
Effect of Low-Frequency Magnetic Field Stimulation on Physical Performance and Inflammation in Post-Stroke Patients: A Feasibility and Safety Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Participants, Intervention, and Assesement
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALT | Alanine Aminotransferase |
| AST | Aspartate Aminotransferase |
| CREA | Creatinine |
| CRP | C-reactive Protein (High-sensitivity) |
| ELF-MFs | Extremely Low-Frequency Magnetic Fields Therapy |
| FIM | Functional Independence Measure |
| HCT | Hematocrit |
| HGB | Hemoglobin |
| K | Potassium |
| MCH | Mean Corpuscular Hemoglobin |
| MCHC | Mean Corpuscular Hemoglobin Concentration |
| MCV | Mean Corpuscular Volume |
| MPV | Mean Platelet Volume |
| MT1 | Group receiving magnetotherapy applied to the head |
| MT2 | Group receiving magnetotherapy applied to the pelvic area |
| NA | Sodium |
| PCT | Procalcitonin |
| PLT | Platelets |
| RBC | Red Blood Cells |
| RDW | Red Cell Distribution Width |
| rTMS | Repetitive Transcranial Magnetic Stimulation |
| SPPB | Short Physical Performance Battery |
| UREA | Urea |
| WBC | White Blood Cells |
References
- Coscia, M.; Wessel, M.J.; Chaudary, U.; Del Millán, J.R.; Micera, S.; Guggisberg, A.; Vuadens, P.; Donoghue, J.; Birbaumer, N.; Hummel, F.C. Neurotechnology-aided interventions for upper limb motor rehabilitation in severe chronic stroke. Brain 2019, 142, 2182–2197. [Google Scholar] [CrossRef] [PubMed]
- Wareńczak-Pawlicka, A.; Lisiński, P. Can We Target Close Therapeutic Goals in the Gait Re-Education Algorithm for Stroke Patients at the Beginning of the Rehabilitation Process? Sensors 2024, 24, 3416. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Yousufuddin, M.; Young, N. Aging and ischemic stroke. Aging 2019, 11, 2542–2544. [Google Scholar] [CrossRef]
- Nguyen, P.T.; Chou, L.-W.; Hsieh, Y.-L. Proprioceptive Neuromuscular Facilitation-Based Physical Therapy on the Improvement of Balance and Gait in Patients with Chronic Stroke: A Systematic Review and Meta-Analysis. Life 2022, 12, 882. [Google Scholar] [CrossRef]
