

A Small Implantable Compact Antenna for Wireless Telemetry Applied to Wireless Body Area Networks


Abstract
1. Introduction
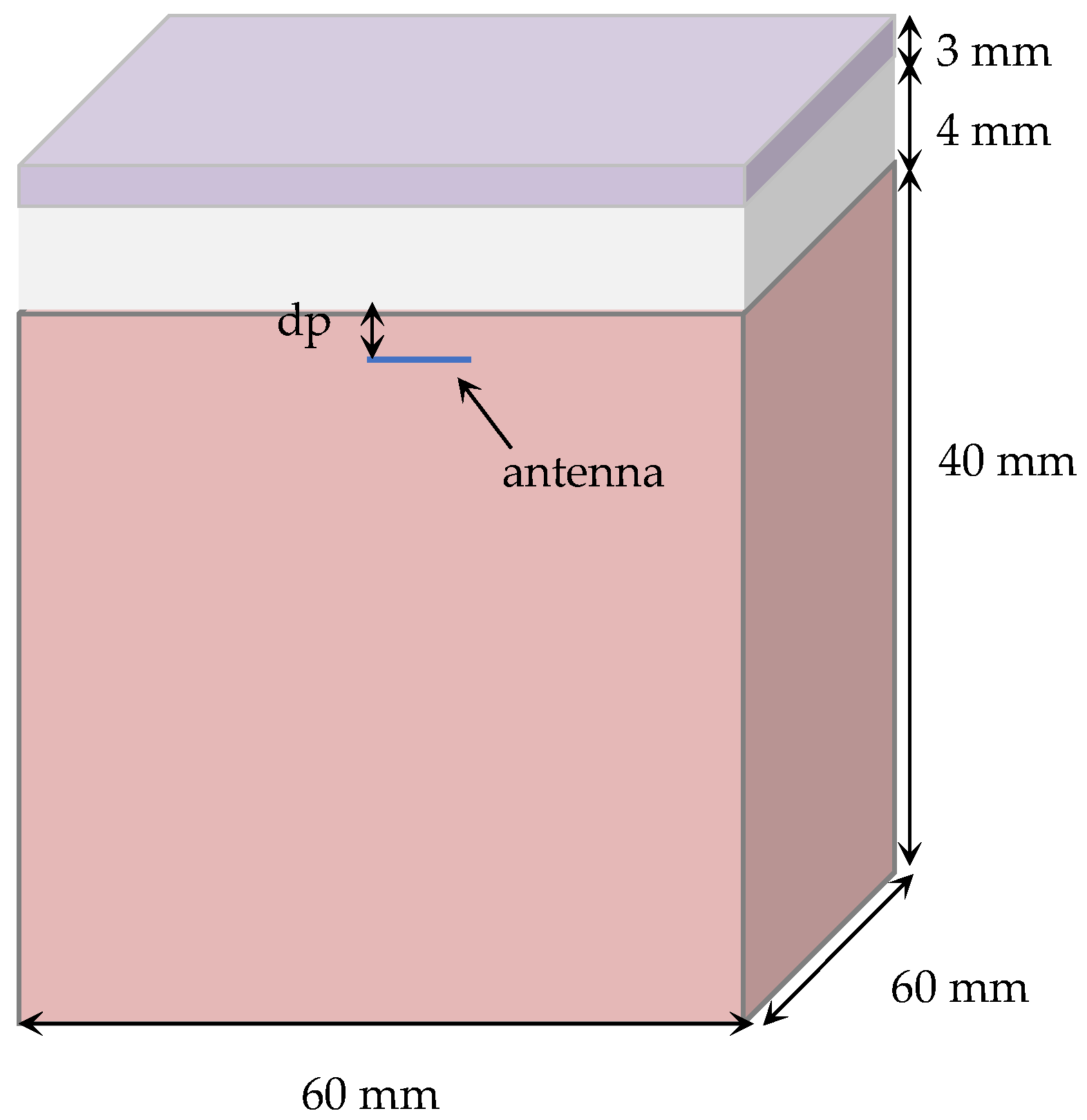
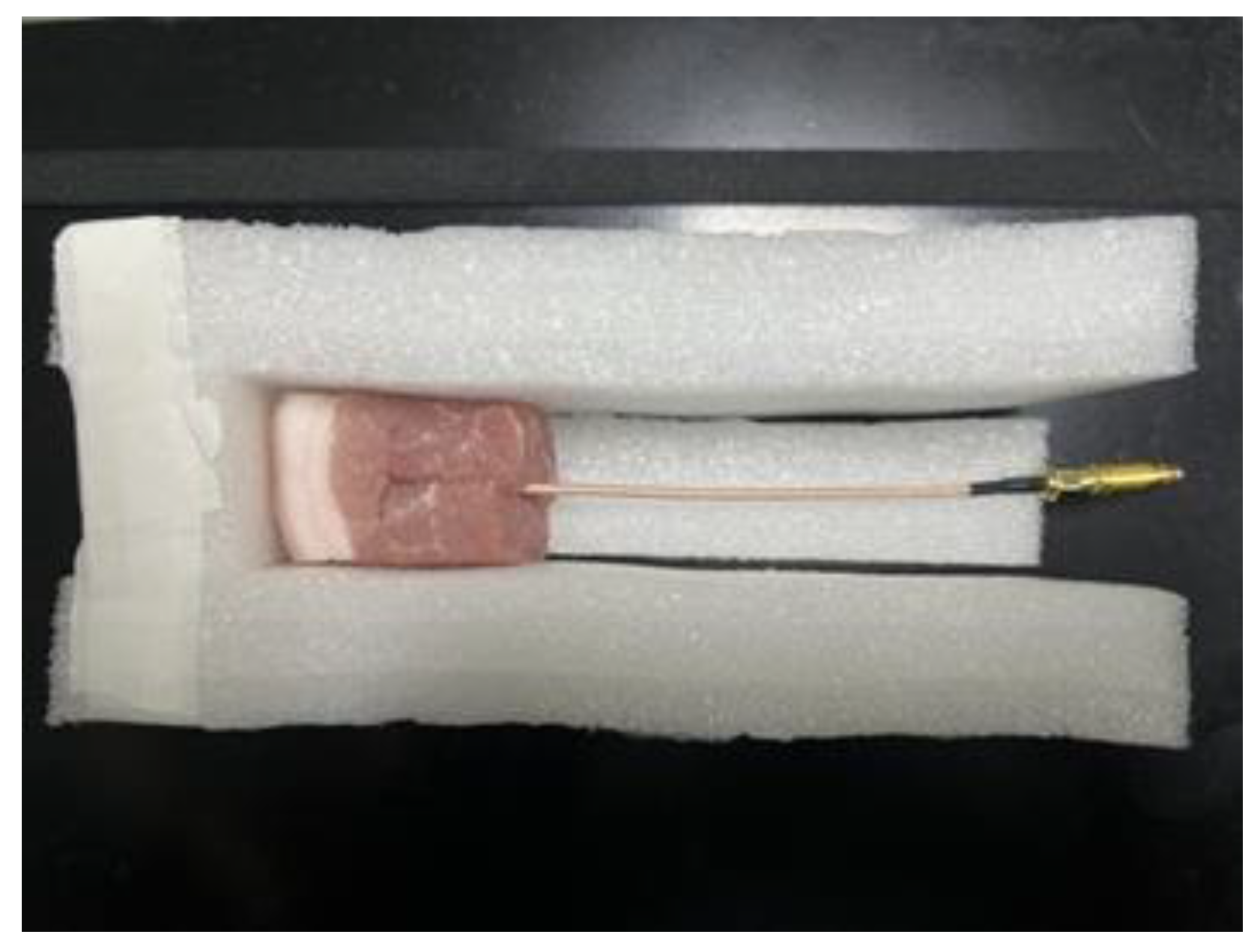
2. Methods
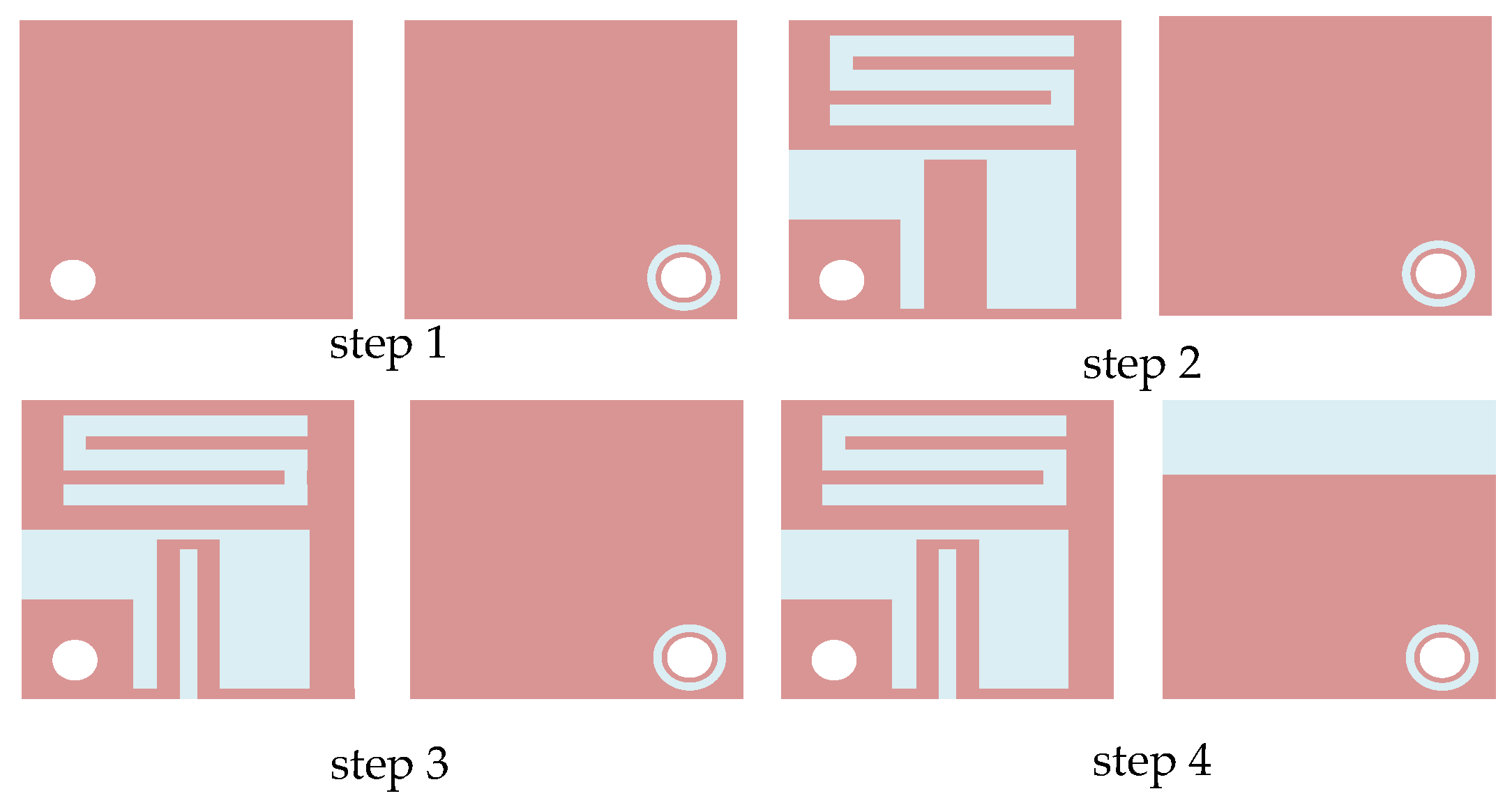
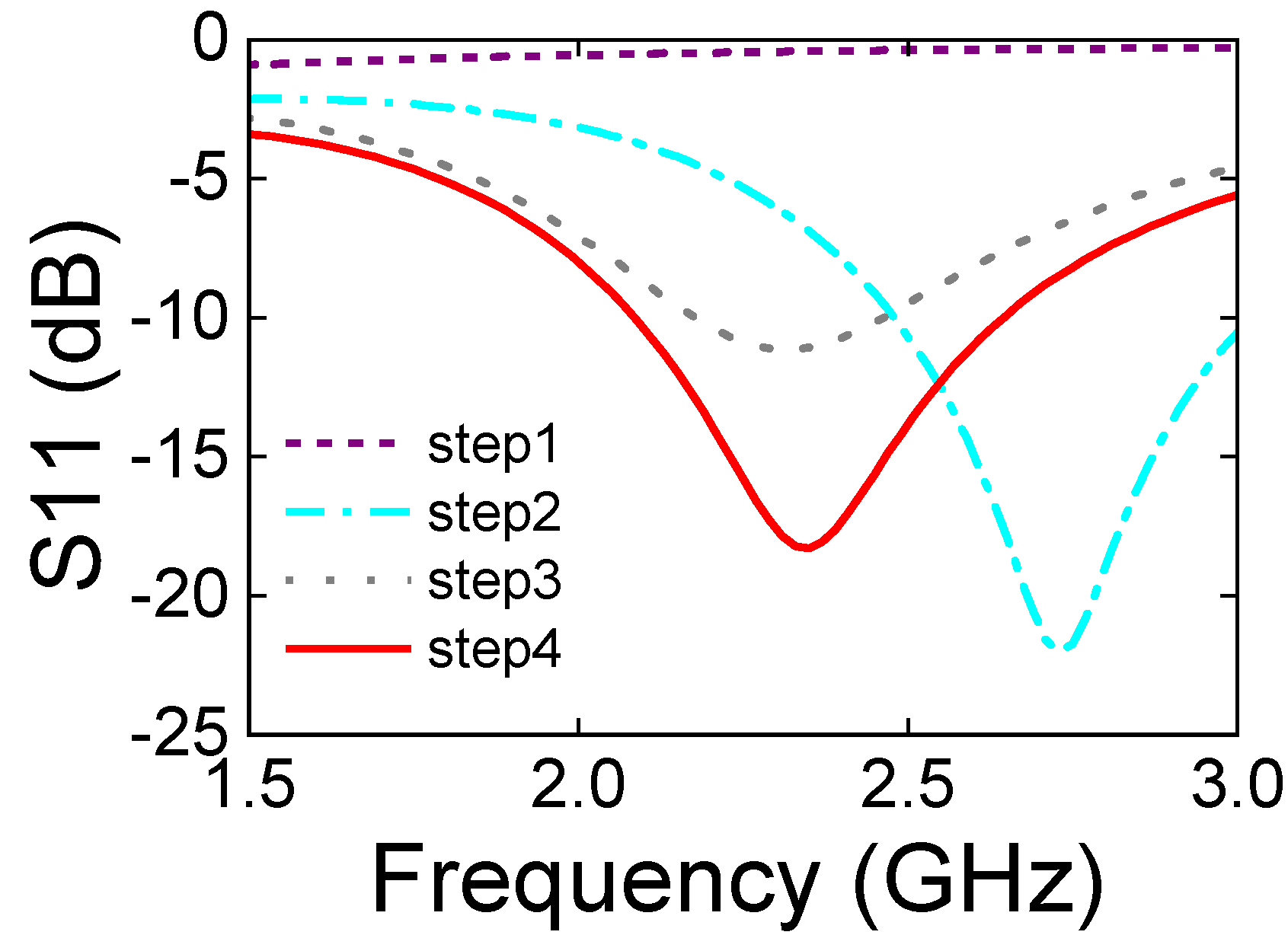
3. Antenna Design and Simulation
3.1. Antenna Structural Design
3.2. Antenna Silicone Layer Design
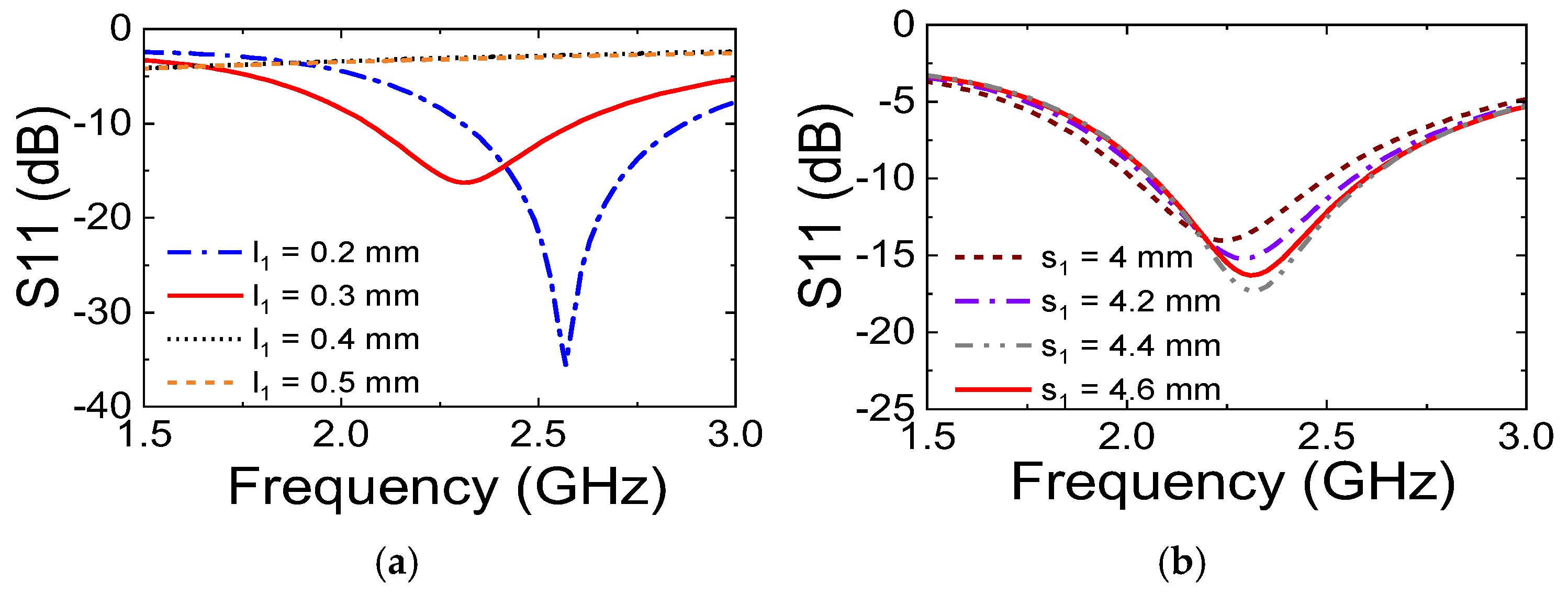
3.3. Antenna Parameter Analysis
4. Discussion
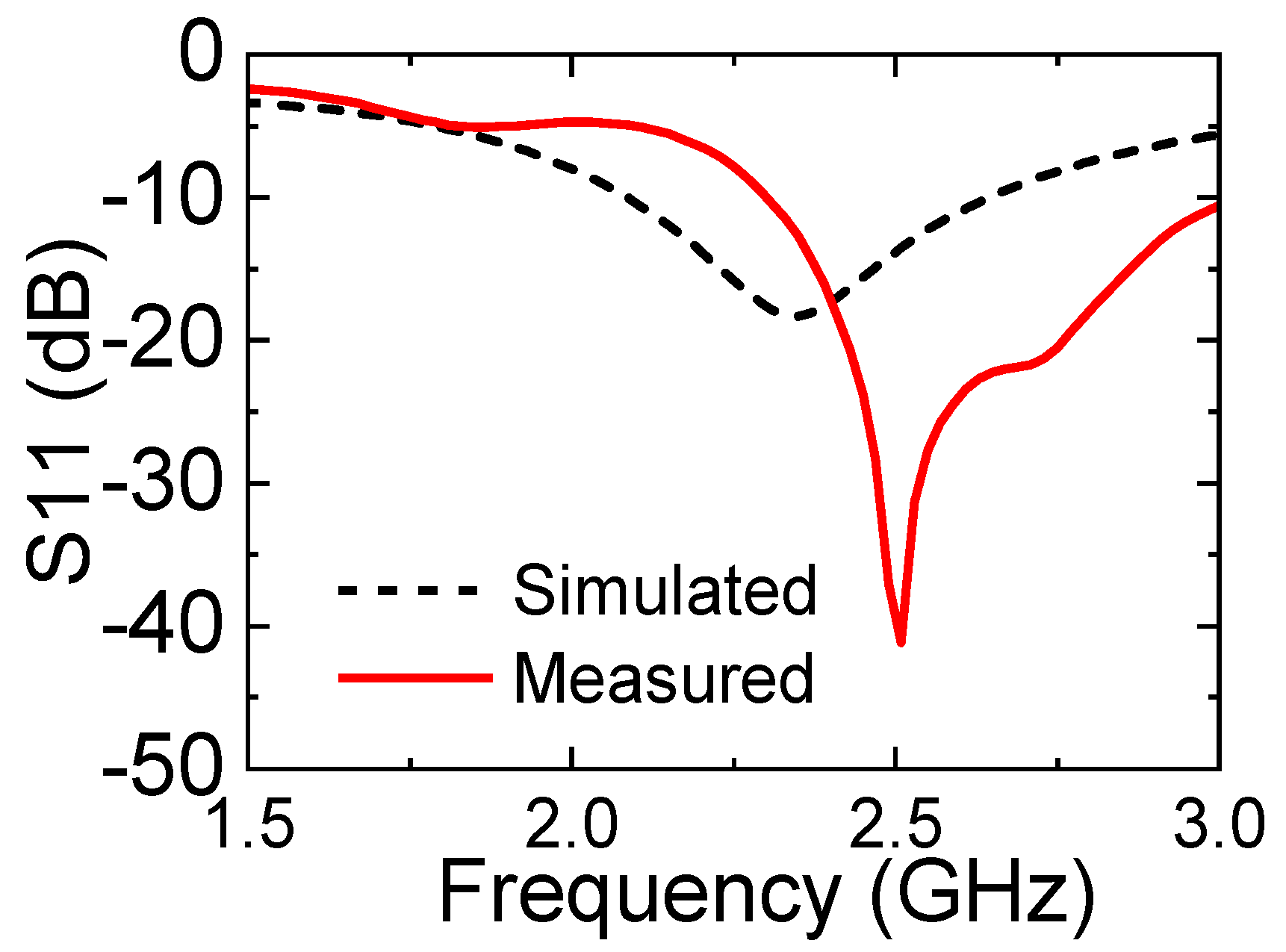
4.1. Reflection Coefficient of the Antenna
4.2. Radiation Direction Map of the Antenna
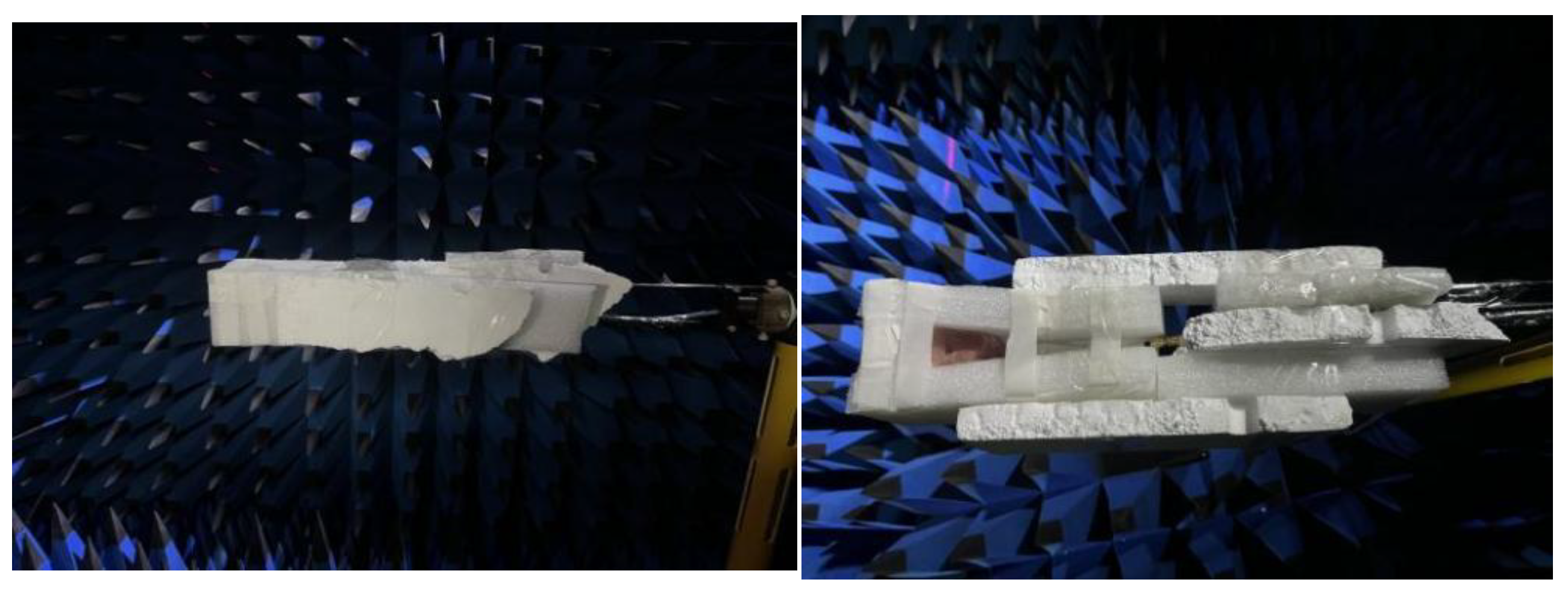
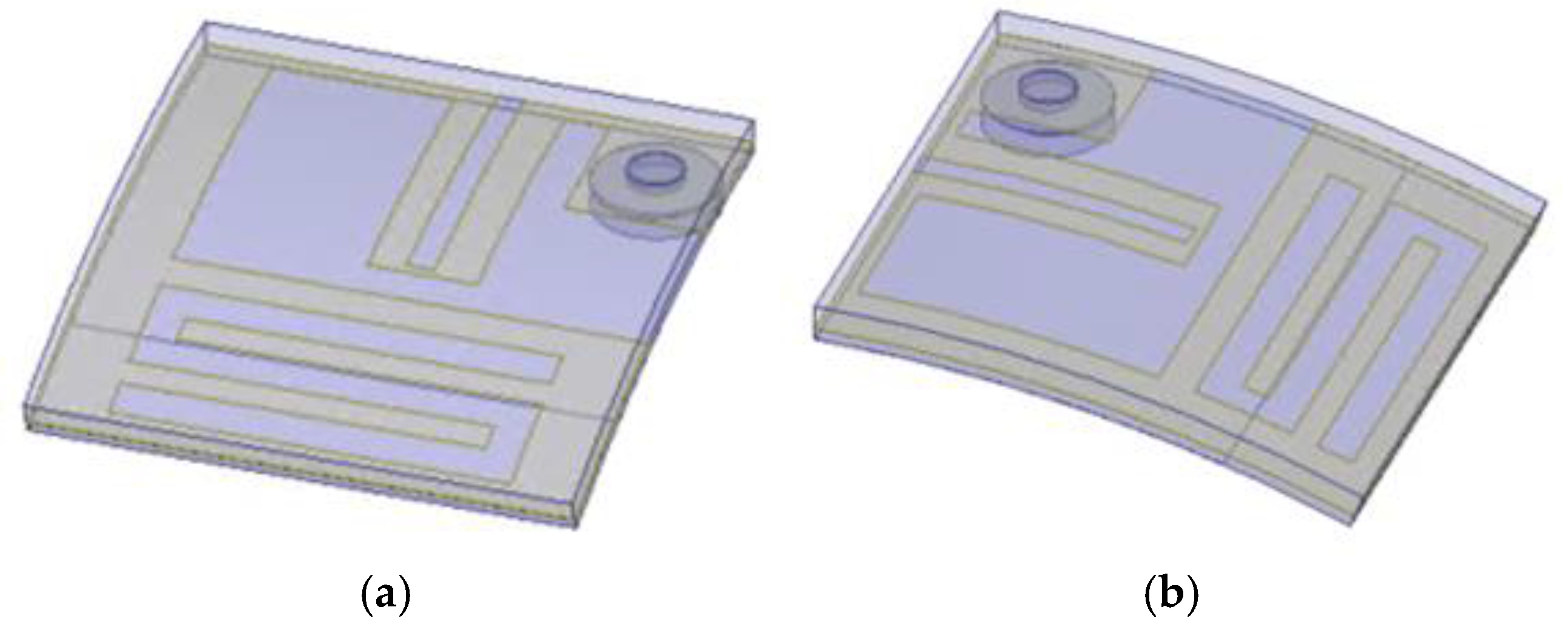
4.3. Antenna Bending Test Setup and Test
4.3.1. Reflection Coefficient Measurement Results
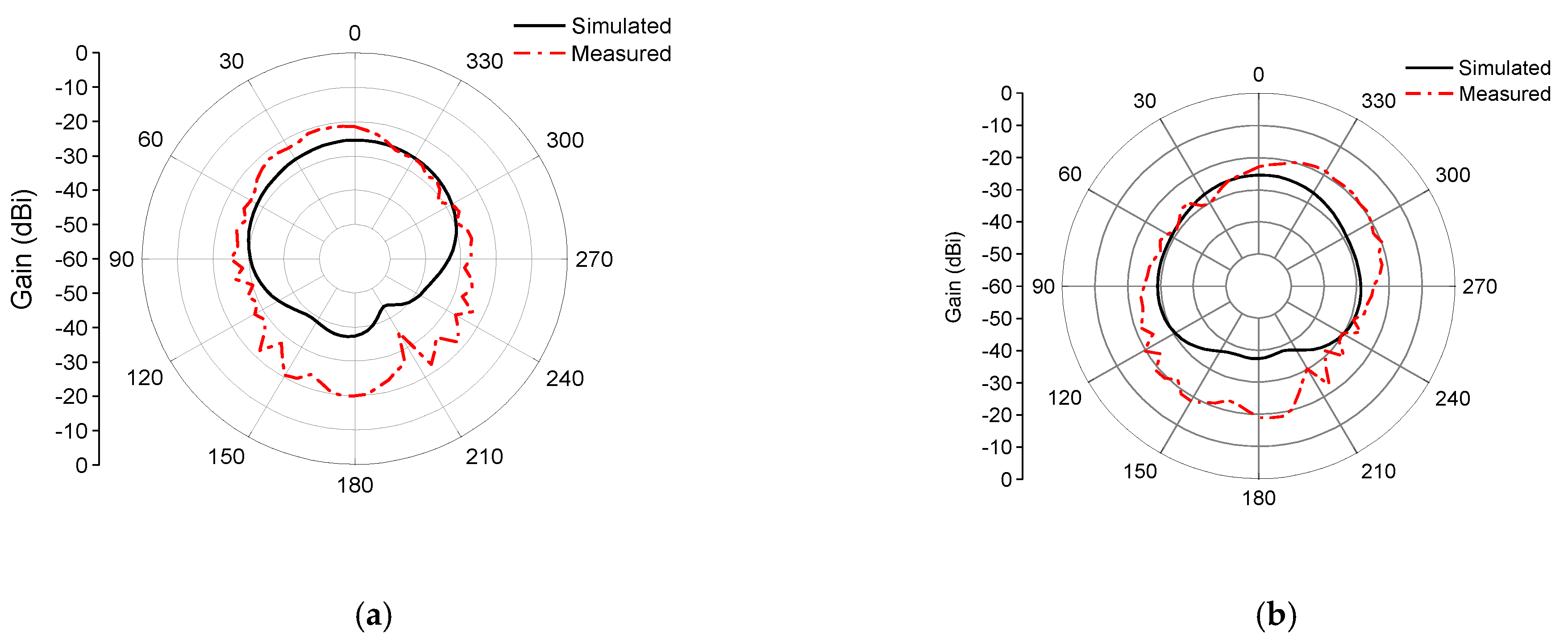
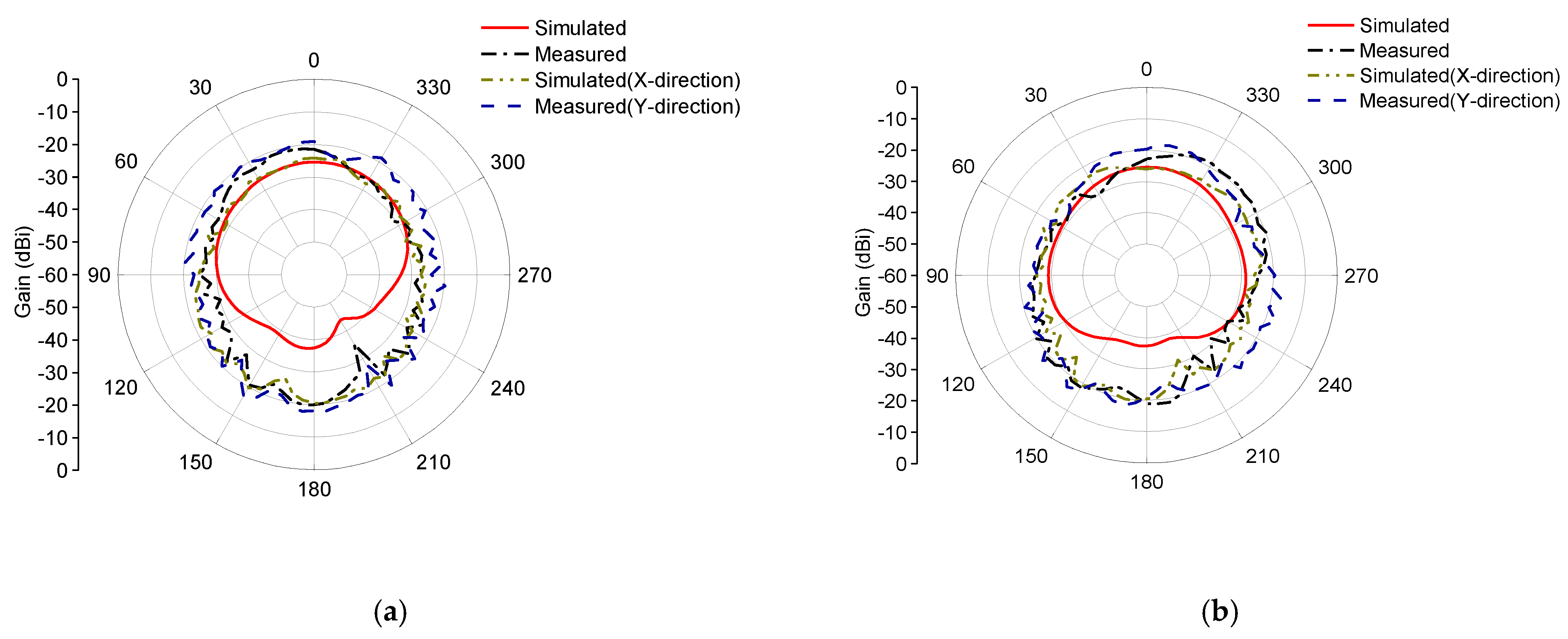
4.3.2. Radiation Direction Map Measurement Results
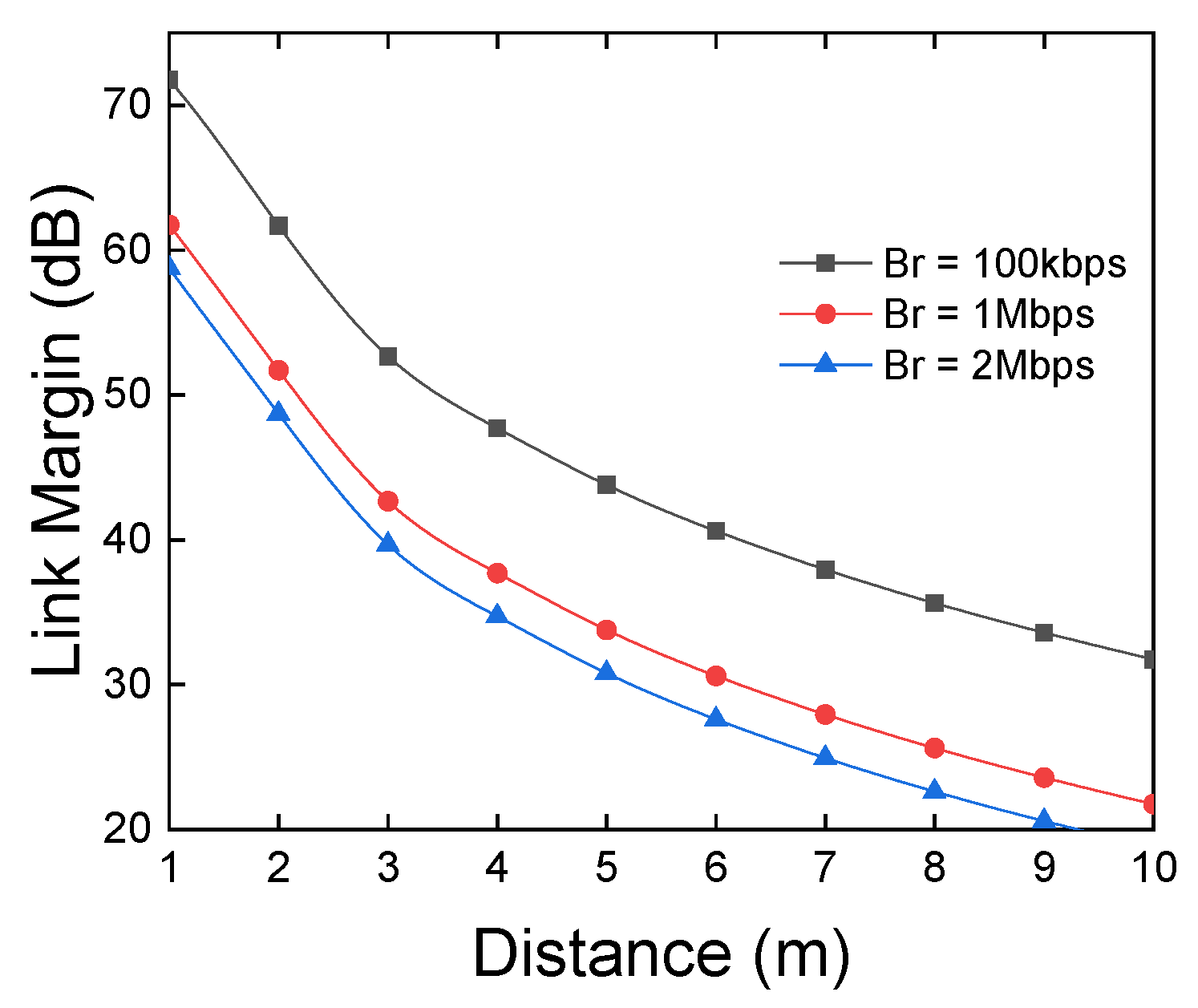
4.4. Wireless Link Budget Analysis
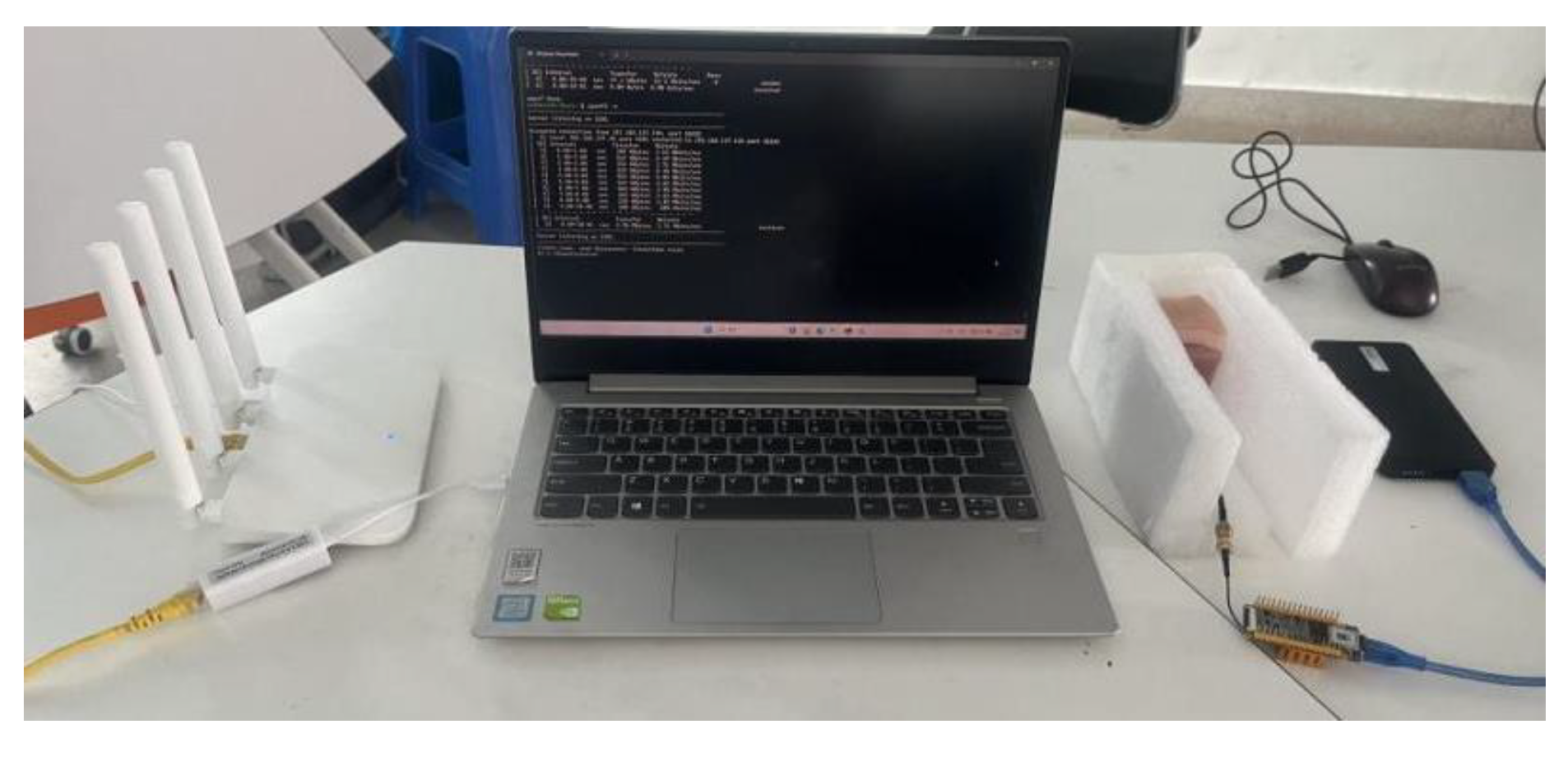
4.5. Wireless Data Transmission Verification
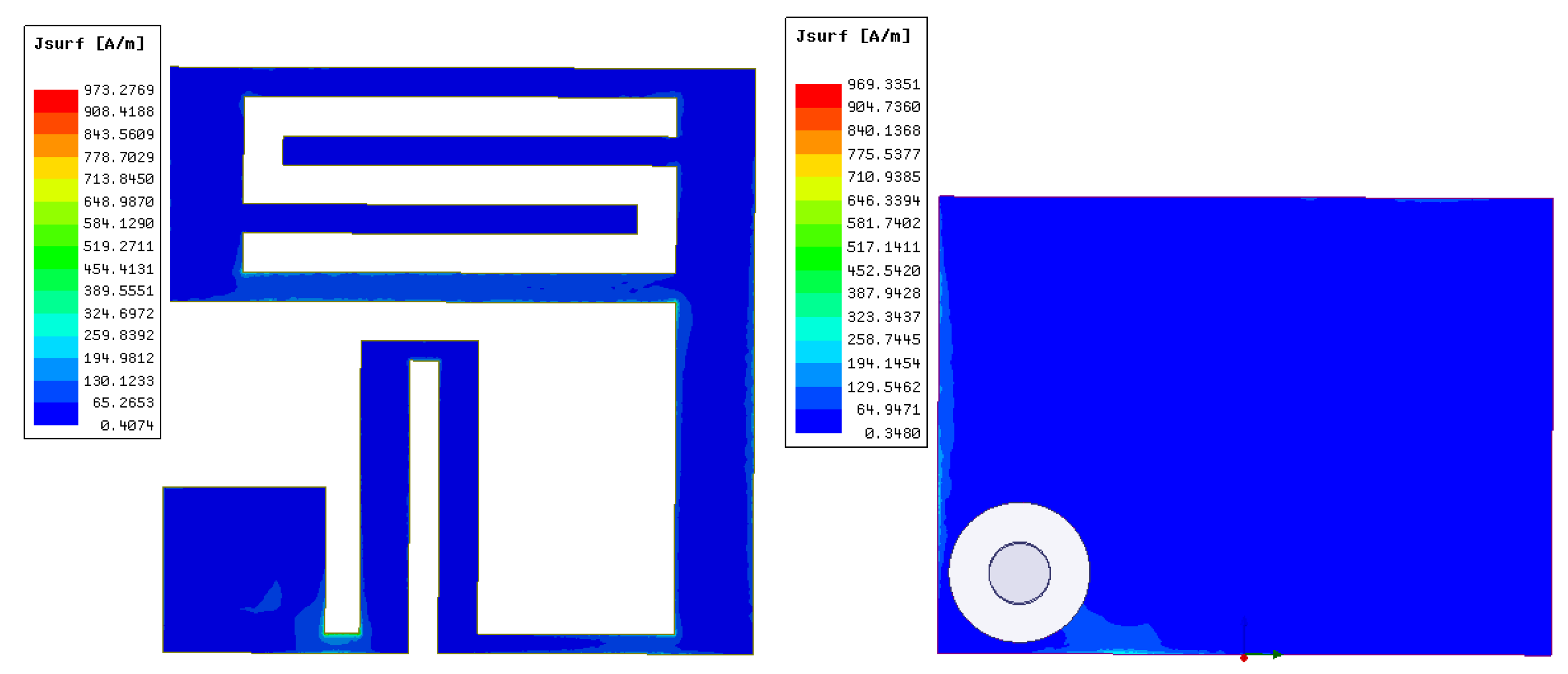
