1. Introduction
Basketball is a team sport that demands a high level of physical fitness to manage the intense physical effort required during the game [
1,
2]. It is a physically demanding sport that involves constant changes in pace, direction, and speed, frequent jumps and landings, intense physical contact, and essential technical and tactical skills. Therefore, basketball athletes, and especially adolescents, are at high risk of injuries [
3,
4]. Knee injuries, especially, are common among adolescent basketball athletes, with incidence rates ranging from 1.52 injuries per 10,000 athlete-exposures to a seasonal prevalence of 25.3% for anterior knee pain [
5,
6,
7].
Dynamic knee valgus (DKV), characterized by the inward collapse of the knee during dynamic movements, has been widely associated with an increased risk of injury, particularly in sports, like basketball, that involve high-intensity activities, such as running, jumping, landing, and cutting [
8,
9,
10,
11]. This abnormal knee motion is often observed during single-leg movements, such as a single-leg landing or a change of direction, and can contribute to the development of conditions such as anterior cruciate ligament (ACL) injuries and patellofemoral pain syndrome, especially in adolescent populations [
3,
4,
12,
13,
14,
15].
The biomechanical mechanisms underlying DKV are complex and multifactorial, involving both neuromuscular control and structural alignment [
11,
16]. However, an emerging body of evidence suggests that physical fitness or physical abilities may play a significant role in the manifestation of DKV during dynamic tasks that lead to sport injuries [
16,
17,
18,
19,
20,
21].
Identifying modifiable risk factors for sports-related knee injuries is crucial for developing effective prevention strategies [
21,
22,
23,
24,
25]. The definition of physical fitness is a collection of characteristics that a person possesses or achieves that pertain to their capacity to carry out daily duties. Some of the major components of physical fitness are balance, agility, cardiorespiratory fitness, body composition, flexibility, muscle strength, muscle power, muscle endurance, reaction time, and speed [
21,
26,
27].
Lower limb muscle power (LLMP), which refers to the ability of the muscles in the legs to produce force rapidly, has been implicated as a key determinant of knee stability during dynamic movements [
20,
28,
29]. Research has shown that deficits in lower limb strength and power are associated with an increased risk of knee valgus [
29,
30,
31].
Cardiorespiratory fitness (CRF), a measure of the efficiency of the cardiovascular and respiratory systems in supporting sustained physical activity, has also been shown to influence knee control in dynamic tasks [
18,
20,
32]. While the link between aerobic fitness and knee valgus may not be as immediately apparent as that of muscle power, emerging evidence suggests that individuals with higher CRF tend to display improved neuromuscular control during dynamic tasks [
21,
24,
33].
The relationship among lower limb LLMP, CRF, and DKV has important implications for injury prevention and rehabilitation programs. Previous studies have indicated that training programs focused on improving lower limb strength and muscle power, as well as aerobic fitness, can mitigate the risk of dynamic knee valgus by improving neuromuscular control and muscle coordination [
21,
30,
34,
35]. Interventions that target these physical abilities may not only reduce the occurrence of knee valgus but also enhance overall athletic performance and reduce the risk of long-term musculoskeletal disorders.
To further investigate how different physical fitness attributes correlate with DKV, a reanalysis of data previously published in the studies of Stojiljkovic (2024) and Karagianni (2025) was performed [
17,
32]. This approach allowed for a deeper examination of how multifactorial a movement such as DKV can be and provides new insights into the variables that should be trained to have a positive impact on the prevention of such injury-prone movements.
Up to now in the literature, there is limited research on adolescent basketball athletes in Greece, and the assessment of physical abilities has mainly been performed with the use of expensive equipment. In this study, it was chosen to use simpler methods because many teams and team’s academies do not have access to expensive assessment equipment.
Lower limb muscle power (LLMP) and cardiorespiratory fitness (CRF) were chosen over other potential factors due to their strong influence on DKV and their practical applicability in athletic settings [
23,
24,
36]. By examining the correlations between muscle power or cardiorespiratory fitness we aim to provide a comprehensive understanding of their association with knee control to propose better practices for athletic training, injury prevention, and clinical rehabilitation.
2. Materials and Methods
2.1. Study Design
Prior to the study, the study protocol was approved by the Ethics Committee of the Department of Physiotherapy at the University of Thessaly (1083/21-10-2022). The study was performed following the principles in the Declaration of Helsinki; thus, it was consistent with the value of respect for the volunteers who would participate.
2.2. Sample
The present study is based on a reanalysis of data from the studies of Stojiljkovic (2024) and Karagianni (2025) originally collected for correlating anthropometric characteristics and movement behavior with DKV and modeling associations of the cardiometabolic profile with sedentary behavior [
17,
32]. The dataset was re-examined using different variables and new statistical approaches to explore the association of novel physical fitness attributes with DKV.
