
A Systematic Review Comparing Conservative and Surgical Approaches in the Management of Patellofemoral Instability

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Criteria
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction, Bias, and Outcomes
3. Results
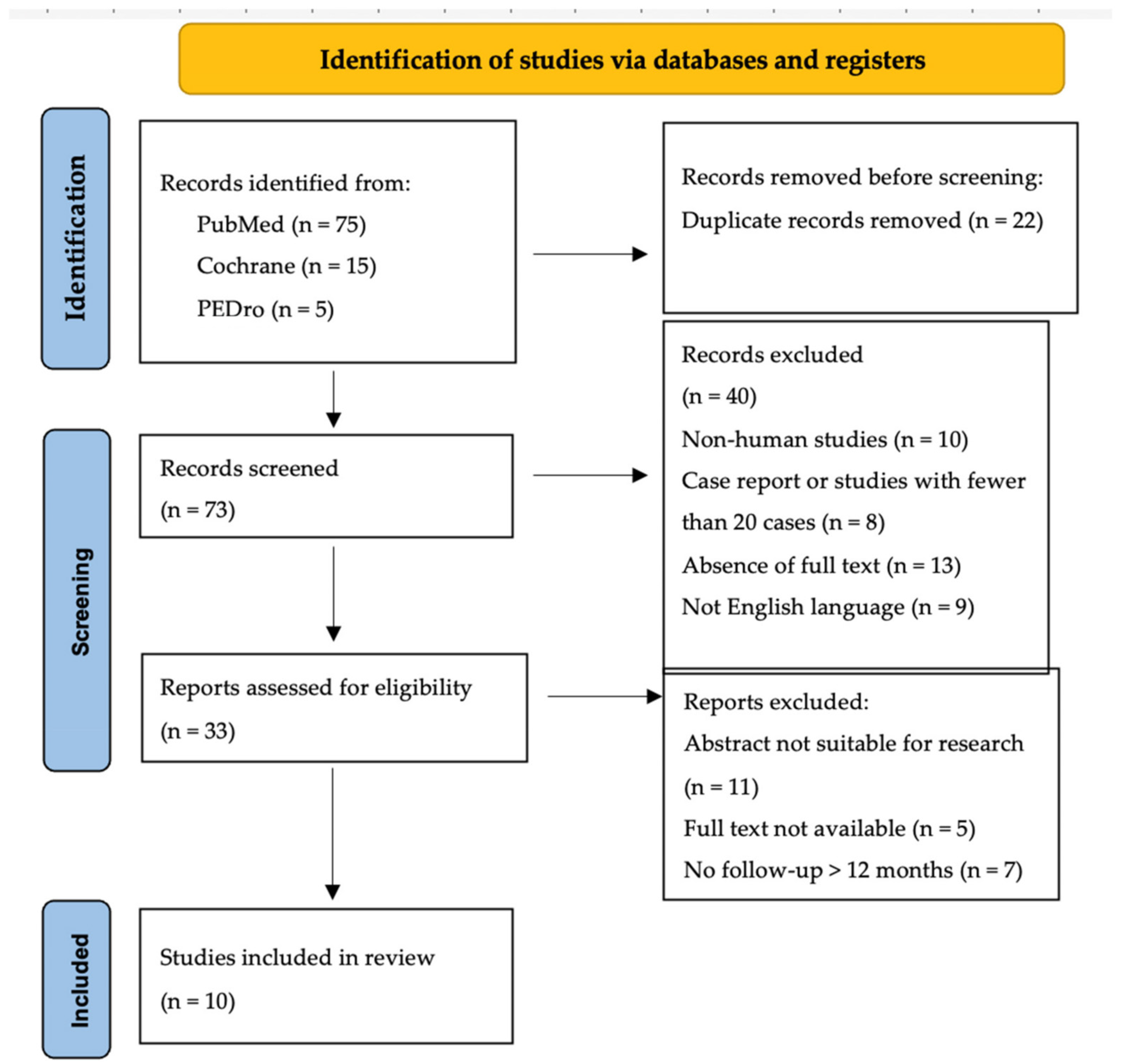
3.1. Eligible Studies
3.2. Demographics, Outcomes, and Success Rates
3.3. Success Rate
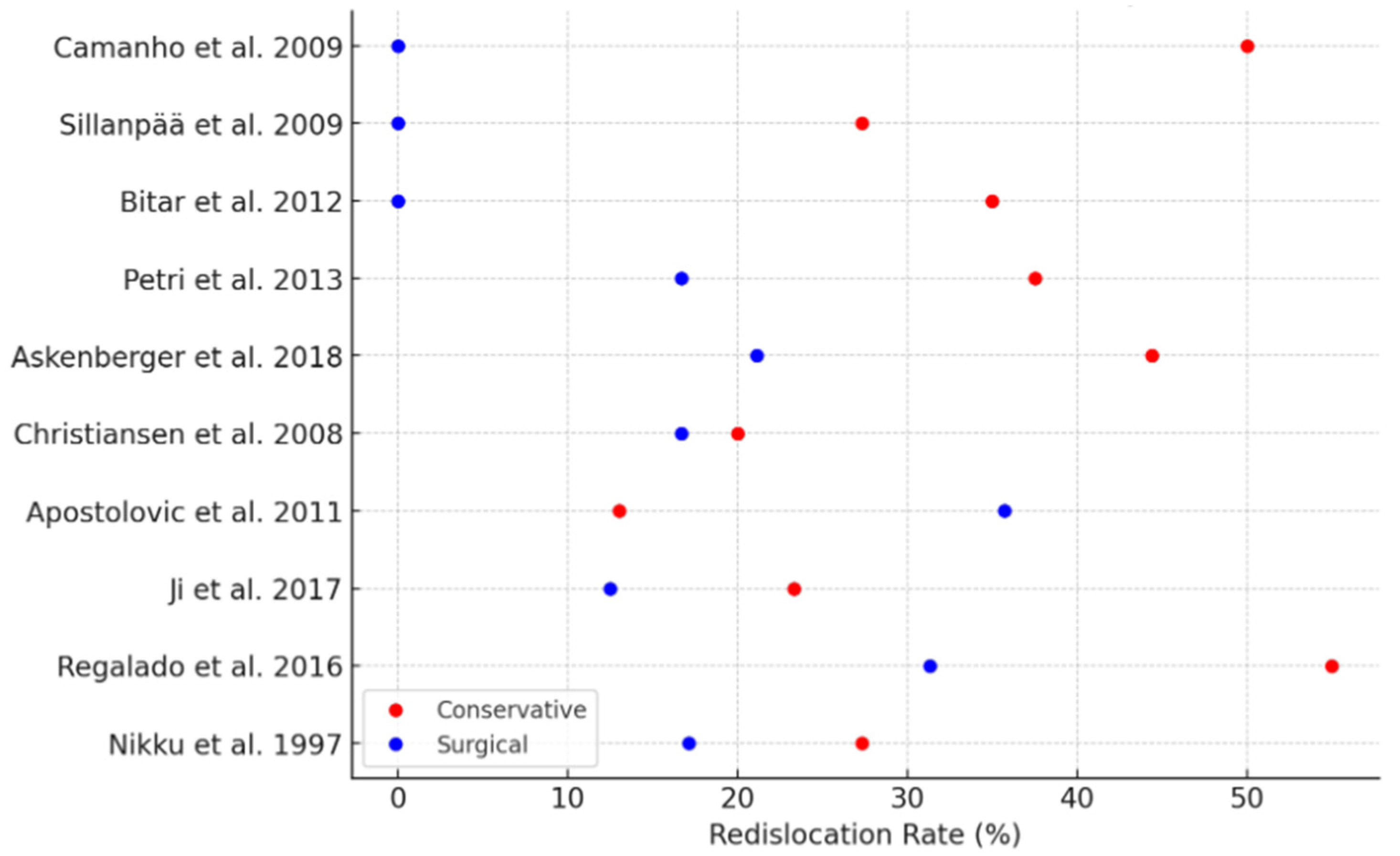
3.4. Re-Dislocation Rates
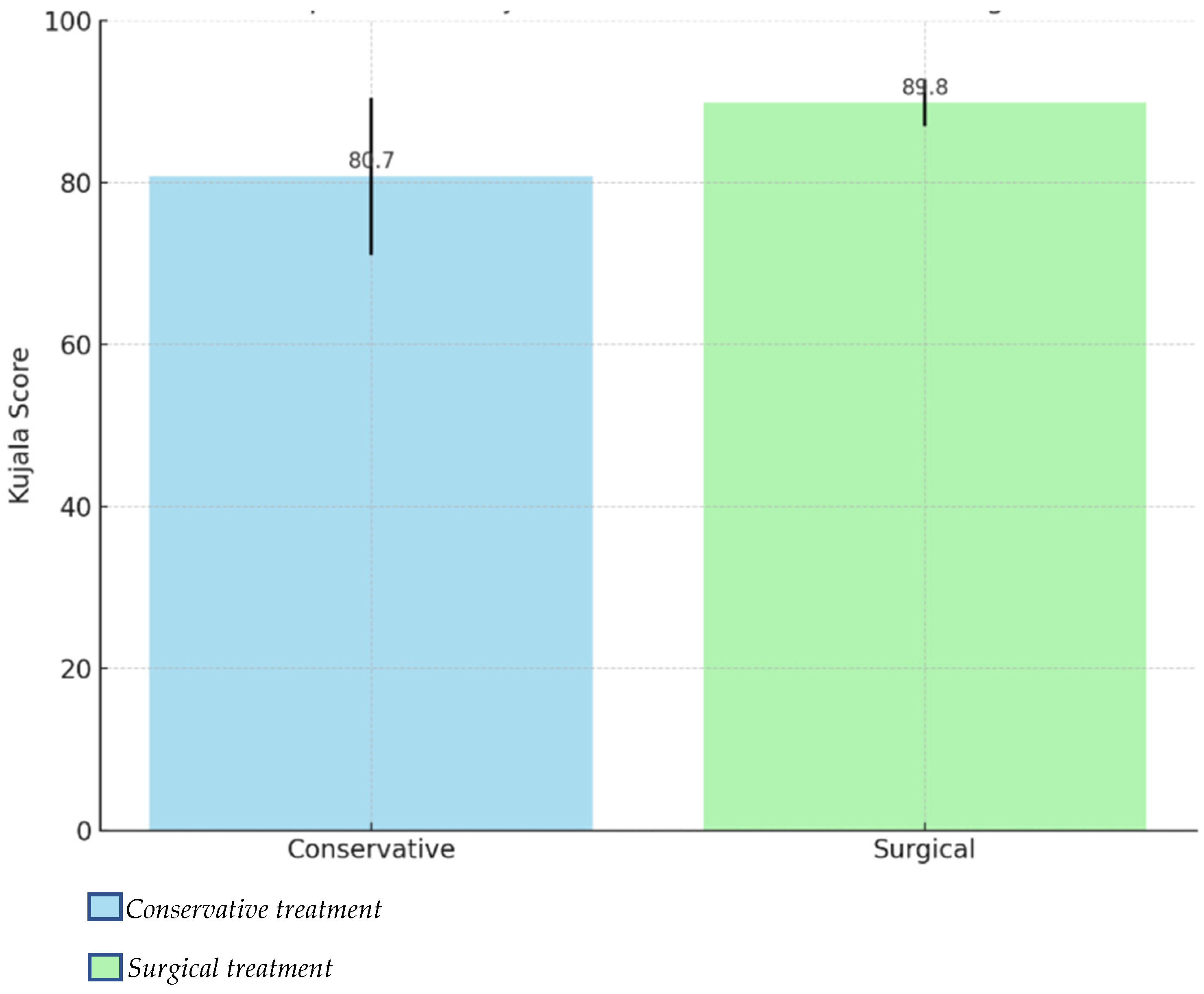
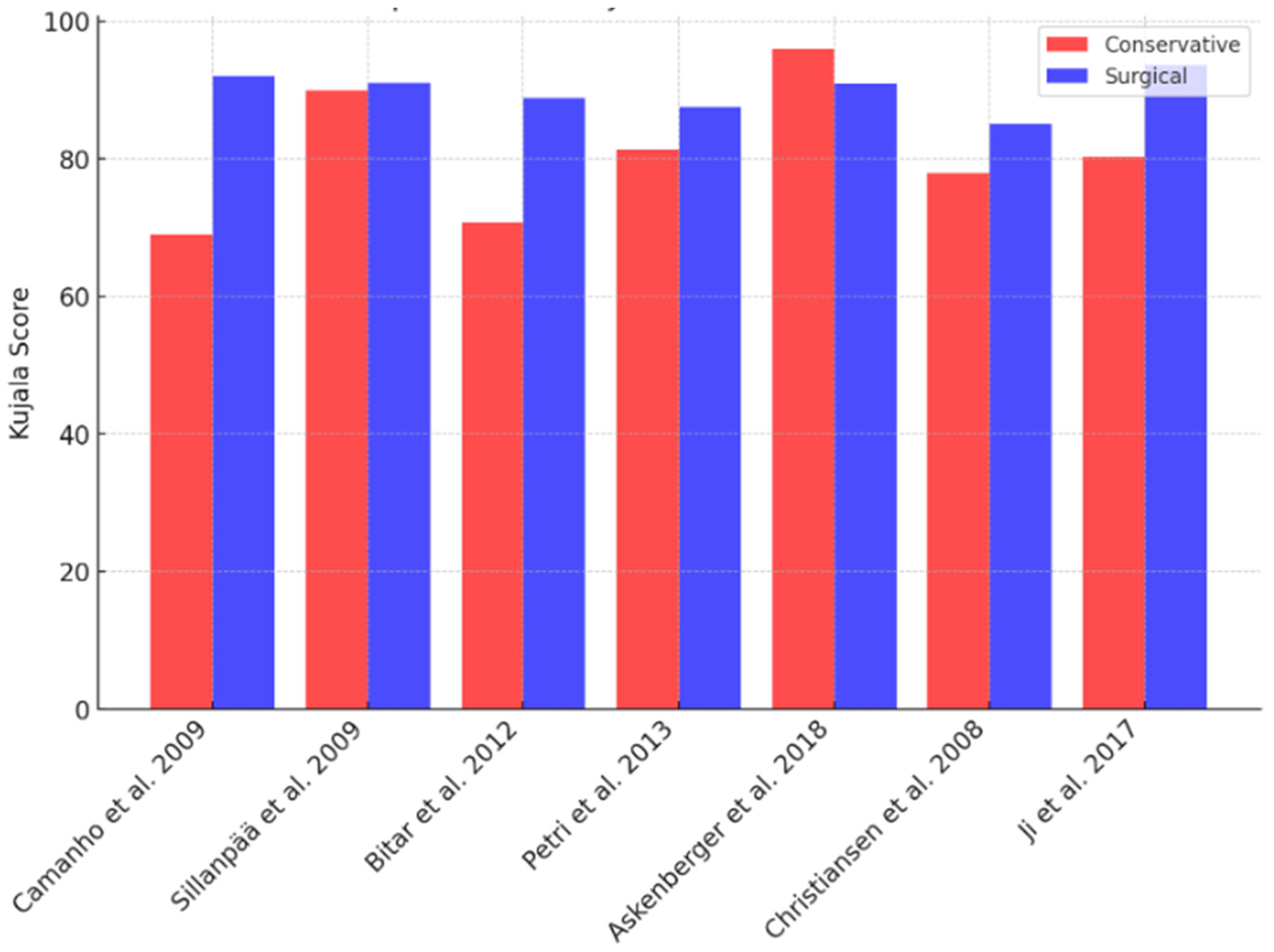
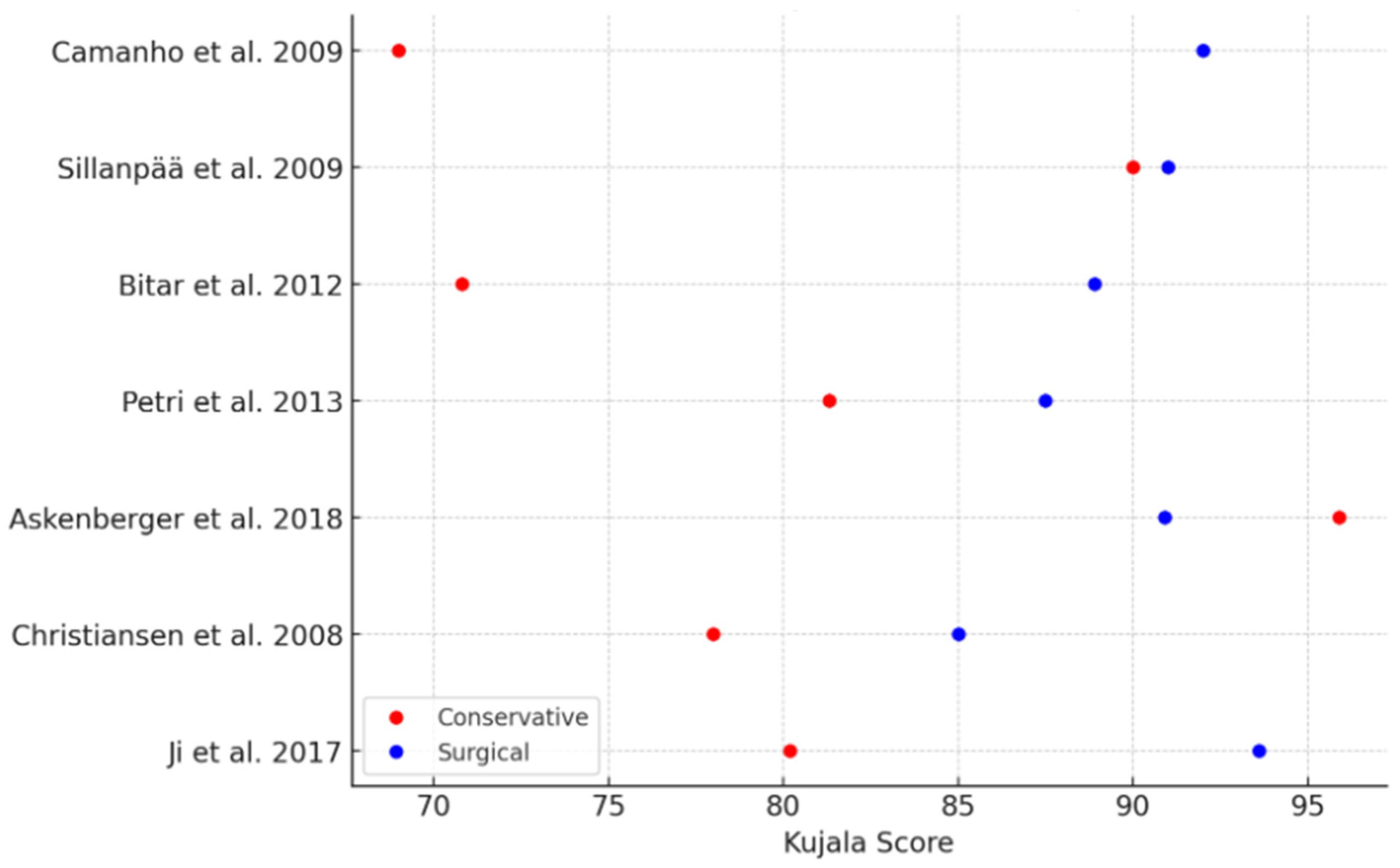
3.5. Kujala Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kasitinon, D.; Li, W.-X.; Wang, E.X.S.; Fredericson, M. Physical Examination and Patellofemoral Pain Syndrome: An Updated Review. Curr. Rev. Musculoskelet. Med. 2021, 14, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L.M. Epidemiology and Natural History of Acute Patellar Dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Csintalan, R.P.; Schulz, M.M.; Woo, J.; McMahon, P.J.; Lee, T.Q. Gender Differences in Patellofemoral Joint Biomechanics. Clin. Orthop. Relat. Res. 2002, 402, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Maffulli, N.; Vaishya, R. Patellofemoral Instability: Current Status and Future Perspectives. J. Orthop. 2022, 36, 49–50. [Google Scholar] [CrossRef]
- Hayat, Z.; El Bitar, Y.; Case, J.L. Patella Dislocation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Smith, T.O.; Davies, L.; O’Driscoll, M.-L.; Donell, S.T. An Evaluation of the Clinical Tests and Outcome Measures Used to Assess Patellar Instability. Knee 2008, 15, 255–262. [Google Scholar] [CrossRef]
