
The Impact of Digital Imaging Tools and Artificial Intelligence on Self-Reported Outcomes of Dentists

 , ,
, ,  and
and
Abstract
1. Introduction
- (a)
- to assess, analyze, and correlate dental clinicians’ self-reported outcomes related to the impact of digital and AI technologies on their clinical activities;
- (b)
- to compare these outcomes between users and non-users of digital imaging tools;
- (c)
- to qualitatively evaluate the experiences and satisfaction levels among practitioners who currently utilize AI-based software applications.
- (a)
- dental clinicians’ self-reported outcomes are not significantly correlated with the use of digital and AI technologies in their clinical activities;
- (b)
- users and non-users of digital imaging tools do not differ in self-reported outcomes;
- (c)
- AI-based software applications do not influence clinical experience and satisfaction.
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
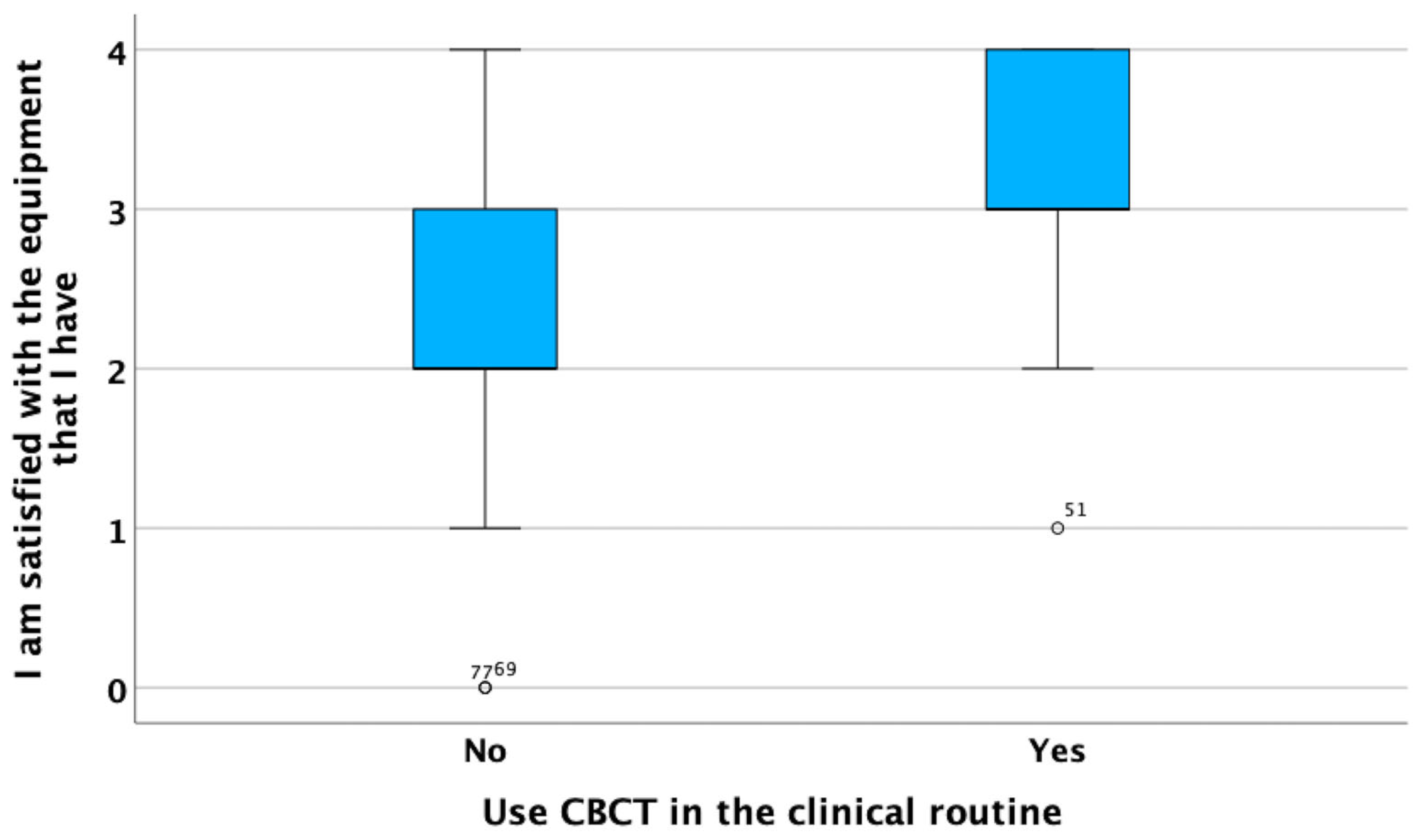
- The Digital Imaging Tools domain included statements addressing the essential role of photographic cameras, intraoral scanners, and CBCT devices in dental clinics, along with a general assessment of satisfaction with available equipment.
