Abstract
With the growing use of high-intensity LED units in orthodontics, the effect of ultra-fast curing protocols on polymerization efficiency remains unclear. This study aimed to evaluate the influence of conventional and rapid high-intensity light curing protocols on the degree of conversion (DC) of orthodontic adhesive systems. Three commercially available materials were tested under two conditions, without bracket interference (control group, CG) and with a metal bracket present during curing (metal bracket group, MBG). Two light-curing protocols were employed: conventional curing, using two consecutive 10 s exposures at 1100 mW/cm2, and rapid curing, with two consecutive 3 s exposures at 2900 mW/cm2. The DC was assessed via Fourier-transform infrared (FTIR) spectroscopy at short-term intervals (2, 6, and 10 min) and after 24 h. The results showed that rapid high-intensity curing yielded significantly lower DC values at both the short term and 24 h period compared to the conventional protocol. Short-term DC values ranged from 44.4% to 64.4% for conventional curing and from 43.0% to 60.0% for rapid curing. At 24 h, DC values increased for all materials, reaching 54.4–82.8% in the conventional group and 49.7–81.4% in the rapid curing group. The largest difference in DC values between curing protocols was observed in the MBG, with reductions of up to 5.9% (short-term) and 4.7% (24 h). The 24 h DC values were mostly material-dependent, while external factors (curing protocol and the presence of a bracket) had more impact on the short-term DC values.
1. Introduction
Ultra-fast polymerization (3 s) with light curing units (LCUs) capable of producing a high radiant exitance of 3000 mW/cm2 can accelerate the clinical procedure of bonding [1,2], making it more comfortable for the patient and saving time for the clinician. Today, the development of high-power light emitting diode (LED) chips has enabled progressively higher radiant exitance (up to 3000 mW/cm2) in modern LCUs [1,3]. LED technology is now the most used method for light curing of orthodontic adhesive systems for bracket bonding [1,2]. Compared to halogen curing units, LED LCUs achieve successful clinical bonding in a shorter curing time [2,4,5].
Polymerization in light-cured dental resin composites depends on the total energy received [6,7,8]. Total energy, i.e., radiant exposure or energy density (J/cm2), is equal to radiant exitance or power density (mW/cm2) multiplied by exposure time (s) [7,9,10]. The rapid polymerization protocol, using a very short (3 s) curing time, is based on the concept of “exposure reciprocity,” that is, the higher the light intensity of the LCU, the less time is needed for polymerization, given that the total delivered energy remains the same [1,4,5]. The higher the light intensity, the more photons are emitted, activating a higher amount of photoinitiator molecules and generating more free radicals, ensuring a faster polymerization reaction [11]. The degree of conversion (DC) is a measure of the efficiency of light curing, representing the percentage of monomer double bonds (C=C) that are converted into single bonds (C-C) during polymerization [12,13,14,15,16]. Higher DC values are associated with better mechanical and aesthetic properties as well as biocompatibility [14,17], although the relationship is not always linear [12,18]. Even though rapid high-intensity polymerization with modern LCUs enables delivering the same amount of total energy as with conventional curing by adjusting the curing unit output and curing time (the “reciprocity law”), previous studies [10,19,20,21,22] have demonstrated that at high radiant exitances (above 1000 mW/cm2), the polymerization reaction becomes qualitatively different, leading to different polymer structures, affecting chain length and crosslink density, compared to that formed under slower, more gradual polymerization [23].
The concept of rapid polymerization has been controversial and questioned for composites incorporating Norrish Type II photoinitiator systems like camphorquinone combined with a tertiary amine, and it was assumed to be achievable only for materials using Norrish Type I photoinitiators (e.g., Lucirin-TPO) [1]. Some material properties, like DC and other mechanical properties (like flexural strength and modulus), may be adversely affected by rapid polymerization [24]. Faster polymerization rates have been shown to hinder the propagation of the reaction, as a high number of activated free radicals terminate each other in the process called bimolecular termination, preventing further monomer activation [19,25,26]. This can result in lower final DC values, as well as a more heterogeneous polymer network with unreacted monomers trapped inside [27]. Although the adverse biological effects of orthodontic adhesive systems have not been as extensively investigated as those of restorative composites [28], prior studies investigating cytotoxicity of orthodontic adhesive systems [18,27] showed that unreacted monomers could have adverse biological effects, especially considering the long exposure time over the duration of orthodontic therapy, which is typically 1.5–2 years. Inadequate polymerization of the orthodontic adhesive layer beneath brackets can facilitate the diffusion of cytotoxic components (resin components, like Bis-GMA and TEGDMA) into the enamel, dentin, and pulp tissues [18,27].
There are some resin-based dental composites on the market that are advertised specifically for rapid high-intensity light curing [1]. These materials are intended for restorative (not orthodontic) applications and their composition is modified by adding reversible addition-fragmentation chain transfer (RAFT) agents to an organic matrix [1]. The DC values of these materials were shown to be comparable to those of conventional composites and not affected by curing light intensity (high intensity or conventional) [13]. To the best of our knowledge, RAFT polymerization is currently used only in restorative composites from a specific manufacturer and has not yet been implemented in orthodontic adhesives.
Resin-based orthodontic adhesive systems are the most widely used materials for bonding brackets [2,6,14]. Since bracket bonding is a clinically sensitive and time-consuming procedure [5], there is a need to simplify this process and to reduce chair time [23,29,30]. As a result, practitioners may be inclined to use rapid (3 s) light curing, originally introduced as an option for restorative resin composites, as a time-saving measure. Additionally, light curing of orthodontic adhesive systems is complicated by the presence of a non-transparent bracket material [9]. The effectiveness of light curing, represented as DC of these materials, is affected by the presence of brackets. DC values increase over time to a material-dependent extent due to the continuation of post-cure polymerization, but this increase is typically unable to fully compensate for an initially lower DC value [31].