- Anley, C.M.; Morris, G.V.; Saithna, A.; James, S.L.; Snow, M. Defining the Role of the Tibial Tubercle-Trochlear Groove and Tibial Tubercle-Posterior Cruciate Ligament Distances in the Work-up of Patients With Patellofemoral Disorders. Am. J. Sports Med. 2015, 43, 1348–1353. [Google Scholar] [CrossRef]
- Frings, J.; Balcarek, P.; Tscholl, P.; Liebensteiner, M.; Dirisamer, F.; Koenen, P. Conservative Versus Surgical Treatment for Primary Patellar Dislocation. Dtsch. Arztebl. Int. 2020, 117, 279–286. [Google Scholar] [CrossRef]
- Dejour, D.H.; Mesnard, G.; Giovannetti de Sanctis, E. Updated Treatment Guidelines for Patellar Instability: “Un Menu à La Carte”. J. Exp. Orthop. 2021, 8, 109. [Google Scholar] [CrossRef]
- Flores, G.W.; de Oliveira, D.F.; Ramos, A.P.S.; Sanada, L.S.; Migliorini, F.; Maffulli, N.; Okubo, R. Conservative Management Following Patellar Dislocation: A Level I Systematic Review. J. Orthop. Surg. Res. 2023, 18, 393. [Google Scholar] [CrossRef]
- Sanchis-Alfonso, V. Guidelines for Medial Patellofemoral Ligament Reconstruction in Chronic Lateral Patellar Instability. JAAOS-J. Am. Acad. Orthop. Surg. 2014, 22, 175. [Google Scholar] [CrossRef]
- Migliorini, F.; Oliva, F.; Maffulli, G.D.; Eschweiler, J.; Knobe, M.; Tingart, M.; Maffulli, N. Isolated Medial Patellofemoral Ligament Reconstruction for Recurrent Patellofemoral Instability: Analysis of Outcomes and Risk Factors. J. Orthop. Surg. Res. 2021, 16, 239. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.N.; Howard, J.S.; Flanigan, D.C.; Brophy, R.H.; Carey, J.L.; Lattermann, C. A Systematic Review of Complications and Failures Associated with Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Dislocation. Am. J. Sports Med. 2012, 40, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Lieber, A.C.; Steinhaus, M.E.; Liu, J.N.; Hurwit, D.; Chiaia, T.; Strickland, S.M. Quality and Variability of Online Available Physical Therapy Protocols From Academic Orthopaedic Surgery Programs for Medial Patellofemoral Ligament Reconstruction. Orthop. J. Sports Med. 2019, 7, 2325967119855991. [Google Scholar] [CrossRef] [PubMed]
- Barber-Westin, S.D.; Noyes, F.R.; McCloskey, J.W. Rigorous Statistical Reliability, Validity, and Responsiveness Testing of the Cincinnati Knee Rating System in 350 Subjects with Uninjured, Injured, or Anterior Cruciate Ligament-Reconstructed Knees. Am. J. Sports Med. 1999, 27, 402–416. [Google Scholar] [CrossRef] [PubMed]
- Briggs, K.K.; Lysholm, J.; Tegner, Y.; Rodkey, W.G.; Kocher, M.S.; Steadman, J.R. The Reliability, Validity, and Responsiveness of the Lysholm Score and Tegner Activity Scale for Anterior Cruciate Ligament Injuries of the Knee: 25 Years Later. Am. J. Sports Med. 2009, 37, 890–897. [Google Scholar] [CrossRef]
- Smith, T.O.; Choudhury, A.; Navratil, R.; Hing, C.B. Psychometric Properties of the Norwich Patellar Instability Score in People with Recurrent Patellar Dislocation. Knee 2019, 26, 1192–1197. [Google Scholar] [CrossRef]