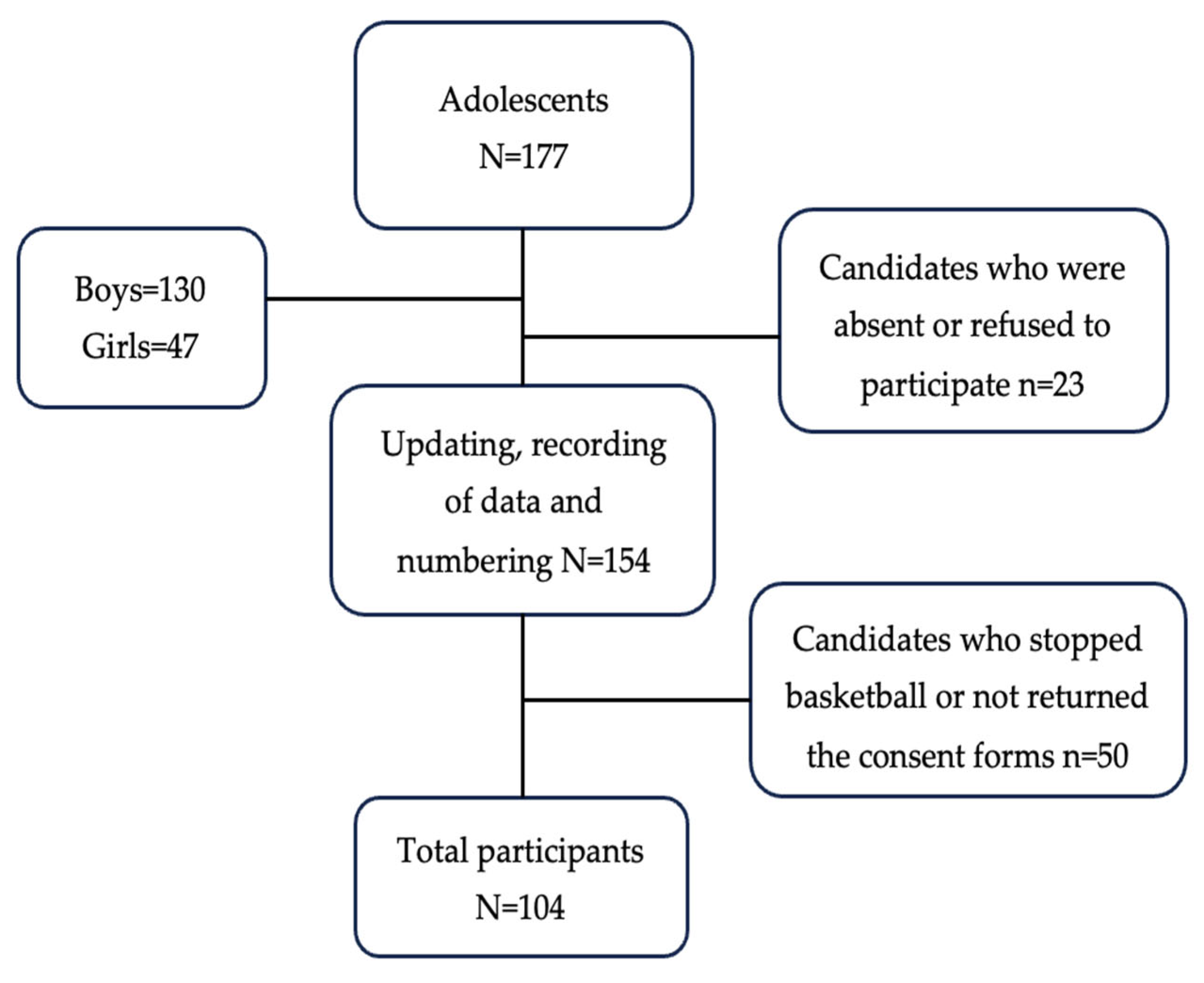
The study sample’s characteristics, as described in the studies of Stojiljkovic et al. (2024) and Karagianni (2025), were adolescents from two basketball academies from two different cities in Central Greece [
17,
32]. The final sample consisted of 104 adolescents (63.5% males, 36.5% females) from the 177 available (
Figure 1).
The eligibility criteria were (a) adolescents aged between 12 and 17 years, (b) no lower limb injuries in the last 3 months or any other comorbidity (e.g., illness, cognitive or neurological condition) precluding exercise implementation, and (c) parents who signed informed consent [
17]. The sample size was calculated using the G*Power 3.1.9.4 program with a 95% confidence level and a significance level of 5% or 0.05.
2.3. Data Collection
Data collection was performed daily, for 5 days per week, during the scheduled afternoon basketball practices for 8 weeks. Three independent physiotherapists, who were trained on the testing procedures prior to the beginning of the study, under the supervision of the research team, performed all the measurements and data collection. The measurements were taken without the presence of the study’s main investigator. Initially, all the data were recorded on a laptop and backed up on an external hard drive. At the completion of all measurements, access to data was given to the main researcher for data processing.