- Pathak, A.; Gyanpuri, V.; Dev, P.; Dhiman, N.R. The Bobath Concept (NDT) as rehabilitation in stroke patients: A systematic review. J. Fam. Med. Prim. Care 2021, 10, 3983–3990. [Google Scholar] [CrossRef]
- Błażejewska-Hyżorek, B.; Czernuszenko, A.; Członkowska, A.; Ferens, A.; Gąsecki, D.; Kaczorowski, R.; Karaszewski, B.; Karliński, M.; Kaźmierski, R.; Kłysz, B.; et al. Wytyczne postępowania w udarze mózgu. Pol. Przegl. Neurol. 2019, 15, 1–156. [Google Scholar] [CrossRef]
- García-Pérez, P.; Del Rodríguez-Martínez, M.C.; Lara, J.P.; La Cruz-Cosme, C.d. Early Occupational Therapy Intervention in the Hospital Discharge after Stroke. Int. J. Environ. Res. Public Health 2021, 18, 12877. [Google Scholar] [CrossRef]
- Dąbrowski, J.; Czajka, A.; Zielińska-Turek, J.; Jaroszyński, J.; Furtak-Niczyporuk, M.; Mela, A.; Poniatowski, Ł.A.; Drop, B.; Dorobek, M.; Barcikowska-Kotowicz, M.; et al. Brain Functional Reserve in the Context of Neuroplasticity after Stroke. Neural Plast. 2019, 2019, 9708905. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, C.; Wu, X.; Nie, D.; Yu, H. Neuroplasticity of Acupuncture for Stroke: An Evidence-Based Review of MRI. Neural Plast. 2021, 2021, 2662585. [Google Scholar] [CrossRef]
- Aderinto, N.; AbdulBasit, M.O.; Olatunji, G.; Adejumo, T. Exploring the transformative influence of neuroplasticity on stroke rehabilitation: A narrative review of current evidence. Ann. Med. Surg. 2023, 85, 4425–4432. [Google Scholar] [CrossRef] [PubMed]
- Cichoń, N.; Czarny, P.; Bijak, M.; Miller, E.; Śliwiński, T.; Szemraj, J.; Saluk-Bijak, J. Benign Effect of Extremely Low-Frequency Electromagnetic Field on Brain Plasticity Assessed by Nitric Oxide Metabolism during Poststroke Rehabilitation. Oxid. Med. Cell. Longev. 2017, 2017, 2181942. [Google Scholar] [CrossRef] [PubMed]
- Marchewka, R.; Trzmiel, T.; Hojan, K. The Effect of Extremely Low-Frequency Magnetic Field on Stroke Patients: A Systematic Review. Brain Sci. 2024, 14, 430. [Google Scholar] [CrossRef]