- Xie, C.X.; Machado, G.C. Clinimetrics: Grading of Recommendations, Assessment, Development and Evaluation (GRADE). J. Physiother. 2021, 67, 66. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Kujala, U.M.; Jaakkola, L.H.; Koskinen, S.K.; Taimela, S.; Hurme, M.; Nelimarkka, O. Scoring of Patellofemoral Disorders. Arthroscopy 1993, 9, 159–163. [Google Scholar] [CrossRef]
- Sillanpää, P.J.; Mattila, V.M.; Mäenpää, H.; Kiuru, M.; Visuri, T.; Pihlajamäki, H. Treatment with and without Initial Stabilizing Surgery for Primary Traumatic Patellar Dislocation. A Prospective Randomized Study. J. Bone Joint Surg. Am. 2009, 91, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Nikku, R.; Nietosvaara, Y.; Kallio, P.E.; Aalto, K.; Michelsson, J.E. Operative versus Closed Treatment of Primary Dislocation of the Patella. Similar 2-Year Results in 125 Randomized Patients. Acta Orthop. Scand. 1997, 68, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Regalado, G.; Lintula, H.; Kokki, H.; Kröger, H.; Väätäinen, U.; Eskelinen, M. Six-Year Outcome after Non-Surgical versus Surgical Treatment of Acute Primary Patellar Dislocation in Adolescents: A Prospective Randomized Trial. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 6–11. [Google Scholar] [CrossRef]
- Bitar, A.C.; Demange, M.K.; D’Elia, C.O.; Camanho, G.L. Traumatic Patellar Dislocation: Nonoperative Treatment Compared with MPFL Reconstruction Using Patellar Tendon. Am. J. Sports Med. 2012, 40, 114–122. [Google Scholar] [CrossRef]