- The AI Software domain consisted of a single item, focusing on the use of AI-powered software for diagnostic and treatment planning purposes, consisting of three different qualitative open-ended follow-up questions to identify specific tools, their functions, and rationale for use.
- The Job Satisfaction items explored whether dentists felt they had sufficient time for patient care, satisfaction with their workload, and whether they felt their work was appreciated by patients.
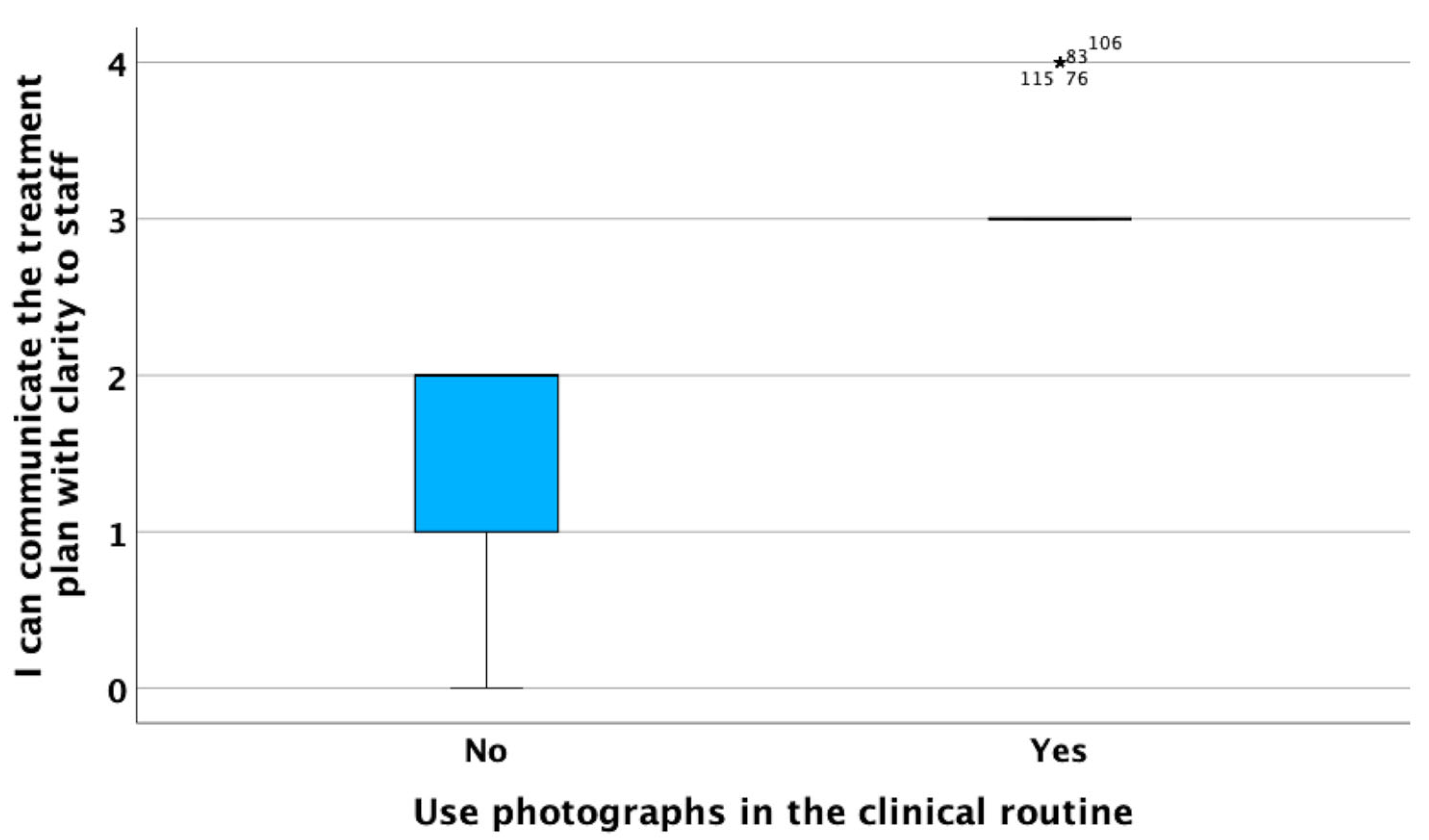
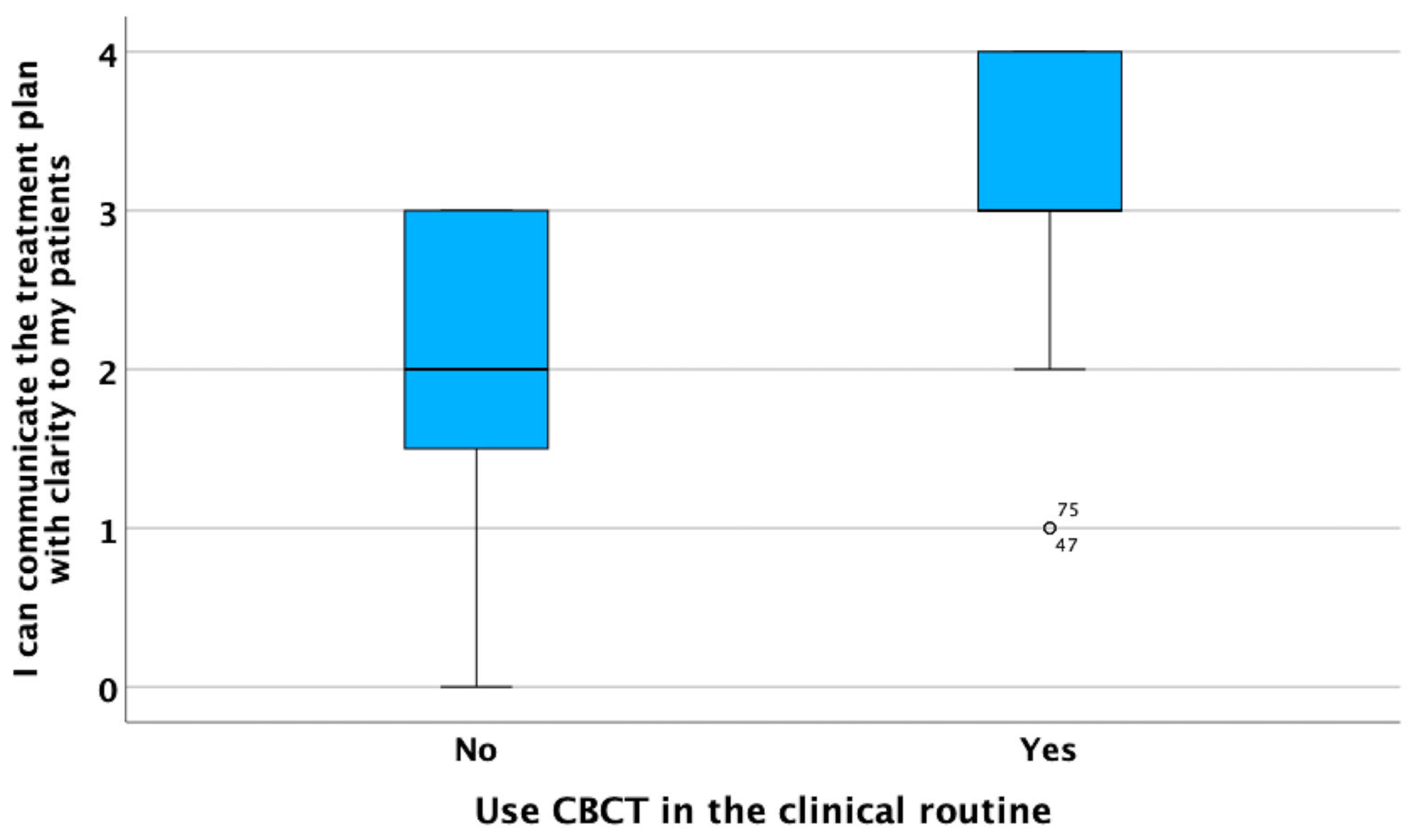
- The Time and Communication cluster assessed the clarity of treatment plan communication with patients, staff, and dental laboratories, as well as the ability to visually present treatment outcomes to patients before starting procedures.
