
Assessment of Fluoride-Releasing Materials in Remineralization of Adjacent Demineralized Enamel



Abstract
1. Introduction
2. Materials and Methods
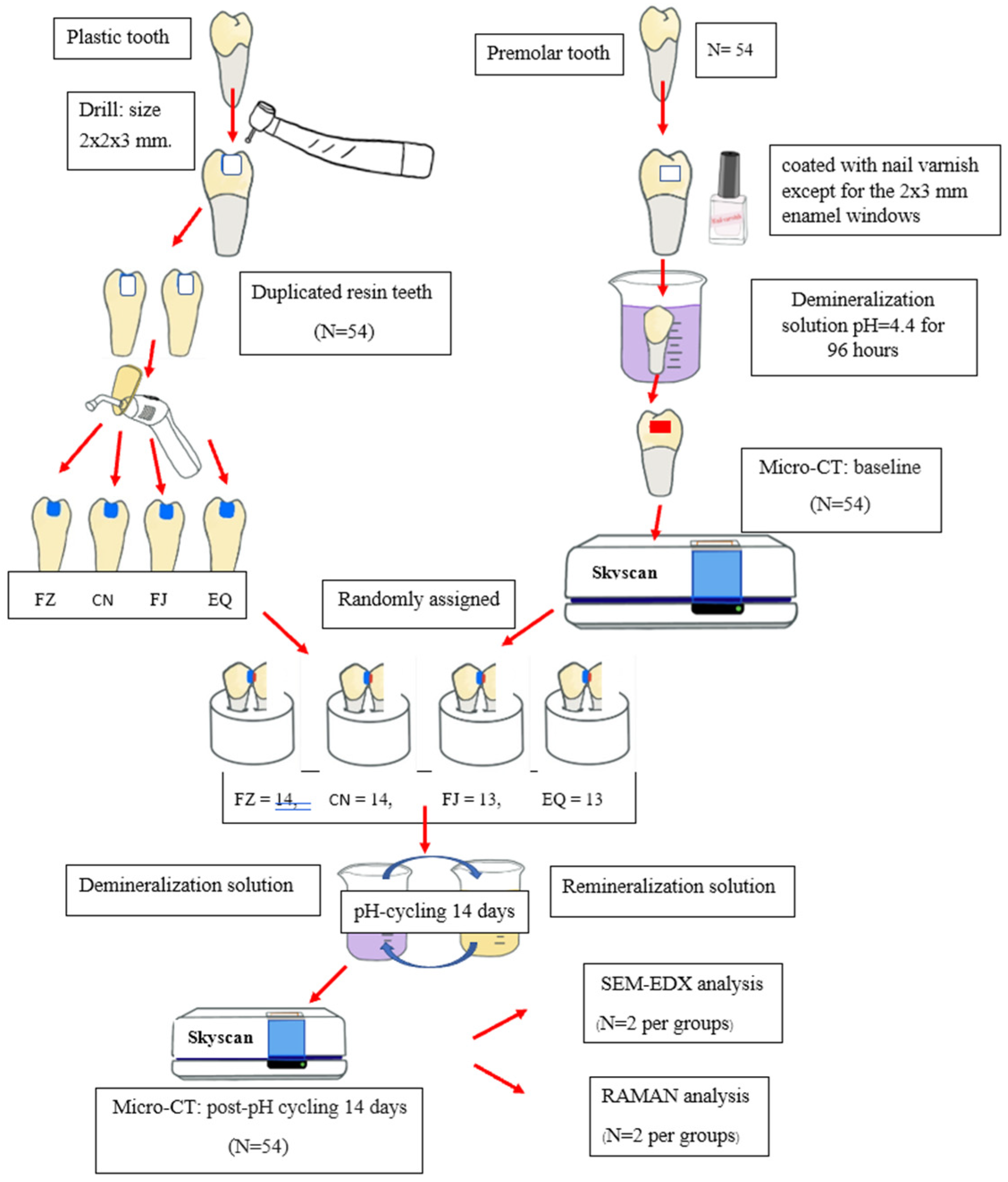
2.1. Sample Size Calculation and Tooth Selection
2.2. Formation of Artificially Demineralized Proximal Enamel Lesion
2.3. Preparation of Restoration Tooth and Mounting in Contact
2.4. pH Cycling Model
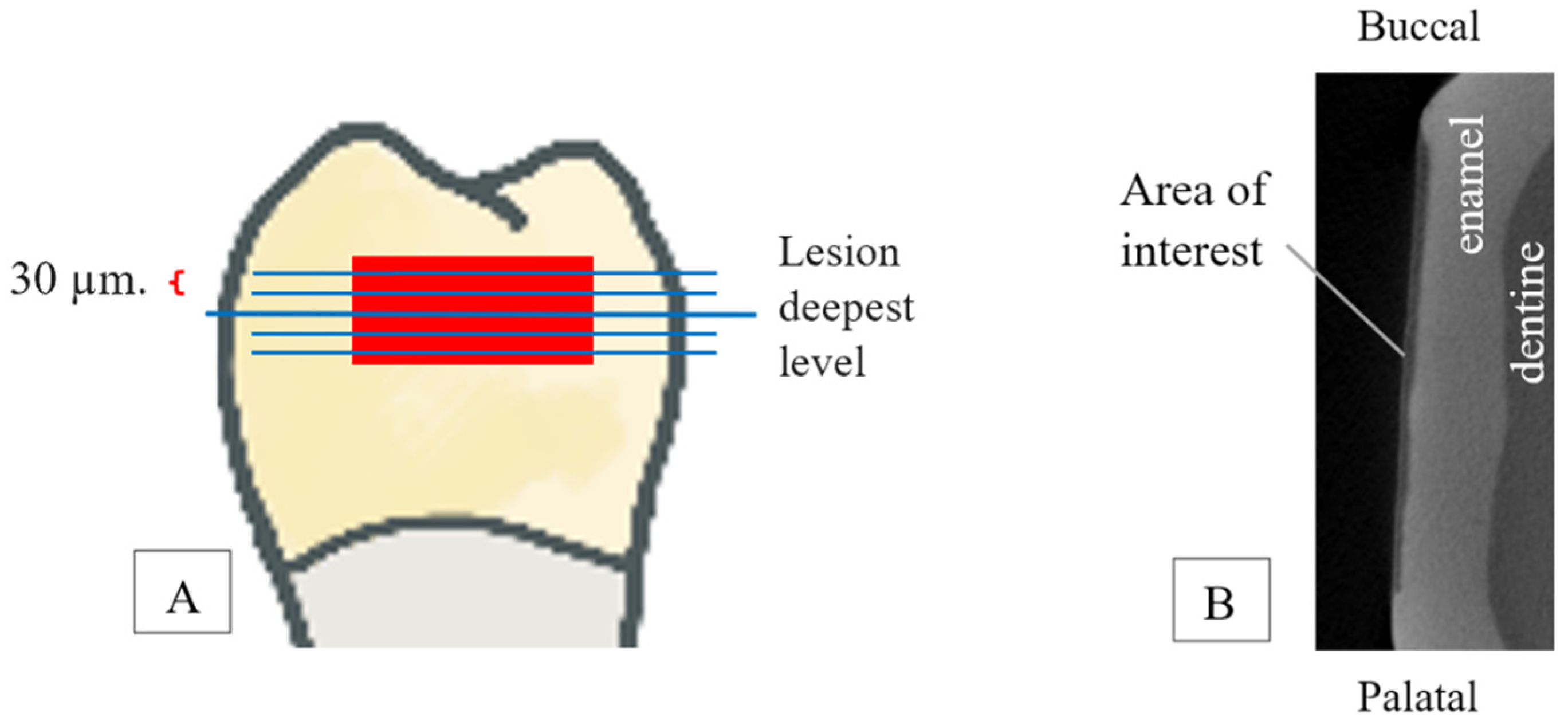
2.5. Micro-CT Scanning
2.6. Scanning Electron Microscope (SEM) and Energy-Dispersive X-Ray Microscope (EDX)
2.7. Raman Imaging Microscope
2.8. Statistical Analysis
3. Results
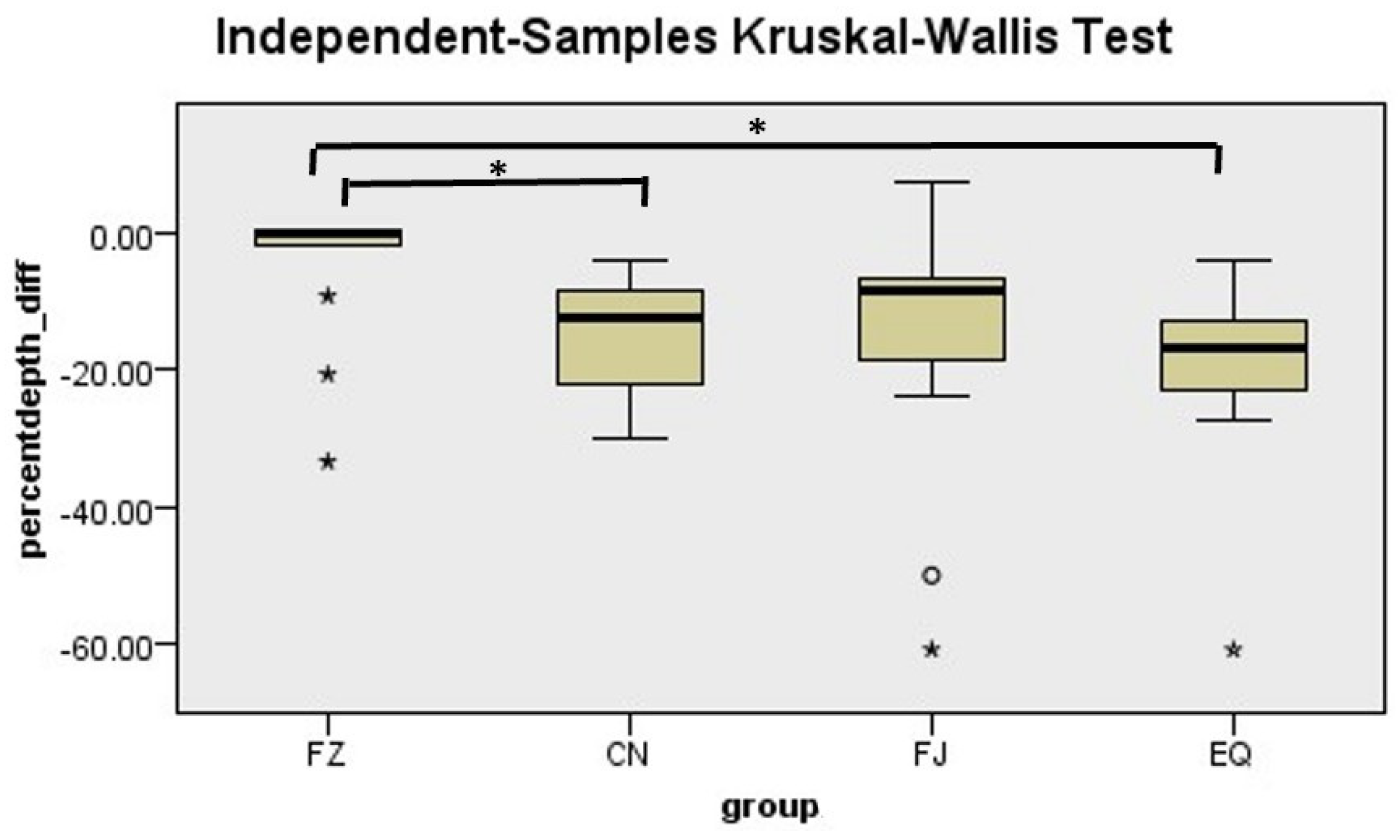
3.1. Lesion Depth
3.2. Mineral Density
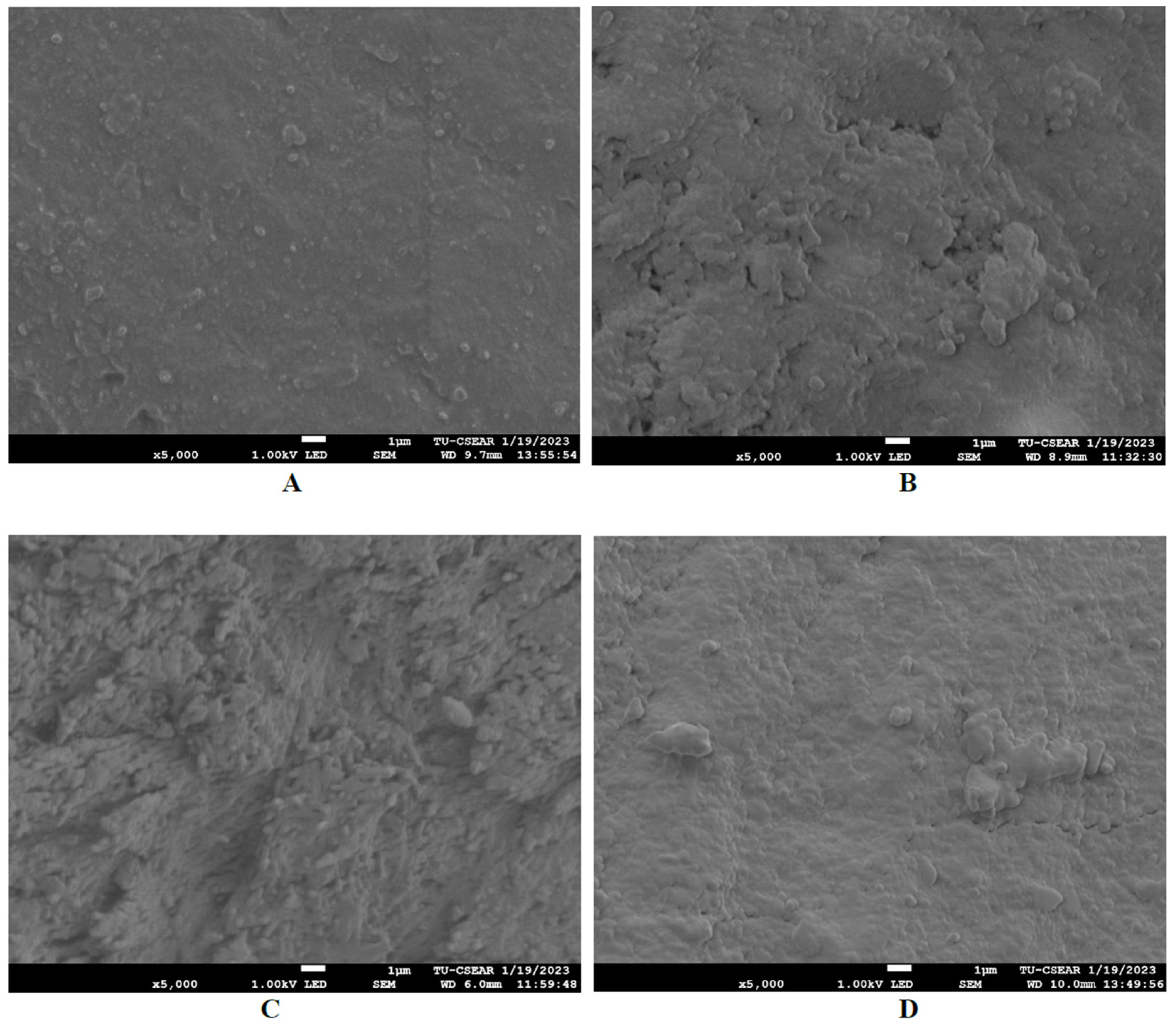
3.3. Scanning Electron Microscope (SEM) and Energy-Dispersive X-Ray Microscope (EDX)
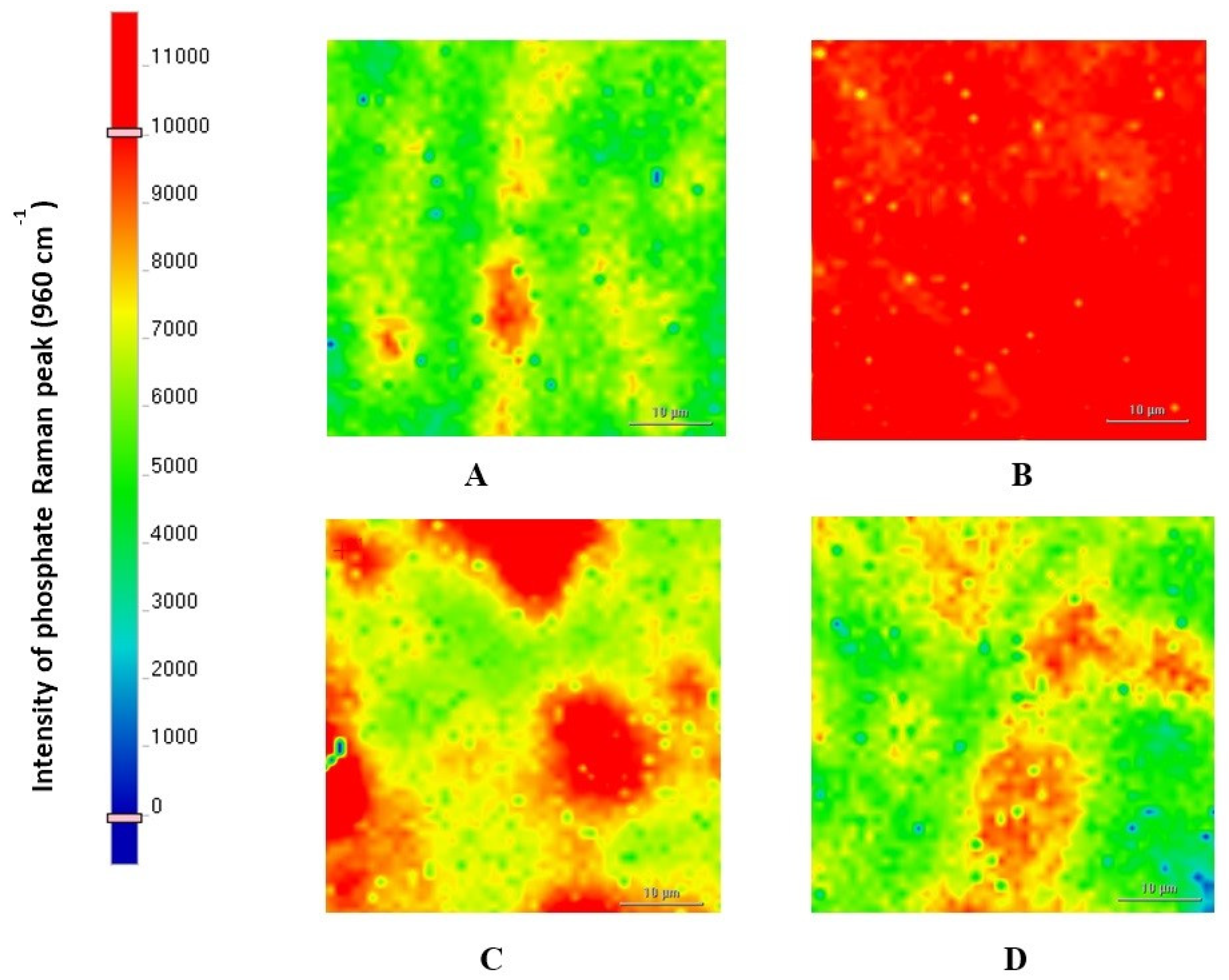
3.4. Raman Imaging Microscope
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gao, S.S.; Zhang, S.; Mei, M.L.; Lo, E.C.; Chu, C.H. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment—A systematic review. BMC Oral. Health 2016, 16, 12. [Google Scholar] [CrossRef]
- Tedesco, T.K.; Bonifacio, C.C.; Calvo, A.F.; Gimenez, T.; Braga, M.M.; Raggio, D.P. Caries lesion prevention and arrestment in approximal surfaces in contact with glass ionomer cement restorations—A systematic review and meta-analysis. Int. J. Paediatr. Dent. 2016, 26, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Trairatvorakul, C.; Itsaraviriyakul, S.; Wiboonchan, W. Effect of glass-ionomer cement on the progression of proximal caries. J. Dent. Res. 2011, 90, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Philip, N. State of the Art Enamel Remineralization Systems: The Next Frontier in Caries