


Cable-Driven Exoskeleton for Ankle Rehabilitation in Children with Cerebral Palsy
 , , , ,
, , , ,  and
and
Abstract
Featured Application
Abstract
1. Introduction
- Develop a new ankle control module that is capable of guiding ankle movement in 3 DOFs (x and z translations and rotation) by mimicking healthy human gait patterns.
- Make sure to restrict unwanted abduction and adduction rotations of the ankle (lateral rotation of the ankle).
- Ensure the modular character of the exoskeleton for easy implementation and communication with the global D2W system.
- Implement the Assistance-as-Needed (AAN) model that combines robotic actuation with the patient’s effort and ability to move for the correct performance of movements during rehabilitation (to be detailed more specifically in Section 2.2.4).
- To carry out the experimental validation of the prototype with a CP patient to ensure its safety and ability to guide the movements of interest. This would lead, if successful, to the start of the clinical validation process of the prototype.
2. Exoskeleton Development and Control Methodology
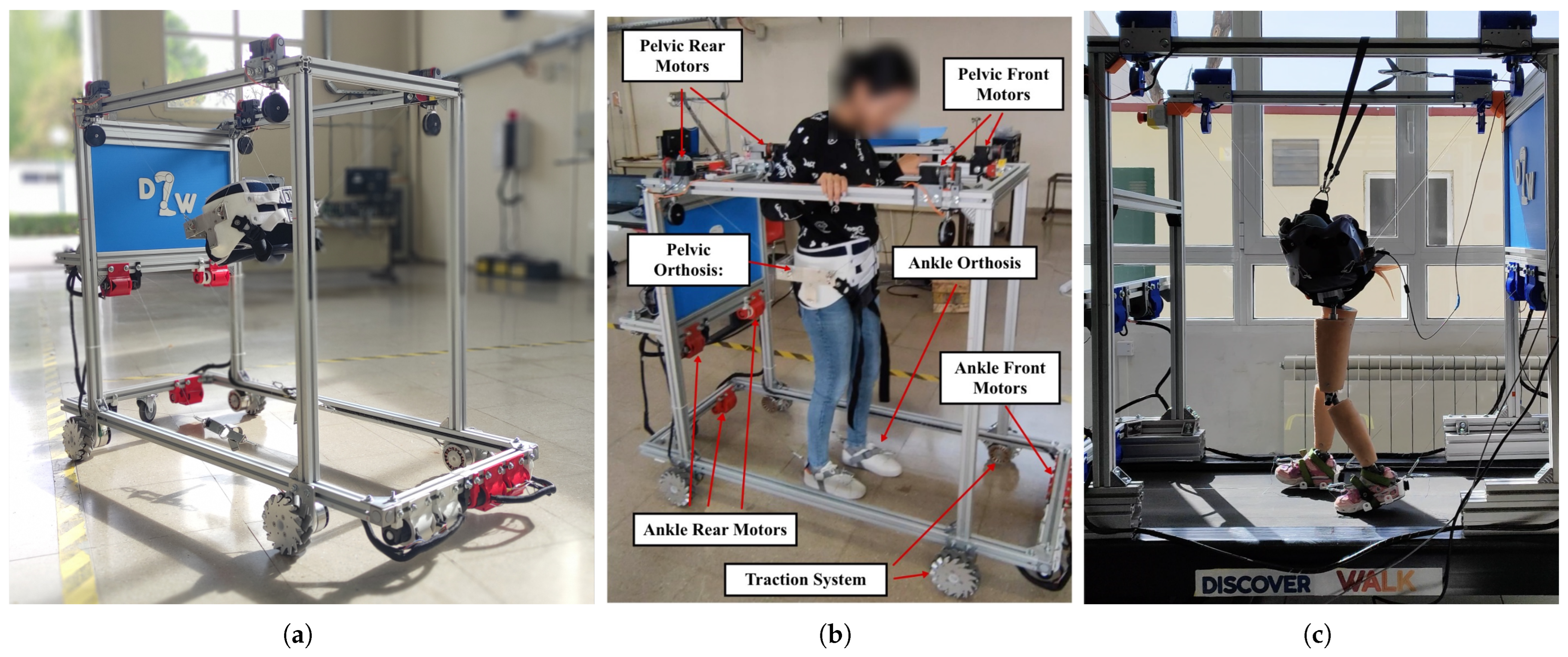
2.1. Discover2Walk Overview
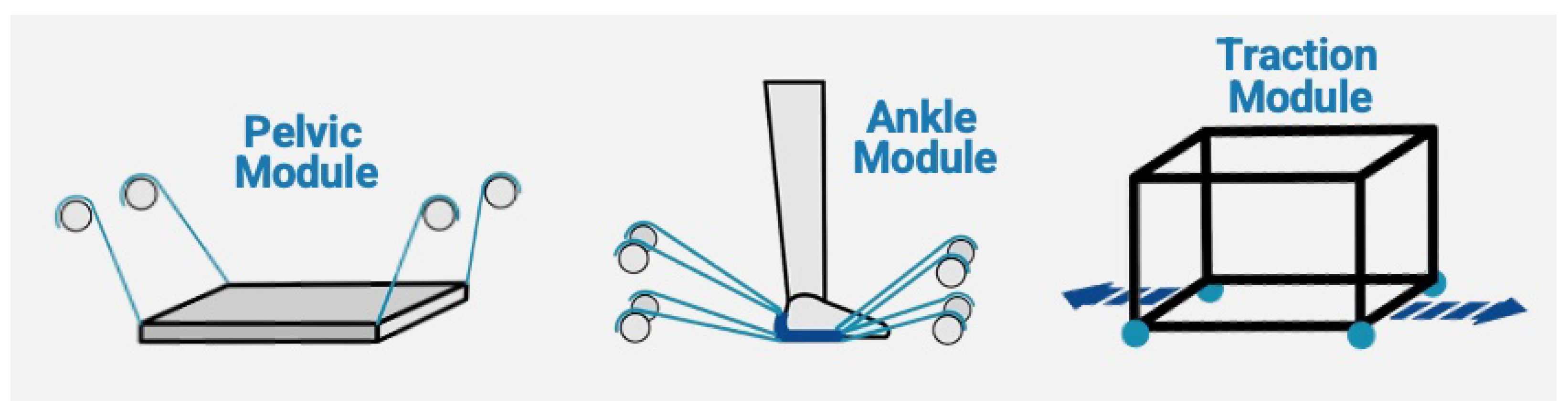
2.1.1. Pelvic Module
- Inertial measurement unit (IMU): allows the monitoring of the pelvis angular position, velocity, and linear acceleration. The model used is BNO055 IMU (BoschSensortec, Reutlingen, Germany).
