
An Objective and Subjective Evaluation of Masticatory Efficiency in Periodontal Patients Before and After Basic Periodontal Therapy: A Case Series Study

 and
and
Abstract
1. Introduction
2. Material and Methods
2.1. Clinical Sample
2.2. Ethical Considerations
- (a)
- Patients over 18 years old.
- (b)
- Diagnosed with periodontitis stage II or III, grade B [18].
- (c)
- Signed informed consent.
- (d)
- At least 20 teeth with antagonists.
- (e)
- Completion of basic periodontal treatment, attending a follow-up visit one month after the last scaling and root planing.
- (f)
- Patients had to understand and properly complete the Quality of Masticatory Function Questionnaire (QMFQ).
- (a)
- Pregnancy or lactation.
- (b)
- Systemic diseases affecting immune response.
- (c)
- Periodontal treatment in the last 12 months.
- (d)
- History of neoplasm or maxillofacial radiotherapy in the past 5 years.
- (e)
- Patients without periodontitis or with periodontitis stage I or IV, or grade A or C.
- (f)
- Smoking.
- (g)
- Use of removable prostheses.
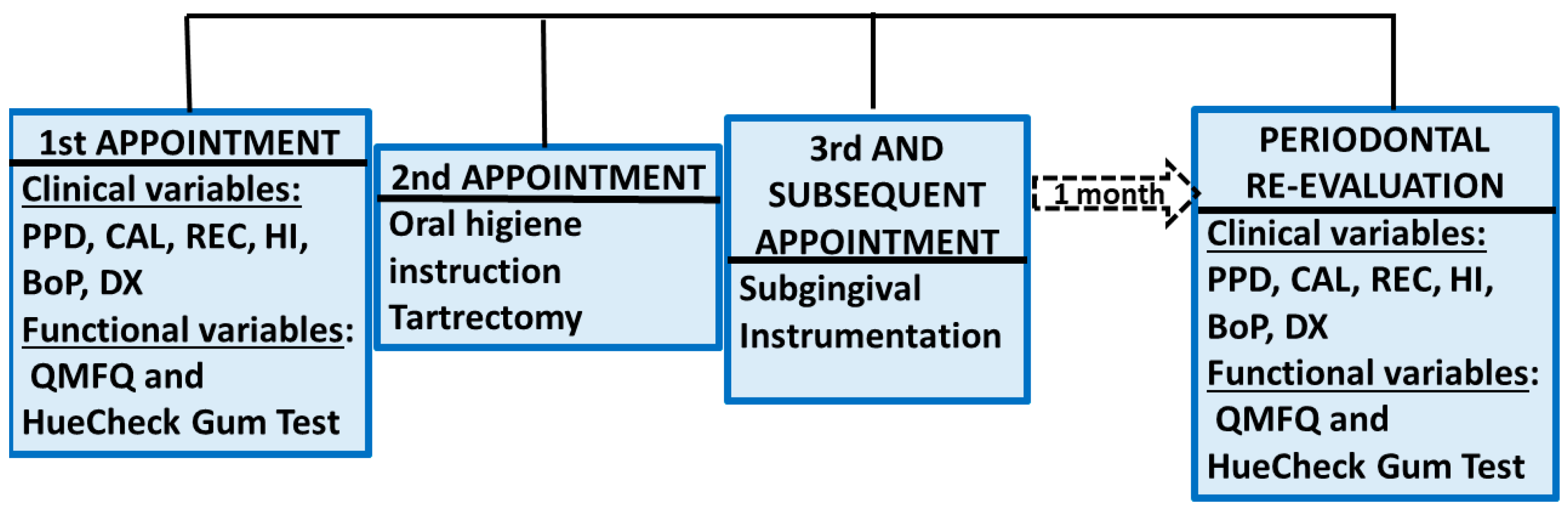
2.3. Clinical Method
2.4. Statistical Analysis
- “N” (Initial Sample Size): Based on the sample size from the Halazonetis study [23].
- Measured Variable: The hue value obtained from the HueCheck Gum test.
- Precision (d): A margin of 0.15 points for accuracy.
- Significance Level (α): 0.05 (95% confidence level).
- Power (1 − β): 90% (10% probability of type II error).
