kazanavicius, E.; Gircys, R.; Vrubliauskas, A.; Lugin, S. Mathematical methods for determining the foot point of the arterial pulse wave and evaluation of proposed methods. Inf. Technol. Control 2005, 34, 29–36. [Google Scholar]
- Banerjee, R.; Ghose, A.; Dutta Choudhury, A.; Sinha, A.; Pal, A. Noise cleaning and Gaussian modeling of smart phone photoplethysmogram to improve blood pressure estimation. In Proceedings of the 2015 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), South Brisbane, Queensland, Australia, 19–24 April 2015; pp. 967–971. [Google Scholar]
- Akl, T.J.; Wilson, M.A.; Ericson, M.N.; Coté, G.L. Quantifying tissue mechanical properties using photoplethysmography. Biomed. Opt. Express 2014, 5, 2362–2375. [Google Scholar] [CrossRef] [PubMed]
- Datta, S.; Banerjee, R.; Choudhury, A.D.; Sinha, A.; Pal, A. Blood pressure estimation from photoplethysmogram using latent parameters. In Proceedings of the 2016 IEEE International Conference on Communications (ICC), Kuala Lumpur, Malaysia, 22–27 May 2016; pp. 1–7. [Google Scholar]
- White, W.B.; Berson, A.S.; Robbins, C.; Jamieson, M.J.; Prisant, L.M.; Roccella, E.; Sheps, S.G. National standard for measurement of resting and ambulatory blood pressures with automated sphygmomanometers. Hypertension 1993, 21, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Int. J. Nurs. Stud. 2010, 47, 931–936. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| r (p < 0.001) | MD | SD | er, % |
|---|---|---|---|
| 0.86 | −0.043 | 6.79 | 0.025 ± 5.44 |
| Methods | Systolic Blood Pressure Method Performance | ||
|---|---|---|---|
| MD | SD | SPS | |
| Proposed method | −0.043 | 6.79 | 60 Hz |
| Ding [15] | 0.37 | 5.21 | 1 KHz |
| Lin [13] | 3.22 | 8.02 | 1 KHz |
| Yan [25] | −0.37 | 4.3 | 200 Hz |
| Kurylyak [22] | 3.24 | 3.47 | 125 Hz |
| Choudhury [20] | 0.78 | 13.1 | 100 Hz |
| Khalid [19] | −1.1 | 5.7 | 100 Hz |
| Xing [21] | −1.67 | 2.46 | 100 Hz |
| Mousavi [10] Method 1 | 0.25 | 6.7 | 125 Hz |
| Method 2 | 0.66 | 7.5 | 125 Hz |
| Method 3 | 0.19 | 4.17 | 125 Hz |
| Method 4 | 0.2 | 4.73 | 125 Hz |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gircys, R.; Liutkevicius, A.; Kazanavicius, E.; Lesauskaite, V.; Damuleviciene, G.; Janaviciute, A. Photoplethysmography-Based Continuous Systolic Blood Pressure Estimation Method for Low Processing Power Wearable Devices. Appl. Sci. 2019, 9, 2236. https://doi.org/10.3390/app9112236
Gircys R, Liutkevicius A, Kazanavicius E, Lesauskaite V, Damuleviciene G, Janaviciute A. Photoplethysmography-Based Continuous Systolic Blood Pressure Estimation Method for Low Processing Power Wearable Devices. Applied Sciences. 2019; 9(11):2236. https://doi.org/10.3390/app9112236
Chicago/Turabian StyleGircys, Rolandas, Agnius Liutkevicius, Egidijus Kazanavicius, Vita Lesauskaite, Gyte Damuleviciene, and Audrone Janaviciute. 2019. "Photoplethysmography-Based Continuous Systolic Blood Pressure Estimation Method for Low Processing Power Wearable Devices" Applied Sciences 9, no. 11: 2236. https://doi.org/10.3390/app9112236
APA StyleGircys, R., Liutkevicius, A., Kazanavicius, E., Lesauskaite, V., Damuleviciene, G., & Janaviciute, A. (2019). Photoplethysmography-Based Continuous Systolic Blood Pressure Estimation Method for Low Processing Power Wearable Devices. Applied Sciences, 9(11), 2236. https://doi.org/10.3390/app9112236