- Motor absolutes encoders: to measure the length of the cables. The model used is AMT102-V encoders (CUI Devices, Oswego, OR, USA).
- Load cells: to control partial body weight support. The model used is DYMH-103 load cells with a maximum capacity of 20 kg (CALT Sensor, Shanghai, China).
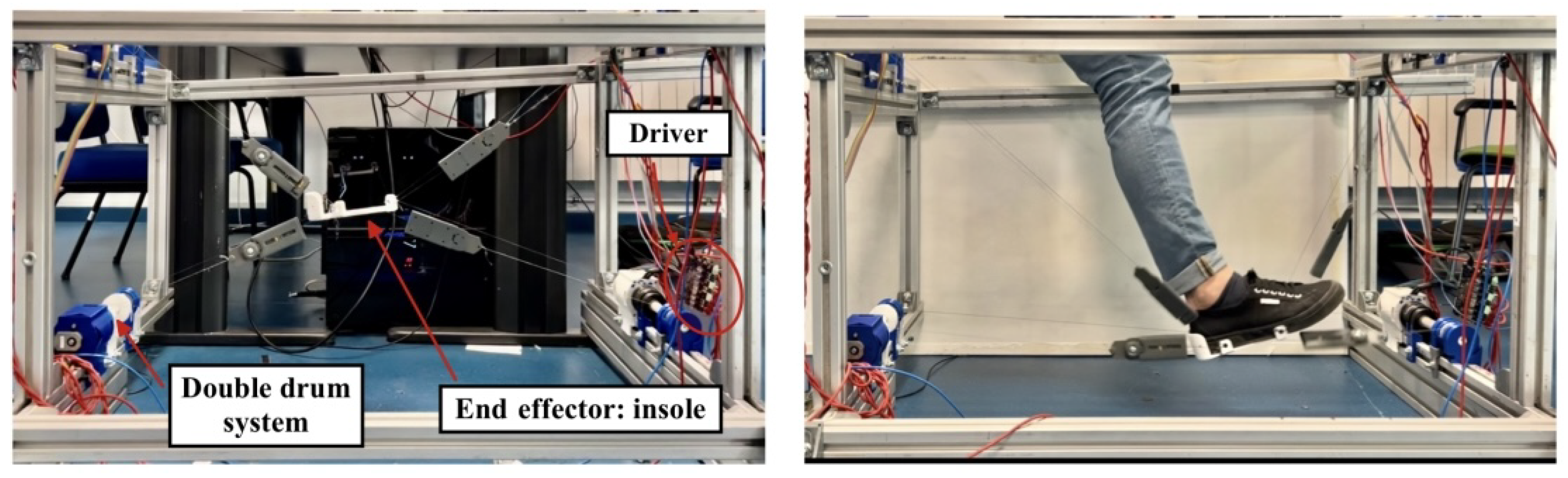
2.1.2. Ankle Control Module
2.1.3. Traction Control Module
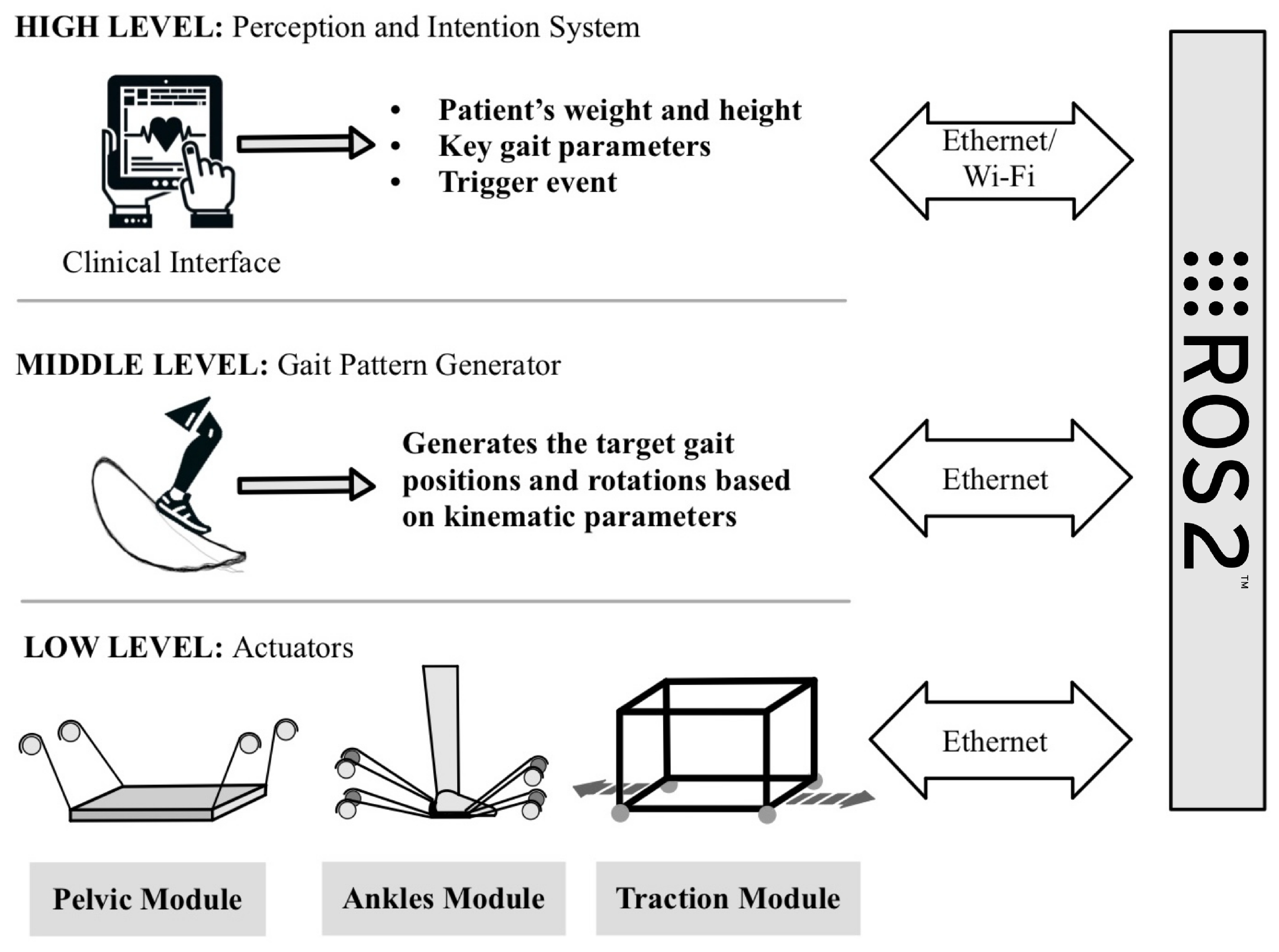
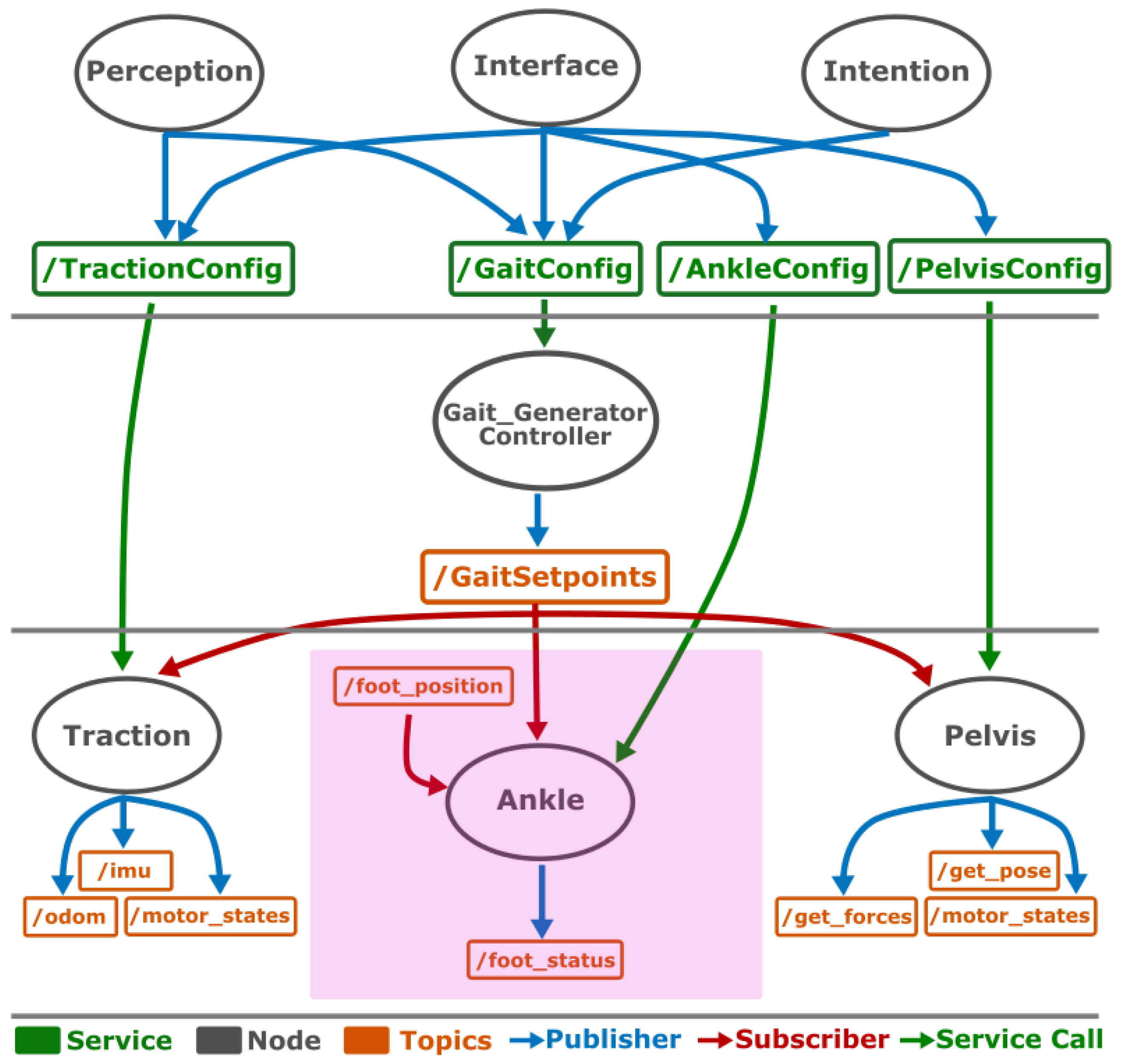
2.1.4. Bio-Inspired Architecture