Several studies have examined the effect of light curing intensity on the shear bond strength of orthodontic brackets [32,33]. While some found no significant difference in bond strength between conventional and rapid high-intensity curing [33], others concluded that reducing the curing time to 3 s significantly lowered bond strength [32]. A lower DC value can influence the bond strength between the adhesive and enamel, affecting the risk of enamel damage during bracket debonding and the adhesive clean-up process [34]. Ward et al. [2] found no significant differences in the percentage of bonding failures when using a 3200 mW/cm2 LED light for 6 s compared to a 1200 mW/cm2 LED light for 20 s, suggesting that rapid high-intensity curing may be a clinically viable procedure. Previous studies [30,35,36] confirmed the positive influence of extending the curing time and intensity on the DC of orthodontic adhesive systems. However, concerns have been raised about the efficacy of high irradiance delivered over a short duration in achieving adequate polymerization [1]. To our knowledge, research on the effects of rapid high-intensity curing on the DC of orthodontic adhesive systems, especially in the presence of bracket material, is scarce.
Although some studies [2,35] showed that rapid high-intensity curing provides clinically acceptable bond strength of orthodontic adhesive systems, research on restorative composites indicates that it may alter polymerization kinetics and compromise mechanical properties [3,14]. Also, orthodontic adhesive systems lack specific compositional adjustments specifically designed for rapid high-intensity curing. Therefore, the present study compared the short-term and 24 h post-cure DC values of orthodontic adhesive systems, both in the absence of a bracket (control group) and under a metal bracket, using two light curing protocols: rapid high intensity and conventional. The null hypotheses were: (1) there is no significant difference in the DC of the tested orthodontic adhesive systems between the conventional and rapid high-intensity curing protocols; and (2) the presence of a metal bracket does not influence the DC of the tested orthodontic adhesive systems.
2. Materials and Methods
Three commercially available resin-based light-cured orthodontic adhesive systems, Enlight (Ormco, Brea, CA, USA), Heliosit (Ivoclar Vivadent, Schaan, Liechtenstein), and Transbond XT (3M Unitek, Monrovia, CA, USA) were tested in two groups according to the presence of a bracket during light curing: the control group without a bracket (CG) and the metal bracket group (MBG) in which Equilibrium 2 (Dentaurum, Ispringen, Germany) brackets were used (Figure 1). The compositions of the investigated orthodontic adhesives are presented in Table 1.
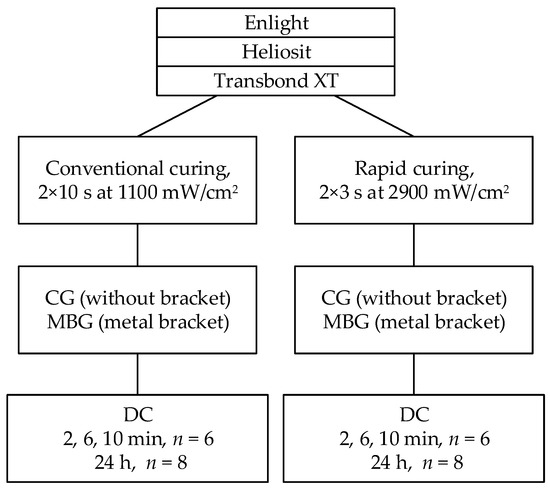
Figure 1.
Study design.

Table 1.
Composition of resin-based orthodontic adhesive systems tested in this study.
According to a power analysis based on a previous study [31], 36 samples were prepared for short-term measurements (3 materials × 2 curing protocols × n = 6 per experimental group) and 48 samples were prepared for for 24 h DC measurements (3 materials × 2 curing protocols × n = 8 per experimental group).
2.1. Curing Protocols, Sample Preparation, and DC Measurements
The specimens were irradiated using an LED curing unit (Bluephase PowerCure; Ivoclar, Schaan, Liechtenstein). Two curing protocols were applied: (1) a conventional protocol consisting of two consecutive 10 s exposures at 1100 mW/cm2 (radiant exposure: 22 J/cm2) and (2) a rapid high-intensity protocol involving two consecutive 3 s exposures at 2900 mW/cm2 (radiant exposure: 17.4 J/cm2). FTIR-ATR spectroscopy was used to determine DC at 2, 6, 10 min, and 24 h.
Samples in the CG were cured directly above the material.
Samples in the MBG were cured for 10 s from the mesial side and 10 s from the distal side of the bracket for conventional curing, and 3 s mesial and 3 s distal to the bracket for rapid curing, under a 45° angle [23].
Sample preparation and DC measurements were carried out following the methodology described in a previous study [31].
For short-term DC, a thin layer (~0.2 mm) of unpolymerized orthodontic adhesive, approximately matching the bracket base size (4 × 4 mm), was applied to the ATR crystal. A polyethylene terephthalate (PET) foil was placed over the sample, followed by positioning a metal bracket with gentle pressure to replicate clinically relevant thickness. An upper incisor bracket was selected due to its flat base. Excess material was removed with a dental probe. For CG samples, the bracket was removed before curing, while for MBG samples, the bracket remained in place.
For 24 h DC, the unpolymerized orthodontic adhesive was placed on a PET foil on top of a microscope slide, with two laterally positioned cover glasses, to attain a ~0.2 mm thickness and planar dimensions of 4 × 4 mm. A second PET foil was placed over the sample and pressed with a glass slide, which was then removed. For MBG samples, a bracket was placed on the upper PET foil before curing. After curing, the PET foil (and bracket, for MBG) was removed, and the samples were gently detached, placed in dark boxes in an incubator at 37 °C, and stored for 24 h. The surface of the specimen opposite to the light-exposed side was positioned on the ATR accessory and pressed using a load-controlled spectrometer press. FTIR spectra were collected as described below. Spectra of unpolymerized materials (n = 5) were also recorded for use in DC calculations.
Short-term and 24 h DC were measured using Fourier-transform infrared (FTIR) spectroscopy coupled to an attenuated total reflectance (ATR) module (Nicolet iS50, Thermo Fisher, Madison, WI, USA). Spectra covering 500–3500 cm−1 were collected at a resolution of 8 cm−1 for short-term measurements and 4 cm−1 for 24 h measurements. For the short-term measurements, two scans were collected at a rate of two spectra per second, starting when the light curing unit was activated and continuing for 10 min. For the 24 h measurements, a single spectrum comprising 30 co-added scans was acquired 24 h after curing. A new background spectrum was recorded before each specimen.