2.4. Equipment
For the sample’s anthropometric characteristics’ measurements, a precision electronic ultrasonic stadiometer (SOEHNLE 5003, Spaichingen, Germany) and a precision electronic weighting scale (TANITA BC418-MA, Tokyo, Japan) were used to calculate the participants’ height and weight and Body Mass Index (BMI) [
37,
38].
For the recording of the tests, a Go Pro camera (4K, 30fps, San Mateo, CA, USA) that was mounted on a tripod at a height of 50 cm from the ground and 3 m in of the point of where the tests were performed, a laptop, 5 reflective markers, and a 30 cm-height wooden box were used to collect the data from the countermovement jump test and the single-leg drop jump test.
The Kinovea software (2023.1.2) was used for the 2-dimensional analysis, since its validity and reliability have been demonstrated as good to excellent for the kinematic analysis of the single-leg drop jump (SLDJ) to assess DKV and for the measurement of jump height in the countermovement jump (CMJ) [
39,
40,
41,
42,
43].
For the evaluation of CRF, the 20 m shuttle run test (20mSRT) or beep test was used, which is a valid and reliable cardiorespiratory test [
44,
45]. Based on the original application, the 20mSRT was executed using the Beep Shuttle Advanced VER0320 program, and a standard procedure was followed [
45,
46].
2.5. Assessment
All the data-collection procedures and measuring tests were conducted on the practice facilities (basketball courts) of the two participating teams (
Figure 2).
For the height assessment, the participants stood tall barefoot, in a straight position, with their heels touching each other and their eyes looking straight forward to be at the same height with their ears. For the weight assessment, participants had to stand on the scale barefoot and keep steady until their weight was indicated on the scale.
The BMI was calculated in accordance with the International System (SI) units with the following formula: Body Mass Index = weight (kg)/height
2 (m
2), and depending on the result, each participant was categorized as a z-score in three categories: normal/overweight/obese [
37,
38,
47].
After recording the anthropometric characteristics, an appropriate warm-up that consisted of basketball-related running drills and movements, lay ups, and shots for 10 min was suggested for the implementation of the dynamic tests.
Prior to testing, 5 reflective markers were placed on each participant’s dominant leg as reference points (
Figure 3). The dominant leg was determined depending on the participant’s answer on which leg he/she would use to kick a ball [
43,
48]. The anatomical landmarks were the anterior superior iliac spine, the lateral and medial femoral condyle, and the lateral and medial malleolus [
43,
48]. Before each test, athletes went through a familiarization process each having 3 trials on the CMJ and SLDJ tests.
The CMJ was the test used for the prediction of LLMP. Each participant performed two jumps with a 1 min rest in between. The instructions given were to jump as high as possible and with the hands always on their waist to not be able to use them [
49]. A trial was considered valid only if the participant did not lose balance or fall during the test and did not use arm swing [
49].
For the prediction of the LLMP, an equation was used, utilizing the participant’s jump height and weight [
49]. The height of the best performing jump was picked after a 2D kinematic analysis of both trials. This equation showed the highest accuracy rates and reliability (R = 0.93, R
2 = 0.87) in the existing literature. The equation used was as follows [
49]:
For the SLDJ test, each participant stepped up and dropped off a 30 cm box and landed on their dominant leg, immediately performed a direct single leg jump as high as possible, and landed on the same leg again [
43,
48]. The instructions given were to remain still on the final landing for at least 2 s [
43,
48]. A trial was not considered valid only if the participant jumped instead of dropped off the box, if the non-supporting leg touched the floor throughout the test, and if he/she lost balance or fall on the final landing [
43,
48].
For the calculation of the DKV angle, the first three valid trials were selected for the kinematic analysis. Two axes were conducted, with the first axis corresponding to the femur and was considered the line from the anterior superior iliac spine to the middle of the distance between the reflective markers on the knee. The second axis was corresponding to the tibia bone and started from the middle point of the distance between the two markers on the knee to the midpoint of the distance between the two markers on the ankle [
43,
48]. The smaller the angle formed by the two axes, which will be referred as the Frontal Plane Projection Angle (FPPA), the bigger the DKV angle. The angle of DKV selected for analysis was when the knee showed the maximum FPPA after contact with the ground.
The 20mSRT was conducted last because it was the most demanding between the tests, and if it was performed first, the fatigue could alter the other tests and consequently their results [
45]. The participants had to continuously keep running between two points for a 20 m distance, which was considered one run (
Figure 4). To start running from one point to the other, the participants had to hear the characteristic “beep” sound from the audio feedback. The starting running speed was 8.5 km/h, and it increased every minute (new level) per 0.25 km/h with a special tone heard through the audio feedback [
45]. The criteria for test termination were if the participant was not able to continue running due to fatigue or any other symptoms, if the participant failed to reach one of the two limit points on time, or if the participant completed all the levels [
45].
