

Strength Training vs. Aerobic Interval Training: Effects on Anaerobic Capacity, Aerobic Power and Second Ventilatory Threshold in Men


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Somatic Measurements
2.3. Physical Activity
2.4. Anaerobic Capacity
2.5. Aerobic Capacity and Second Ventilatory Threshold
2.6. Strength Training
2.7. Aerobic Interval Training
2.8. Statistical Analysis
3. Results
3.1. Physical Activity
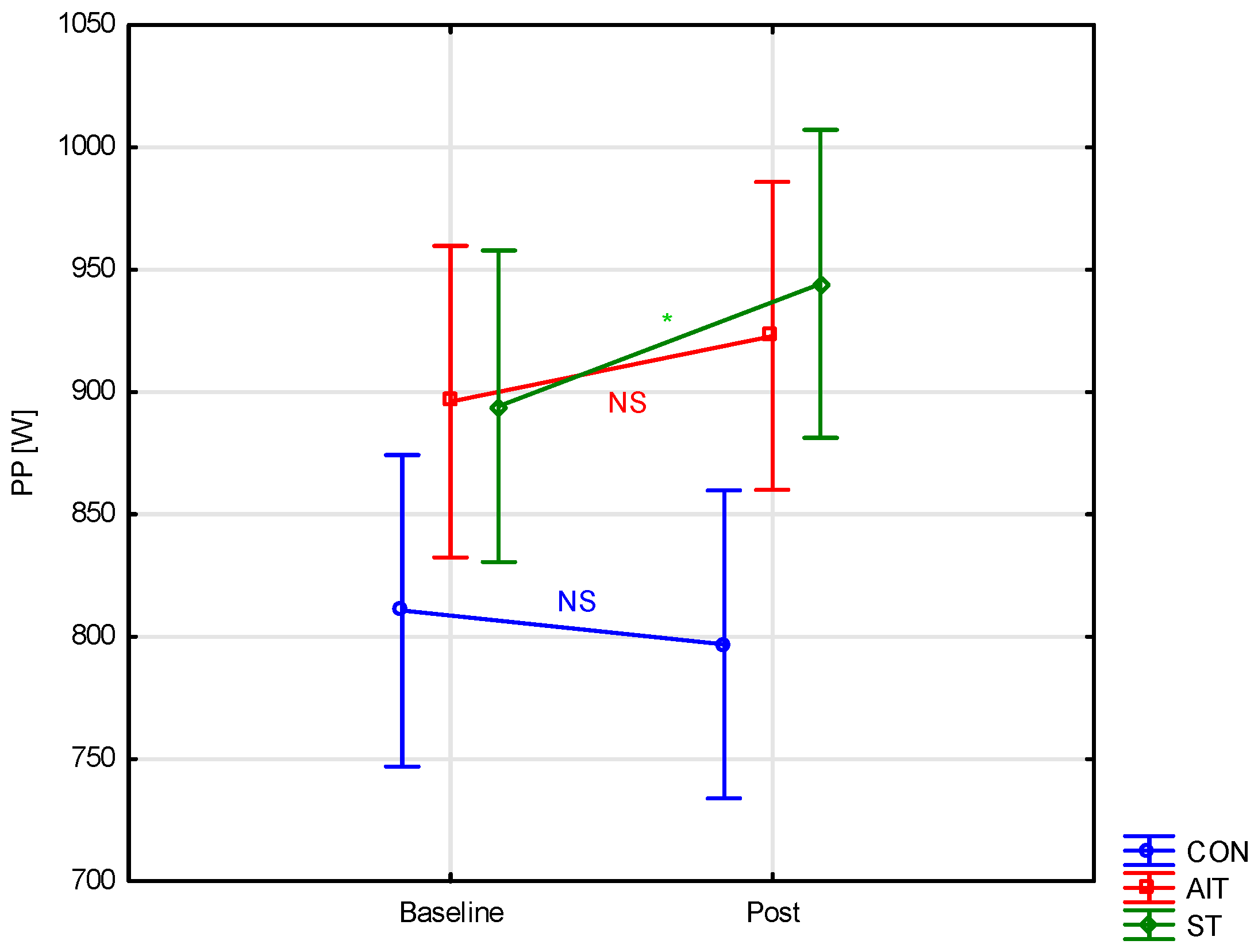
3.2. Anaerobic Capacity
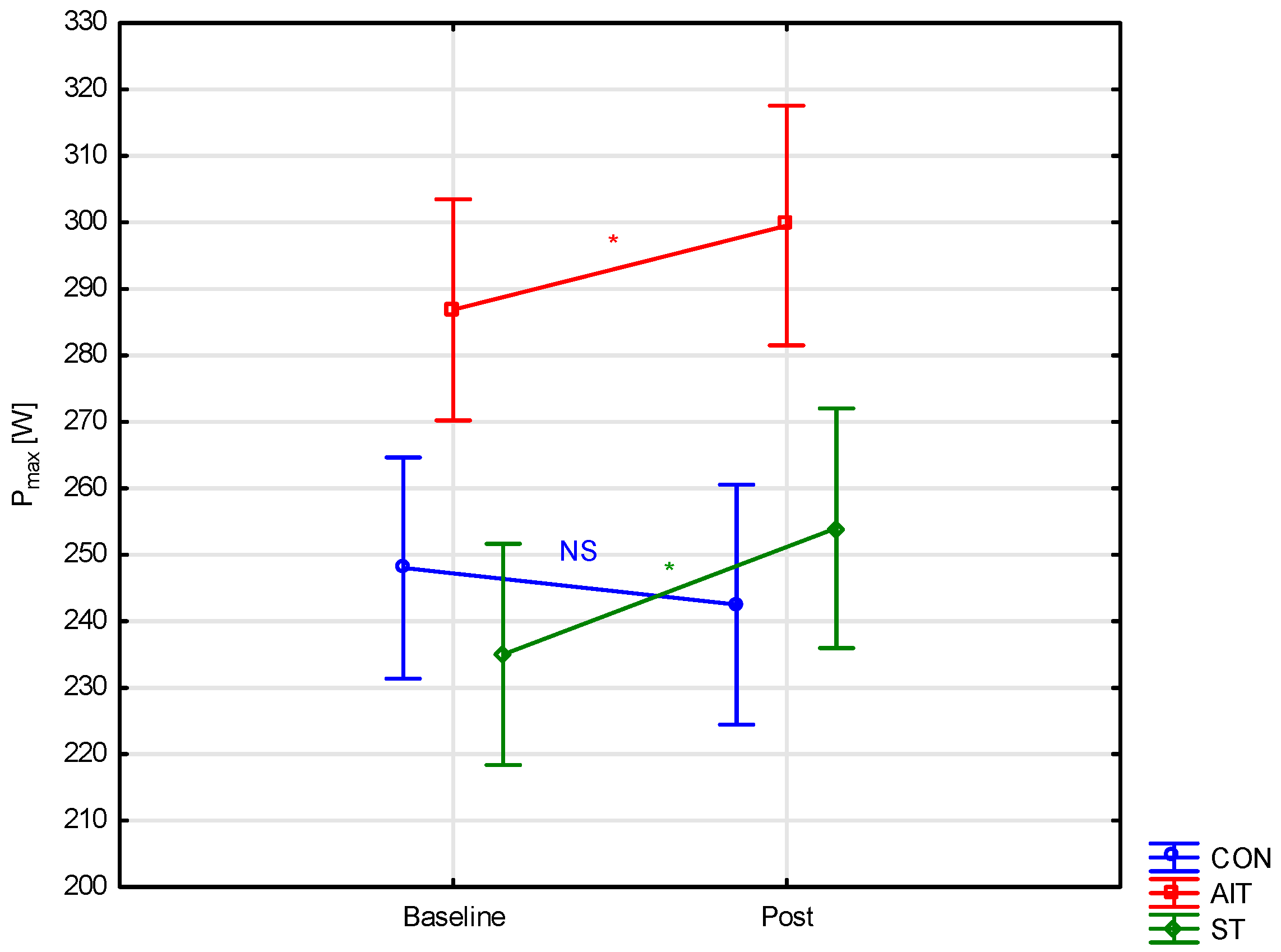
3.3. Aerobic Capacity and Second Ventilatory Threshold
4. Discussion
Limitation of the Study, Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ST | strength training |
| AIT | aerobic interval training |
| CON | control group |
| PP | peak power |
| MP | mean power |
| FI | fatigue index |
| Pmax | maximal power |
| VO2max | maximal oxygen uptake |
| HRmax | maximal heart rate |
| RER | respiratory exchange ratio |
| VT | ventilatory threshold |
References
- Gastin, P.B. Quantification of anaerobic capacity. Scand. J. Med. Sci. Sports 1994, 4, 91–112. [Google Scholar] [CrossRef]
- Sözen, H. The effects of aerobic and anaerobic training on aerobic and anaerobic capacity. J. Int. Anatolia Sport Sci. 2018, 3, 331–337. [Google Scholar] [CrossRef]
- Aagaard, P. Training-induced changes in neural function. Exerc. Sport Sci. Rev. 2003, 31, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Conwit, R.A.; Stashuk, D.; Tracy, B.; McHugh, M.; Brown, W.F.; Metter, E.J. The relationship of motor unit size, firing rate and force. Clin. Neurophysiol. 1999, 110, 1270–1275. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.J.; Bishop, P.A.; Woods, A.K.; Green, J.M. Cross-sectional area and muscular strength: A brief review. Sports Med. 2008, 38, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, W.J.; Patton, J.F.; Gordon, S.E.; Harman, E.A.; Deschenes, M.R.; Reynolds, K.; Dziados, J.E. Compatibility of high-intensity strength and endurance training on hormonal and skeletal muscle adaptations. J. Appl. Physiol. 1995, 78, 976–989. [Google Scholar] [CrossRef] [PubMed]
- Sporiš, G.; Jovanović, M.; Krakan, I.; Fiorentini, F. Effects of strength training on aerobic and anaerobic power in female soccer players. Sport Sci. 2011, 4, 32–37. [Google Scholar]