DC was calculated from the change in the ratio of the aliphatic C=C absorption at 1638 cm−1 to that of the aromatic C=C reference at 1608 cm−1, comparing pre- and post-polymerization values, using the equation described in [37]:
2.2. Statistical Analysis
Normality of data distribution was assessed using the Shapiro–Wilk test, and homogeneity of variances was verified using Levene’s test. For short-term DC data, a four-way ANOVA was conducted to examine the effects of “Material,” “Bracket,” “Curing protocol,” and “Time point.” For the 24 h DC values, a three-way ANOVA including “Material,” “Bracket,” and “Curing protocol” was performed, as only one time point was available. Effect sizes were reported using partial eta-squared (η2). When significant main effects or interactions were found, one-way ANOVA was used to compare conventional and rapid light curing within fixed levels of the other factors. All analyses were performed using SPSS (version 26.0; IBM Corp., Armonk, NY, USA), with a significance threshold of p < 0.05.
3. Results
Short-term DC values (%) obtained through real-time kinetics measurements using the conventional curing protocol ranged from 50.5 to 64.4 in the CG and from 44.4 to 55.9 in the MBG, with the highest value observed for Enlight (10 min) in the CG and the lowest for Enlight (2 min) in the MBG. Under the rapid curing protocol, short-term DC values were significantly lower (p < 0.001) across all materials in both groups, ranging from 45.8 to 60.0 in the CG and from 43.0 to 50.1 in the MBG (Figure 2). The greatest differences in short-term DC under rapid curing, compared to conventional curing, were observed for Enlight in the CG (4.4%) and Heliosit in the MBG (up to 5.9%) (Figure 3).
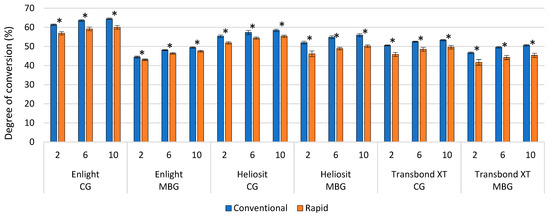
Figure 2.
DC values for Enlight, Heliosit, and Transbond XT at 2, 6, and 10 min. Statistically significant differences (p < 0.05) between curing protocols are indicated with asterisks (*).
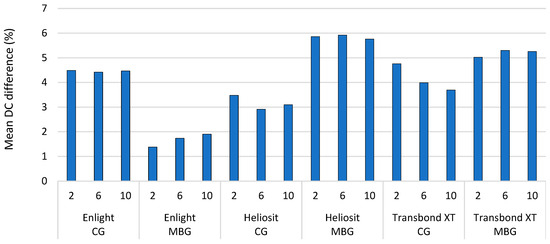
Figure 3.
Mean differences for Enlight, Heliosit, and Transbond XT between conventional and rapid curing protocol at 2, 6, and 10 min.
The 24 h DC values were consistently higher than the short-term values for all materials and protocols (Figure 4). For the conventional curing protocol, the 24 h DC values ranged from 56.7 to 82.8 in the CG and from 54.4 to 82.7 in the MBG, with Enlight showing the highest values in both groups. Rapid curing resulted in lower 24 h DC values across all materials (p = 0.001–0.012), except for Transbond XT in the CG, where no significant difference was observed (p = 0.244). For the rapid curing protocol, the 24 h DC values ranged from 54.8 to 81.4 in the CG and from 49.7 to 79.0 in the MBG. The differences between rapid and conventional curing in the 24 h DC values were smaller than those observed in the short-term DC values, varying from 0.5% to 1.9% in the CG and from 1.7% to 4.7% in the MBG, with the greatest difference seen in Heliosit (Figure 5).
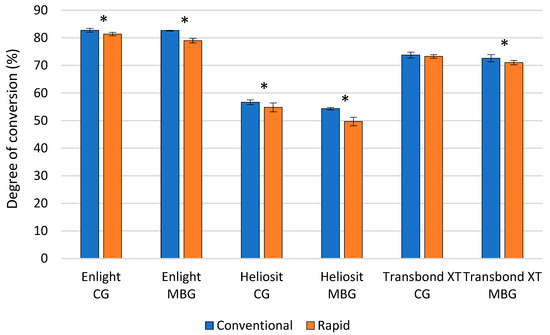
Figure 4.
DC values for Enlight, Heliosit, and Transbond XT at 24 h. Statistically significant differences (p < 0.05) between curing protocols are indicated with asterisks (*).
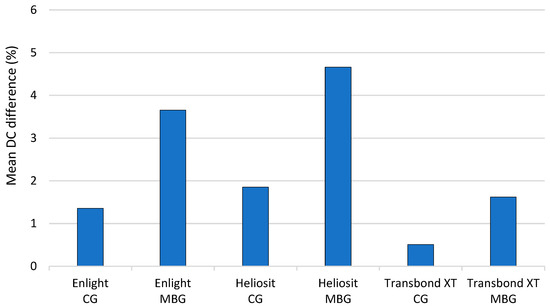
Figure 5.
Mean differences for Enlight, Heliost, and Transbond XT between conventional and rapid curing protocol at 24 h.
Rapid curing mode was associated with increased inter-sample variability for short-term measurements (Figure 6), ranging from 0.9% to 3.6%, in comparison to conventional curing, which demonstrated variability between 0.8% and 1.5%. Heliosit and Transbond XT in the MBG showed the highest levels of variability, particularly at the 2 min time point (3.1% and 3.6%, respectively).
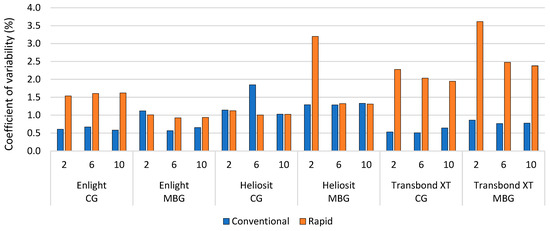
Figure 6.