- High level: it is the one associated with the processes of perception and intention. It is implemented through a clinical interface that modifies the parameters of the exoskeleton according to the anthropometric conditions of the patient (height and weight) and uses a trigger event to initialize the movement.
- Medium level: based on the parameters determined at the high level and the sensor readings of the subject’s movement, it is responsible for generating the gait patterns to be performed by the subjects [42]. These trajectories will be sent to the low level.
- Low level: it is in charge of ensuring that each of the actuators of the three modules (pelvis, ankle, and traction) reaches the positions calculated by the middle level so that the trajectories are performed correctly. As in the human body, each actuator has sensors that send feedback to the middle level.
2.2. Novel Ankle CDPR Module
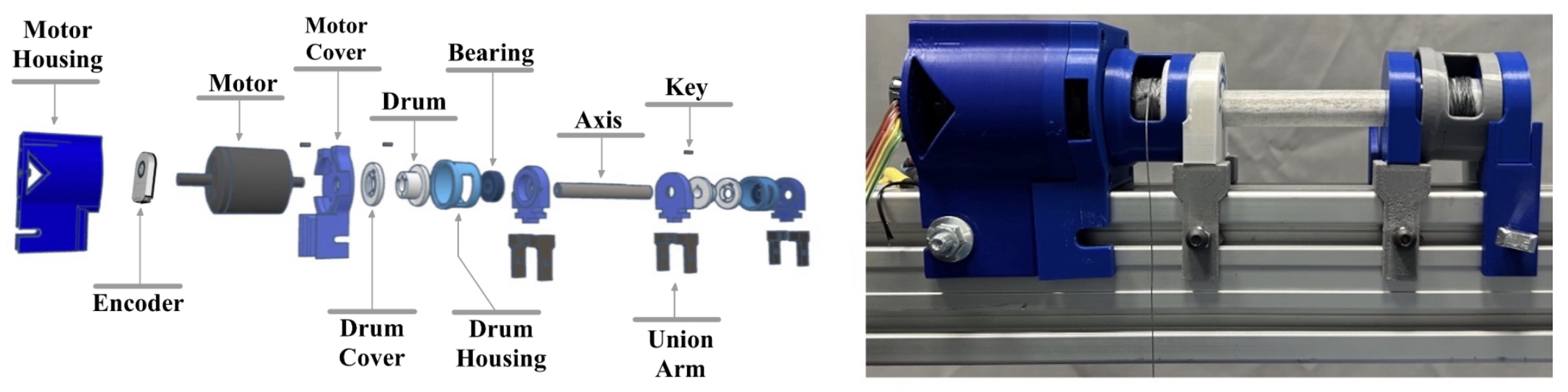
2.2.1. Mechanical System
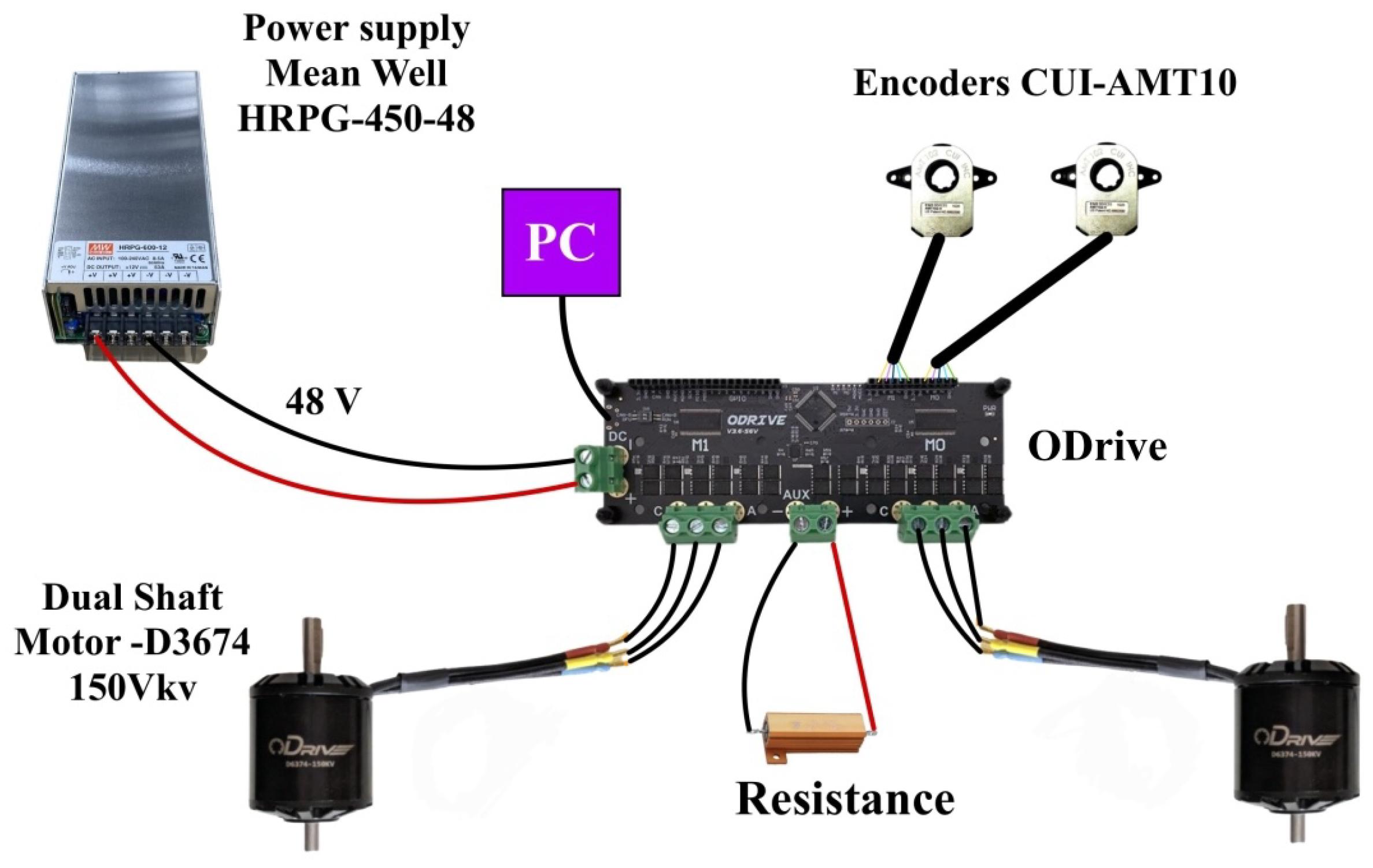
2.2.2. Electronic Architecture
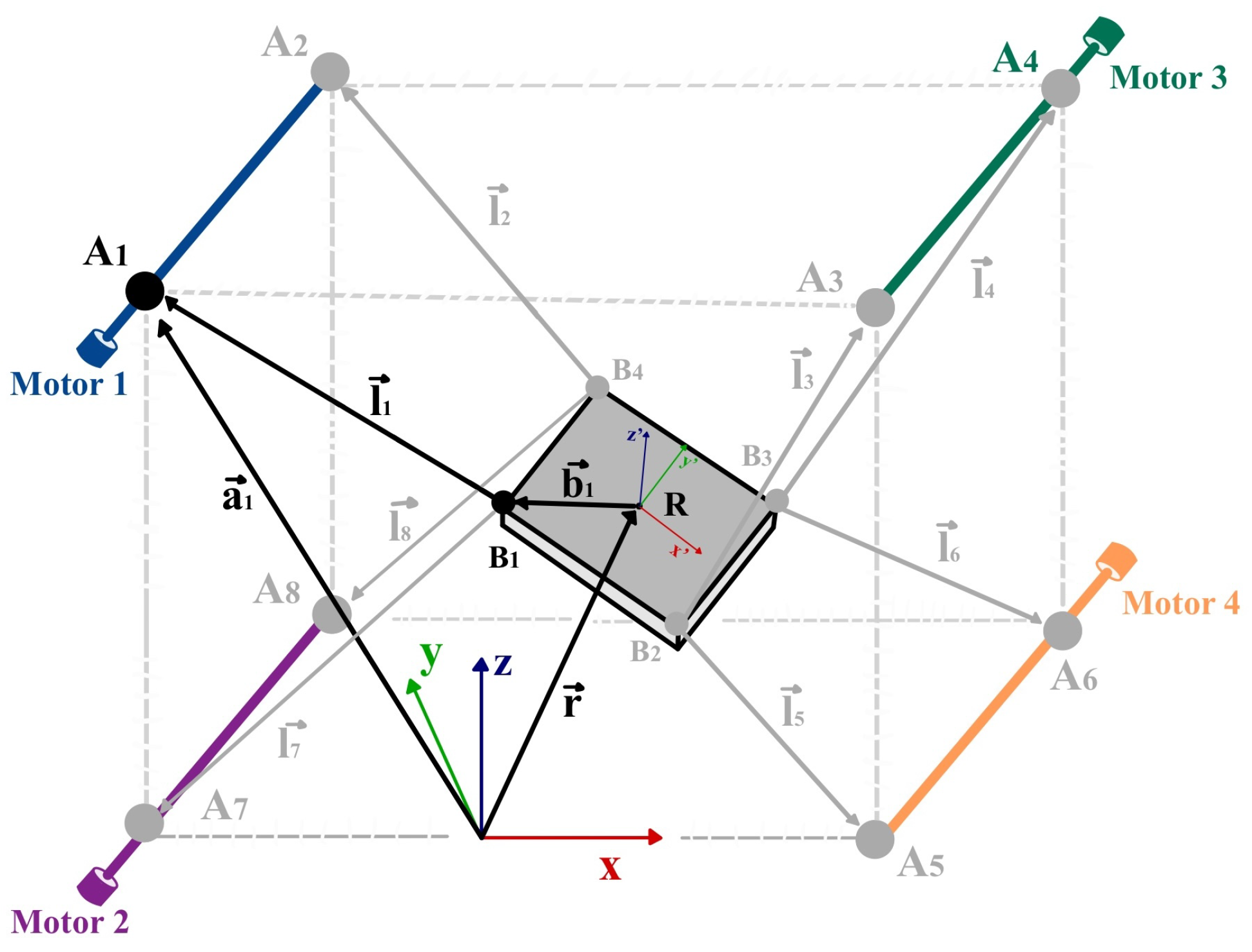
2.2.3. Kinematic Model
Inverse Kinematics
Forward Kinematics
2.2.4. Control System
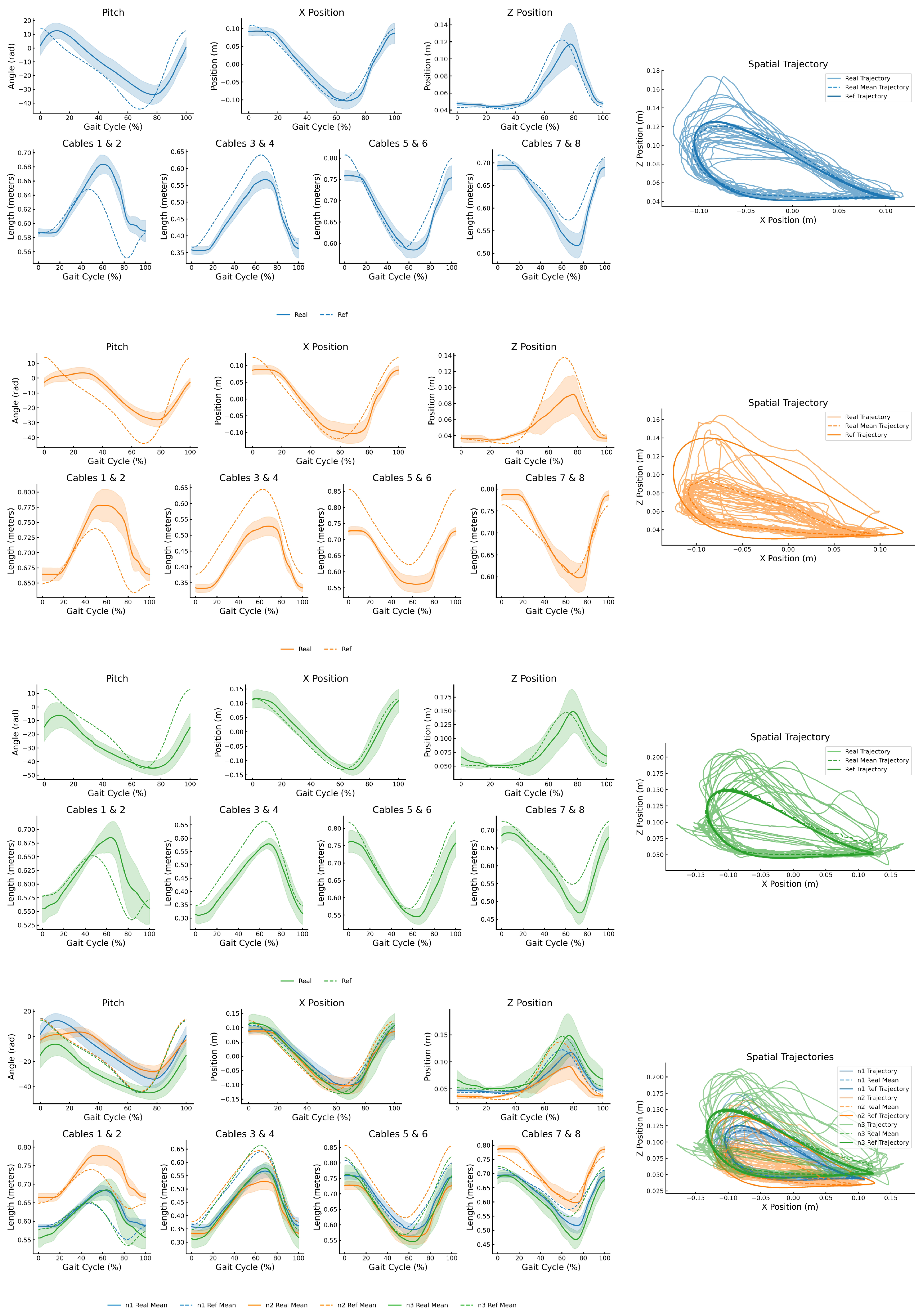
3. Results
- Participant N1: A 4-year-old child (mass: 17 kg; height: 1.06 m), classified as Level III on the Gross Motor Function Classification System (GMFCS) [49]. This level indicates that the child walks using a hand-held mobility device and requires assistive equipment (e.g., walker or crutches), particularly for outdoor ambulation.
- Participant N2: A 3-year-old child (mass: 13 kg; height: 0.96 m), classified as Level IV on the GMFCS [49]. This level indicates severely limited self-mobility; the child primarily relies on powered mobility or is transported in a manual wheelchair, especially for longer distances or community settings.