- Vikmoen, O.; Ellefsen, S.; Trøen, Ø.; Hollan, I.; Hanestadhaugen, M.; Raastad, T.; Rønnestad, B. Strength training improves cycling performance, fractional utilization of VO2max and cycling economy in female cyclists. Scand. J. Med. Sci. Sports 2016, 26, 384–396. [Google Scholar] [CrossRef] [PubMed]
- Hoff, J.; Gran, A.; Helgerud, J. Maximal strength training improves aerobic endurance performance. Scand. J. Med. Sci. Sports 2002, 12, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Loveless, D.J.; Weber, C.L.; Haseler, L.J.; Schneider, D.A. Maximal leg-strength training improves cycling economy in previously untrained men. Med. Sci. Sports Exerc. 2005, 37, 1231–1236. [Google Scholar] [CrossRef] [PubMed]
- Østerås, H.; Helgerud, J.; Hoff, J. Maximal strength-training effects on force-velocity and force-power relationships explain increases in aerobic performance in humans. Eur. J. Appl. Physiol. 2002, 88, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Rønnestad, B.R.; Hansen, J.; Hollan, I.; Ellefsen, S. Strength training improves performance and pedaling characteristics in elite cyclists. Scand. J. Med. Sci. Sports 2015, 25, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Støren, Ø.; Helgerud, J.N.; Støa, E.M.; Hoff, J.N. Maximal strength training improves running economy in distance runners. Med. Sci. Sports Exerc. 2008, 40, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Finni, T.; Sedliak, M.; Zhou, W.; Alen, M.; Cheng, S. Seasonal variation of red blood cell variables in physically inactive men: Effects of strength training. Int. J. Sports Med. 2008, 29, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Schjerve, I.E.; Tyldum, G.A.; Tjønna, A.E.; Stølen, T.; Loennechen, J.P.; Hansen, H.E.; Wisløff, U. Both aerobic endurance and strength training programmes improve cardiovascular health in obese adults. Clin. Sci. 2008, 115, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Beneke, R. Methodological aspects of maximal lactate steady state implications for performance testing. Eur. J. Appl. Physiol. 2003, 89, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Coyle, E.F. Integration of the physiological factors determining endurance performance ability. Exerc. Sport Sci. Rev. 1995, 23, 25–64. [Google Scholar] [CrossRef] [PubMed]
- Mahood, N.V.; Kenefick, R.W.; Kertzer, R.; Quinn, T.J. Physiological determinants of cross-country ski racing performance. Med. Sci. Sports Exerc. 2001, 33, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, K.; Beaver, W.L.; Whipp, B.J. Gas exchange theory and the lactic acidosis (anaerobic) threshold. Circulation 1990, 81, 14–30. [Google Scholar]