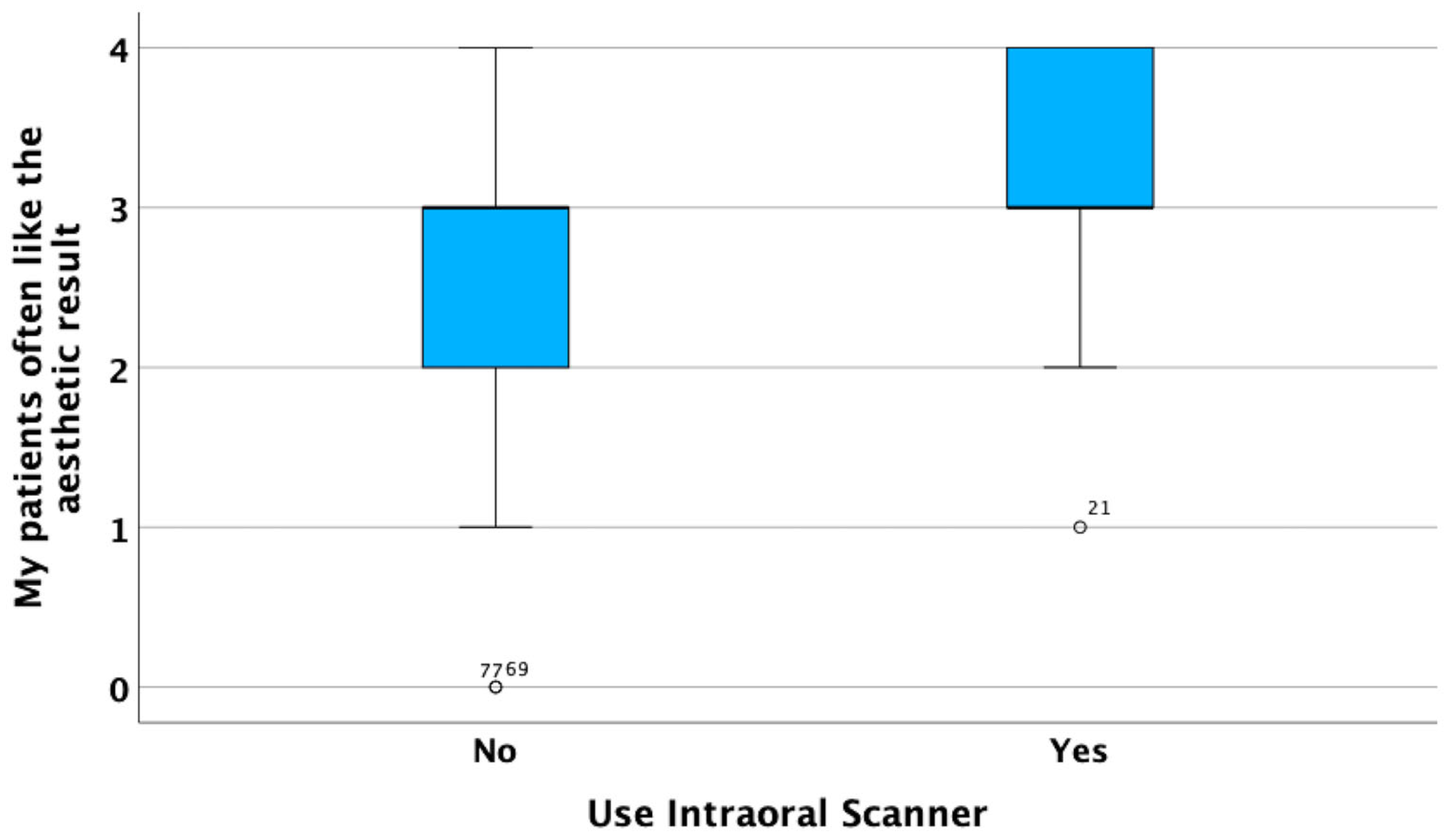
- The Patient Expectations domain included items evaluating the frequency with which patient expectations were met, the quality of dentist–patient relationships, feedback on treatment comfort, and satisfaction with aesthetic results.