- Participant N3: A 5-year-old child (mass: 17.5 kg; height: 1.15 m), classified as Level I on the GMFCS [49], indicating that the child walks without limitations but may exhibit reduced coordination or balance during more advanced motor activities such as running or jumping.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAN | Assistance-as-Needed |
| BCI | brain–computer interface |
| BWS | body weight support |
| CAR | Centro de Automática y Robótica |
| CDPR | Cable-Driven Parallel Robot |
| CNS | central nervous system |
| CP | cerebral palsy |
| CSIC | Consejo Superior de Investigaciones Científicas |
| D2W | Discover2Walk |
| DOFs | degrees of freedom |
| FDA | Food and Drug Administration |
| GMFCS | Gross Motor Function Classification System |
| IMU | inertial measurement unit |
| MaxE | Maximum Error |
| ME | Mean Error |
| RMSE | Root Mean Square Error |
| ROM | range of motion |
| STD | Standard Deviation |
| TCorr | Pearson Correlation Coefficient for Tracking |
| UPM | Universidad Politécnica de Madrid |
References
- Krigger, K.W. Cerebral palsy: An overview. Am. Fam. Physician 2006, 73, 91–100. [Google Scholar] [PubMed]
- Peláez-Cantero, M.J.; Gallego-Gutiérrez, S.; Moreno-Medinilla, E.E.; Cordón-Martínez, A.; Madrid-Rodríguez, A.; Núñez-Cuadros, E.; Ramos-Fernández, J.M. Parálisis Cerebral en Pediatría: Problemas Asociados. Rev. Ecuat. Neurol. 2021, 30, 115–124. [Google Scholar] [CrossRef]
- Patel, A.V.; Hildebrand, J.S.; Leach, C.R.; Campbell, P.T.; Doyle, C.; Shuval, K.; Wang, Y.; Gapstur, S.M. Walking in Relation to Mortality in a Large Prospective Cohort of Older U.S. Adults. Am. J. Prev. Med. 2018, 54, 10–19. [Google Scholar] [CrossRef]
- Tonmukayakul, U.; Shih, S.T.F.; Bourke-Taylor, H.; Imms, C.; Reddihough, D.; Cox, L.; Carter, R. Systematic review of the economic impact of cerebral palsy. Res. Dev. Disabil. 2018, 80, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Sarajchi, M.; Al-Hares, M.K.; Sirlantzis, K. Wearable Lower-Limb Exoskeleton for Children with Cerebral Palsy: A Systematic Review of Mechanical Design, Actuation Type, Control Strategy, and Clinical Evaluation. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 2695–2707. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Damiano, D.L.; Park, H.S.; Gravunder, A.J.; Bulea, T.C. A Robotic Exoskeleton for Treatment of Crouch Gait in Children with Cerebral Palsy: Design and Initial Application. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Heim, A.; van Hedel, H.J.A.; Rüsch-Bohtz, C.; Sennhauser, F.H.; Heinen, F.; Künzle, C.; Dietz, V. Improvement of Walking Abilities After Robotic-Assisted Locomotion Training in Children with Cerebral Palsy. Arch. Dis. Child. 2009, 94, 615–620. [Google Scholar] [CrossRef]
- Krebs, H.I.; Palazzolo, J.J.; Dipietro, L.; Ferraro, M.; Krol, J.; Rannekleiv, K.; Volpe, B.T.; Hogan, N. Rehabilitation Robotics: Performance-Based Progressive Robot-Assisted Therapy. Auton. Robot. 2003, 15, 7–20. [Google Scholar] [CrossRef]
- Zhang, M.; Davies, T.C.; Xie, S. Effectiveness of Robot-Assisted Therapy on Ankle Rehabilitation—A Systematic Review. J. Neuroeng. Rehabil. 2013, 10, 30. [Google Scholar] [CrossRef]
- Hybart, R.L.; Ferris, D.P. Embodiment for Robotic Lower-Limb Exoskeletons: A Narrative Review. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 657–678. [Google Scholar] [CrossRef]
- Chen, L.; Zhou, D.; Leng, Y. A Systematic Review on Rigid Exoskeleton Robot Design for Wearing Comfort: Joint Self-Alignment, Attachment Interface, and Structure Customization. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 3815–3840. [Google Scholar] [CrossRef] [PubMed]
- Delgado, E.; Cumplido, C.; Ramos, J.; Garcés, E.; Puyuelo, G.; Plaza, A.; Hernández, M.; Gutiérrez, A.; Taverner, T.; Destarac, M.A.; et al. ATLAS2030 Pediatric Gait Exoskeleton: Changes on Range of Motion, Strength and Spasticity in Children with Cerebral Palsy. A Case Series Study. Front. Pediatr. 2021, 9, 753226. [Google Scholar] [CrossRef]
- Castro, P.; Martí, M.; Oliván-Blázquez, B.; Boñar, N.; García, V.; Gascón-Santos, S.; Panzano, A.; Vela, S.; Tajadura, S.; Peña, A.; et al. Benefits of Robotic Gait Assistance with ATLAS 2030 in Children with Cerebral Palsy. Front. Pediatr. 2024, 12, 1398044. [Google Scholar] [CrossRef] [PubMed]
- Erdogan-Uçar, D.; Paker, N.; Bugdaycı, D. Lokomat: A Therapeutic Chance for Patients with Chronic Hemiplegia. NeuroRehabilitation 2014, 34, 447–453. [Google Scholar] [CrossRef]
- Wu, L.; Xu, G.; Wu, Q. The Effect of the Lokomat Robotic-Orthosis System on Lower Extremity Rehabilitation in Patients with Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2023, 14, 1260652. [Google Scholar] [CrossRef]
- Blazkiewicz, M.; Hadamus, A. Assessing the Efficacy of Lokomat Training in Pediatric Physiotherapy for Cerebral Palsy: A Progress Evaluation. J. Clin. Med. 2024, 13, 6417. [Google Scholar] [CrossRef]
- Morris, L.; Diteesawat, R.S.; Rahman, N.; Turton, A.; Cramp, M.; Rossiter, J. The State-of-the-Art of Soft Robotics to Assist Mobility: A Review of Physiotherapist and Patient Identified Limitations of Current Lower-Limb Exoskeletons and the Potential Soft-Robotic Solutions. J. Neuroeng. Rehabil. 2023, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.A.; Font-Llagunes, J.M. Lower-Limb Exosuits for Rehabilitation or Assistance of Human Movement: A Systematic Review. Appl. Sci. 2021, 11, 8743. [Google Scholar] [CrossRef]
- Siviy, C.; Baker, L.M.; Quinlivan, B.T.; Porciuncula, F.; Swaminathan, K.; Awad, L.N.; Walsh, C.J. Opportunities and Challenges in the Development of Exoskeletons for Locomotor Assistance. Nat. Biomed. Eng. 2023, 7, 456–472. [Google Scholar] [CrossRef]