- Camanho, G.L.; de Christo Viegas, A.; Bitar, A.C.; Demange, M.K.; Hernandez, A.J. Conservative versus Surgical Treatment for Repair of the Medial Patellofemoral Ligament in Acute Dislocations of the Patella. Arthroscopy 2009, 25, 620–625. [Google Scholar] [CrossRef]
- Petri, M.; Liodakis, E.; Hofmeister, M.; Despang, F.J.; Maier, M.; Balcarek, P.; Voigt, C.; Haasper, C.; Zeichen, J.; Stengel, D.; et al. Operative vs Conservative Treatment of Traumatic Patellar Dislocation: Results of a Prospective Randomized Controlled Clinical Trial. Arch. Orthop. Trauma. Surg. 2013, 133, 209–213. [Google Scholar] [CrossRef]
- Christiansen, S.E.; Jakobsen, B.W.; Lund, B.; Lind, M. Isolated Repair of the Medial Patellofemoral Ligament in Primary Dislocation of the Patella: A Prospective Randomized Study. Arthroscopy 2008, 24, 881–887. [Google Scholar] [CrossRef]
- Askenberger, M.; Bengtsson Moström, E.; Ekström, W.; Arendt, E.A.; Hellsten, A.; Mikkelsen, C.; Janarv, P.-M. Operative Repair of Medial Patellofemoral Ligament Injury Versus Knee Brace in Children With an Acute First-Time Traumatic Patellar Dislocation: A Randomized Controlled Trial. Am. J. Sports Med. 2018, 46, 2328–2340. [Google Scholar] [CrossRef]
- Ji, G.; Wang, S.; Wang, X.; Liu, J.; Niu, J.; Wang, F. Surgical versus Nonsurgical Treatments of Acute Primary Patellar Dislocation with Special Emphasis on the MPFL Injury Patterns. J. Knee Surg. 2017, 30, 378–384. [Google Scholar] [CrossRef]
- Apostolovic, M.; Vukomanovic, B.; Slavkovic, N.; Vuckovic, V.; Vukcevic, M.; Djuricic, G.; Kocev, N. Acute Patellar Dislocation in Adolescents: Operative versus Nonoperative Treatment. Int. Orthop. 2011, 35, 1483–1487. [Google Scholar] [CrossRef]