Management. Caries Res. 2019, 53, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Guntermann, L.; Rohrbach, A.; Schäfer, E.; Dammaschke, T. Remineralization and protection from demineralization: Effects of a hydroxyapatite-containing, a fluoride-containing and a fluoride-and hydroxyapatite-free toothpaste on human enamel in vitro. Head Face Med. 2022, 18, 26. [Google Scholar] [CrossRef]
- Wang, Y.; Mei, L.; Gong, L.; Li, J.; He, S.; Ji, Y.; Sun, W. Remineralization of early enamel caries lesions using different bioactive elements containing toothpastes: An in vitro study. Technol. Health Care 2016, 24, 701–711. [Google Scholar] [CrossRef] [PubMed]
- Wongphattarakul, S.; Kuson, R.; Sastraruji, T.; Suttiat, K. Fluoride Release and Rechargeability of Poly(lactic acid) Composites with Glass Ionomer Cement. Polymers 2023, 15, 4041. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, A.M.; Elshehawy, T.M.; Ibrahim, H.M. Fluoride release and recharge behavior of bioactive glass ionomer cements using ion chromatography. Egypt. Dent. J. 2019, 65, 399–406. [Google Scholar] [CrossRef]
- Smith, D.C. Development of glass-ionomer cement systems. Biomat 1998, 19, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Krämer, N.; Schmidt, M.; Lücker, S.; Domann, E.; Frankenberger, R. Glass ionomer cement inhibits secondary caries in an in vitro biofilm model. Clin. Oral. Investig. 2018, 22, 1019–1031. [Google Scholar] [CrossRef] [PubMed]
- Qvist, V.; Poulsen, A.; Teglers, P.T.; Mjör, I.A. Fluorides leaching from restorative materials and the effect on adjacent teeth. Int. Dent. J. 2010, 60, 156–160. [Google Scholar] [PubMed]
- Roulet, J.; Hussein, H.; Abdulhameed, N.; Shen, C. In vitro wear of two bioactive composites and a glass ionomer cement. DZZ Int. 2019, 1, 24–30. [Google Scholar]