- Kóra, S.; Bíró, A.; Prontvai, N.; Androsics, M.; Drotár, I.; Prukner, P.; Haidegger, T.; Széphelyi, K.; Tollár, J. Investigation of the Effectiveness of the Robotic ReStore Soft Exoskeleton in the Development of Early Mobilization, Walking, and Coordination of Stroke Patients: A Randomized Clinical Trial. Robotics 2024, 13, 44. [Google Scholar] [CrossRef]
- Chandran, V.D.; Nam, S.; Hexner, D.; Bauman, W.A.; Pal, S. Comparison of the Dynamics of Exoskeletal-Assisted and Unassisted Locomotion in an FDA-Approved Lower Extremity Device: Controlled Experiments and Development of a Subject-Specific Virtual Simulator. PLoS ONE 2023, 18, e0270078. [Google Scholar] [CrossRef] [PubMed]
- Awad, L.N.; Esquenazi, A.; Francisco, G.E.; Nolan, K.J.; Jayaraman, A. The ReWalk ReStore™ Soft Robotic Exosuit: A Multi-Site Clinical Trial of the Safety, Reliability, and Feasibility of Exosuit-Augmented Post-Stroke Gait Rehabilitation. J. Neuroeng. Rehabil. 2020, 17, 80. [Google Scholar] [CrossRef] [PubMed]
- Sanjuan, J.D.; Castillo, A.D.; Padilla, M.A.; Quintero, M.C.; Gutierrez, E.E.; Sampayo, I.P.; Hernandez, J.R.; Rahman, M.H. Cable Driven Exoskeleton for Upper-Limb Rehabilitation: A Design Review. Robot. Auton. Syst. 2020, 126, 103445. [Google Scholar] [CrossRef]
- Zhang, F.; Fu, Y.; Yang, L.; Fu, Y. A Novel Cable Configuration Method for Fully-Actuated Parallel Cable-Driven Systems: Application in a Shoulder Rehabilitation Exoskeleton. Mech. Mach. Theory 2024, 199, 105693. [Google Scholar] [CrossRef]
- Gonçalves, R.S.; Alves, T.; Carbone, G.; Ceccarelli, M. Cable-Driven Robots in Physical Rehabilitation: From Theory to Practice. In Handbook of Research on Advancements in Robotics and Mechatronics; IGI Global: Hershey, PA, USA, 2020; pp. 52–96. [Google Scholar] [CrossRef]
- Lee, S.H.; Park, G.; Cho, D.Y.; Kim, H.Y.; Lee, J.Y.; Kim, S.; Park, S.B.; Shin, J.H. Comparisons Between End-Effector and Exoskeleton Rehabilitation Robots Regarding Upper Extremity Function Among Chronic Stroke Patients with Moderate-to-Severe Upper Limb Impairment. Sci. Rep. 2020, 10, 1806. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; van Wegen, E.E.; Meskers, C.G.; Kwakkel, G. Effects of Robot-Assisted Therapy for the Upper Limb After Stroke. Neurorehabilit. Neural Repair 2017, 31, 107–121. [Google Scholar] [CrossRef]
- Cui, X.; Chen, W.; Jin, X.; Agrawal, S.K. Design of a 7-DOF Cable-Driven Arm Exoskeleton (CAREX-7) and a Controller for Dexterous Motion Training or Assistance. IEEE/ASME Trans. Mechatronics 2017, 22, 161–172. [Google Scholar] [CrossRef]
- Jones, C.L.; Wang, F.; Morrison, R.; Sarkar, N.; Kamper, D.G. Design and Development of the Cable Actuated Finger Exoskeleton for Hand Rehabilitation Following Stroke. Ieee/Asme Trans. Mechatronics 2014, 19, 131–140. [Google Scholar] [CrossRef]
- Germanotta, M.; Guerrini, A.; Siotto, M.; Fasano, A.; Cipollini, V.; Cortellini, L.; Pavan, A.; Insalaco, S.; Antonacci, E.; Ruco, E.; et al. Malnutrition Diagnosis and Food Consumption in Subacute Post-Stroke Patients During Rehabilitation. Nutrients 2024, 16, 3589. [Google Scholar] [CrossRef]
- Aprile, I.G.; Fasano, A.; Pavan, A.; Guerrini, A.; Antonacci, E.; Cipollini, V.; Germanotta, M. Robotic-Assisted Rehabilitation of the Upper Limb After Stroke: The Role of the Diego System. Neurorehabilitation 2024, 54, 367–380. [Google Scholar] [CrossRef]
- Barbosa, A.M.; Carvalho, J.C.M.; Gonçalves, R.S. Cable-Driven Lower Limb Rehabilitation Robot. J. Braz. Soc. Mech. Sci. Eng. 2018, 40, 245. [Google Scholar] [CrossRef]
- Li, X.; Zhang, W.; Chen, H.; Wang, Y.; Liu, J.; Yang, Y. Design and Development of a New Cable-Driven Parallel Robot for Waist Rehabilitation. J. Mech. Robot. 2024, 16, 021008. [Google Scholar] [CrossRef]
- Huo, Y.; Khan, M.N.; Shao, Z.F.; Pan, Y. Development of a novel cable-driven parallel robot for full-cycle ankle rehabilitation. Mechatronics 2024, 101, 103210. [Google Scholar] [CrossRef]
- Prasad, R.; El-Rich, M.; Awad, M.I.; Agrawal, S.K.; Khalaf, K. Bi-Planar Trajectory Tracking with a Novel 3DOF Cable Driven Lower Limb Rehabilitation Exoskeleton (C-LREX). Sensors 2023, 23, 1677. [Google Scholar] [CrossRef] [PubMed]
- Prasad, R.; El-Rich, M.; Awad, M.I.; Kim, J.; Khalaf, K. Muscle-inspired bi-planar cable routing: A novel framework for designing cable driven lower limb rehabilitation exoskeletons (C-LREX). Sci. Rep. 2024, 14, 5158. [Google Scholar] [CrossRef]
- Wu, M.; Hornby, T.G.; Landry, J.M.; Roth, H.; Schmit, B.D. A cable-driven locomotor training system for restoration of gait in human SCI. Gait Posture 2011, 33, 256–260. [Google Scholar] [CrossRef]
- Wu, M.; Landry, J.M.; Yen, S.C.; Schmit, B.D.; Hornby, T.G.; Rafferty, M. A novel cable-driven robotic training improves locomotor function in individuals post-stroke. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 8539–8542. [Google Scholar] [CrossRef]
- Dellibarda, I.; Romero-Sorozabal, P.; Delgado-Oleas, G.; Gutiérrez, Á.; Muñoz, J.; Rocon, E. A Cable-Driven Exoskeleton to Control Ankle Mobility During Gait in Children with Cerebral Palsy. In Proceedings of the 2024 7th Iberian Robotics Conference (ROBOT), Madrid, Spain, 6–8 November 2024; pp. 1–6. [Google Scholar] [CrossRef]
- Romero-Sorozabal, P.; Delgado-Oleas, G.; Laudanski, A.F.; Gutiérrez, Á.; Rocon, E. Discover2Walk: A Cable-Driven Robotic Platform to Promote Gait in Pediatric Population. In Proceedings of the 2024 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Madrid, Spain, 14–18 October 2024. [Google Scholar]