- Fan, H.; Song, Y.; Cen, X.; Yu, P.; Bíró, I.; Gu, Y. The Effect of Repetitive Transcranial Magnetic Stimulation on Lower-Limb Motor Ability in Stroke Patients: A Systematic Review. Front. Hum. Neurosci. 2021, 15, 620573. [Google Scholar] [CrossRef]
- Di Lazzaro, V.; Capone, F.; Apollonio, F.; Borea, P.A.; Cadossi, R.; Fassina, L.; Grassi, C.; Liberti, M.; Paffi, A.; Parazzini, M.; et al. A consensus panel review of central nervous system effects of the exposure to low-intensity extremely low-frequency magnetic fields. Brain Stimul. 2013, 6, 469–476. [Google Scholar] [CrossRef]
- Capone, F.; Liberti, M.; Apollonio, F.; Camera, F.; Setti, S.; Cadossi, R.; Quattrocchi, C.C.; Di Lazzaro, V. An open-label, one-arm, dose-escalation study to evaluate safety and tolerability of extremely low frequency magnetic fields in acute ischemic stroke. Sci. Rep. 2017, 7, 12145. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. 2016, 2, 64. [Google Scholar] [CrossRef]
- Teresi, J.A.; Yu, X.; Stewart, A.L.; Hays, R.D. Guidelines for Designing and Evaluating Feasibility Pilot Studies. Med. Care 2022, 60, 95–103. [Google Scholar] [CrossRef]
- Cichon, N.; Synowiec, E.; Miller, E.; Sliwinski, T.; Ceremuga, M.; Saluk-Bijak, J.; Bijak, M. Effect of Rehabilitation with Extremely Low Frequency Electromagnetic Field on Molecular Mechanism of Apoptosis in Post-Stroke Patients. Brain Sci. 2020, 10, 266. [Google Scholar] [CrossRef]
- Cichon, N.; Saluk-Bijak, J.; Miller, E.; Sliwinski, T.; Synowiec, E.; Wigner, P.; Bijak, M. Evaluation of the effects of extremely low frequency electromagnetic field on the levels of some inflammatory cytokines in post-stroke patients. J. Rehabil. Med. 2019, 51, 854–860. [Google Scholar] [CrossRef]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the functional independence measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil. Stud. 1988, 10, 61–63. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, H.; Weatherall, M.; Taylor, W.; McPherson, K. Factors influencing rate of Barthel Index change in hospital following stroke. Clin. Rehabil. 2001, 15, 422–427. [Google Scholar] [CrossRef]