- Minocha, A.; Sharma, V.; Gupta, A.; Sharma, N. Comparative evaluation of Cention N and Amalgam in Class II posterior restorations. Univ. J. Dent. Sci. 2021, 7. [Google Scholar] [CrossRef]
- Mazumdar, P.; Das, A.; Das, U.K. Comparative evaluation of microleakage of three different direct restorative materials (silver amalgam, glass ionomer cement, Cention N), in class II restorations using stereomicroscope: An in vitro study. Indian J. Dent. Res. 2019, 30, 277. [Google Scholar] [PubMed]
- Chole, D.; Shah, H.K.; Kundoor, S.; Bakle, S.; Gandhi, N.; Hatte, N. In vitro comparison of flexural strength of cention-n, bulkFill composites, light-cure nanocomposites and resin-modified glass ionomer cement. J. Dent. Med. Sci. 2018, 17, 79. [Google Scholar]
- Mazumdar, P.; Das, A.; Guha, C. Comparative evaluation of hardness of different restorative materials (restorative gic, cention N, nanohybrid composite resin and silver amalgam)—An in vitro study. Int. J. Adv. Res. 2018, 6, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Deepak, S.; Nivedhitha, M. Proximal contact tightness between two different restorative materials—An in vitro study. J. Adv. Pharm. Educ. Res. 2017, 7, 153–156. [Google Scholar]
- Gupta, N.; Jaiswal, S.; Nikhil, V.; Gupta, S.; Jha, P.; Bansal, P. Comparison of fluoride ion release and alkalizing potential of a new bulk-fill alkasite. J. Conserv. Dent. 2019, 22, 296. [Google Scholar] [CrossRef] [PubMed]
- Theerarath, T.; Sriarj, W. An alkasite restorative material effectively remineralized artificial interproximal enamel caries in vitro. Clin. Oral. Investig. 2022, 26, 4437–4445. [Google Scholar] [CrossRef] [PubMed]