- Maciejczyk, M.; Szymura, J.; Cempla, J.; Gradek, J.; Więcek, M.; Bawelski, M. Respiratory compensation point during incremental test in overweight and normoweight boys: Is it useful in assessing aerobic performance? A longitudinal study. Clin. Physiol. Funct. Imaging 2014, 34, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Maciejczyk, M.; Wiecek, M.; Szymura, J.; Cempla, J.; Wiecha, S.; Szygula, Z.; Brown, L.E. Effect of body composition on respiratory compensation point during an incremental test. J. Strength Cond. Res. 2014, 28, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Meyer, T.; Faude, O.; Scharhag, J.; Urhausen, A.; Kindermann, W. Is lactic acidosis a cause of exercise induced hyperventilation at the respiratory compensation point? Br. J. Sports Med. 2004, 38, 622–625. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N.; Haskell, W.L.; Ho, P.; Paffenbarger, J.R.R.S.; Vranizan, K.M.; Farquhar, J.W.; Wood, P.D. Assessment of habitual physical activity by a Seven-Day recall in a community survey and controlled experiments. Am. J. Epidemiol. 1985, 122, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Sarkin, J.; Campbell, J.; Gross, L.; Roby, J.; Bazzo, S.; Sallis, J.; Calfas, K. Sevenday physical activity recall. Med. Sci. Sports Excerc. 1997, 29, 89–103. [Google Scholar]
- Inbar, O.; Bar-Or, O. Anaerobic characteristics in male children and adolescents. Med. Sci. Sports Excerc. 1986, 18, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.G.S.; Hale, T.; Hamley, E.J. A comparison of power outputs with rolling and stationary starts in the Wingate Anaerobic Test. J. Sports Sci. 1985, 3, 207. [Google Scholar]
- Howley, E.T.; Bassett, D.R.; Welch, H.G. Criteria for maximal oxygen uptake: Review and commentary. Med. Sci. Sports Excerc. 1995, 27, 1292–1301. [Google Scholar] [CrossRef]
- Bhambhani, Y.; Singh, M. Ventilatory thresholds during a graded exercise test. Respiration 1985, 47, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Binder, R.K.; Wonisch, M.; Corra, U.; Cohen-Solal, A.; Vanhees, L.; Saner, H. Methodological approach to the firstand second lactate threshold in incremental cardiopulmonaryexercise testing. Eur. J. Prev. Cardiol. 2008, 15, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, J.M.; Triplett, N.T.; Haf, G.G.; Triplett, N.T. Essentials of Strength Training and Conditioning. Strength Cond. J. 2016, 4, 452. [Google Scholar]