3. Results
3.1. Comparison of the Sample Before and After Periodontal Treatment
3.2. The Behaviour of the Variables “Gender”, “Facial Pattern”, and “Parafunction” in the Scores of the QMFQ and the HueCheck Gum Test
- (a)
- Gender:
- (b)
- Facial pattern:
- (c)
- Parafunction:
3.3. The Correlation Between the QMFQ and the HueCheck Gum Test
4. Discussion
4.1. Assessment Methods of Masticatory Function
4.2. Subjective Assessment with the QMFQ
4.3. Clinical Findings and Periodontal Outcomes
- HI decreased from 30.14% ± 32.71% to 13.10% ± 17.28%.
- Mean PD decreased from 2.46 ± 0.67 mm to 1.88 ± 0.53 mm.
- CAL improved from 3.26 ± 1.19 mm to 2.51 ± 0.74 mm.
4.4. Influence of Gender, Facial Pattern, and Parafunctional Habits
4.5. Limitations and Clinical Relevance
4.6. Future Research and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S.; et al. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89 (Suppl. S1), S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M.; Rams, T.E. Global epidemiology of periodontal diseases: An overview. Periodontol. 2000, 29, 7–10. [Google Scholar] [CrossRef]
- Johansson, A.S.; Svensson, K.G.; Trulsson, M. Impaired Masticatory Behavior in Subjects with Reduced Periodontal Tissue Support. J. Periodontol. 2006, 77, 1491–1497. [Google Scholar] [CrossRef]
- Borges, T.D.F.; Regalo, S.C.; Taba, M.; Siéssere, S.; Mestriner, W.; Semprini, M. Changes in Masticatory Performance and Quality of Life in Individuals with Chronic Periodontitis. J. Periodontol. 2013, 84, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Lamba, A.K.; Tandon, S.; Faraz, F.; Garg, V.; Aggarwal, K.; Gaba, V. Effect of periodontal disease on electromyographic activity of muscles of mastication: A cross-sectional study. J. Oral. Rehabil. 2020, 47, 599–605. [Google Scholar] [CrossRef]
- Palinkas, M.; Borges, T.d.F.; Junior, M.T.; Monteiro, S.A.C.; Bottacin, F.S.; Mestriner-Junior, W.; Regalo, I.H.; Siessere, S.; Semprini, M.; Regalo, S.C.H. Alterations in masticatory cycle efficiency and bite force in individuals with periodontitis. Int. J. Health Sci. 2019, 13, 25–29. [Google Scholar]
- Tada, A.; Miura, H. Systematic review of the association of mastication with food and nutrient intake in the independent elderly. Arch. Gerontol. Geriatr. 2014, 59, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Kossioni, A.E. The Association of Poor Oral Health Parameters with Malnutrition in Older Adults: A Review Considering the Potential Implications for Cognitive Impairment. Nutrients 2018, 10, 1709. [Google Scholar] [CrossRef]
- Schott Börger, S.; Ocaranza Tapia, D.; Peric Cáceres, K.; Yévenes López, I.; Romo Ormazábal, F.; Schulz Rosales, R.; Torres-Quintana, M.A. Métodos de Evaluación del Rendimiento Masticatorio. Una Revisión. Rev. Clínica Periodoncia Implantol. Rehabil. Oral. 2010, 3, 51–55. [Google Scholar]
- Palomares, T.; Montero, J.; Rosel, E.M.; Del-Castillo, R.; Rosales, J.I. Oral health-related quality of life and masticatory function after conventional prosthetic treatment: A cohort follow-up study. J. Prosthet. Dent. 2018, 119, 755–763. [Google Scholar] [CrossRef]
- Foster Page, L.A.; Thomson, W.M.; Jokovic, A.; Locker, D. Validation of the Child Perceptions Questionnaire (CPQ 11–14). J. Prosthet. Dent. 2005, 84, 649–652. [Google Scholar]
- Hildebrandt, G.H.; Dominguez, B.L.; Schork, M.A.; Loesche, W.J. Functional units, chewing, swallowing, and food avoidance among the elderly. J. Prosthet. Dent. 1997, 77, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Hatch, J.P.; Shinkai, R.S.; Sakai, S.; Rugh, J.D.; Paunovich, E.D. Determinants of masticatory performance in dentate adults. Arch. Oral Biol. 2001, 46, 641–648. [Google Scholar] [CrossRef]