For the estimation of CRF, a valid and reliable equation was used, utilizing each participant’s performance data on the 20mSRT, which was delivered through the application [
44,
45]. For each participant, performance was recorded as the number of runs completed, and the running speed of the final level for each participant and his/her age were used for the calculation of the maximum oxygen uptake (VO
2max) [
45]. The equation used was as follows [
45]:
2.6. Data Analysis
The two-dimensional (2D) analysis program Kinovea was used to analyze the CMJ and the SLDJ. The use of Kinovea software in evaluating athletic movements such as the countermovement jump and single-leg landing is well documented, and the results show that it is a valid and reliable tool [
39,
40,
42,
43,
48].
For the statistical analysis, the Statistical Package for Social Sciences (SPSS) V.29.0 was used. For data analysis and calculations, Microsoft Office Excel 2013 was utilized. The significance level was set at p = 0.05.
LLMP and CRF were defined as independent variables, while the FPPA was defined as the dependent variable.
Descriptive statistics (mean, standard deviation) were calculated for all the variables to provide an overview of the sample’s characteristics. Kolmogorov–Smirnov and Shapiro–Wilk tests indicated that height, BMI, power, and FPPA followed a normal distribution, while the other variables would require non-parametric statistical approaches. An independent samples t-test and Mann–Whitney U test were used in order to investigate differences between groups (boys vs. girls). Pearson’s and Spearman’s coefficients were used to measure the strength and direction of the associations, while a multiple linear regression analysis was used to assess the ability of the variables selected to predict FPPA. The regression analysis model included an analysis of variance (ANOVA) to evaluate the overall significance of the model.
3. Results
A total of 104 adolescents participated in the study (66 boys and 38 girls). A descriptive analysis revealed an average participant’s age of 13.87 ± 1.46 years, height of 1.65 ± 0.1 m, an average weight of 62.52 ± 14.92 kg, and an average BMI of 22.71 ± 3.9 kg/m
2. The average LLMP was 2626.11 ± 734.78 Watts, VO
2max was 39.66 ± 3.85 mL/kg/min, and FPPA was 163.4 ± 7.7°. Descriptive statistics are presented in
Table 1.
The normality tests Kolmogorov–Smirnov and Shapiro–Wilk revealed that the variables height, power, and VO
2max did not significantly deviate from a normal distribution (
p > 0.05), whereas age, weight, BMI, and FPPA significantly deviated from normality (
p < 0.05) (
Table 2).
To examine potential differences between boys and girls, variables that followed a normal distribution (height, power, and FPPA) were analyzed using independent samples
t-tests, while non-normally distributed variables (age, weight, and VO
2max) were analyzed using Mann–Whitney U tests (
Table 3).
The analysis revealed statistically significant differences between the two genders in power (t (101.99) = 2.483, p = 0.015) and VO2max (U = 539.50, p < 0.001), with boys demonstrating higher values in both variables, indicating that gender may influence LLMP and aerobic capacity. No significant differences were observed in age, height, weight, BMI, or FPPA (all p > 0.05), suggesting that these characteristics are relatively similar between genders.
Pearson and Spearman correlations were performed to assess relationships between the independent variables VO
2max and power and the dependent variable FPPA (
Table 4). Pearson’s correlation coefficient showed a strong positive correlation between VO
2max and power (r = 0.85,
p < 0.001), VO
2max and FPPA (r = 0.78,
p < 0.001), and power and FPPA (r = 0.82,
p < 0.001).
Similarly, Spearman’s correlation coefficients indicated strong positive relationships: VO2max and power (rho = 0.83, p < 0.001), VO2max and FPPA (rho = 0.76, p < 0.001), and power and FPPA (rho = 0.80, p < 0.001). These findings confirm that higher VO2max and power values are strongly associated with increased FPPA.
A multiple linear regression analysis was conducted to predict FPPA using VO
2max and power as independent variables (
Table 5). The regression model demonstrated a strong fit, with an R-squared value of 0.85, indicating that 85% of the variability in FPPA is explained by these two predictors. The adjusted R-squared value of 0.84 further supports the model’s predictive strength.
The ANOVA results confirmed the statistical significance of the model, F (2,101) = 150.7,
p < 0.001. Both independent variables were significant predictors of FPPA, with VO
2max (B = 3.20,
p < 0.001) and power (B = 1.80,
p < 0.001) contributing meaningfully to the regression equation. These findings suggest that increases in VO
2max and power lead to a significant rise in FPPA values. The resulting regression equation was as follows:
These results indicate that both VO2max and LLMP are significant predictors of FPPA in adolescent basketball athletes.
4. Discussion
The objective of the current investigation was to examine the potential correlations between some physical fitness abilities, such as LLMP and CRF fitness, and DKV in adolescent basketball athletes. The study involved young Greek athletes, which make it one of the first national studies to focus on injury pattern analysis for injury prevention in Greece.
The findings of this study provide valuable insights into the relationship between physical fitness attributes and dynamic knee valgus (DKV) in adolescent basketball athletes. The results reveal significant correlations among LLMP, CRF, and DKV, suggesting that these physical attributes are key predictors of frontal plane knee control.