- Raîche, M.; Hébert, R.; Prince, F.; Corriveau, H. Screening older adults at risk of falling with the Tinetti balance scale. Lancet 2000, 356, 1001–1002. [Google Scholar] [CrossRef]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [CrossRef]
- Western, M.J.; Malkowski, O.S. Associations of the Short Physical Performance Battery (SPPB) with Adverse Health Outcomes in Older Adults: A 14-Year Follow-Up from the English Longitudinal Study of Ageing (ELSA). Int. J. Environ. Res. Public Health 2022, 19, 16319. [Google Scholar] [CrossRef]
- Bian, J.; Guo, S.; Huang, T.; Li, X.; Zhao, S.; Chu, Z.; Li, Z. CRP as a potential predictor of outcome in acute ischemic stroke. Biomed. Rep. 2023, 18, 17. [Google Scholar] [CrossRef]
- Lowe, N.K. What Is a Pilot Study? J. Obstet. Gynecol. Neonatal Nurs. 2019, 48, 117–118. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Parameter | Measure | Group | ||
|---|---|---|---|---|
| MT1 | MT2 | Control | ||
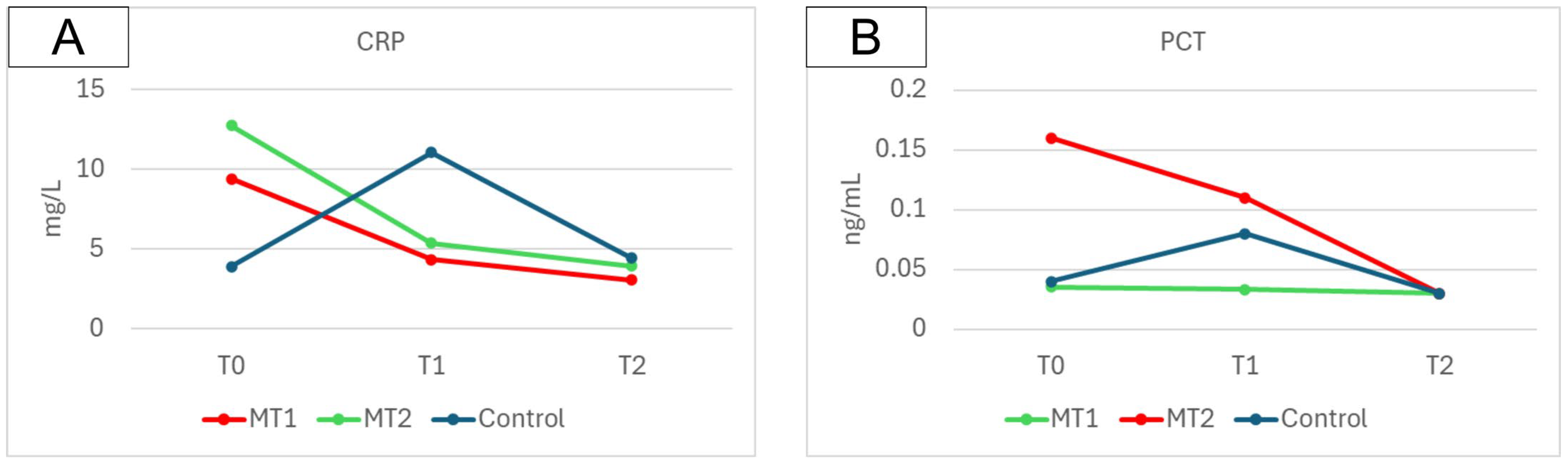
| CRP (mg/L) | T0 | 9.43 ± 8.48 | 12.75 ± 16.99 | 3.92 ± 4.54 |
| T1 | 4.36 ± 3.44 | 5.38 ± 5.75 | 11.06 ± 27.78 | |
| T2 | 3.07 ± 2.07 | 3.93 ± 3.69 | 4.45 ± 5.40 | |
| PCT (ng/mL) | T0 | 0.16 ± 0.48 | 0.04 ± 0.02 | 0.04 ± 0.03 |
| T1 | 0.11 ± 1.20 | 0.03 ± 0.02 | 0.08 ± 0.18 | |
| T2 | 0.03 ± 0.01 | 0.03 ± 0.01 | 0.03 ± 0.02 | |
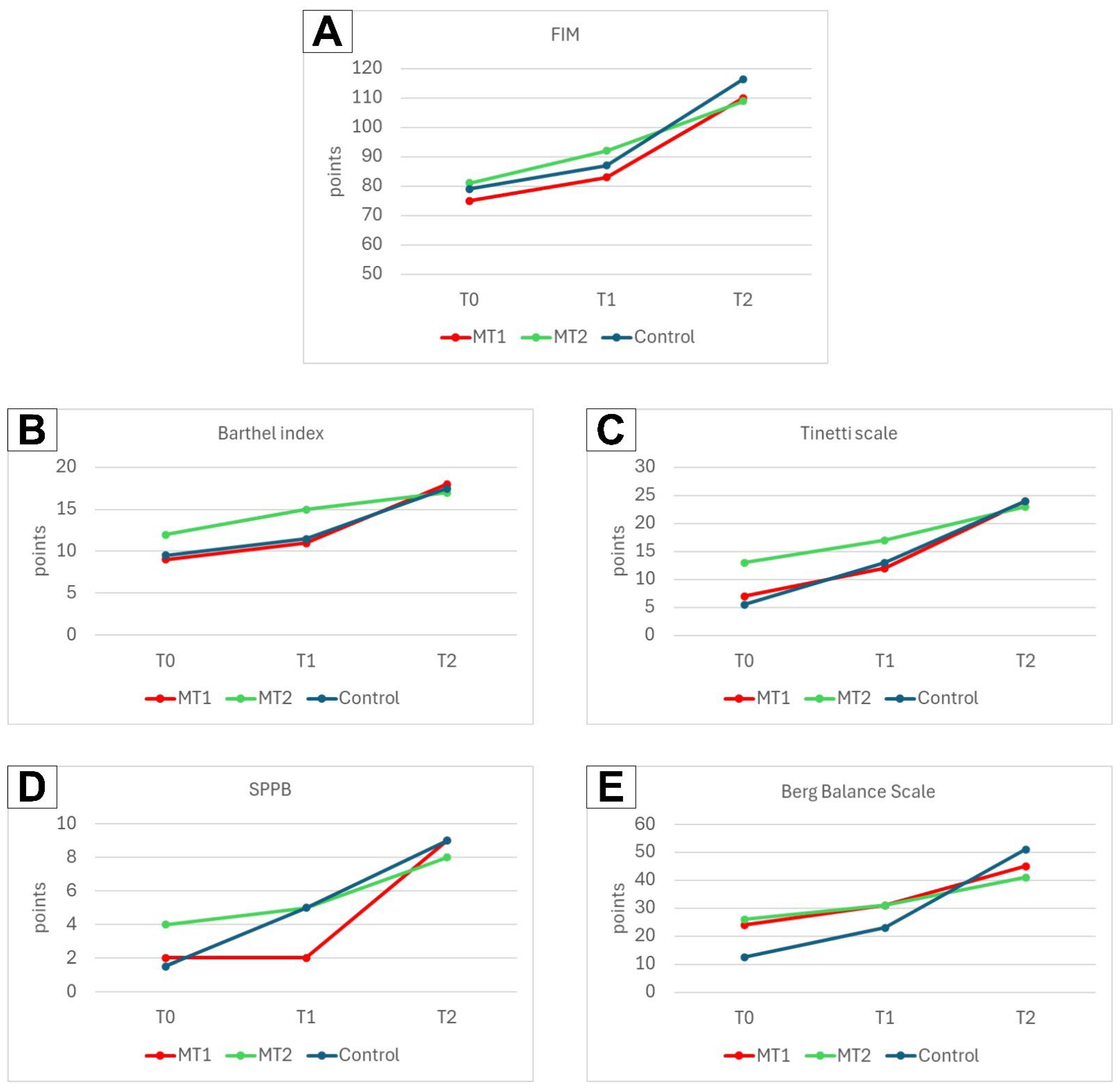
| FIM | T0 | 75 (4–98) | 81 (6–96) | 79 (4–110) |
| T1 | 83 (8–103) | 92 (10–104) | 87 (10–118) | |
| T2 | 110 (13–125) | 109 (29–125) | 116.5 (43–124) | |
| Barthel index | T0 | 9 (1–15) | 12 (2–15) | 9.5 (2–16) |
| T1 | 11 (4–18) | 15 (4–16) | 11.5 (3–19) | |
| T2 | 18 (4–20) | 17 (6–20) | 17.5 (6–20) | |
| Tinetti scale | T0 | 7 (0–21) | 13 (0–23) | 5.5 (0–25) |
| T1 | 12 (0–24) | 17 (1–25) | 13 (0–25) | |
| T2 | 24 (0–28) | 23 (5–28) | 24 (2–28) | |
| SPPB | T0 | 2 (0–11) | 4 (0–11) | 1.5 (0–9) |
| T1 | 2 (0–11) | 5 (0–12) | 5 (0–9) | |
| T2 | 9 (0–12) | 8 (1–12) | 9 (0–11) | |