- Cohen, J. Statistical power analysis for the behavioral sciences. Routledge 2013, 58–59. [Google Scholar]
- Maté-Muñoz, J.L.; Domínguez, R.; Lougedo, J.H.; Garnacho-Castaño, M.V. The lactate and ventilatory thresholds in resistance training. Clin. Physiol. Funct. Imaging 2017, 37, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Sunde, A.; Støren, Ø.; Bjerkaas, M.; Larsen, M.H.; Hoff, J.; Helgerud, J. Maximal strength training improves cycling economy in competitive cyclists. J. Strength Cond. Res. 2010, 24, 2157–2165. [Google Scholar] [CrossRef] [PubMed]
- Nakao, M.; Inoue, Y.; Murakami, H. Longitudinal study of the effect of high intensity weight training on aerobic capacity. Eur. J. Appl. Physiol. Occup. Physiol. 1995, 70, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Cantrell, G.S.; Schilling, B.K.; Paquette, M.R.; Murlasits, Z. Maximal strength, power, and aerobic endurance adaptations to concurrent strength and sprint interval training. Eur. J. Appl. Physiol. 2014, 114, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Heggelund, J.; Fimland, M.S.; Helgerud, J.; Hoff, J. Maximal strength training improves work economy, rate of force development and maximal strength more than conventional strength training. Eur. J. Appl. Physiol. 2013, 113, 1565–1573. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Mean ± SD |
|---|---|---|
| Age [yrs] | CON | 22.8 ± 1.7 |
| ST | 22.4 ± 3.2 | |
| AIT | 20.6 ± 1 | |
| BH [cm] | CON | 178.1 ± 7.1 |
| ST | 179.7 ± 4.3 | |
| AIT | 180 ± 5.7 | |
| BM [kg] | CON | 73.3 ± 9.2 |
| ST | 82.9 ± 8.3 | |
| AIT | 77 ± 8.6 | |
| LBM [kg] | CON | 60.2 ± 6.4 |
| ST | 66 ± 6.8 | |
| AIT | 63.4 ± 6.1 | |
| FM [kg] | CON | 13.1 ± 4.3 |
| ST | 16.9 ± 4.5 | |
| AIT | 13.6 ± 4.1 | |
| FM [%] | CON | 17.6 ± 4.3 |
| ST | 20.3 ± 4.5 | |
| AIT | 17.4 ± 3.9 | |
| BMI [kg/m2] | CON | 23.1 ± 2.1 |
| ST | 25.6 ± 2.1 | |
| AIT | 23.7 ± 2.2 |
| Week | Training | Exercise | Volume (Series × Reps) | Intensity [%1RM] | Pace (s) | Recovery Time (s) |
|---|---|---|---|---|---|---|
| I | I | 1. Barbell squat | 5 × 5 | 70% | 3/0/1/0 | 180 s |
| 2. Push press | 3 × 5 | 70% | 3/0/1/0 | 180 s | ||
| 3. Hip thrust | 3 × 5 | 70% | 3/0/1/0 | 180 s | ||
| 4. Nordic curl | 3 × 3 | Body mass | 4/0/1/0 | 180 s | ||
| II | 1. Deadlift | 3 × 5 | 70% | 3/1/1/0 | 180 s | |