Coefficient of variability within each experimental group (n = 6) for short-term DC measurements. CG: Control group, MBG: Metal bracket group.
Coefficients of variability were similar in the 24 h DC measurements, ranging from 0.8% to 1.7% for the conventional protocol and 0.8% to 1.8% for the rapid curing protocol (Figure 7).
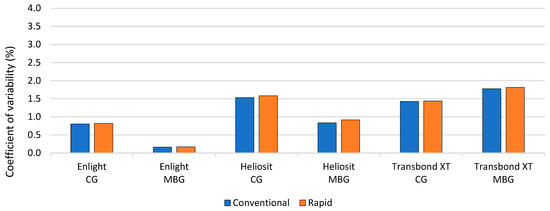
Figure 7.
Coefficient of variability within each experimental group (n = 8) for 24 h DC measurements. CG: Control group, MBG: Metal bracket group.
The partial eta-squared values describing relative effect size of the factors “Material,” “Bracket,” and “Curing protocol” for both short-term and 24 h DC and “Time point” for short-term DC are presented in Table 2 and Table 3. Partial eta-squared is a measure of effect size that quantifies the proportion of total variance in the dependent variable that is attributable to a specific factor. It reflects relative effect sizes of each factor and provides information about practical significance. This information complements the p-value (which indicates only statistical significance regardless of the effect size) by enabling evaluation of whether a statistically significant effect is also meaningful in magnitude. According to Cohen’s guidelines, η2 > 0.14 indicates a large effect. Thus, all of the investigated factors exhibited large effects on DC outcomes.
Table 2.
Partial eta-squared values describing the effect size of different factors on short-term DC values.
Table 3.
Partial eta-squared values describing the effect size of different factors on 24 h DC values.
For short-term DC values, the significance of factors was in descending order of “Bracket” > “Material” > “Curing mode” > “Time point”, and for the 24 h DC values, the order was “Material” > “Curing mode” > “Bracket.” There was significant interaction between factors “Material” ↔ “ Bracket” and “Material” ↔ “Curing mode” for both short-term and 24 h DC values, with greater impact on short-term DC values. The interaction between factors “Bracket” ↔ “Curing mode” was significant in the 24 h DC measurements, while the interaction between factors “Material” ↔ “Bracket” ↔ “Curing mode” was significant only in the short-term DC measurements.
Detailed DC data, presented as mean values and standard deviations for each experimental group, are provided in Supplementary Tables S1 and S2.
4. Discussion
This study evaluated the influence of rapid high-intensity curing on the DC of orthodontic adhesive systems. The findings confirm that rapid curing leads to lower DC values, especially under metal brackets. Material composition was the most influential factor. The “exposure reciprocity” principle did not hold at higher intensities, likely due to bimolecular termination and radical quenching.
The null hypotheses were rejected since the rapid curing protocol and presence of a metal bracket resulted in lower short-term and 24 h DC values for all materials and groups except for the 24 h DC values for Transbond XT in the CG, where both curing protocols led to statistically similar results.
The observed short-term (44.4–64.4% for conventional curing and 43.0–60.0% for rapid curing, Figure 2) and 24 h DC values (54.4–82.8% for the conventional curing protocol and 49.7–81.4% for the rapid curing protocol, Figure 4) in this study fell within the ranges reported in prior literature [14,17,31,38,39,40,41]. This consistency indicated that the polymerization efficiency observed in the present study is as expected. However, a more detailed comparison with previously published data is limited because differences in sample preparation, curing conditions, and other incompletely specified study variables can considerably influence the reported values [12,31].
Lower short-term and 24 h DC values observed with the rapid curing protocol in both groups could be attributed to lower total energy received during curing. Regardless of higher radiant exitance in rapid curing compared to conventional curing, the total energy received was lower by approximately 4600 J/cm2 (2 × 10 s × 1100 J/cm2 = 22,000 J/cm2; 2 × 3 s × 2900 J/cm2 = 17,400 J/cm2; 22,000 – 17,400 = 4600 J/cm2). These findings are in accordance with another study [23] where lower DC values were also obtained with a high-intensity curing protocol. Nevertheless, considering the very thin material layer (0.2 mm), both protocols should have provided sufficient energy for complete polymerization [6,7]. Hence, the observed differences could be attributed to the negative effects of rapid polymerization, like increased rate of bimolecular termination—a phenomenon commonly associated with high-intensity curing modes with modern LED LCUs [13]. High-intensity light activates a greater number of photoinitiator molecules and generates more free radicals, accelerating the polymerization reaction. However, the abundance of free radicals increases the likelihood of their mutual termination, thereby reducing the activation of additional monomers and ultimately lowering overall polymerization efficiency [20,21].
The conventional and rapid curing protocols resulted in lower short-term (1.3–5.9%, Figure 2) and 24 h DC values (1.7–4.7%, Figure 4) in the MBG compared to the CG. Other studies also confirmed that lower DC values obtained by curing in the presence of the bracket [23,31,42]. Indirect curing underneath a metal bracket increases the complexity of the polymerization conditions, as the presence of the bracket attenuates the curing light and lowers the total energy delivered for polymerization [9,23,39], resulting in lower DC values regardless of curing mode. Under clinical conditions, it is common to cure the orthodontic adhesive when bonding the metal bracket from two directions, occlusally/gingivally or mesially/distally, under a 45° angle [23,39]. In this study, for rapid curing, samples in the MBG were cured for 6 s, i.e., 3 s mesial and 3 s distal to the bracket. Additionally, some studies [5,9,10] reported that efficient bracket bonding could not be guaranteed unless the exposure time was more than 4 s in total, irrespective of the power density. In continuation, the factor “Bracket” had a more pronounced impact on short-term DC and the least impact on 24 h DC. This could also be explained by a lower energy received at the beginning, which resulted in fewer free radicals and activated monomers, leading to a slower rise of viscosity of the reaction medium and leaving more reactants available for post-cure DC development [31], which in turn compensated for the presence of the bracket at the beginning of the reaction.