4.6. Antenna Current Distribution and Analysis
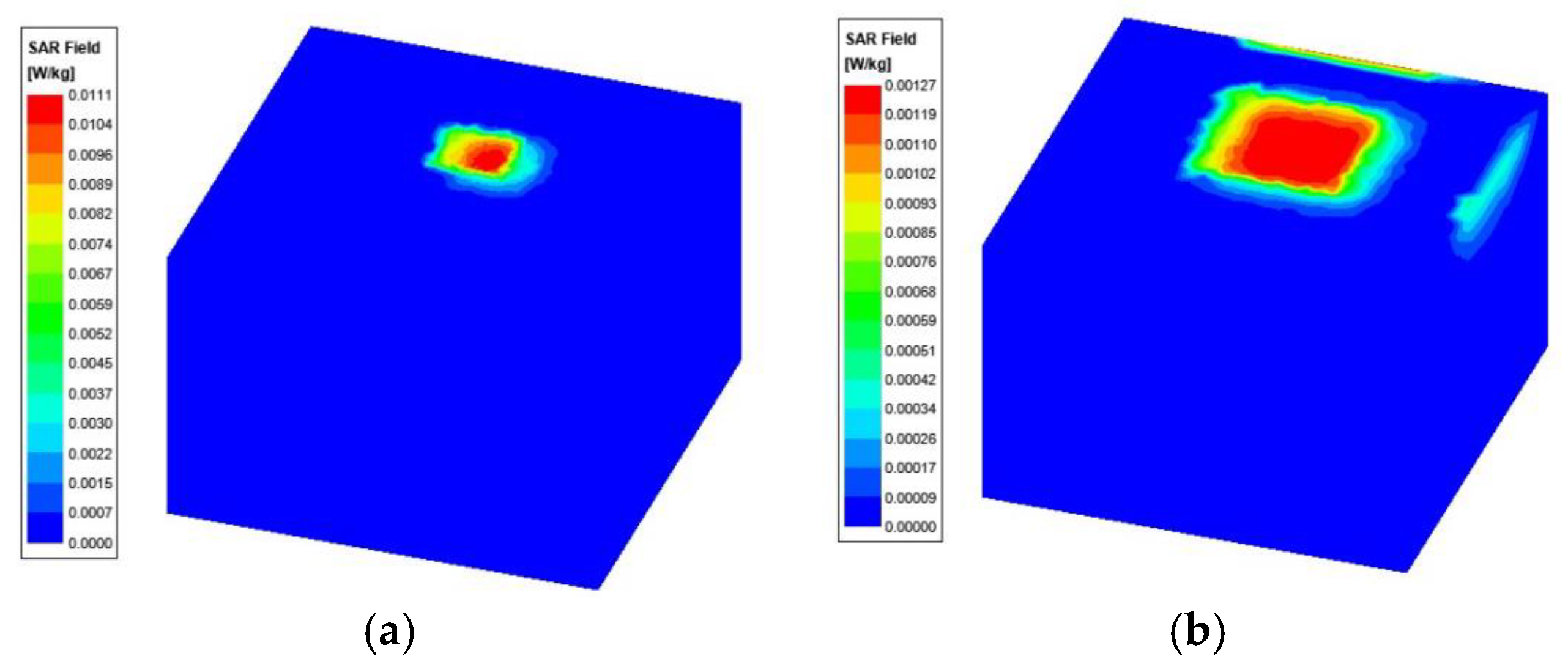
4.7. Specific Absorption Rate (SAR) Measurement and Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Faisal, F.; Zada, M.; Ejaz, A.; Amin, Y.; Ullah, S.; Yoo, H. A Miniaturized Dual-Band Implantable Antenna System for Medical Applications. IEEE Trans. Antennas Propag. 2020, 68, 1161–1165. [Google Scholar] [CrossRef]
- Cornet, B.; Fang, H.; Ngo, H.; Boyer, E.W.; Wang, H.G. An Overview of Wireless Body Area Networks for Mobile Health Applications. IEEE Netw. 2022, 36, 76–82. [Google Scholar] [CrossRef]
- Wang, S.; Deng, W.; Yang, T.; Tian, G.; Xiong, D.; Xiao, X.; Zhang, H.; Sun, Y.; Ao, Y.; Huang, J.; et al. Body-area sensor network featuring micropyramids for sports healthcare. Nano Res. 2022, 16, 1330–1337. [Google Scholar] [CrossRef]
- Sui, Y.; Hou, C.; Wang, Y.; Chung, K.L.; Wei, C.; Li, Z.; Zong, W.-H.; Wang, J. A Tissue-Independent Flexible Antenna With Miniaturized Size for Injectable Implants. IEEE Antennas Wirel. Propag. Lett. 2023, 23, 945–949. [Google Scholar] [CrossRef]