- Phyo, W.M.; Saket, D.; da Fonseca, M.A.; Auychai, P.; Sriarj, W. In vitro remineralization of adjacent interproximal enamel carious lesions in primary molars using a bioactive bulk-fill composite. BMC Oral. Health. 2024, 24, 37. [Google Scholar] [CrossRef]
- Lee, H.S.; Berg, J.H.; García-Godoy, F.; Jang, K.T. Long-term evaluation of the remineralization of interproximal caries-like lesions adjacent to glass-ionomer restorations: A micro-CT study. Am. J. Dent. 2008, 21, 129–132. [Google Scholar] [PubMed]
- Rana, R.; Itthagarun, A.; King, N.M. Effects of dentifrices on artificial caries like lesions: An in vitro pH cycling study. Int. Dent. J. 2007, 57, 243–248. [Google Scholar] [CrossRef]
- Ten Cate, J.; Arends, J. Remineralization of artificial enamel lesions in vitro: III. A study of the deposition mechanism. Caries Res. 1980, 14, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.; Glena, R.; Shariati, M.; Shields, C. Dependence of in vitro demineralization of apatite and remineralization of dental enamel on fluoride concentration. J. Dent. Res. 1990, 69, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Brzović-Rajić, V.; Miletić, I.; Gurgan, S.; Peroš, K.; Verzak, Ž.; Ivanišević-Malčić, A. Fluoride release from glass ionomer with nano filled coat and varnish. Acta Stomatol. Croat. 2018, 52, 307. [Google Scholar] [CrossRef] [PubMed]
- Donly, K.J.; Segura, A.; Wefel, J.S.; Hogan, M.M. Evaluating the effects of fluoride-releasing dental materials on adjacent interproximal caries. J. Am. Dent. Assoc. 1999, 130, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Baliga, M.S.; Bhat, S.S. Effect of fluorides from various restorative materials on remineralization of adjacent tooth: An in vitro study. J. Indian Soc. Pedod. Prev. Dent. 2010, 28, 84–90. [Google Scholar] [CrossRef]