The 24 h DC values were higher by 18.4–21.4% (Figure 3) than the corresponding short-term DC values, suggesting post-cure DC development. Post-cure DC development is typical for methacrylate resin-based dental composites [14,43]. Free radicals generated during curing remain active, allowing continued addition polymerization of monomers. Immediately after curing, the polymer network is macroscopically rigid, yet the mobility of unreacted monomers and free radicals allows for continuation of the reaction, leading to greater post-cure DC values [37]. Post-cure development could also explain the observed lesser difference in DC values due to rapid curing for the 24 h DC measurements compared to the short-term DC measurements in both groups (0.5–4.7%, Figure 5). Additionally, the samples for the 24 h DC measurements were stored in a laboratory incubator at 37 °C to mimic intraoral conditions. The exposure to simulated body temperature promotes the mobility of free radicals and monomers, sustaining the continuation of the polymerization reaction “in the dark” [44].
The viscosity of the material can also play a role in the final DC value attained by a specific material formulation [19]. Following prior literature, exposure reciprocity seems to be more valid for highly filled materials [22] like Enlight and Transbond XT. The lower sensitivity of these more highly filled materials to negative effects of bimolecular termination could be less significant, allowing them to reach DC values that are closer to those attained with conventional light curing [45]. While a high filler volume fraction may impede light transmission [16,45], small, well-distributed filler particles can enhance light scattering, improving light penetration and supporting ongoing polymerization [45,46,47]. Since light scattering increases exponentially with layer thickness [48,49], its effect is limited in the thin layers typically used for orthodontic adhesives systems. That may explain why Enlight and Transbond XT, compared to Heliosit, showed much higher 24 h DC values than at the end of the short-term measurements in both groups (Figure 2 and Figure 4). These findings are consistent with a previous study where the same observation was noted [31]. The same explanation could be offered for Transbond XT in the CG for the 24 h DC measurements where no difference was observed between curing protocols (Figure 4), suggesting the material’s ability to compensate for lower initial DC values through a more extensive post-cure DC development.
The short-term DC values for Heliosit for the conventional and rapid curing protocols were in the high-end range among all of the tested materials (Figure 2). Heliosit is a more flowable and translucent system than Enlight and Transbond XT as it has a higher monomer ratio (>85 wt%), which could promote higher initial DC values, but as polymerization progresses, fewer monomers are left for post-cure DC development, resulting in lower 24 h DC values [50]. Similar observations were made in a previous study [31] where Heliosit showed the same changes in comparisons between short-term and 24 h DC values. Furthermore, Heliosit exhibited the most pronounced difference in DC values when the curing protocol was changed, which could also be attributed to the previously discussed mechanism of accelerated monomer consumption during the initial phase of the reaction. It has been reported that curing with a higher light intensity can lead to a better crosslinking density of organic matrix, which can in turn impair the mobility of reactive species and, together with the higher rate of bimolecular termination, diminish the final extent of polymerization [3,43].
Rapid curing resulted in more variable DC values across experimental runs within the same group (coefficients of variability of 0.9–3.6%) compared to the conventional protocol in short-term DC measurements (0.8–1.5%, Figure 6), while the coefficients of variability were similar for both curing protocols within the same group for 24 h DC measurements (0.8–1.7% for the conventional protocol and 0.8–1.8% for the rapid curing protocol, Figure 7). Previous studies [51,52] reported that the early stage of polymerization tends to be significantly affected by high-intensity curing due to a rapid increase in viscosity of the reaction medium, which could result in uneven and incomplete monomer conversion. The highest variability in the second minute of short-term DC measurements for Heliosit and Transbond XT supported this finding. Additionally, Transbond XT had pronounced variability for rapid curing modes in both groups and time points of measurement compared to Heliosit and Enlight, suggesting that some materials could better compensate for the negative effects of rapid curing in the early stages of polymerization, depending on the material’s composition [52].
The analysis of the relative influences of the factors “Material,” “Curing protocol,” and “Bracket” on DC showed that the factor “Material” had a notable and similar impact on both short-term and 24 h DC values compared to other factors (Table 2 and Table 3). This indicated that the DC variability is strongly dependent on the material’s composition [53], which is not fully disclosed by the manufacturers [40] and therefore limits interpretation for relating the quantitative results with a specific compositional feature. Interestingly, the factor “Bracket” was the most influential on short-term DC values in contrast to 24 h DC values, where it was of the least significance, indicating that light attenuation and the consequent reduction in total received energy more significantly affected the early stage of polymerization. By contrast, for the 24 h DC values, apart from the factor “Material,” which ranked the highest, “Curing protocol” ranked as the second most influential factor, indicating its more significant role over time. The interaction between the factors “Material” ↔ “ Bracket” was more significant than the interaction between the factors “Material” ↔ “Curing protocol,” indicating that given the same material, the presence of the bracket had a greater effect on both DC values than the curing protocol. The interaction between the aforementioned factors was less significant for the 24 h DC values, and the difference between them was smaller, showing that the 24 h DC values were more material dependent, and that the presence of the bracket and choice of curing protocol had a similar effect. The short-term DC values appeared to be more sensitive, reflecting a greater influence of external factors such as bracket or curing protocol. While these factors also affected the 24 h DC values, they may be compensated over time due to the nature of the polymerization reaction and certain specific components within the material.
The highest difference in DC values between curing protocols was in the MBG, 5.9% for short-term DC measurements and 4.7% for 24 h measurements. Part of the difference was due to the presence of the bracket during curing. Given that the tested materials do not incorporate specific compositional adjustments that would benefit rapid polymerization, and that the obtained DC values attained using rapid high-intensity curing were significantly lower, a clinician inclined to use rapid curing protocols on modern LED LCUs can be advised to use more highly filled materials as it appears that these are less affected by negative effects of rapid polymerization. Lower DC values can lead to deterioration in material’s mechanical properties and the development of caries, and they are also associated with reduced bond strength and more frequent debonding of brackets from the tooth surface [54,55]. Although statistically significant, the clinical relevance of differences in DC < 5% remains uncertain and may not impact the clinical performance of the material to a significant extent.