- Cerciello, S.; Corona, K.; Morris, B.J.; Visonà, E.; Maccauro, G.; Maffulli, N.; Ronga, M. Cross-Cultural Adaptation and Validation of the Italian Versions of the Kujala, Larsen, Lysholm and Fulkerson Scores in Patients with Patellofemoral Disorders. J. Orthop. Traumatol. 2018, 19, 18. [Google Scholar] [CrossRef]
- Dopirak, R.M.; Steensen, R.N.; Maurus, P.B. The Medial Patellofemoral Ligament. Orthopedics 2008, 31, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Hinckel, B.; Smith, J.; Tanaka, M.J.; Matsushita, T.; Martinez-Cano, J.P. Patellofemoral Instability Part 1 (When to Operate and Soft Tissue Procedures): State of the Art. J. ISAKOS 2024, 10, 100278. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.S.; Turner, P.G. Management of the First-Time Lateral Patellar Dislocation. Knee 2019, 26, 1161–1165. [Google Scholar] [CrossRef] [PubMed]
- Arendt, E.A.; Donell, S.T.; Sillanpää, P.J.; Feller, J.A. The Management of Lateral Patellar Dislocation: State of the Art. J. ISAKOS 2017, 2, 205–212. [Google Scholar] [CrossRef]
- Amis, A.A.; Firer, P.; Mountney, J.; Senavongse, W.; Thomas, N.P. Anatomy and Biomechanics of the Medial Patellofemoral Ligament. Knee 2003, 10, 215–220. [Google Scholar] [CrossRef]
- Mäenpää, H.; Lehto, M.U. Patellar Dislocation. The Long-Term Results of Nonoperative Management in 100 Patients. Am. J. Sports Med. 1997, 25, 213–217. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Sample | Type of Study | Follow Up |