- Jang, K.-T.; Garcia-Godoy, F.; Donly, K.J.; Segura, A. Remineralizing effects of glass ionomer restorations on adjacent interproximal caries. ASDC J. Dent. Child. 2001, 68, 125–128+142. [Google Scholar] [PubMed]
- Kuphasuk, S.; Kunawarote, S. In vitro Caries Inhibition in Enamel Adjacent to Ion-releasing Resin Composite: Original articles. CM Dent. J. 2022, 43, 50–61. [Google Scholar]
- Albelasy, E.H.; Chen, R.; Fok, A.; Montasser, M.; Hamama, H.H.; Mahmoud, S.H.; Abdelrehim, T.; Chew, H.P. Inhibition of Caries around Restoration by Ion-Releasing Restorative Materials: An In Vitro Optical Coherence Tomography and Micro-Computed Tomography Evaluation. Materials 2023, 16, 5558. [Google Scholar] [CrossRef] [PubMed]
- Todd, J.C. Scientific Documentation: Cention N; Ivoclar-Vivadent Press: Schaan, Liechtenstein, 2016; pp. 1–58. [Google Scholar]
- Wiriyasatiankun, P.; Sakoolnamarka, R.; Thanyasrisung, P. The impact of an alkasite restorative material on the pH of Streptococcus mutans biofilm and dentin remineralization: An in vitro study. BMC Oral. Health 2022, 22, 334. [Google Scholar] [CrossRef]
- Nantanee, R.; Santiwong, B.; Trairatvorakul, C.; Hamba, H.; Tagami, J. Silver diamine fluoride and glass ionomer differentially remineralize early caries lesions, in situ. Clin. Oral. Investig. 2016, 20, 1151–1157. [Google Scholar] [CrossRef]
- Retief, D.; Bradley, E.; Denton, J.; Switzer, P. Enamel and cementum fluoride uptake from a glass ionomer cement. Caries Res. 1984, 18, 250–257. [Google Scholar] [CrossRef]
- Ruengrungsom, C.; Burrow, M.F.; Parashos, P.; Palamara, J.E. Evaluation of F, Ca, and P release and microhardness of eleven ion-leaching restorative materials and the recharge efficacy using a new Ca/P containing fluoride varnish. J. Dent. 2020, 102, 103474. [Google Scholar] [CrossRef]