Since this in vitro study was focused exclusively on DC as a fundamental parameter, its main limitations include the absence of bond strength and mechanical testing after simulated aging. These properties should be tested in a follow-up study. Since rapid light curing negatively affected DC, future studies should examine whether the small, but statistically significant, reduction in DC values observed in our study translates into meaningful reductions of mechanical properties, (flexural properties and bond strength to enamel) as well as biological properties, including elution of residual monomers and cytotoxicity.
5. Conclusions
Rapid high-intensity curing results in significantly lower DC values across most materials and conditions compared to conventional protocols. Despite these reductions, post-cure polymerization contributes to improved outcomes at 24 h. Material composition plays a dominant role, and highly filled orthodontic adhesives appear more resilient to the effects of rapid curing. Clinicians should exercise caution when applying ultra-fast curing techniques to orthodontic adhesive systems not specifically designed for them.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/app15147641/s1, Table S1: Short-term degree of conversion, presented as mean values with standard deviations in parentheses; Table S2: 24-h degree of conversion, presented as mean values with standard deviations in parentheses.
Author Contributions
Conceptualization, I.P.K. and S.M.; Data curation, I.P.K.; Formal analysis, H.M. and M.P.; Funding acquisition, Z.T.; Investigation, I.P.K.; Methodology, H.M. and M.P.; Project administration, D.M. and Z.T.; Resources, D.M., Z.T. and M.P.; Software, M.P.; Supervision, S.M., D.M., Z.T. and M.P.; Visualization, I.P.K.; Writing—original draft, I.P.K.; Writing—review & editing, S.M., H.M., D.M., Z.T. and M.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within the article and Supplementary Tables S1 and S2.
Acknowledgments
The authors would like to extend their gratitude to Vladimir Profeta for providing the materials for testing and Matija Krznar for developing an application to help calculate the degree of conversion.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DC | degree of conversion |
| LCU | light curing unit |
| LED | light emitting diode |
| RAFT | reversible addition-fragmentation chain transfer |
| PET | polyethylene terephthalate |
| FTIR | Fourier-transform infrared spectroscopy |
| ATR | attenuated total reflectance |
References
- Ilie, N.; Watts, D.C. Outcomes of Ultra-Fast (3 s) Photo-Cure in a RAFT-Modified Resin-Composite. Dent. Mater. 2020, 36, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.D.; Wolf, B.J.; Leite, L.P.; Zhou, J. Clinical Effect of Reducing Curing Times with High-Intensity LED Lights. Angle Orthod. 2015, 85, 1064–1069. [Google Scholar] [CrossRef]
- Par, M.; Marovic, D.; Attin, T.; Tarle, Z.; Tauböck, T.T. The Effect of Rapid High-Intensity Light-Curing on Micromechanical Properties of Bulk-Fill and Conventional Resin Composites. Sci. Rep. 2020, 10, 10560. [Google Scholar] [CrossRef] [PubMed]
- Lamper, T.; Steinhäuser-Andresen, S.; Huth, K.C.; Ilie, N.; Paschos, E. Does a Reduction of Polymerization Time and Bonding Steps Affect the Bond Strength of Brackets? Clin. Oral Investig. 2012, 16, 665–671. [Google Scholar] [CrossRef]
- Cerekja, E.; Cakirer, B. Effect of Short Curing Times with a High-Intensity Light-Emitting Diode or High-Power Halogen on Shear Bond Strength of Metal Brackets before and after Thermocycling. Angle Orthod. 2011, 81, 510–516. [Google Scholar] [CrossRef]
- Rahiotis, C. Degree of Cure and Monomer Leaching from Orthodontic Adhesive Resins: In Vitro and in Vivo Evidence. Semin. Orthod. 2010, 16, 266–273. [Google Scholar] [CrossRef]
- Gange, P. The Evolution of Bonding in Orthodontics. Am. J. Orthod. Dentofac. Orthop. 2015, 147, S56–S63. [Google Scholar] [CrossRef]
- Grazioli, G.; Cuevas Suárez, C.; Mederos, M.; LEON, E.; Garcia, A.; Zamarripa, E.; Piva, E. Evaluation of Irradiance and Radiant Exposure on the Polymerization and Mechanical Properties of a Resin Composite. Braz. Oral Res. 2022, 36, e082. [Google Scholar] [CrossRef]
- Mavropoulos, A.; Cattani-Lorente, M.; Krejci, I.; Staudt, C.B. Kinetics of Light-Cure Bracket Bonding: Power Density vs Exposure Duration. Am. J. Orthod. Dentofacial Orthop. 2008, 134, 543–547. [Google Scholar] [CrossRef]
- Musanje, L.; Darvell, B.W. Polymerization of Resin Composite Restorative Materials: Exposure Reciprocity. Dent. Mater. 2003, 19, 531–541. [Google Scholar] [CrossRef]
- Emami, N.; Söderholm, K.-J.M.; Berglund, L.A. Effect of Light Power Density Variations on Bulk Curing Properties of Dental Composites. J. Dent. 2003, 31, 189–196. [Google Scholar] [CrossRef]
- Carek, A.; Dukaric, K.; Miler, H.; Marovic, D.; Tarle, Z.; Par, M. Post-Cure Development of the Degree of Conversion and Mechanical Properties of Dual-Curing Resin Cements. Polymers 2022, 14, 3649. [Google Scholar] [CrossRef] [PubMed]