- Owens, S.; Buschang, P.H.; Throckmorton, G.S.; Palmer, L.; English, J. Masticatory performance and areas of occlusal contact and near contact in subjects with normal occlusion and malocclusion. Am. J. Orthod. Dentofacial Orthop. 2002, 121, 602–609. [Google Scholar] [CrossRef]
- Barbosa, T.S.; Tureli, M.C.M.; Gavião, M.B.D. Validity and reliability of the Child Perceptions Questionnaires applied in Brazilian children. BMC Oral Health 2009, 9, 13. [Google Scholar] [CrossRef]
- Herrera, D.; Sanz, M.; Kebschull, M.; Jepsen, S.; Sculean, A.; Berglundh, T.; Papapanou, P.N.; Chapple, I.; Tonetti, M.S.; Consultant, E.W.P.A.M. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 4–60. [Google Scholar]
- Moya-Villaescusa, M.J.; Sánchez-Pérez, A.; Esparza-Marín, J.; Jornet-García, A.; Montoya-Carralero, J.M. Periodontal Disease and Nonsurgical Periodontal Therapy on the OHRQoL of the Patient: A Pilot Study of Case Series. Dent. J. 2023, 11, 94. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S173–S182. [Google Scholar]
- Herrera, D.; Berglundh, T.; Schwarz, F.; Chapple, I.; Jepsen, S.; Sculean, A.; Kebschull, M.; Papapanou, P.N.; Tonetti, M.S.; Sanz, M.; et al. Prevention and treatment of peri-implant diseases—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2023, 50, 4–76. [Google Scholar] [CrossRef]
- Hilasaca-Mamani, M.; Barbosa, T.D.S.; Fegadolli, C.; Castelo, P.M. Validity and reliability of the quality of masticatory function questionnaire applied in Brazilian adolescents. CoDAS 2016, 28, 149–154. [Google Scholar] [CrossRef]
- Buser, R.; Ziltener, V.; Samietz, S.; Fontolliet, M.; Nef, T.; Schimmel, M. Validation of a purpose-built chewing gum and smartphone application to evaluate chewing efficiency. J. Oral. Rehabil. 2018, 45, 845–853. [Google Scholar] [CrossRef]
- Schimmel, M.; Christou, P.; Herrmann, F.; Müller, F. A two-colour chewing gum test for masticatory efficiency: Development of different assessment methods. J. Oral. Rehabil. 2007, 34, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Halazonetis, D.J.; Schimmel, M.; Antonarakis, G.S.; Christou, P. Novel software for quantitative evaluation and graphical representation of masticatory efficiency. J. Oral. 2013, 40, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, T.; Ono, T.; Yoshimuta, Y.; Kida, M.; Kikui, M.; Nokubi, T.; Maeda, Y.; Kokubo, Y.; Watanabe, M.; Miyamoto, Y. The effect of periodontal status and occlusal support on masticatory performance: The S uita study. J. Clin. Periodontol. 2014, 41, 497–503. [Google Scholar] [CrossRef]
- Van Der Bilt, A.; Van Der Glas, H.W.; Mowlana, F.; Heath, M.R. A comparison between sieving and optical scanning for the determination of particle size distributions obtained by mastication in man. Arch. Oral Biol. 1993, 38, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Schimmel, M.; Christou, P.; Miyazaki, H.; Halazonetis, D.; Herrmann, F.R.; Müller, F. A novel colourimetric technique to assess chewing function using two-coloured specimens: Validation and application. J. Dent. 2015, 43, 955–964. [Google Scholar] [CrossRef]
- Barbe, A.G.; Javadian, S.; Rott, T.; Scharfenberg, I.; Deutscher, H.C.D.; Noack, M.J.; Derman, S.H.M. Objective masticatory efficiency and subjective quality of masticatory function among patients with periodontal disease. J. Clin. Periodontol. 2020, 47, 1344–1353. [Google Scholar] [CrossRef]