2.3. Participants
2.4. Statistical Analyses
2.5. Ethical Aspects
3. Results
4. Discussion
4.1. Influence of Digital Imaging Tools on Self-Reported Outcomes
4.2. User–Non-User Comparisons and the Role of Training
4.3. The Emerging but Underpowered Role of AI Software
4.4. Broader Implications for Digital Dentistry
4.5. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suganna, M.; Nayakar, R.P.; Alshaya, A.A.; Khalil, R.O.; Alkhunaizi, S.T.; Kayello, K.T.; Alnassar, L.A. The Digital Era Heralds a Paradigm Shift in Dentistry: A Cross-Sectional Study. Cureus 2024, 16, e53300. [Google Scholar] [CrossRef] [PubMed]
- Van Noort, R. The Future of Dental Devices Is Digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Cortes, A.R.G. Digital Dentistry: A Step-By-Step Guide and Case Atlas, 1st ed.; Wiley Blackwell: Hoboken, NJ, USA, 2022; pp. 281–285. [Google Scholar]
- Yeslam, H.E.; von Maltzahn, N.F.; Nassar, H.M. Revolutionizing CAD/CAM-Based Restorative Dental Processes and Materials with Artificial Intelligence: A Concise Narrative Review. PeerJ 2024, 12, e17793. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, M.; Zhu, Y.; Shrestha, A. A Review of Advancements of Artificial Intelligence in Dentistry. Dent. Rev. 2024, 4, 100081. [Google Scholar] [CrossRef]
- Sikri, A.; Sikri, J.; Piplani, V.; Thakur, Y. Applications of Artificial Intelligence in Dentistry: A Narrative Review. South Asian Res. J. Oral Dent. Sci. 2024, 6, 1–10. [Google Scholar] [CrossRef]
- Moon, W.; Kim, S.; Lim, B.S.; Park, Y.S.; Kim, R.J.Y.; Chung, S.H. Dimensional Accuracy Evaluation of Temporary Dental Restorations with Different 3D Printing Systems. Materials 2021, 14, 1487. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.H.; Jeong, S.N.; Choi, S.H. Detection and Diagnosis of Dental Caries Using a Deep Learning-Based Convolutional Neural Network Algorithm. J. Dent. 2018, 77, 106–111. [Google Scholar] [CrossRef]
- Schwendicke, F.; Samek, W.; Krois, J. Artificial Intelligence in Dentistry: Chances and Challenges. J. Dent. Res. 2020, 99, 769–774. [Google Scholar] [CrossRef]
- Mangano, F.; Veronesi, G.; Hauschild, U.; Mijiritsky, E.; Mangano, C. Trueness and Precision of Four Intraoral Scanners in Oral Implantology: A Comparative In Vitro Study. PLoS ONE 2016, 11, e0163107. [Google Scholar] [CrossRef]
- Ahmed, N.; Abbasi, M.S.; Zuberi, F.; Qamar, W.; Halim, M.S.B.; Maqsood, A.; Alam, M.K. Artificial Intelligence Techniques: Analysis, Application, and Outcome in Dentistry—A Systematic Review. Biomed Res. Int. 2021, 2021, 9751564. [Google Scholar] [CrossRef]
- Buduru, S.; Cofar, F.; Mesaroș, A.; Tăut, M.; Negucioiu, M.; Almășan, O. Perceptions in Digital Smile Design: Assessing Laypeople and Dental Professionals’ Preferences Using an Artificial-Intelligence-Based Application. Dent. J. 2024, 12, 104. [Google Scholar] [CrossRef]
- Tabatabaian, F.; Vora, S.R.; Mirabbasi, S. Applications, Functions, and Accuracy of Artificial Intelligence in Restorative Dentistry: A Literature Review. J. Esthet. Restor. Dent. 2023, 35, 842–859. [Google Scholar] [CrossRef]
- Revilla-León, M.; Gómez-Polo, M.; Vyas, S.; Barmak, A.B.; Özcan, M.; Att, W.; Krishnamurthy, V.R. Artificial Intelligence Applications in Restorative Dentistry: A Systematic Review. J. Prosthet. Dent. 2022, 128, 867–875. [Google Scholar] [CrossRef]
- Bell, J. Doing Your Research Project: A Guide for First-Time Researchers in Education, Health and Social Science, 5th ed.; Open University Press: Maidenhead, UK, 2010. [Google Scholar]