| 2. Bulgarian squat | 3 × 5 | 70% | 3/0/1/0 | 180 s | ||
| 3. Calf raise on leg press machine | 3 × 5 | 70% | 3/0/1/0 | 180 s | ||
| 4. Abs wheel | 3 × 5 | Body mass | 3/0/1/0 | 180 s | ||
| III | 1. Barbell squat | 3 × 5 | 70% | 1/2/1/0 | 180 s | |
| 2. Push press | 3 × 5 | 70% | 1/0/1/0 | 180 s | ||
| 3. Hip thrust | 3 × 5 | 70% | 1/0/1/2 | 180 s | ||
| 4. Nordic curl | 3 × 3 | Body mass | 4/0/1/0 | 180 s | ||
| II | IV | 1. Barbell squat | 3 × 5 | 80% | 3/0/1/0 | 240 s |
| 2. Push press | 3 × 5 | 80% | 3/0/1/0 | 240 s | ||
| 3. Hip thrust | 3 × 5 | 80% | 3/0/1/0 | 240 s | ||
| 4. Nordic curl | 3 × 3 | Body mass | 4/0/1/0 | 180 s | ||
| V | 1. Deadlift | 3 × 5 | 80% | 3/1/1/0 | 240 s | |
| 2. Bulgarian squat | 3 × 5 | 80% | 1/0/1/0 | 240 s | ||
| 3. Calf raise on leg press machine | 3 × 5 | 80% | 3/0/1/0 | 180 s | ||
| 4. Abs wheel | 3 × 5 | Body mass | 1/0/1/2 | 180 s | ||
| VI | 1. Barbell squat | 3 × 5 | 80% | 1/2/1/0 | 240 s | |
| 2. Push press | 3 × 5 | 80% | 1/0/1/0 | 240 s | ||
| 3. Hip thrust | 3 × 5 | 80% | 1/0/1/2 | 240 s | ||
| 4. Nordic curl | 3 × 3 | Body mass | 3/0/1/0 | 180 s | ||
| III | VII | 1. Barbell squat | 5 × 5 | 80% | 3/0/1/0 | 240 s |
| 2. Push press | 3 × 5 | 80% | 3/0/1/0 | 240 s | ||
| 3. Hip thrust | 3 × 5 | 80% | 3/0/1/0 | 240 s | ||
| 4. Nordic curl | 3 × 4 | Body mass | 3/0/1/0 | 180 s | ||
| VIII | 1. Deadlift | 3 × 5 | 80% | 3/1/1/0 | 240 s | |
| 2. Bulgarian squat | 3 × 5 | 80% | 1/0/1/0 | 240 s | ||
| 3. Calf raise on leg press machine | 3 × 5 | 80% | 3/0/1/0 | 180 s | ||
| 4. Abs wheel | 4 × 5 | Body mass | 1/0/1/2 | 180 s | ||
| IX | 1. Barbell squat | 3 × 5 | 80% | 1/2/1/0 | 240 s | |
| 2. Push press | 3 × 5 | 80% | 1/0/1/0 | 240 s | ||
| 3. Hip thrust | 3 × 5 | 80% | 1/0/1/2 | 240 s | ||
| 4. Nordic curl | 3 × 4 | Body mass | 3/0/1/0 | 180 s | ||
| IV | X | 1. Barbell squat | 3 × 3 | 85% | 1/0/1/0 | 300 s |
| 2. Push press | 3 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 3. Hip thrust | 3 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 4. Nordic curl | 3 × 4 | Body mass | 3/0/1/0 | 180 s | ||
| XI | 1. Deadlift | 3 × 3 | 85% | 1/1/1/0 | 300 s | |
| 2. Bulgarian squat | 3 × 5 | 85% | 1/0/1/0 | 300 s | ||
| 3. Calf raise on leg press machine | 3 × 5 | 85% | 3/0/1/0 | 180 s | ||
| 4. Abs wheel | 4 × 5 | Body mass | 1/0/1/2 | 180 s | ||
| XII | 1. Barbell squat | 3 × 3 | 85% | 1/2/1/0 | 300 s | |