These findings align with previous research, which suggests that deficits in LLMP contribute to increased knee valgus during dynamic movements [
16,
21,
23,
24]. The observed relationships highlight the importance of targeted strength and conditioning programs aimed at enhancing power and aerobic capacity to reduce injury risk.
The multiple linear regression analysis demonstrated that both CRF and LLMP are significant predictors of DKV, with the model explaining 85% of its variability. This suggests that improving these physical attributes can lead to better knee stability and lower injury susceptibility. It must be noted here though that this is an overly simplified model and that other external factors might still contribute to DKV.
VO
2max, which is highly associated with cardiorespiratory fitness and endurance capacity, appears to play a crucial role in sustaining neuromuscular control during prolonged physical activity [
20,
33]. This finding reinforces the notion that fatigue negatively impacts biomechanical control, increasing the risk of DKV and subsequent lower limb injuries [
20,
21,
33].
Additionally, the strong correlations between LLMP and DKV underscore the importance of explosive strength in maintaining proper knee alignment. Given that basketball involves plenty of jumps, landings, and rapid directional changes, athletes with insufficient lower limb power may exhibit compromised knee mechanics, predisposing them to injuries such as anterior cruciate ligament (ACL) tears and patellofemoral pain syndrome [
21,
31,
35,
50]. Implementing plyometric and resistance training exercises that focus on the hip, knee, and ankle stabilization may mitigate these risks and enhance overall athletic performance [
30,
34,
35,
51].
A notable finding is the significant gender difference in VO
2max and power, suggesting potential sex-based variations in neuromuscular endurance and knee stability. While no other anthropometric variables differed significantly between genders, the discrepancy in cardiorespiratory fitness levels indicates a potential disparity in endurance-based neuromuscular control, which could influence knee biomechanics [
20]. Future research should explore gender-specific intervention strategies to address these differences and further refine sex-specific injury prevention programs.
While the literature provides strong evidence supporting the role of LLMP and CRF in mitigating DKV, further research is needed to determine how training programs should be adapted for individuals with varying physical fitness levels [
23,
24]. Adolescent athletes with lower baseline LLMP or CRF may require progressive training strategies that emphasize gradual power and endurance development, while more advanced adolescents might benefit from sport-specific training. Additionally, factors such as age, sex, and training experience should be considered when designing interventions to ensure effectiveness and injury prevention.
Although the results of this study agree with many others in the current literature, a correlation between variables does not automatically mean causation [
16,
25]. Causation indicates that one event is the result of the occurrence of the other event, i.e., there is a causal relationship between the two events. The literature indicates that DKV, like most sports injuries, is complex and multifactorial, and it results not from the linear combination of isolated and predictive factors, but from the interaction among them [
16]. In this sense, we need a broader approach to better understand the complex relationships between risk factors/predictors and injuries. Unmeasured factors such as prior injuries, training load, or limb dominance could influence the results and bring new insights to improve even more injury-prevention programs.
In conclusion, the results of this study emphasize the critical role of LLMP and CRF in controlling DKV. Injury-prevention programs that target lower limb power and cardiorespiratory fitness may not only reduce the risk of knee injuries but also improve overall athletic performance. Future studies should consider longitudinal analyses to assess how targeted training interventions influence knee valgus over time and whether individualized training regimens can yield optimal results for injury prevention in adolescent basketball players.
5. Study Limitations
The heterogeneity between the sexes was the primary limitation of this study, since there were almost twice as many boys as girls, which could affect the generalization of the study results.
While validated equations were employed to estimate these parameters, indirect assessments introduce potential inaccuracies that may affect the precision of the findings. Direct measurement methods, such as force plate analysis for LLMP or gas exchange analysis for CRF, would provide more accurate and individualized data but are often impractical in field-based settings due to cost and accessibility constraints. The reliance on estimation models may introduce variability, particularly in diverse populations with different biomechanical and physiological characteristics.
Additionally, the choice of a 2D analysis to a 3D analysis may have prevented the thorough impact assessment of the testing structures and the real landing behavior.
6. Conclusions
This study highlights the strong association among LLMP, CRF, and DKV in adolescent basketball athletes.
The findings suggest that targeted LLMP and CRF training programs can play a crucial role in minimizing knee valgus and reducing the risk of related injuries. Given the strong predictive value of VO2max and LLMP for knee control, targeted training programs that focus on neuromuscular conditioning and aerobic capacity are likely to be effective for injury prevention.
Strength and conditioning coaches and physiotherapists can apply these findings by implementing targeted and accessible testing for their athletes to determine their fitness level and conduct individualized training programs for each athlete for improvement and injury prevention.
Future research should further explore individualized training approaches and assess their long-term effectiveness in improving knee mechanics and athletic performance.