- Delgado-Oleas, G.; Romero-Sorozabal, P.; Lora-Millan, J.; Gutierrez, Á.; Rocon, E. Bioinspired Hierarchical Electronic Architecture for Robotic Locomotion Assistance: Application in Exoskeletons. IEEE Access 2023, 11, 131610–131622. [Google Scholar] [CrossRef]
- Romero-Sorozabal, P.; Delgado-Oleas, G.; Gutiérrez, Á.; Rocon, E. Individualized Three-Dimensional Gait Pattern Generator for Lower Limbs Rehabilitation Robots. In Proceedings of the 2023 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Detroit, MI, USA, 1–5 October 2023. [Google Scholar]
- Lerma Lara, S.; del Castillo, M.D.; Serrano, J.I.; Rocon, E.; Raya, R.; Caballero, I. EEG Control of Gait in Children with Cerebral Palsy: Preliminary Data for the Construction of a Brain-Computer Interface. Gait Posture 2015, 42, S42. [Google Scholar] [CrossRef]
- Thevenon, A.; Gabrielli, F.; Lepvrier, J.; Faupin, A.; Allart, E.; Tiffreau, V.; Wieczorek, V. Collection of Normative Data for Spatial and Temporal Gait Parameters in a Sample of French Children Aged Between 6 and 12. Ann. Phys. Rehabil. Med. 2015, 58, 139–144. [Google Scholar] [CrossRef]
- Pott, A. Cable-Driven Parallel Robots: Theory and Application, 1st ed.; Springer Tracts in Advanced Robotics; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar] [CrossRef]
- Emken, J.L.; Benitez, R.; Reinkensmeyer, D.J. Human-Robot Cooperative Movement Training: Learning a Novel Sensory Motor Transformation during Walking with Robotic Assistance-as-Needed. J. Neuroeng. Rehabil. 2007, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Pehlivan, A.U.; Losey, D.P.; O’Malley, M.K. Minimal Assist-as-Needed Controller for Upper Limb Robotic Rehabilitation. IEEE Trans. Robot. 2016, 32, 113–124. [Google Scholar] [CrossRef]
- Carmichael, M.G.; Liu, D. Admittance Control Scheme for Implementing Model-Based Assistance-as-Needed on a Robot. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 870–873. [Google Scholar] [CrossRef]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Burdet, E.; Osu, R.; Franklin, D.W.; Milner, T.E.; Kawato, M. The Central Nervous System Stabilizes Unstable Dynamics by Learning Optimal Impedance. Nature 2001, 414, 446–449. [Google Scholar] [CrossRef]
- Yang, C.; Ganesh, G.; Haddadin, S.; Parusel, S.; Albu-Schaeffer, A.; Burdet, E. Human-like Adaptation of Force and Impedance in Stable and Unstable Interactions. IEEE Trans. Robot. 2011, 27, 918–930. [Google Scholar] [CrossRef]
- Tian, Y.; Guo, Y.; Wang, H.; Caldwell, D.G. Training task planning-based adaptive assist-as-needed control for upper limb exoskeleton using neural network state observer. Neural Comput. Appl. 2024, 36, 16037–16055. [Google Scholar] [CrossRef]
- Afschrift, M.; van Asseldonk, E.; van Mierlo, M.; Bayon, C.; Keemink, A.; D’Hondt, L.; van der Kooij, H.; Groote, F.D. Assisting walking balance using a bio-inspired exoskeleton controller. J. Neuroeng. Rehabil. 2023, 20, 82. [Google Scholar] [CrossRef]
- Almeida, J.F.; Santos, C.P. A Review on Bio-Inspired Control Strategies for Wearable Robotic Devices. SSRN Electron. J. 2024. Available online: https://ssrn.com/abstract=4895828 (accessed on 8 July 2025).
- Dellibarda Varela, I.; Romero-Sorozabal, P.; Delgado-Oleas, G.; Gutiérrez, Á.; Muñoz, J.; Rocon, E. Implementación y control de un exoesqueleto basado en estructura de cables para la asistencia de tobillo durante la marcha en niños con parálisis cerebral. In Proceedings of the CASEIB, Sevilla, Spain, 13–15 November 2024; pp. 1–10. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Part | Diameter (mm) | Width (mm) | Height (mm) |
|---|---|---|---|
| Motor Housing | 75 | 80 | 113 |
| Motor | 63 | 120 | 63 |
| Motor Cover | 75 | 32 | 113 |
| Drum Cover | 45 | 4 | 45 |
| Drum | 17 | 22 | 45 |
| Drum Housing | 55 | 35 | 55 |
| Bearing | 35 | 10 | 35 |
| Bearing Arm | 55 | 15 | 58 |
| Axis | 17 | 180 | 17 |
| Union Arm | - | 16 | 52 |
| Participant N1 | Participant N2 | Participant N3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Metric | X (mm) | Z (mm) | Pitch (°) | X (mm) | Z (mm) | Pitch (°) | X (mm) | Z (mm) | Pitch (°) |
| Steps | 31 Steps | 39 Steps | 24 Steps | ||||||
| ME | 0.36 | −1.24 | 3.95 | −3.51 | −11.65 | 4.45 | 5.15 | 0.74 | −13.62 |
| STD | 14.32 | 10.03 | 10.53 | 27.62 | 19.52 | 12.36 | 19.54 | 14.03 | 9.86 |
| RMSE | 14.32 | 10.11 | 11.24 | 27.84 | 22.73 | 13.13 | 20.21 | 14.05 | 16.81 |
| MaxE | 28.11 | 24.91 | 18.29 | 51.36 | 53.45 | 18.72 | 28.11 | 30.02 | 32.84 |
| TCorr | 0.98 | 0.94 | 0.83 | 0.95 | 0.98 | 0.76 | 0.98 | 0.92 | 0.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dellibarda Varela, I.; Romero-Sorozabal, P.; Delgado-Oleas, G.; Muñoz, J.; Gutiérrez, Á.; Rocon, E. Cable-Driven Exoskeleton for Ankle Rehabilitation in Children with Cerebral Palsy. Appl. Sci. 2025, 15, 7817. https://doi.org/10.3390/app15147817
Dellibarda Varela I, Romero-Sorozabal P, Delgado-Oleas G, Muñoz J, Gutiérrez Á, Rocon E. Cable-Driven Exoskeleton for Ankle Rehabilitation in Children with Cerebral Palsy. Applied Sciences. 2025; 15(14):7817. https://doi.org/10.3390/app15147817
Chicago/Turabian StyleDellibarda Varela, Iñaki, Pablo Romero-Sorozabal, Gabriel Delgado-Oleas, Jorge Muñoz, Álvaro Gutiérrez, and Eduardo Rocon. 2025. "Cable-Driven Exoskeleton for Ankle Rehabilitation in Children with Cerebral Palsy" Applied Sciences 15, no. 14: 7817. https://doi.org/10.3390/app15147817
APA StyleDellibarda Varela, I., Romero-Sorozabal, P., Delgado-Oleas, G., Muñoz, J., Gutiérrez, Á., & Rocon, E. (2025). Cable-Driven Exoskeleton for Ankle Rehabilitation in Children with Cerebral Palsy. Applied Sciences, 15(14), 7817. https://doi.org/10.3390/app15147817