| 2. Push press | 3 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 3. Hip thrust | 3 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 4. Nordic curl | 3 × 4 | Body mass | 3/0/1/0 | 180 s | ||
| V | XIII | 1. Barbell squat | 5 × 3 | 85% | 1/0/1/0 | 300 s |
| 2. Push press | 3 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 3. Hip thrust | 3 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 4. Nordic curl | 3 × 5 | Body mass | 3/0/1/0 | 180 s | ||
| XIV | 1. Deadlift | 3 × 3 | 85% | 1/1/1/0 | 300 s | |
| 2. Bulgarian squat | 3 × 5 | 85% | 1/0/1/0 | 300 s | ||
| 3. Calf raise on leg press machine | 3 × 5 | 85% | 3/0/1/0 | 180 s | ||
| 4. Abs wheel | 5 × 5 | Body mass | 1/0/1/0 | 180 s | ||
| XV | 1. Barbell squat | 3 × 3 | 85% | 1/2/1/0 | 300 s | |
| 2. Push press | 3 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 3. Hip thrust | 3 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 4. Nordic curl | 3 × 5 | Body mass | 3/0/1/0 | 180 s | ||
| VI | XVI | 1. Barbell squat | 1 × 3 | 85% | 1/0/1/0 | 300 s |
| 2. Push press | 1 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 3. Hip thrust | 1 × 3 | 85% | 1/0/1/0 | 300 s | ||
| 4. Nordic curl | 1 × 5 | Body mass | 3/0/1/0 | 180 s | ||
| XVII | 1. Bulgarian squat | 3 × 5 | 85% | 1/0/1/0 | 300 s | |
| 2. Calf raise on leg press machine | 3 × 5 | 85% | 3/0/1/0 | 180 s | ||
| 3. Abs wheel | 3 × 5 | Body mass | 1/0/1/0 | 180 s | ||
| XVIII | 1. Barbell squat | 1 × 1 | 100% | 1/0/1/0 | 300 s | |
| 2. Deadlift | 1 × 1 | 100% | 1/0/1/0 | 300 s | ||
| 3. Hip thrust | 1 × 1 | 100% | 1/0/1/0 | 300 s |
| Variable | Group | Pre | Post | Effect: Group F p ηp2 | Effect: Time F p ηp2 | Interaction F p ηp2 | Post-Hoc | ES |
|---|---|---|---|---|---|---|---|---|
| MP [W] | CON | 639.99 ± 91.98 | 637.92 ± 92.94 | 1.55 | 7.58 | 5.41 | 0.99 | 0.02 |
| ST | 671.06 ± 86.19 | 697.25 ± 78.83 | 0.22 | 0.001 | 0.001 | 0.002 | 0.32 | |
| AIT | 685.44 ± 76.29 | 691.22 ± 8.85 | 0.07 | 0.15 | 0.2 | 0.94 | 0.07 | |
| rel_MP [W/kg] | CON | 8.74 ± 0.72 | 8.69 ± 0.75 | 3.02 | 2.54 | 2.48 | 0.99 | 0.07 |
| ST | 8.12 ± 0.96 | 8.37 ± 0.76 | 0.06 | 0.12 | 0.1 | 0.12 | 0.29 | |
| AIT | 8.94 ± 0.75 | 9.01 ± 1.05 | 0.12 | 0.06 | 0.1 | 0.98 | 0.08 | |
| PP [W] | CON | 810.57 ± 132.39 | 796.79 ± 137.79 | 4.27 | 13.65 | 10.74 | 0.73 | 0.10 |
| ST | 894.15 ± 112.28 | 944.15 ± 116.19 | 0.02 | <0.001 | <0.001 | <0.001 | 0.44 | |
| AIT | 896.07 ± 121.14 | 922.91 ± 106.29 | 0.17 | 0.24 | 0.34 | 0.09 | 0.24 | |