- Kim, M.J.; Lee, M.J.; Kim, K.M.; Yang, S.Y.; Seo, J.Y.; Choi, S.H.; Kwon, J.S. Enamel demineralization resistance and remineralization by various fluoride-releasing dental restorative materials. Materials 2021, 14, 4554. [Google Scholar] [CrossRef] [PubMed]
- Panpisut, P.; Toneluck, A. Monomer conversion, dimensional stability, biaxial flexural strength, and fluoride release of resin-based restorative material containing alkaline fillers. Dent. Mater. J. 2020, 39, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Tran, D.; Kang, Y.; Dunn, K.; Kugel, G. Hydroxyapatite Formation of Dental Restorative Materials. J. Dent. Sci. 2020, 5, 000263. [Google Scholar] [CrossRef]
- Di Lauro, A.; Di Duca, F.; Montuori, P.; Dal Piva, A.M.O.; Tribst, J.P.M.; Borges, A.L.S.; Ausiello, P. Fluoride and Calcium Release from Alkasite and Glass Ionomer Restorative Dental Materials: In Vitro Study. J. Funct. Biomater. 2023, 14, 109. [Google Scholar] [CrossRef] [PubMed]
- Feiz, A.; Nicoo, M.A.; Parastesh, A.; Jafari, N.; Sarfaraz, D. Comparison of antibacterial activity and fluoride release in tooth-colored restorative materials: Resin-modified glass ionomer, zirconomer, giomer, and cention N. Dent. Res. J. 2022, 19, 104. [Google Scholar]
- Singbal, K.; Shan, M.K.W.; Dutta, S.; Kacharaju, K.R. Cention N Compared to Other Contemporary Tooth-Colored Restorative Materials in Terms of Fluoride Ion Releasing Efficacy: Validation of a Novel Caries-Prevention-Initiative by the Ministry of Health, Malaysia. Biomed. Pharmacol. J. 2022, 15, 669–676. [Google Scholar] [CrossRef]