- Par, M.; Burrer, P.; Prskalo, K.; Schmid, S.; Schubiger, A.-L.; Marovic, D.; Tarle, Z.; Attin, T.; Tauböck, T.T. Polymerization Kinetics and Development of Polymerization Shrinkage Stress in Rapid High-Intensity Light-Curing. Polymers 2022, 14, 3296. [Google Scholar] [CrossRef]
- Çörekçi, B.; Malkoç, S.; Öztürk, B.; Gündüz, B.; Toy, E. Polymerization Capacity of Orthodontic Composites Analyzed by Fourier Transform Infrared Spectroscopy. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e299–e304. [Google Scholar] [CrossRef]
- Rueggeberg, F.A.; Hashinger, D.T.; Fairhurst, C.W. Calibration of FTIR Conversion Analysis of Contemporary Dental Resin Composites. Dent. Mater. Off. Publ. Acad. Dent. Mater. 1990, 6, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, S.; Abbasi, M.; Sadeghi Mahounak, F.; Moradi, Z. Curing Depth and Degree of Conversion of Five Bulk-Fill Composite Resins Compared to a Conventional Composite. Open Dent. J. 2019, 13, 422–429. [Google Scholar] [CrossRef]
- Arana, A.F.M.; Justus, B.; Dávila-Sánchez, A.; Sugahara, M.D.O.; Coelho, U.; Farago, P.V.; Arrais, C. Influence of Radiant Exposure Values from Two Third Generation LED Curing Units on Polymerization Profile and Microhardness of Orthodontic Composite under Ceramic and Metallic Brackets. Dent. Press J. Orthod. 2021, 26, e2119150. [Google Scholar] [CrossRef] [PubMed]
- Jagdish, N.; Padmanabhan, S.; Chitharanjan, A.B.; Revathi, J.; Palani, G.; Sambasivam, M.; Sheriff, K.; Saravanamurali, K. Cytotoxicity and Degree of Conversion of Orthodontic Adhesives. Angle Orthod. 2009, 79, 1133–1138. [Google Scholar] [CrossRef]
- Hadis, M.; Leprince, J.G.; Shortall, A.C.; Devaux, J.; Leloup, G.; Palin, W.M. High Irradiance Curing and Anomalies of Exposure Reciprocity Law in Resin-Based Materials. J. Dent. 2011, 39, 549–557. [Google Scholar] [CrossRef]
- Feng, L.; Suh, B.I. Exposure Reciprocity Law in Photopolymerization of Multi-Functional Acrylates and Methacrylates. Macromol. Chem. Phys. 2007, 208, 295–306. [Google Scholar] [CrossRef]
- Sadeghyar, A.; Watts, D.C.; Schedle, A. Limited Reciprocity in Curing Efficiency of Bulk-Fill Resin-Composites. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2020, 36, 997–1008. [Google Scholar] [CrossRef]
- Palagummi, S.V.; Hong, T.; Wang, Z.; Moon, C.K.; Chiang, M.Y.M. Resin Viscosity Determines the Condition for a Valid Exposure Reciprocity Law in Dental Composites. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2020, 36, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Faria-e-Silva, A.L.; Covell, D.A.; Ferracane, J.L.; Pfeifer, C.S. Effectiveness of High Irradiance for Short-Time Exposures on Polymerization of Composite under Metal Brackets. Angle Orthod. 2017, 87, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, M.M.; Lien, W.; Mansell, M.R.; Risk, D.L.; Savett, D.A.; Vandewalle, K.S. Effect of High-Intensity Curing Lights on the Polymerization of Bulk-Fill Composites. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2018, 34, 1531–1541. [Google Scholar] [CrossRef]
- da Silva, E.M.; Poskus, L.T.; Guimarães, J.G.A.; Barcellos, A.d.A.L.; Fellows, C.E. Influence of Light Polymerization Modes on Degree of Conversion and Crosslink Density of Dental Composites. J. Mater. Sci. Mater. Med. 2008, 19, 1027–1032. [Google Scholar] [CrossRef]
- Lang, M.; Hirner, S.; Wiesbrock, F.; Fuchs, P. A Review on Modeling Cure Kinetics and Mechanisms of Photopolymerization. Polymers 2022, 14, 2074. [Google Scholar] [CrossRef] [PubMed]
- Çörekçi, B.; Irgın, C.; Halıcıoğlu, K.; Dursun, S.; Yavuz, M. Effects of Plasma-Emulating Light-Emitting Diode (LED) versus Conventional LED on Cytotoxic Effects and Polymerization Capacity of Orthodontic Composites. Hum. Exp. Toxicol. 2014, 33, 1000–1007. [Google Scholar] [CrossRef]
- Romo-Huerta, M.J.; del Refugio Cervantes-Urenda, A.; Velasco-Neri, J.; Torres-Bugarin, O.; Valdivia, A.D.C.M. Genotoxicity Associated with Residual Monomers in Restorative Dentistry: A Systematic Review. Oral Health Prev. Dent. 2021, 19, b2081469. [Google Scholar] [CrossRef]
- Ilie, N.; Diegelmann, J. Impact of Ultra-Fast (3 s) Light-Cure on Cell Toxicity and Viscoelastic Behavior in a Dental Resin-Based Composite with RAFT-Mediated Polymerization. J. Mech. Behav. Biomed. Mater. 2021, 124, 104810. [Google Scholar] [CrossRef]
- Eliades, T. Polymerization Lamps and Photocuring in Orthodontics. Semin. Orthod. 2010, 16, 83–90. [Google Scholar] [CrossRef]
- Profeta Krznar, I.; Par, M.; Tarle, Z.; Meštrović, S. Influence of the Bracket Material on the Post-Cure Degree of Conversion of Resin-Based Orthodontic Adhesive Systems. Polymers 2024, 16, 318. [Google Scholar] [CrossRef] [PubMed]
- Almeida, L.F.; Martins, L.P.; Martins, R.P. Effects of Reducing Light-Curing Time of a High-Power LED Device on Shear Bond Strength of Brackets. J. Orofac. Orthop. Fortschritte Kieferorthopädie 2018, 79, 352–358. [Google Scholar] [CrossRef]
- Mohammed, O.K.; Younis, M.T.; Dawood, A.E. The Effect of Light Curing Time and Intensity on the Bond Strength and Fracture Resistance of Orthodontic Adhesive. J. Dent. Res. Dent. Clin. Dent. Prospect. 2023, 17, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Paolone, G.; Mandurino, M.; Baldani, S.; Paolone, M.G.; Goracci, C.; Scolavino, S.; Gherlone, E.; Cantatore, G.; Gastaldi, G. Quantitative Volumetric Enamel Loss after Orthodontic Debracketing/Debonding and Clean-Up Procedures: A Systematic Review. Appl. Sci. 2023, 13, 5369. [Google Scholar] [CrossRef]