- Magill, M.; Conway, G.A.; Scanlon, W. Tissue-Independent Implantable Antenna for In-Body Communications at 2.36–2.5 GHz. IEEE Trans. Antennas Propag. 2017, 65, 4406–4417. [Google Scholar] [CrossRef]
- Liu, R.-P.; Zhang, K.-L.; Li, Z.-W.; Cui, W.-J.; Liang, W.-B.; Wang, M.-J.; Fan, C.; Zheng, H.-X.; Li, E.P. A Wideband Circular Polarization Implantable Antenna for Health Monitor Microsystem. IEEE Antennas Wirel. Propag. Lett. 2021, 20, 848–852. [Google Scholar] [CrossRef]
- Xia, Z.; Li, H.; Lee, Z.; Xiao, S.; Shao, W.; Ding, X.; Yang, X. A Wideband Circularly Polarized Implantable Patch Antenna for ISM Band Biomedical Applications. IEEE Trans. Antennas Propag. 2020, 68, 2399–2404. [Google Scholar] [CrossRef]
- Zhang, J.; Das, R.; Hoare, D.; Wang, H.; Ofiare, A.; Mirzai, N.; Mercer, J.; Heidari, H. A Compact Dual-Band Implantable Antenna for Wireless Biotelemetry in Arteriovenous Grafts. IEEE Trans. Antennas Propag. 2023, 71, 4759–4771. [Google Scholar] [CrossRef]
- Kamel, A.; Mohamed, A.; Elsadek, H.; ELhennawy, H.M. Miniaturized Triple-Band Circular-Polarized Implantable Patch Antenna for Bio-Telemetry Applications. IEEE Antennas Wirel. Propag. Lett. 2023, 22, 74–78. [Google Scholar] [CrossRef]