- Silva, L.C.; Nogueira, T.E.; Rios, L.F.; Schimmel, M.; Leles, C.R. Reliability of a two-colour chewing gum test to assess masticatory performance in complete denture wearers. J. Oral Rehabil. 2018, 45, 301–307. [Google Scholar] [CrossRef]
- Kapur, K.K.; Soman, S.D. Masticatory performance and efficiency in denture wearers. 1964. J. Prosthet. Dent. 2006, 95, 407–411. [Google Scholar] [CrossRef]
- Mowlana, F.; Heath, M.R.; Van der Bilt, A.; Van der Glas, H.W. Assessment of chewing efficiency: A comparison of particle size distribution determined using optical scanning and sieving of almonds. J. Oral Rehabil. 1994, 21, 545–551. [Google Scholar] [CrossRef]
- Abe, R.; Furuya, J.; Suzuki, T. Videoendoscopic measurement of food bolus formation for quantitative evaluation of masticatory function. J. Prosthodont. Res. 2011, 55, 171–178. [Google Scholar] [CrossRef]
- Muller, K. The Mandibular Implant Overdenture Versus the Mandibular Conventional Denture: Impact on the Nutritional Status. Ph.D. Thesis, Faculty of Dentistry, McGill University, Montreal, QC, Canada, 1999. [Google Scholar]
- Muller, K.; Morais, J.; Feine, J. Nutritional and anthropometric analysis of edentulous patients wearing implant overdentures or conventional dentures. Braz. Dent. J. 2008, 19, 145–150. [Google Scholar] [CrossRef]
- Nagarajappa, R.; Batra, M.; Sanadhya, S.; Daryani, H.; Ramesh, G. Oral impacts on daily performance: Validity, reliability and prevalence estimates among Indian adolescents. Int. J. Dent. Hyg. 2018, 16, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, C.; Henrikson, T.; Bondemark, L.; Ekberg, E. Masticatory function in patients with dentofacial deformities before and after orthognathic treatment-a prospective, longitudinal, and controlled study. Eur. J. Orthod. 2015, 37, 67–72. [Google Scholar] [CrossRef]
- Pero, A.C.; Scavassin, P.M.; Policastro, V.B.; Júnior, N.M.d.O.; Marin, D.O.M.; da Silva, M.D.D.; Cassiano, A.F.B.; Santana, T.d.S.; Compagnoni, M.A. Masticatory function in complete denture wearers varying degree of mandibular bone resorption and occlusion concept: Canine-guided occlusion versus bilateral balanced occlusion in a cross-over trial. J. Prosthodont. Res. 2019, 63, 421–427. [Google Scholar] [CrossRef]
- Murakami, S.; Mealey, B.L.; Mariotti, A.; Chapple, I.L.C. Dental plaque-induced gingival conditions. J. Periodontol. 2018, 89 (Suppl. S1), S17–S27. [Google Scholar] [PubMed]
- Díaz, B.F.; Pomarino, S.G. Reevaluación del paciente periodontal: Intervalo de tiempo adecuado para reevaluar sus parámetros. Acta Odontológica Colomb 2017, 7, 65–71. [Google Scholar]
- Pereira, L.J.; Gazolla, C.M.; Magalhães, I.B.; Dominguete, M.H.L.; Vilela, G.R.; Castelo, P.M.; Marques, L.S.; Van Der Bilt, A. Influence of periodontal treatment on objective measurement of masticatory performance. J. Oral Sci. 2012, 54, 151–157. [Google Scholar] [CrossRef]
- Ingervall, B.; Bitsanis, E. A pilot study of the effect of masticatory muscle training on facial growth in long-face children. Eur. J. Orthod. 1987, 9, 15–23. [Google Scholar] [CrossRef]
- Gomes, S.G.F.; Custodio, W.; Faot, F.; Del Bel Cury, A.A.; Garcia, R.C.M.R. Masticatory features, EMG activity and muscle effort of subjects with different facial patterns. J. Oral Rehabil. 2010, 37, 813–819. [Google Scholar] [CrossRef]
- Paulino, M.R.; Moreira, V.G.; Lemos, G.A.; Silva PLPda Bonan, P.R.F.; Batista, A.U.D. Prevalence of signs and symptoms of temporomandibular disorders in college preparatory students: Associations with emotional factors, parafunctional habits, and impact on quality of life. Cienc Saude Coletiva 2018, 23, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Sterenborg, B.A.M.M.; Kalaykova, S.I.; Loomans, B.A.C.; Huysmans, M.C.D.N.J.M. Impact of tooth wear on masticatory performance. J. Dent. 2018, 76, 98–101. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| FEEDING–CHEWING | Never | Hardy Ever | Occasionally | Fairly Often | Very Often | N/A |