| rel_PP [W/kg] | CON | 11.06 ± 1.07 | 10.83 ± 1.22 | 3.26 | 7.04 | 7.39 | 0.64 | 0.20 |
| ST | 10.8 ± 0.95 | 11.32 ± 1.02 | 0.05 | 0.01 | 0.002 | <0.001 | 0.53 | |
| AIT | 11.66 ± 1.03 | 12.02 ± 1.15 | 0.13 | 0.14 | 0.26 | 0.15 | 0.33 | |
| FI [%] | CON | 21.61 ± 6.69 | 20.39 ± 4.46 | 5.14 | 0.79 | 2.01 | 0.87 | 0.22 |
| ST | 25.97 ± 4.79 | 27.45 ± 5.87 | 0.01 | 0.38 | 0.15 | 0.75 | 0.28 | |
| AIT | 24.02 ± 5.94 | 25.42 ± 4 | 0.2 | 0.02 | 0.09 | 0.78 | 0.28 | |
| FI [W/s] | CON | 14.16 ± 4.12 | 14.37 ± 3.59 | 9.38 | 5.83 | 0.8 | 0.99 | 0.05 |
| ST | 18.79 ± 3.08 | 19.92 ± 3.25 | <0.001 | 0.02 | 0.46 | 0.4 | 0.36 | |
| AIT | 16.8 ± 4.09 | 17.9 ± 1.99 | 0.31 | 0.12 | 0.04 | 0.42 | 0.36 |
| Variable | Group | Pre | Post | Effect: Group F p ηp2 | Effect: Time F p ηp2 | Interaction F p ηp2 | Post-Hoc | ES |
|---|---|---|---|---|---|---|---|---|
| Pmax [W] | CON | 248 ± 27.84 | 242.5 ± 28.44 | 11.22 | 12.71 | 9.01 | 0.78 | 0.20 |
| ST | 235 ± 33.86 | 254 ± 38.75 | <0.001 | <0.001 | <0.001 | <0.001 | 0.52 | |
| AIT | 286.87 ± 33.69 | 299.53 ± 35.84 | 0.35 | 0.23 | 0.3 | 0.05 | 0.36 | |
| rel_Pmax [W/kg] | CON | 3.38 ± 3.04 | 3.3 ± 3.17 | 13.41 | 7.73 | 7.46 | 0.66 | 0.03 |
| ST | 2.84 ± 4.06 | 3.04 ± 4.63 | <0.001 | <0.001 | <0.001 | 0.01 | 0.05 | |
| AIT | 3.72 ± 3.93 | 3.88 ± 4.25 | 0.39 | 0.15 | 0.26 | 0.09 | 0.04 | |
| HRmax [bpm] | CON | 186.33 ± 10.43 | 184.33 ± 10.22 | 0.29 | 1.08 | 1.44 | 0.76 | 0.19 |
| ST | 184.6 ± 9.47 | 186 ± 9,77 | 0.99 | 0.97 | 0.25 | 0.93 | 0.15 | |
| AIT | 184.87 ± 10.88 | 185.53 ± 14.2 | 0.01 | 0.01 | 0.06 | 0.99 | 0.05 | |
| VO2max [L/min] | CON | 3.16 ± 0.41 | 3.14 ± 0.41 | 6.69 | 19.51 | 6.63 | 0.99 | 0.05 |
| ST | 3.06 ± 0.55 | 3.34 ± 0.56 | 0.002 | <0.001 | 0.003 | <0.001 | 0.50 | |
| AIT | 3.58 ± 0.36 | 3.78 ± 0.37 | 0.24 | 0.32 | 0.24 | 0.02 | 0.55 | |
| VO2max [ml/kg/min] | CON | 43.87 ± 7.19 | 43.33 ± 6.75 | 7.42 | 11.58 | 5.23 | 0.98 | 0.08 |
| ST | 37.4 ± 8.02 | 40.07 ± 7.21 | 0.002 | 0.001 | <0.001 | 0.02 | 0.35 | |
| AIT | 46.93 ± 5.91 | 49.47 ± 6.09 | 0.26 | 0.22 | 0.19 | 0.03 | 0.42 | |
| RER | CON | 1.18 ± 0.09 | 1.14 ± 0.09 | 4.88 | 11.98 | 0.04 | 0.32 | 0.44 |
| ST | 1.19 ± 0.08 | 1.16 ± 0.09 | 0.01 | 0.001 | 0.96 | 0.49 | 0.38 | |
| AIT | 1.12 ± 0.05 | 1.08 ± 0.07 | 0.19 | 0.22 | 0.001 | 0.28 | 0.80 |
| Variable | Group | Pre | Post | Effect: Group F p ηp2 | Effect: Time F p ηp2 | Interaction F p ηp2 | Post-Hoc | ES |
|---|---|---|---|---|---|---|---|---|