|---|---|---|---|---|
| Camanho et al. [26] | 2009 | N = 33 13 M, 20 F Average age 24.6 | RCT | Average 38.35 months |
| Sillanpää et al. [22] | 2009 | N = 40 37 M, 3 F Average age 20 | RCT | Average 7 years |
| Bitar et al. [25] | 2012 | N = 39 21 M, 20 F Average age 24.2 | RCT | Average 44 months |
| Petri et al. [27] | 2013 | N = 20 Average age 24.6 | RCT | 24 months |
| Askenberger et al. [29] | 2018 | N = 74 36 M, 38 F Age 9–14 | RCT | 24 months |
| Christiansen et al. [28] | 2008 | N = 80 Age = 14–40 | RCT | 24 months |
| Apostolovic et al. [31] | 2011 | N = 37 Average age 13.8 | NRSI | Average 6.1 years |
| Ji et al. [30] | 2017 | N = 62 | RCT | Average 42 months |
| Regalado et al. [24] | 2016 | N = 36 Average age 13.5 | RCT | 72 months |
| Nikku et al. [23] | 1997 | N = 125 Average age 20 | RCT | 25 months |
| Studies | N° of Patients | Conservative Treatment | Surgical Treatment | Re-Dislocation in Conservative | Re-Dislocation in Surgical | Kujala in Conservative | Kujala in Surgical |
|---|---|---|---|---|---|---|---|
| Comanho et al., 2009 | 33 | 16 | 17 | 8 (50%) | 0 | 69 | 92 |
| Sillanpää et al., 2009 | 40 | 22 | 18 | 6 (27.3%) | 0 | 90 | 91 |
| Bitar et al., 2012 | 39 | 20 | 19 | 7 (35%) | 0 | 70.8 | 88.9 |
| Petri et al., 2013 | 20 | 8 | 12 | 3 (37.5%) | 2 (16.7%) | 81.3 | 87.5 |
| Askenberger et al., 2018 | 74 | 36 | 38 | 16 (44.4%) | 8 (21.1%) | 95.9 | 90.9 |
| Christiansen et al., 2008 | 77 | 35 | 42 | 7 (20%) | 7 (16.7%) | 78 | 85 |