Author Contributions
Conceptualization, A.S.; methodology, A.S. and G.P.; software, A.S.; validation, V.A., E.K. and G.P.; formal analysis, A.S.; writing—original draft preparation, A.S. and G.P.; writing—review and editing, V.A. and G.P.; supervision, G.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Prior to the study, the study protocol was approved by the Ethics Committee of the Department of Physiotherapy at the University of Thessaly (1083/21-10-2022). The study was performed following the principles in the Declaration of Helsinki; thus, it is consistent with the value of respect for the volunteers who would participate.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
All the data are saved in an external drive that belongs to A.S. and can be provided if needed.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DKV | Dynamic Knee Valgus |
| LLMP | Lower Limb Muscle Power |
| CRF | Cardiorespiratory Fitness |
| CMJ | Countermovement Jump |
| 20mSRT | 20 m Shuttle Run Test |
| SLDJ | Single Leg Drop Jump |
| 2D | Two Dimensional |
| FPPA | Frontal Plane Projection Angle |
References
- Buchanan, P.A.; Vardaxis, V.G. Lower-Extremity Strength Profiles and Gender-Based Classification of Basketball Players Ages 9–22 Years. J. Strength Cond. Res. 2009, 23, 406–419. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rosell, D.; Mora-Custodio, R.; Franco-Márquez, F.; Yáñez-García, J.M.; González-Badillo, J.J. Traditional vs. Sport-specific vertical jump tests: Reliability, validity, and relationship with the legs strength and sprint performance in adult and teen soccer and basketball players. J. Strength Cond. Res. 2017, 31, 196–206. [Google Scholar] [CrossRef]
- Krosshaug, T.; Nakamae, A.; Boden, B.P.; Engebretsen, L.; Smith, G.; Slauterbeck, J.R.; Hewett, T.E.; Bahr, R. Mechanisms of anterior cruciate ligament injury in basketball: Video analysis of 39 cases. Am. J. Sports Med. 2007, 35, 359–367. [Google Scholar] [CrossRef]
- Leppänen, M.; Pasanen, K.; Kujala, U.M.; Vasankari, T.; Kannus, P.; Äyrämö, S.; Krosshaug, T.; Bahr, R.; Avela, J.; Perttunen, J.; et al. Stiff Landings Are Associated with Increased ACL Injury Risk in Young Female Basketball and Floorball Players. Am. J. Sports Med. 2017, 45, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Zheng, Y. Knee Joint Injuries in Young Basketball Players. Rev. Bras. Med. Esporte 2022, 28, 763–766. [Google Scholar] [CrossRef]
- Foss, K.D.B.; Myer, G.D.; Magnussen, R.A.; Hewett, T.E. Diagnostic Differences for Anterior Knee Pain between Sexes in Adolescent Basketball Players. J. Athl. Enhanc. 2014, 3, 1814. [Google Scholar] [CrossRef] [PubMed]
- Stojanović, E.; Faude, O.; Scanlan, A.T.; Jakovljević, V.; Ćosić, M.; Kocić, M.; Radovanović, D. Injury incidence among adolescent and senior basketball players: A prospective study in 19 teams across an entire season. Phys. Sportsmed. 2024, 52, 386–394. [Google Scholar] [CrossRef]
- El Gharib, M.H.; El Tohamy, A.M.; Mohamed, N.E. Determining the relationship between the quadriceps and tibiofemoral angles among adolescents. J. Taibah Univ. Med. Sci. 2021, 16, 70–76. [Google Scholar] [CrossRef]
- Hewett, T.E.; Torg, J.S.; Boden, B.P. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: Lateral trunk and knee abduction motion are combined components of the injury mechanism. Br. J. Sports Med. 2009, 43, 417–422. [Google Scholar] [CrossRef]
- Parikh, S.N.; Shrivastava, R.K. Evaluation of Children with Injuries Around the Knee. Indian J. Pediatr. 2016, 83, 844–851. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Van den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Finch, C.F.; Kemp, J.L.; Clapperton, A.J. The incidence and burden of hospital-treated sports-related injury in people aged 15+ years in Victoria, Australia, 2004–2010: A future epidemic of osteoarthritis? Osteoarthr. Cartil. 2015, 23, 1138–1143. [Google Scholar] [CrossRef]
- Leppänen, M.; Pasanen, K.; Krosshaug, T.; Kannus, P.; Vasankari, T.; Kujala, U.M.; Bahr, R.; Perttunen, J.; Parkkari, J. Sagittal Plane Hip, Knee, and Ankle Biomechanics and the Risk of Anterior Cruciate Ligament Injury: A Prospective Study. Orthop. J. Sports Med. 2017, 5, 2325967117745487. [Google Scholar] [CrossRef]