- Donly, K.J.; Liu, J.A. Dentin and enamel demineralization inhibition at restoration margins of Vitremer, Z 100 and Cention N. Am. J. Dent. 2018, 31, 166–168. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Chemical Compositions | Lot Number | Manufacturer |
|---|---|---|---|
| Filtek Z350 XT (Nanofilled resin composite) | Urethane dimethacrylate, Bis-GMA, PEGDMA, Bis-EMA, TEGDMA, zirconia, silica | 10130616 (shade A3) | 3M ESPE, St. Paul, MN, USA |
| Cention N (Alkasite resin-based restorative material) | Powder: inorganic fillers (Ba-Al-Ca-Ba-Al-F silicate glass, Ca-F silicate glass, YtF3) and customized fillers Liquid: urethane dimethacrylate, tricyclodecan- dimethanol dimethacrtylate, polyethylene glycol dimethacrylate | Z0232K (shade A2) | Ivoclar Vivadent, Schaan, Liechtenstein |
| GC Fuji II LC (Light-cured resin- modified glass ionomer cement) | Powder: 100% fluoroalumino silicate glass Liquid: 20–22% polyacrylic acid, 30–40% 2-hydroxyethyl methacrylate (HEMA), 5–7% trimethyl hexamethylene dicarbonate, 4–6% triethylene glycol dimethacrylate, ˂10% urethane dimethacrylate, initiator, ˂1% camphroquinone | 2105081 (shade A3) | GC Corporation, Tokyo, Japan |
| Equia Forte Fil (Glass hybrid self-cured glass ionomer cement) | Powder: 95% strontium fluoroalumino silicate glass and 5% polyacrylic acid Liquid: 40% aqueous polyacrylic acid | 2108031 (shade A3) | GC Corporation, Tokyo, Japan |
| Group (n) | Lesion Depth (µm) | Mineral Density (mgHA/cm3) | ||
|---|---|---|---|---|
| Baseline | Post-pH Cycling | Baseline | Post-pH Cycling | |
| FZ (14) | 125.50 ± 18.07 a | 119.36 ± 20.48 | 1543.37 ± 86.44 a | 1595.56 ± 94.00 * |
| CN (14) | 128.14 ± 19.01 a | 109.71 ± 22.91 * | 1543.35 ± 153.81 a | 1604.91 ± 144.45 * |
| FJ (13) | 132.15 ± 27.84 a | 112.00 ± 39.27 * | 1507.01 ± 122.38 a | 1610.46 ± 144.12 * |