- Kauppi, M.R.; Combe, E.C. Polymerization of Orthodontic Adhesives Using Modern High-Intensity Visible Curing Lights. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Niepraschk, M.; Rahiotis, C.; Bradley, T.G.; Eliades, T.; Eliades, G. Effect of Various Curing Lights on the Degree of Cure of Orthodontic Adhesives. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 382–384. [Google Scholar] [CrossRef]
- Par, M.; Tarle, Z.; Hickel, R.; Ilie, N. Polymerization Kinetics of Experimental Bioactive Composites Containing Bioactive Glass. J. Dent. 2018, 76, 83–88. [Google Scholar] [CrossRef]
- Üşümez, S.; Büyükyilmaz, T.; Karaman, A.İ.; Gündüz, B. Degree of Conversion of Two Lingual Retainer Adhesives Cured with Different Light Sources. Eur. J. Orthod. 2005, 27, 173–179. [Google Scholar] [CrossRef]
- Eliades, T. Degree of Cure of Orthodontic Adhesives with Various Polymerization Initiation Modes. Eur. J. Orthod. 2000, 22, 395–399. [Google Scholar] [CrossRef]
- Soyland, R.; Currier, G.F.; Kadioglu, O.; Li, J.; Esteban Florez, F.L.; Rueggeberg, F.A.; Khajotia, S.S. Pairing Orthodontic Adhesive Resins and Light-Curing Units for Optimal Degree of Conversion. J. World Fed. Orthod. 2020, 9, 68–74. [Google Scholar] [CrossRef]
- Bolaños-Carmona, V.; Zein, B.; Menéndez-Núñez, M.; Sánchez-Sánchez, P.; Ceballos-García, L.; González-López, S. Influence of the Bracket on Bonding and Physical Behavior of Orthodontic Resin Cements. Dent. Mater. J. 2015, 34, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Shinya, M.; Shinya, A.; Lassila, L.V.J.; Varrela, J.; Vallittu, P.K. Enhanced Degree of Monomer Conversion of Orthodontic Adhesives Using a Glass-Fiber Layer under the Bracket. Angle Orthod. 2009, 79, 546–550. [Google Scholar] [CrossRef]
- Andrzejewska, E. Photopolymerization Kinetics of Multifunctional Monomers. Prog. Polym. Sci. 2001, 26, 605–665. [Google Scholar] [CrossRef]
- Par, M.; Gamulin, O.; Marovic, D.; Klaric, E.; Tarle, Z. Effect of Temperature on Post-Cure Polymerization of Bulk-Fill Composites. J. Dent. 2014, 42, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Fidalgo-Pereira, R.; Carvalho, Ó.; Catarino, S.O.; Henriques, B.; Torres, O.; Braem, A.; Souza, J.C.M. Effect of Inorganic Fillers on the Light Transmission through Traditional or Flowable Resin-Matrix Composites for Restorative Dentistry. Clin. Oral Investig. 2023, 27, 5679–5693. [Google Scholar] [CrossRef]
- Turssi, C.P.; Ferracane, J.L.; Vogel, K. Filler Features and Their Effects on Wear and Degree of Conversion of Particulate Dental Resin Composites. Biomaterials 2005, 26, 4932–4937. [Google Scholar] [CrossRef] [PubMed]
- Eliades, G.C.; Vougiouklakis, G.J.; Caputo, A.A. Degree of Double Bond Conversion in Light-Cured Composites. Dent. Mater. 1987, 3, 19–25. [Google Scholar] [CrossRef]
- Watts, D.C.; Amer, O.; Combe, E.C. Characteristics of Visible-Light-Activated Composite Systems. Br. Dent. J. 1984, 156, 209–215. [Google Scholar] [CrossRef]
- Heyder, M.; Kranz, S.; Beck, J.; Wettemann, M.; Hennig, C.-L.; Schulze-Späte, U.; Sigusch, B.W.; Reise, M. Influence of Layer Thickness and Shade on the Transmission of Light through Contemporary Resin Composites. Materials 2024, 17, 1554. [Google Scholar] [CrossRef]
- Mohamad, D.; Young, R.J.; Mann, A.B.; Watts, D.C. Post-Polymerization of Dental Resins Composite Evaluated with Nanoindentation and Micro-Raman Spectroscopy. Arch. Orofac. Sci. 2007, 2, 26–31. [Google Scholar]
- Par, M.; Marovic, D.; Attin, T.; Tarle, Z.; Tauböck, T.T. Effect of Rapid High-Intensity Light-Curing on Polymerization Shrinkage Properties of Conventional and Bulk-Fill Composites. J. Dent. 2020, 101, 103448. [Google Scholar] [CrossRef] [PubMed]
- Abedin, F.; Ye, Q.; Camarda, K.; Spencer, P. Impact of Light Intensity on the Polymerization Kinetics and Network Structure of Model Hydrophobic and Hydrophilic Methacrylate Based Dental Adhesive Resin. J. Biomed. Mater. Res. B Appl. Biomater. 2016, 104, 1666–1678. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.; Fidalgo-Pereira, R.; Torres, O.; Carvalho, O.; Henriques, B.; Özcan, M.; Souza, J.C.M. The Impact of Inorganic Fillers, Organic Content, and Polymerization Mode on the Degree of Conversion of Monomers in Resin-Matrix Cements for Restorative Dentistry: A Scoping Review. Clin. Oral Investig. 2024, 28, 454. [Google Scholar] [CrossRef] [PubMed]
- Kelch, M.; Stawarczyk, B.; Mayinger, F. Time-Dependent Degree of Conversion, Martens Parameters, and Flexural Strength of Different Dual-Polymerizing Resin Composite Luting Materials. Clin. Oral Investig. 2022, 26, 1067–1076. [Google Scholar] [CrossRef]
- Aldossary, M.S.; Abu Hajia, S.S.; Santini, A. Light Energy Transmission through Six Different Makes of Ceramic Orthodontic Brackets. Int. Orthod. 2018, 16, 638–651. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).