| Apostolovic et al., 2011 | 37 | 23 | 14 | 3 (13%) | 5 (35.7%) | NI | NI |
| Ji et al., 2017 | 62 | 30 | 32 | 7 (23.3%) | 4 (12.5%) | 80.2 | 93.6 |
| Regalado et al., 2016 | 36 | 20 | 16 | 11 (55%) | 5 (31.3%) | NI | NI |
| Nikku et al., 1997 | 125 | 55 | 70 | 15 (27.3%) | 12 (17.1%) | NI | NI |
| Total | 543 | 265 | 278 | 83 (33.1%) | 43 (17.1%) | 80.7 | 89.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavone, V.; Perricone, E.; Pirrone, G.S.; Caldaci, A.; Iacona, M.; Sapienza, M.; Testa, G. A Systematic Review Comparing Conservative and Surgical Approaches in the Management of Patellofemoral Instability. Appl. Sci. 2025, 15, 2585. https://doi.org/10.3390/app15052585
Pavone V, Perricone E, Pirrone GS, Caldaci A, Iacona M, Sapienza M, Testa G. A Systematic Review Comparing Conservative and Surgical Approaches in the Management of Patellofemoral Instability. Applied Sciences. 2025; 15(5):2585. https://doi.org/10.3390/app15052585
Chicago/Turabian StylePavone, Vito, Emanuele Perricone, Giorgio Santi Pirrone, Alessia Caldaci, Michele Iacona, Marco Sapienza, and Gianluca Testa. 2025. "A Systematic Review Comparing Conservative and Surgical Approaches in the Management of Patellofemoral Instability" Applied Sciences 15, no. 5: 2585. https://doi.org/10.3390/app15052585
APA StylePavone, V., Perricone, E., Pirrone, G. S., Caldaci, A., Iacona, M., Sapienza, M., & Testa, G. (2025). A Systematic Review Comparing Conservative and Surgical Approaches in the Management of Patellofemoral Instability. Applied Sciences, 15(5), 2585. https://doi.org/10.3390/app15052585