- Dawa, H.; Neves, J.; Vicente, H. Evaluating the Impact of Digital Tool Utilization in Dentistry on Burnout Syndrome Among Dentists: An Entropy Analysis and AI-Driven Approach. Eng 2025, 6, 47. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral Scanners in Dentistry: A Review of the Current Literature. BMC Oral. Health 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Zarone, F.; Ferrari, M. The Complete Digital Workflow in Fixed Prosthodontics: A Systematic Review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef] [PubMed]
- Iniesta, M.; Pérez-Higueras, J.J. Global Trends in the Use of Artificial Intelligence in Dental Education: A Bibliometric Analysis. Eur. J. Dent. Educ. 2025. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Shibli, J.A.; Fortin, T. Digital Dentistry: New Materials and Techniques. Int. J. Dent. 2016, 2016, 5261247. [Google Scholar] [CrossRef]
- Kau, C.H.; Li, J.; Li, Q.; Abou Kheir, N. Update on Cone Beam Technology and Orthodontic Analysis. Curr. Dent. Technol. 2014, 58, 653–669. [Google Scholar] [CrossRef]
- Sarwar, S.; Jabin, S. AI Techniques for Cone Beam Computed Tomography in Dentistry: Trends and Practices. arXiv 2023, arXiv:2306.03025. [Google Scholar] [CrossRef]
- Subramanian, A.K.; Chen, Y.; Almalki, A.; Sivamurthy, G.; Kafle, D. Cephalometric Analysis in Orthodontics Using Artificial Intelligence—A Comprehensive Review. Biomed. Res. Int. 2022, 2022, 1880113. [Google Scholar] [CrossRef]
- Diagnocat. AI-Powered Dental Intelligence. Available online: https://diagnocat.com/uk/usage/doctors-claim-intelligence-platform/ (accessed on 3 July 2025).
- Hello Pearl. Second Opinion for Real-Time Diagnosis. Available online: https://www.hellopearl.com/products/second-opinion (accessed on 3 July 2025).
- Institute of Digital Dentistry. Diagnocat Review. Available online: https://instituteofdigitaldentistry.com/ai/ (accessed on 3 July 2025).
- Spot On Business Planning. Diagnocat and Patient Communication. Available online: https://www.spoton-businessplanning.co.uk/blog/ (accessed on 3 July 2025).
- Umer, F.; Adnan, S.; Lal, A. Research and Application of Artificial Intelligence in Dentistry from Lower-Middle Income Countries: A Scoping Review. BMC Oral Health 2024, 24, 220. [Google Scholar] [CrossRef] [PubMed]
- Villena, F.; Véliz, C.; García-Huidobro, R.; Aguayo, S. Generative Artificial Intelligence in Dentistry: Current Approaches and Future Challenges. arXiv 2024, arXiv:2407.17532. [Google Scholar] [CrossRef]
- Pérez de Frutos, J.; Helland, R.H.; Desai, S.; Nymoen, L.C.; Langø, T.; Remman, T.; Sen, A. AI-Dentify: Deep Learning for Proximal Caries Detection on Bitewing X-ray—HUNT4 Oral Health Study. arXiv 2023, arXiv:2310.00354. [Google Scholar] [CrossRef] [PubMed]
- Rokaya, D.; Jaghsi, A.A.; Jagtap, R.; Srimaneepong, V. Artificial Intelligence in Dentistry and Dental Biomaterials. Front. Dent. Med. 2024, 5, 1525505. [Google Scholar] [CrossRef]
- Stanford, C. Implant Dentistry and Artificial Intelligence: A Double-Edged Innovation? Int. J. Oral Maxillofac. Implants 2025, 40, 280. [Google Scholar] [CrossRef]
- Cortes, A.R.G. Artificial Intelligence in Planning Oral Rehabilitations: Current Status. Appl. Sci. 2024, 14, 4093. [Google Scholar] [CrossRef]
- Agrawal, A.A.; Prakash, N.; Almagbol, M.; Alobaid, M.; Alqarni, A.; Altamni, H. Synoptic review on existing and potential sources for bias in dental research methodology with methods on their prevention and remedies. World. J. Methodol. 2023, 13, 426–438. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Digital Imaging Tools | Photographic cameras are essential. |
| Intraoral scanners are indispensable. | |
| Cone Beam CT is indispensable. | |
| I am satisfied with the dental equipment I have. | |