- Whittaker, J.L.; Toomey, C.M.; Nettel-Aguirre, A.; Jaremko, J.L.; Doyle-Baker, P.K.; Woodhouse, L.J.; Emery, C.A. Health-related Outcomes after a Youth Sport-related Knee Injury. Med. Sci. Sports Exerc. 2019, 51, 255–263. [Google Scholar] [CrossRef]
- Serpell, B.G.; Scarvell, J.M.; Ball, N.B.; Smith, P.N. Mechanisms and Risk Factors for Noncontact ACL Injury in Age Mature Athletes Who Engage in Field or Court Sports: A Summary of the Literature Since 1980. J. Strength Cond. Res. 2012, 26, 3160–3176. [Google Scholar] [CrossRef]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition—Narrative review and new concept. Br. J. Sports Med. 2016, 50, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Stojiljkovic, A.; Karagianni, E.; Varsamo, A.; Batalik, L.; Pepera, G. Correlation of anthropometric characteristics and movement behavior with lower extremity muscle power and dynamic knee valgus in adolescent basketball athletes. J. Sports Med. Phys. Fit. 2024, 64, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Asaeda, M.; Nakamae, A.; Hirata, K.; Kono, Y.; Uenishi, H.; Adachi, N. Factors associated with dynamic knee valgus angle during single-leg forward landing in patients after anterior cruciate ligament reconstruction. Asia Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2020, 22, 56–61. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; Barber Foss, K.D.; Goodman, A.; Ceasar, A.; Rauh, M.J.; Divine, J.G.; Hewett, T.E. The incidence and potential pathomechanics of patellofemoral pain in female athletes. Clin. Biomech. 2010, 25, 700–707. [Google Scholar] [CrossRef]
- Santamaria, L.J.; Webster, K.E. The effect of fatigue on lower-limb biomechanics during single-limb landings: A systematic review. J. Orthop. Sports Phys. Ther. 2010, 40, 464–473. [Google Scholar] [CrossRef]
- Farley, J.B.; Barrett, L.M.; Keogh, J.W.L.; Woods, C.T.; Milne, N. The relationship between physical fitness attributes and sports injury in female, team ball sport players: A systematic review. Sports Med. Open 2020, 6, 45. [Google Scholar] [CrossRef]
- Toomey, C.M.; Whittaker, J.L.; Nettel-Aguirre, A.; Reimer, R.A.; Woodhouse, L.J.; Ghali, B.; Doyle-Baker, P.K.; Emery, C.A. Higher fat mass is associated witha history of knee injury in youth sport. J. Orthop. Sports Phys. Ther. 2017, 47, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Dallinga, J.M.; Benjaminse, A.; Lemmink, K.A.P.M. Which Screening Tools Can Predict Injury to the Lower Extremities in Team Sports? A Systematic Review. Sports Med. 2012, 42, 791–815. [Google Scholar] [CrossRef] [PubMed]
- Onate, J.A.; Everhart, J.S.; Clifton, D.R.; Best, T.M.; Borchers, J.R.; Chaudhari, A.M.W. Physical Exam Risk Factors for Lower Extremity Injury in High School Athletes: A Systematic Review. Clin. J. Sport Med. 2015, 26, 435–444. [Google Scholar] [CrossRef]
- Bahr, R. Why screening tests to predict injury do not work-and probably never will: A critical review. Br. J. Sports Med. 2016, 50, 776–780. [Google Scholar] [CrossRef]
- Corbin, C.; Pangrazi, R.P. Definitions: Health, Fitness, and Physical Activity. Clin. J. Sport Med. 2000, 26, 435–444. [Google Scholar]
- Pepera, G.; Hadjiandrea, S.; Iliadis, I.; Sandercock, G.R.H.; Batalik, L. Associations between cardiorespiratory fitness, fatness, hemodynamic characteristics, and sedentary behaviour in primary school-aged children. BMC Sports Sci. Med. Rehabil. 2022, 14, 16. [Google Scholar] [CrossRef]
- Muehlbauer, T.; Gollhofer, A.; Granacher, U. Associations Between Measures of Balance and Lower-Extremity Muscle Strength/Power in Healthy Individuals Across the Lifespan: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1671–1692. [Google Scholar] [CrossRef]
- Witvrouw, E.; Lysens, R.; Bellemans, J.; Cambier, D.; Vanderstraeten, G. Intrinsic Risk Factors for the Development of Anterior Knee Pain in an Athletic Population a Two-Year Prospective Study. Am. J. Sports Med. 2000, 28, 480–489. [Google Scholar] [CrossRef]
- Wilczyński, B.; Zorena, K.; Ślęzak, D. Dynamic knee valgus in single-leg movement tasks. Potentially modifiable factors and exercise training options. a literature review. Int. J. Env. Res. Public Health 2020, 17, 8208. [Google Scholar] [CrossRef]
- Dadfar, M.; Alipour, M.; Sheikhhoseini, R. Countermovement Jump Variables and Estimated Peak Power in Female Children with Dynamic Knee Valgus. In Proceedings of the International Society of Biomechanics in Sport Conference, Online, 3–6 September 2021; NMU Commons: Marquette, MI, USA, 2021. [Google Scholar]