| PVT2 (W) | CON | 136 ± 19.42 | 136.3 ± 26.1 | 9.34 | 1.94 | 0.78 | 1.0 | 0.01 |
| ST | 130 ± 37.03 | 134 ± 33.76 | <0.001 | 0.17 | 0.46 | 0.98 | 0.11 | |
| AIT | 164.93 ± 19.42 | 175.53 ± 26.08 | 0.31 | 0.04 | 0.04 | 0.51 | 0.47 | |
| Pmax [%] | CON | 54.7 ± 8.62 | 56.7 ± 8.2 | 0.71 | 0.001 | 0.98 | 0.97 | 0.24 |
| ST | 55.33 ± 13.12 | 52.6 ± 10.46 | 0.49 | 0.97 | 0.39 | 0.88 | 0.23 | |
| AIT | 58.07 ± 8.62 | 59 ± 8.2 | 0.03 | 0.03 | 0.04 | 0.99 | 0.11 | |
| HRVT2 [bpm] | CON | 136.8 ± 13.2 | 137.3 ± 16.65 | 3.14 | 0.16 | 0.01 | 0.99 | 0.03 |
| ST | 139.33 ± 14.39 | 141.2 ± 16.15 | 0.05 | 0.69 | 0.91 | 0.99 | 0.12 | |
| AIT | 148.93 ± 13.19 | 148.8 ± 16.65 | 0.13 | 0.003 | 0.005 | 1.0 | 0.01 | |
| HRmax [%] | CON | 72.93 ± 6.21 | 74.73 ± 6.25 | 4.47 | 0.43 | 0.37 | 0.89 | 0.29 |
| ST | 75.47 ± 7.35 | 75.8 ± 7.93 | 0.02 | 0.51 | 0.69 | 0.99 | 0.04 | |
| AIT | 80.4 ± 6.22 | 80.2 ± 6.25 | 0.17 | 0.01 | 0.02 | 0.99 | 0.03 | |
| VO2VT2 [L/min] | CON | 1.84 ± 0.26 | 1.87 ± 0.33 | 11.08 | 6.67 | 1.11 | 0.99 | 0.10 |
| ST | 1.78 ± 0.42 | 1.89 ± 0.38 | <0.001 | 0.01 | 0.34 | 0.65 | 0.28 | |
| AIT | 2.19 ± 0.26 | 2.38 ± 0.33 | 0.34 | 0.14 | 0.05 | 0.04 | 0.64 | |
| VO2max [%] | CON | 58.1 ± 10.1 | 60.6 ± 8.5 | 1.35 | 0.63 | 0.61 | 0.86 | 0.27 |
| ST | 58 ± 8.63 | 57.13 ± 9.57 | 0.27 | 0.43 | 0.55 | 0.99 | 0.10 | |
| AIT | 61.73 ± 10.07 | 63.13 ± 8.5 | 0.06 | 0.01 | 0.03 | 0.99 | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drwal, A.; Maciejczyk, M. Strength Training vs. Aerobic Interval Training: Effects on Anaerobic Capacity, Aerobic Power and Second Ventilatory Threshold in Men. Appl. Sci. 2025, 15, 7953. https://doi.org/10.3390/app15147953
Drwal A, Maciejczyk M. Strength Training vs. Aerobic Interval Training: Effects on Anaerobic Capacity, Aerobic Power and Second Ventilatory Threshold in Men. Applied Sciences. 2025; 15(14):7953. https://doi.org/10.3390/app15147953
Chicago/Turabian StyleDrwal, Aleksander, and Marcin Maciejczyk. 2025. "Strength Training vs. Aerobic Interval Training: Effects on Anaerobic Capacity, Aerobic Power and Second Ventilatory Threshold in Men" Applied Sciences 15, no. 14: 7953. https://doi.org/10.3390/app15147953
APA StyleDrwal, A., & Maciejczyk, M. (2025). Strength Training vs. Aerobic Interval Training: Effects on Anaerobic Capacity, Aerobic Power and Second Ventilatory Threshold in Men. Applied Sciences, 15(14), 7953. https://doi.org/10.3390/app15147953