| EQ (13) | 132.77 ± 21.20 a | 107.31 ± 26.88 * | 1499.20 ± 115.24 a | 1600.26 ± 135.73 * |
| Group (n) | Percentage Change in Lesion Depth (%) | Percentage Change in Mineral Density (%) | ||
|---|---|---|---|---|
| Mean ± SD | Mean Rank | Mean ± SD | Mean Rank | |
| FZ (14) | −4.73 ± 10.03 | 41.00 a | 3.40 ± 3.03 | 23.29 a |
| CN (14) | −14.98 ± 8.81 | 22.43 b | 4.20 ± 5.02 | 26.71 a |
| FJ (13) | −16.16 ± 19.14 | 26.46 a,b | 7.05 ± 7.71 | 32.15 a |
| EQ (13) | −19.18 ± 14.35 | 19.46 b | 6.80 ± 7.66 | 28.23 a |
| % Weight | Ca | P | Ca/P Ratio | |
|---|---|---|---|---|
| % Restorative Material | ||||
| FZ | 1.91 | 2.55 | 0.75 | |
| CN | 10.78 | 8.18 | 1.32 | |
| FJ | 27.3 | 12.59 | 2.17 | |
| EQ | 8.82 | 6.67 | 1.32 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puttipanampai, O.; Panpisut, P.; Sitthisettapong, T. Assessment of Fluoride-Releasing Materials in Remineralization of Adjacent Demineralized Enamel. Appl. Sci. 2025, 15, 2077. https://doi.org/10.3390/app15042077
Puttipanampai O, Panpisut P, Sitthisettapong T. Assessment of Fluoride-Releasing Materials in Remineralization of Adjacent Demineralized Enamel. Applied Sciences. 2025; 15(4):2077. https://doi.org/10.3390/app15042077
Chicago/Turabian StylePuttipanampai, Onsinee, Piyaphong Panpisut, and Thanya Sitthisettapong. 2025. "Assessment of Fluoride-Releasing Materials in Remineralization of Adjacent Demineralized Enamel" Applied Sciences 15, no. 4: 2077. https://doi.org/10.3390/app15042077
APA StylePuttipanampai, O., Panpisut, P., & Sitthisettapong, T. (2025). Assessment of Fluoride-Releasing Materials in Remineralization of Adjacent Demineralized Enamel. Applied Sciences, 15(4), 2077. https://doi.org/10.3390/app15042077