|---|---|---|---|---|---|---|
| ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| HABITS | ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| MEATS | ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| FRUIT | ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| ||||||
| VEGETABLES | ||||||
| ||||||
| ||||||
|
| Variable | Initial (Mean ± SD) | Final (Mean ± SD) | Significance (p-Value) |
|---|---|---|---|
| HI | 30.15 ± 32.71 | 13.10 ± 17.27 | 0.0001 |
| PD | 2.46 ± 0.67 | 1.88 ± 0.53 | 0.0001 |
| CAL | 3.26 ± 1.19 | 2.50 ± 0.74 | 0.0001 |
| Total score QMFQ | 25.06 ± 18.43 | 22.62 ± 14.26 | 0.045 |
| HueCheck Gum Test | 0.59 ± 0.09 | 0.61 ± 0.11 | 0.667 |
| Variable | Men (Mean ± SD) | Women (Mean ± SD) | Significance (p-Value) |
|---|---|---|---|
| Total score QMFQ pre-treatment | 27 ± 20.7 | 23.55 ± 16.92 | 0.46 |
| Total score QMFQ post-treatment | 24.92 ± 16.39 | 20.83 ± 12.54 | 0.42 |
| HueCheck Gum test pre-treatment | 0.63 ± 0.42 | 0.55 ± 0.16 | 0.64 |
| HueCheck Gum test post-treatment | 0.59 ± 0.16 | 0.61 ± 0.02 | 0.72 |
| Dependent Variable | (I) Facial Pattern | (J) Facial Pattern | Mean Difference (I-J) | Standard Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| FRUIT | Dolichofacial | Mesofacial | 4 | 1.91 | 0.129 | −0.781 | 8.781 |
| Brachyfacial | 4.92 | 1.94 | 0.047 | 0.053 | 9.782 | ||
| Dependent Variable | (I) Facial Pattern | (J) Facial Pattern | Mean Difference (I-J) | Standard Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| MEATS | Dolichofacial | Mesofacial | 6.66 | 2.63 | 0.051 | −0.015 | 13.349 |
| Brachyfacial | 7.00 | 2.67 | 0.042 | 0.211 | 13.789 | ||
| FRUITS | Dolichofacial | Mesofacial | 6.48 | 1.94 | 0.007 | 1.539 | 11.428 |
| Brachyfacial | 5.13 | 1.98 | 0.044 | 0.111 | 10.158 | ||
| ANOVA | ||||||
|---|---|---|---|---|---|---|
| Sum of Squares | df | Mean Square | F | Sig. | ||
| Vegetables | Between Groups | 12.72 | 1 | 12.72 | 4.32 | 0.046 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moya-Villaescusa, M.J.; López-Lisón, C.; Montoya-Carralero, J.M.; Jornet-García, A.; Sánchez-Pérez, A. An Objective and Subjective Evaluation of Masticatory Efficiency in Periodontal Patients Before and After Basic Periodontal Therapy: A Case Series Study. Appl. Sci. 2025, 15, 4258. https://doi.org/10.3390/app15084258
Moya-Villaescusa MJ, López-Lisón C, Montoya-Carralero JM, Jornet-García A, Sánchez-Pérez A. An Objective and Subjective Evaluation of Masticatory Efficiency in Periodontal Patients Before and After Basic Periodontal Therapy: A Case Series Study. Applied Sciences. 2025; 15(8):4258. https://doi.org/10.3390/app15084258
Chicago/Turabian StyleMoya-Villaescusa, María José, Claudia López-Lisón, José María Montoya-Carralero, Alfonso Jornet-García, and Arturo Sánchez-Pérez. 2025. "An Objective and Subjective Evaluation of Masticatory Efficiency in Periodontal Patients Before and After Basic Periodontal Therapy: A Case Series Study" Applied Sciences 15, no. 8: 4258. https://doi.org/10.3390/app15084258
APA StyleMoya-Villaescusa, M. J., López-Lisón, C., Montoya-Carralero, J. M., Jornet-García, A., & Sánchez-Pérez, A. (2025). An Objective and Subjective Evaluation of Masticatory Efficiency in Periodontal Patients Before and After Basic Periodontal Therapy: A Case Series Study. Applied Sciences, 15(8), 4258. https://doi.org/10.3390/app15084258