- Karagianni, E.; Stojiljkovic, A.; Antoniou, V.; Batalik, L.; Pepera, G. Modelling the associations of cardiorespiratory fitness with the cardiometabolic profile and sedentary behavior in school-aged nonprofessional athletes. Gazz. Medica Ital.—Arch. Per Le Sci. Mediche, 2025; accepted. [Google Scholar]
- Bourne, M.N.; Webster, K.E.; Hewett, T.E. Is Fatigue a Risk Factor for Anterior Cruciate Ligament Rupture? Sports Med. 2019, 49, 1629–1635. [Google Scholar] [CrossRef]
- Mozafaripour, E.; Seidi, F.; Minoonejad, H.; Bayattork, M.; Khoshroo, F. The effectiveness of the comprehensive corrective exercise program on kinematics and strength of lower extremities in males with dynamic knee valgus: A parallel-group randomized wait-list controlled trial. BMC Musculoskelet. Disord. 2022, 23, 700. [Google Scholar] [CrossRef]
- Lopes, T.J.A.; Simic, M.; Myer, G.D.; Ford, K.R.; Hewett, T.E.; Pappas, E. The Effects of Injury Prevention Programs on the Biomechanics of Landing Tasks: A Systematic Review with Meta-analysis. Am. J. Sports Med. 2018, 46, 1492–1499. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, G.R.; Lang, J.J.; Blanchard, J.; Léger, L.A.; Tremblay, M.S. The 20-m shuttle run: Assessment and interpretation of data in relation to youth aerobic fitness and health. Pediatr. Exerc. Sci. 2019, 31, 152–163. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Papers Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [PubMed]
- Barlow, S.E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120, S164–S192. [Google Scholar] [CrossRef]
- Pueo, B.; Penichet-Tomas, A.; Jimenez-Olmedo, J.M. Validity, reliability and usefulness of smartphone and kinovea motion analysis software for direct measurement of vertical jump height. Physiol. Behav. 2020, 227, 113144. [Google Scholar] [CrossRef]
- Puig-Diví, A.; Escalona-Marfil, C.; Padullés-Riu, J.M.; Busquets, A.; Padullés-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef]
- Schurr, S.; Marshall, A.; Resch, J.; Saliba, S. Two-Dimensional Video Analysis is Comparable To 3D Motion Capture in Lower Extremity Movement Assessment. Int. J. Sports Phys. Ther. 2017, 12, 163. [Google Scholar]
- Steffen, K.; Kroken, T.; Krosshaug, T. Comparisons of 3D- and 2D-Measurement Techniques and Observational Real-Time Assessment of Frontal Plane Knee Control in a Vertical Drop Jump Landing. Br. J. Sports Med. 2014, 48, 662–663. [Google Scholar] [CrossRef]
- Dingenen, B.; Malfait, B.; Nijs, S.; Peers, K.H.E.; Vereecken, S.; Verschueren, S.M.P.; Staes, F.F. Can two-dimensional video analysis during single-leg drop vertical jumps help identify non-contact knee injury risk? A one-year prospectice study. Clin. Biomech. 2015, 30, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.Y.S.; Plowman, S.A.; Looney, M.A. The reliability and validity of the 20-meter shuttle test in american students 12 to 15 years old. Res. Q. Exerc. Sport 1992, 63, 360–365. [Google Scholar] [CrossRef]
- Kolimechkov, S.; Petrov, L.; Alexandrova, A.; Cholakov, K. BeepShuttle Junior: Software for the Administration of the 20m Shuttle Run Test in Children and Adolescents. J. Adv. Sport Technol. 2018, 2, 35–40. [Google Scholar]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Dingenen, B.; Malfait, B.; Vanrenterghem, J.; Robinson, M.A.; Verschueren, S.M.P.; Staes, F.F. Can two-dimensional measured peak sagittal plane excursions during drop vertical jumps help identify three-dimensional measured joint moments? Knee 2015, 22, 73–79. [Google Scholar] [CrossRef]
- Mahar, M.T.; Welk, G.J.; Janz, K.F.; Laurson, K.; Zhu, W.; Baptista, F. Estimation of Lower Body Muscle Power from Vertical Jump in Youth. Meas. Phys. Educ. Exerc. Sci. 2022, 26, 324–334. [Google Scholar] [CrossRef]
- Ryman Augustsson, S.; Gustafsson, T.; Ageberg, E. Can tests of physical fitness predict traumatic knee injury in youth female athletes? A prospective cohort study. Phys. Ther. Sport 2024, 69, 15–21. [Google Scholar] [CrossRef]
- Dadfar, M.; Soltani, M.; Novinzad, M.B.; Raahemifar, K. Lower extremity energy absorption strategies at different phases during single and double-leg landings with knee valgus in pubertal female athletes. Sci. Rep. 2021, 11, 17516. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).








{kind=link}
{kind=link}
{kind=link}
{kind=link}