- Lamkaddem, A.; El Yousfi, A.; Abdalmalak, K.A.; Posadas, V.G.; Segovia-Vargas, D. Circularly Polarized Miniaturized Implantable Antenna for Leadless Pacemaker Devices. IEEE Trans. Antennas Propag. 2022, 70, 6423–6432. [Google Scholar] [CrossRef]
- Shah, A.; Zada, M.; Nasir, J.; Yoo, H. Ultraminiaturized Triband Antenna with Reduced SAR for Skin and Deep Tissue Implants. IEEE Trans. Antennas Propag. 2022, 70, 8518–8529. [Google Scholar] [CrossRef]
- Mosavinejad, S.; Rezaei, P.; Khazaei, A. A miniaturized and biocompatible dual-band implantable antenna for fully-passive wireless signal monitoring. AEU-Int. J. Electron. Commun. 2022, 154, 154303. [Google Scholar] [CrossRef]
- Hertleer, C.; Rogier, H.; Vallozzi, L.; Van Langenhove, L. A Textile Antenna for Off-Body Communication Integrated Into Protective Clothing for Firefighters. IEEE Trans. Antennas Propag. 2009, 57, 919–925. [Google Scholar] [CrossRef]
- Bait-Suwailam, M.; Alomainy, A. Flexible Analytical Curve-Based Dual-Band Antenna for Wireless Body Area Networks. Prog. Electromagn. Res. M 2019, 84, 73–84. [Google Scholar] [CrossRef]
- Vidhya, S.; Shanthi K, G. Ultra Wideband Flexible Antennas: Design, Performance and Integration for Wireless Body Area Network Applications. Int. J. Microw. Opt. Technol. 2023, 18, 435–443. [Google Scholar]
- Ganeshwaran, N.; Jeyaprakash, J.K.; Alsath, M.G.N.; Sathyanarayanan, V. Design of a Dual-Band Circular Implantable Antenna for Biomedical Applications. IEEE Antennas Wirel. Propag. Lett. 2020, 19, 119–123. [Google Scholar] [CrossRef]
- Green, R.B.; Hays, M.R.; Mangino, M.J.; Topsakal, E. An Anatomical Model for the Simulation and Development of Subcutaneous Implantable Wireless Devices. IEEE Trans. Antennas Propag. 2020, 68, 7170–7178. [Google Scholar] [CrossRef]
- Hayat, S.; Shah, A.; Yoo, H. Miniaturized Dual-Band Circularly Polarized Implantable Antenna for Capsule Endoscopic System. IEEE Trans. Antennas Propag. 2021, 69, 1885–1895. [Google Scholar] [CrossRef]