| AI software | I use AI software for diagnosis or treatment planning. |
| Job Satisfaction | I have enough time to dedicate to my patients. |
| I am satisfied with my current workload. | |
| My patients value my work. | |
| Time and communication | I can communicate the treatment plan with clarity to my patients. |
| I can communicate with clarity with staff. | |
| I can communicate with clarity with the dental laboratory | |
| I can show the patient the result before embarking on treatment. | |
| Patient expectations | I often deliver results that correspond to my patients’ anticipated outcome. |
| I always have a pleasant relationship with my patients. | |
| My patients do not complain about long, uncomfortable treatments. | |
| My patients often like the aesthetic result. |
| Section Variables About Dental Professional Activity | Digital Imaging Tools (As Indispensable in Dental Clinics) | ||
|---|---|---|---|
| Photography | Intraoral Scanner | CBCT | |
| I have enough time to devote to patients | r = 0.474 p < 0.001 | r = 0.251 p = 0.005 | r = 0.365 p < 0.001 |
| I am happy with my current work rate | r = 0.454 p < 0.001 | r = 0.211 p = 0.018 | r = 0.478 p < 0.001 |
| My patients value my work | r = 0.285 p = 0.001 | r = 0.378 p < 0.001 | r = 0.155 p = 0.083 |
| I am satisfied with the dental equipment that I have | r = 0.423 p < 0.001 | r = 0.359 p < 0.001 | r = 0.754 p < 0.001 |
| I can communicate the treatment plan with clarity to my patients | r = 0.436 p < 0.001 | r = 0.320 p < 0.001 | r = 0.653 p < 0.001 |
| I can communicate the treatment plan with clarity to staff | r = 0.985 p < 0.001 | r = 0.436 p < 0.001 | r = 0.462 p < 0.001 |
| I can communicate the treatment plan with clarity to the dental technician | r = 0.436 p < 0.001 | r = 0.985 p < 0.001 | r = 0.328 p < 0.001 |
| I can show the patient the result before starting the treatment | r = 0.462 p < 0.001 | r = 0.328 p < 0.001 | r = 0.985 p < 0.001 |
| I am often able to meet my patient’s expectations | r = 0.423 p < 0.001 | r = 0.359 p < 0.001 | r = 0.754 p < 0.001 |
| I always have a pleasant relationship with my patients | r = 0.436 p < 0.001 | r = 0.320 p < 0.001 | r = 0.653 p < 0.001 |
| My patients do not complain about long, uncomfortable treatments | r = 0.277 p = 0.002 | r = 0.494 p < 0.001 | r = 0.478 p < 0.001 |
| My patients often like the aesthetic result | r = 0.372 p < 0.001 | r = 0.401 p < 0.001 | r = 0.429 p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dawa, H.; No-Cortes, J.; Peñarrocha-Diago, M.; Vicente, H.; Ribeiro, C.; Cortes, A.R.G. The Impact of Digital Imaging Tools and Artificial Intelligence on Self-Reported Outcomes of Dentists. Appl. Sci. 2025, 15, 7943. https://doi.org/10.3390/app15147943
Dawa H, No-Cortes J, Peñarrocha-Diago M, Vicente H, Ribeiro C, Cortes ARG. The Impact of Digital Imaging Tools and Artificial Intelligence on Self-Reported Outcomes of Dentists. Applied Sciences. 2025; 15(14):7943. https://doi.org/10.3390/app15147943
Chicago/Turabian StyleDawa, Hossam, Juliana No-Cortes, Miguel Peñarrocha-Diago, Henrique Vicente, Carlos Ribeiro, and Arthur Rodriguez Gonzalez Cortes. 2025. "The Impact of Digital Imaging Tools and Artificial Intelligence on Self-Reported Outcomes of Dentists" Applied Sciences 15, no. 14: 7943. https://doi.org/10.3390/app15147943
APA StyleDawa, H., No-Cortes, J., Peñarrocha-Diago, M., Vicente, H., Ribeiro, C., & Cortes, A. R. G. (2025). The Impact of Digital Imaging Tools and Artificial Intelligence on Self-Reported Outcomes of Dentists. Applied Sciences, 15(14), 7943. https://doi.org/10.3390/app15147943