| BBS | T0 | 24 (0–51) | 26 (0–43) | 12.5 (0–52) |
| T1 | 31 (4–49) | 31 (2–51) | 23 (3–54) | |
| T2 | 45 (11–56) | 41 (5–61) | 51 (6–61) | |
| Parameter | Measure | Group | ||
|---|---|---|---|---|
| MT1 | MT2 | Control | ||
| WBC (103/µL) | T0 | 8.00 ± 2.36 | 7.63 ± 2.33 | 8.26 ± 1.87 |
| T1 | 7.72 ± 3.75 | 6.79 ± 1.68 | 7.94 ± 2.25 | |
| T2 | 8.14 ± 4.98 | 6.48 ± 1.43 | 7.97 ± 1.80 | |
| RBC (106/µL) | T0 | 4.24 ± 0.41 | 4.18 ± 0.50 | 4.55 ± 0.40 |
| T1 | 4.13 ± 0.51 | 4.21 ± 0.65 | 4.51 ± 0.49 | |
| T2 | 4.16 ± 0.41 | 4.15 ± 0.45 | 4.55 ± 0.38 | |
| HGB (g/dL) | T0 | 13.49 ± 1.28 | 12.80 ± 1.31 | 13.71 ± 1.21 |
| T1 | 12.99 ± 1.59 | 12.85 ± 1.54 | 13.65 ± 1.43 | |
| T2 | 13.11 ± 1.30 | 12.85 ± 1.16 | 13.73 ± 1.18 | |
| HCT (%) | T0 | 38.90 ± 3.17 | 37.03 ± 3.50 | 40.49 ± 3.65 |
| T1 | 37.73 ± 4.34 | 37.23 ± 4.56 | 40.16 ± 4.00 | |
| T2 | 38.07 ± 3.34 | 36.97 ± 3.45 | 38.57 ± 7.74 | |
| MCV (fL) | T0 | 89.02 ± 12.21 | 89.55 ± 4.63 | 89.06 ± 4.10 |
| T1 | 91.86 ± 2.82 | 89.01 ± 4.19 | 88.86 ± 3.93 | |
| T2 | 91.40 ± 3.63 | 88.69 ± 3.49 | 85.71 ± 13.03 | |
| MCH (pg) | T0 | 31.63 ± 1.45 | 31.01 ± 2.23 | 30.32 ± 1.80 |
| T1 | 31.60 ± 1.31 | 30.82 ± 2.43 | 30.36 ± 1.85 | |
| T2 | 31.37 ± 1.43 | 30.91 ± 1.70 | 30.80 ± 2.88 | |
| MCHC (g/dL) | T0 | 34.52 ± 1.12 | 34.55 ± 1.65 | 34.06 ± 0.98 |
| T1 | 34.40 ± 0.99 | 34.56 ± 1.68 | 33.26 ± 2.64 | |
| T2 | 34.28 ± 1.23 | 34.69 ± 1.35 | 33.21 ± 2.50 | |
| RDW (%) | T0 | 13.50 ± 1.70 | 13.70 ± 1.59 | 13.21 ± 1.06 |
| T1 | 13.60 ± 1.65 | 13.77 ± 1.55 | 13.21 ± 0.74 | |
| T2 | 14.56 ± 4.85 | 13.76 ± 1.86 | 13.28 ± 0.77 | |
| PLT (103/µL) | T0 | 277.10 ± 147.34 | 256.87 ± 78.97 | 315.57 ± 81.42 |
| T1 | 267.90 ± 105.47 | 248.33 ± 80.48 | 279.36 ± 46.22 | |
| T2 | 253.80 ± 104.81 | 239.73 ± 80.05 | 291.71 ± 76.34 | |
| MPV (fL) | T0 | 10.90 ± 1.22 | 10.73 ± 0.64 | 10.31 ± 0.73 |
| T1 | 10.88 ± 1.08 | 10.51 ± 0.74 | 10.28 ± 0.88 | |
| T2 | 10.84 ± 1.08 | 10.50 ± 0.60 | 10.44 ± 0.92 | |
| CREA (mg/dL) | T0 | 1.00 ± 0.27 | 1.07 ± 0.38 | 0.93 ± 0.31 |
| T1 | 0.95 ± 0.23 | 1.11 ± 0.38 | 0.99 ± 0.30 | |