- Iqbal, A.; Al-Hasan, M.; Ben Mabrouk, I.; Basir, A.; Nedil, M.; Yoo, H. Biotelemetry and Wireless Powering of Biomedical Implants Using a Rectifier Integrated Self-Diplexing Implantable Antenna. IEEE Trans. Microw. Theory Tech. 2021, 69, 3438–3451. [Google Scholar] [CrossRef]
- Kaim, V.; Singh, N.; Kanaujia, B.K.; Matekovits, L.; Esselle, K.P.; Rambabu, K. Multi-Channel Implantable Cubic Rectenna MIMO System with CP Diversity in Orthogonal Space for Enhanced Wireless Power Transfer in Biotelemetry. IEEE Trans. Antennas Propag. 2023, 71, 200–214. [Google Scholar] [CrossRef]
- Iqbal, A.; Al-Hasan, M.; Ben Mabrouk, I.; Denidni, T.A. Self-Quadruplexing Antenna for Scalp-Implantable Devices. IEEE Transactions on Antennas and Devices. IEEE Trans. Antennas Propag. 2024, 72, 2252–2260. [Google Scholar] [CrossRef]
- Yousaf, M.; Ben Mabrouk, I.; Zada, M.; Akram, A.; Amin, Y.; Nedil, M.; Yoo, H. An Ultra-Miniaturized Antenna with Ultra-Wide Bandwidth Characteristics for Medical Implant Systems. IEEE Access 2021, 9, 40086–40097. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue | Relative Dielectric Constant () | Relative Permeability (S/m)] | Loss Angle Tangent |
|---|---|---|---|
| Skin | 38.1 | 1.43 | 0.283 |
| Fat | 5.28 | 0.1 | 0.145 |
| Muscle | 52.7 | 1.74 | 0.242 |
| Parameter | Size (mm) | Parameter | Size (mm) | Parameter | Size (mm) |
|---|---|---|---|---|---|
| W | 6 | s1 | 4.4 | s7 | 0.2 |
| L | 6 | s2 | 0.4 | s8 | 0.3 |
| G | 4.5 | s3 | 2 | s9 | 2.8 |
| l1 | 0.3 | s4 | 1.5 | s10 | 2 |
| h | 0.13 | s5 | 0.5 | s11 | 3 |
| h1 | 0.4 | s6 | 3 | r | 0.3 |
| Parameters | Variable | Value |
|---|---|---|
| Frequency | (GHz) | 2.45 |
| Transmitter power | −16 | |
| Transmitter antenna gain | −23.8 | |
| Receiver antenna gain | 3 | |
| Distance | 1–10 | |
| Temperature | 273 | |
| Noise power density | 203.93 | |
| Ideal-BPSK | 9.6 | |
| Free space path loss | Distance dependent | |
| Available power | Distance dependent | |
| Required power | Adaptive (bitrate) |
| Reference | Year | Size | Relative Bandwidth (MHz) | 1 g SAR (W/kg) |
|---|---|---|---|---|
| [17] | 2020 | 18.74 mm × 16 mm × 2.4 mm | 4.4% | - |
| [22] | 2021 | 5 mm × 5 mm × 0.528 mm | 3.3% | 340.42 |
| [12] | 2022 | 8.5 mm × 8.5 mm × 1.27 mm | 3.5% | 207 |
| [20] | 2023 | 15 mm × 15 mm | 32.6% | 324.4 |
| [8] | 2023 | 5 mm × 5 mm× 0.635 mm | 15.5% | 785 |