| T2 | 0.95 ± 0.22 | 1.11 ± 0.50 | 1.00 ± 0.22 | |
| UREA (mg/dL) | T0 | 32.84 ± 9.42 | 37.16 ± 15.54 | 47.12 ± 19.36 |
| T1 | 32.94 ± 12.24 | 44.08 ± 24.43 | 46.63 ± 21.20 | |
| T2 | 33.27 ± 11.70 | 40.31 ± 18.56 | 37.02 ± 19.43 | |
| ALT (U/L) | T0 | 27.87 ± 20.31 | 21.71 ± 4.28 | 52.56 ± 43.17 |
| T1 | 26.89 ± 11.33 | 22.24 ± 13.49 | 51.57 ± 53.68 | |
| T2 | 30.75 ± 12.73 | 21.16 ± 11.87 | 39.24 ± 21.89 | |
| AST (U/L) | T0 | 27.40 ± 12.96 | 21.73 ± 6.46 | 41.38 ± 26.62 |
| T1 | 27.09 ± 8.31 | 25.88 ± 8.63 | 42.21 ± 41.70 | |
| T2 | 27.61 ± 7.19 | 24.26 ± 10.08 | 32.04 ± 6.24 | |
| NA (mmol/L) | T0 | 140.85 ± 2.28 | 140.07 ± 2.74 | 138.21 ± 2.78 |
| T1 | 139.95 ± 3.25 | 140.60 ± 3.74 | 139.79 ± 3.07 | |
| T2 | 139.80 ± 2.04 | 140.20 ± 2.27 | 139.50 ± 3.11 | |
| K (mmol/L) | T0 | 3.95 ± 0.47 | 3.94 ± 0.35 | 4.24 ± 0.33 |
| T1 | 4.11 ± 0.36 | 4.16 ± 0.29 | 4.44 ± 0.60 | |
| T2 | 4.11 ± 0.42 | 4.13 ± 0.38 | 4.20 ± 0.37 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchewka, R.; Trzmiel, T.; Hojan, K. Effect of Low-Frequency Magnetic Field Stimulation on Physical Performance and Inflammation in Post-Stroke Patients: A Feasibility and Safety Study. Appl. Sci. 2025, 15, 3182. https://doi.org/10.3390/app15063182
Marchewka R, Trzmiel T, Hojan K. Effect of Low-Frequency Magnetic Field Stimulation on Physical Performance and Inflammation in Post-Stroke Patients: A Feasibility and Safety Study. Applied Sciences. 2025; 15(6):3182. https://doi.org/10.3390/app15063182
Chicago/Turabian StyleMarchewka, Renata, Tomasz Trzmiel, and Katarzyna Hojan. 2025. "Effect of Low-Frequency Magnetic Field Stimulation on Physical Performance and Inflammation in Post-Stroke Patients: A Feasibility and Safety Study" Applied Sciences 15, no. 6: 3182. https://doi.org/10.3390/app15063182
APA StyleMarchewka, R., Trzmiel, T., & Hojan, K. (2025). Effect of Low-Frequency Magnetic Field Stimulation on Physical Performance and Inflammation in Post-Stroke Patients: A Feasibility and Safety Study. Applied Sciences, 15(6), 3182. https://doi.org/10.3390/app15063182