| [21] | 2024 | 12 mm× 14.5 mm × 0.13 mm | 1.4% | - |
| This paper | 6 mm × 6 mm × 0.53 mm | 28% | 260.68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gan, Z.; Wang, D.; Liu, L.; Fu, X.; Wang, X.; Chen, P. A Small Implantable Compact Antenna for Wireless Telemetry Applied to Wireless Body Area Networks. Appl. Sci. 2025, 15, 1385. https://doi.org/10.3390/app15031385
Gan Z, Wang D, Liu L, Fu X, Wang X, Chen P. A Small Implantable Compact Antenna for Wireless Telemetry Applied to Wireless Body Area Networks. Applied Sciences. 2025; 15(3):1385. https://doi.org/10.3390/app15031385
Chicago/Turabian StyleGan, Zongsheng, Dan Wang, Lu Liu, Xiaofeng Fu, Xinju Wang, and Peng Chen. 2025. "A Small Implantable Compact Antenna for Wireless Telemetry Applied to Wireless Body Area Networks" Applied Sciences 15, no. 3: 1385. https://doi.org/10.3390/app15031385
APA StyleGan, Z., Wang, D., Liu, L., Fu, X., Wang, X., & Chen, P. (2025). A Small Implantable Compact Antenna for Wireless Telemetry Applied to Wireless Body Area Networks. Applied Sciences, 15(3), 1385. https://doi.org/10.3390/app15031385